
Comparing the Costs and Diagnostic Outcomes of Replacing Cytology with the QIAsure DNA Methylation Test as a Triage within HPV Primary Cervical Cancer Screening in The Netherlands
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
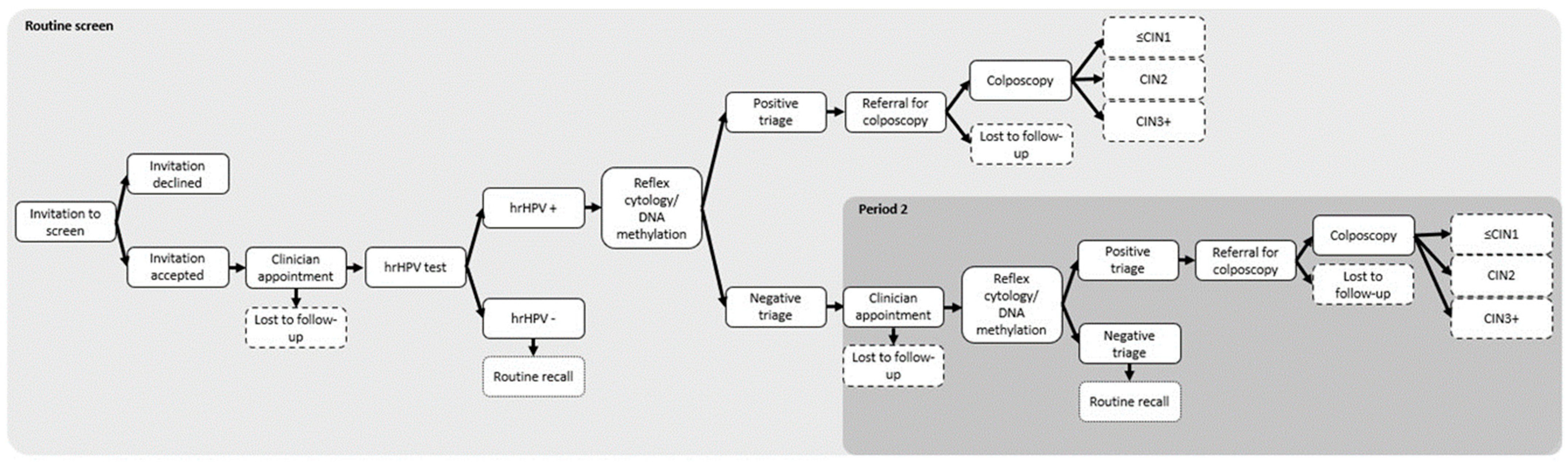
2.1. Model Type and Structure
2.2. Time Horizon
2.3. Outcomes
2.4. Population
2.5. Cost Inputs
2.6. Clinical and Disease Detection Inputs
2.7. Uncertainty Analyses
2.7.1. Deterministic Sensitivity Analysis (DSA)
2.7.2. Probabilistic Sensitivity Analysis (PSA)
2.7.3. Scenario Analyses
3. Results
3.1. Base-Case Results
3.1.1. Base-Case Results for Scenario 1 (where LBC Has Higher Sensitivity and Specificity than Methylation Testing)
3.1.2. Base-Case Results for Scenario 2 (Methylation Testing Has Higher Sensitivity and Specificity than LBC)
3.2. Sensitivity Analyses
3.2.1. Deterministic Sensitivity Analysis
3.2.2. Probabilistic Sensitivity Analysis
3.3. Scenario Analyses
4. Discussion
4.1. Main Findings
4.2. Strengths and Limitations
4.3. Interpretation
4.4. Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Crosbie, E.J.; Einstein, M.H.; Franceschi, S.; Kitchener, H.C. Human papillomavirus and cervical cancer. Lancet 2013, 382, 889–899. [Google Scholar] [CrossRef]
- Chrysostomou, C.A.; Stylianou, C.D.; Constantinidou, A.; Kostrikis, G.L. Cervical Cancer Screening Programs in Europe: The Transition Towards HPV Vaccination and Population-Based HPV Testing. Viruses 2018, 10, 729. [Google Scholar] [CrossRef]
- Sawaya, G.F.; Smith-McCune, K.; Kuppermann, M. Cervical Cancer Screening: More Choices in 2019. JAMA 2019, 321, 2018. [Google Scholar] [CrossRef]
- The National Institute for Public Health and Environment. Framework for the Execution of Cervical Cancer Population Screening. Available online: https://www.rivm.nl/documenten/framework-for-execution-of-cervical-cancer-population-screening (accessed on 11 September 2023).
- Actuele Ontwikkelingen—Bevolkingsonderzoek Baarmoederhalskanker. Available online: https://www.rivm.nl/bevolkingsonderzoek-baarmoederhalskanker/professionals/actuele-ontwikkelingen (accessed on 11 September 2023).
- Davies-Oliveira, J.; Smith, M.; Grover, S.; Canfell, K.; Crosbie, E. Eliminating cervical cancer: Progress and challenges for high-income countries. Clin. Oncol. 2021, 33, 550–559. [Google Scholar] [CrossRef]
- Gezondheidsraad. Verbetermogelijkheden Bevolkingsonderzoek Baarmoederhalskanker. Den Haag. 2021. Available online: https://www.gezondheidsraad.nl/documenten/adviezen/2021/10/19/verbetermogelijkheden-bevolkingsonderzoek-baarmoederhalskanker (accessed on 1 December 2022).
- Nanda, K.; McCrory, D.C.; Myers, E.R.; Bastian, L.A.; Hasselblad, V.; Hickey, J.D.; Matchar, D.B. Accuracy of the Papanicolaou Test in Screening for and Follow-up of Cervical Cytologic Abnormalities: A Systematic Review. Ann. Intern. Med. 2000, 132, 810. [Google Scholar] [CrossRef] [PubMed]
- Fahey, M.T.; Irwig, L.; Macaskill, P. Meta-analysis of Pap Test Accuracy. Am. J. Epidemiol. 1995, 141, 680–689. [Google Scholar] [CrossRef] [PubMed]
- Palmer, T.J.; Nicoll, S.M.; McKean, M.E.; Park, A.J.; Bishop, D.; Baker, L.; Imrie, J.E.A. Prospective parallel randomized trial of the MultiCyteTM ThinPrep® imaging system: The Scottish experience. Cytopathology 2013, 24, 235–245. [Google Scholar] [CrossRef] [PubMed]
- Aitken, C.A.; Van Agt, H.M.E.; Siebers, A.G.; Van Kemenade, F.J.; Niesters, H.G.M.; Melchers, W.J.G.; Vedder, J.E.M.; Schuurman, R.; Van Den Brule, A.J.C.; Van Der Linden, H.C.; et al. Introduction of primary screening using high-risk HPV DNA detection in the Dutch cervical cancer screening programme: A population-based cohort study. BMC Med. 2019, 17, 228. [Google Scholar] [CrossRef] [PubMed]
- Bergeron, C.; Giorgi-Rossi, P.; Cas, F.; Schiboni, M.L.; Ghiringhello, B.; Dalla Palma, P.; Minucci, D.; Rosso, S.; Zorzi, M.; Naldoni, C.; et al. Informed Cytology for Triaging HPV-Positive Women: Substudy Nested in the NTCC Randomized Controlled Trial. JNCI J. Natl. Cancer Inst. 2015, 107, dju423. [Google Scholar] [CrossRef] [PubMed]
- Brink, A.A.T.P.; Meijer, C.J.L.M.; Wiegerinck, M.A.H.M.; Nieboer, T.E.; Kruitwagen, R.F.P.M.; van Kemenade, F.; Fransen Daalmeijer, N.; Hesselink, A.T.; Berkhof, J.; Snijders, P.J.F. High concordance of results of testing for human papillomavirus in cervicovaginal samples collected by two methods, with comparison of a novel self-sampling device to a conventional endocervical brush. J. Clin. Microbiol. 2006, 44, 2518–2523. [Google Scholar] [CrossRef]
- Serrano, B.; Ibáñez, R.; Robles, C.; Peremiquel-Trillas, P.; de Sanjosé, S.; Bruni, L. Worldwide use of HPV self-sampling for cervical cancer screening. Prev. Med. 2022, 154, 106900. [Google Scholar] [CrossRef]
- De Strooper, L.M.A.; Hesselink, A.T.; Berkhof, J.; Meijer, C.J.L.M.; Snijders, P.J.F.; Steenbergen, R.D.M.; Heideman, D.A.M. Combined CADM1/MAL methylation and cytology testing for colposcopy triage of high-risk HPV-positive women. Cancer Epidemiol. Biomark. Prev. 2014, 23, 1933–1937. [Google Scholar] [CrossRef] [PubMed]
- De Strooper, L.M.A.; Berkhof, J.; Steenbergen, R.D.M.; Lissenberg-Witte, B.I.; Snijders, P.J.F.; Meijer, C.J.L.M.; Heideman, D.A.M. Cervical cancer risk in HPV-positive women after a negative FAM19A4/mir124-2 methylation test: A post hoc analysis in the POBASCAM trial with 14 year follow-up. Int. J. Cancer 2018, 143, 1541–1548. [Google Scholar] [CrossRef] [PubMed]
- IKNL. Monitor Bevolkingsonderzoek Baarmoederhalskanker 2021. 2022. Available online: https://www.rivm.nl/documenten/monitor-bevolkingsonderzoek-baarmoederhalskanker-2021 (accessed on 11 October 2023).
- IKNL. Monitor Bevolkingsonderzoek Baarmoederhalskanker 2019. 2021. Available online: https://www.rivm.nl/documenten/monitor-bevolkingsonderzoek-baarmoederhalskanker-2019 (accessed on 11 September 2023).
- The Minister of Health, Welfare and Sport, The Netherlands. Subsidieregeling Publieke Gezondheid (Public Health Subsidy Regulations). Available online: https://wetten.overheid.nl/BWBR0018743/2019-01-01/#HoofdstukII_Paragraaf2_Artikel46 (accessed on 11 September 2023).
- Nederlandse Zorg Autoriteit. Open Data van de Nederlandse Zorgautoriteit. Available online: https://www.opendisdata.nlt (accessed on 11 September 2023).
- IMF Data. Available online: https://data.imf.org/regular.aspx?key=61015892 (accessed on 30 November 2022).
- Bonde, J.; Floore, A.; Ejegod, D.; Vink, F.J.; Hesselink, A.; van de Ven, P.M.; Valenčak, A.O.; Pedersen, H.; Doorn, S.; Quint, W.G.; et al. Methylation markers FAM19A4 and miR124-2 as triage strategy for primary human papillomavirus screen positive women: A large European multicenter study. Int. J. Cancer 2021, 148, 396–405. [Google Scholar] [CrossRef] [PubMed]
- Luttmer, R.; De Strooper, L.M.A.; Berkhof, J.; Snijders, P.J.F.; Dijkstra, M.G.; Uijterwaal, M.H.; Steenbergen, R.D.M.; van Kemenade, F.J.; Rozendaal, L.; Helmerhorst, T.J.M.; et al. Comparing the performance of FAM19A4 methylation analysis, cytology and HPV16/18 genotyping for the detection of cervical (pre)cancer in high-risk HPV-positive women of a gynecologic outpatient population (COMETH study). Int. J. Cancer 2016, 138, 992–1002. [Google Scholar] [CrossRef] [PubMed]
- Dick, S.; Kremer, W.W.; De Strooper, L.M.A.; Lissenberg-Witte, B.I.; Steenbergen, R.D.M.; Meijer, C.J.L.M.; Berkhof, J.; Heideman, D.A.M. Long-term CIN3+ risk of HPV positive women after triage with FAM19A4/miR124-2 methylation analysis. Gynecol. Oncol. 2019, 154, 368–373. [Google Scholar] [CrossRef] [PubMed]
- Kremer, W.W.; Dick, S.; Heideman, D.A.M.; Steenbergen, R.D.M.; Bleeker, M.C.G.; Verhoeve, H.R.; van Baal, W.M.; van Trommel, N.; Kenter, G.G.; Meijer, C.J.L.M.; et al. Clinical Regression of High-Grade Cervical Intraepithelial Neoplasia Is Associated with Absence of FAM19A4/miR124-2 DNA Methylation (CONCERVE Study). J. Clin. Oncol. 2022, 40, 3037–3046. [Google Scholar] [CrossRef] [PubMed]
- Tainio, K.; Athanasiou, A.; Tikkinen, K.A.O.; Aaltonen, R.; Hernándes, J.C.; Glazer-Livson, S.; Jakobsson, M.; Joronen, K.; Kiviharju, M.; Kalliala, I. Clinical course of untreated cervical intraepithelial neoplasia grade 2 under active surveillance: Systematic review and meta-analysis. BMJ 2018, 360, k499. [Google Scholar] [CrossRef]
- McCredie, M.R.; Sharples, K.J.; Paul, C.; Baranyai, J.; Medley, G.; Jones, R.W.; Skegg, D.C. Natural history of cervical neoplasia and risk of invasive cancer in women with cervical intraepithelial neoplasia 3: A retrospective cohort study. Lancet Oncol. 2008, 9, 425–434. [Google Scholar] [CrossRef]
- Luttmer, R.; De Strooper, L.M.; Dijkstra, M.G.; Berkhof, J.; Snijders, P.J.; Steenbergen, R.D.; van Kemenade, F.J.; Rozendaal, L.; Helmerhorst, T.J.; Verheijen, R.H.; et al. FAM19A4 methylation analysis in self-samples compared with cervical scrapes for detecting cervical (pre)cancer in HPV-positive women. Br. J. Cancer 2016, 115, 579–587. [Google Scholar] [CrossRef]
- Peirson, L.; Fitzpatrick-Lewis, D.; Ciliska, D.; Warren, R. Screening for cervical cancer: A systematic review and meta-analysis. Syst. Rev. 2013, 2, 35. [Google Scholar] [CrossRef]
- Ernstson, A.; Urdell, A.; Forslund, O.; Borgfeldt, C. Cervical cancer prevention among long-term screening non-attendees by vaginal self-collected samples for hr-HPV mRNA detection. Infect. Agent. Cancer 2020, 15, 10. [Google Scholar] [CrossRef] [PubMed]
- Gok, M.; Heideman, D.A.M.; van Kemenade, F.J.; Berkhof, J.; Rozendaal, L.; Spruyt, J.W.M.; Voorhorst, F.; Belien, J.A.M.; Babovic, M.; Snijders, P.J.F.; et al. HPV testing on self collected cervicovaginal lavage specimens as screening method for women who do not attend cervical screening: Cohort study. BMJ 2010, 340, c1040. [Google Scholar] [CrossRef] [PubMed]
- Maver, P.J.; Poljak, M. Primary HPV-based cervical cancer screening in Europe: Implementation status, challenges, and future plans. Clin. Microbiol. Infect. 2020, 26, 579–583. [Google Scholar] [CrossRef] [PubMed]
- Dick, S.; Vink, F.J.; Heideman, D.A.M.; Lissenberg-Witte, B.I.; Meijer, C.J.L.M.; Berkhof, J. Risk-stratification of HPV-positive women with low-grade cytology by FAM19A4/miR124-2 methylation and HPV genotyping. Br. J. Cancer 2022, 126, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Polman, N.J.; de Haan, Y.; Veldhuijzen, N.J.; Heideman, D.A.M.; de Vet, H.C.W.; Meijer, C.J.L.M.; Massuger, L.F.A.G.; van Kemenade, F.J.; Berkhof, J. Experience with HPV self-sampling and clinician-based sampling in women attending routine cervical screening in the Netherlands. Prev. Med. 2019, 125, 5–11. [Google Scholar] [CrossRef]
- Rebolj, M.; Bonde, J.; Preisler, S.; Ejegod, D.; Rygaard, C.; Lynge, E. Human Papillomavirus assays and cytology in primary cervical screening of women aged 30 years and above. PLoS ONE 2016, 11, e0147326. [Google Scholar] [CrossRef]


{kind=link}
| Parameter | Strategy | Base Value (EUR) | Low Value (EUR) 1 | High Value (EUR) 1 | PSA Distribution | Reference/ Comment |
|---|---|---|---|---|---|---|
| Cost data | ||||||
| Clinician-collected sampling | ||||||
| Sample collection (routine screen 2) | Both 4 | 24.63 | 22.17 | 27.09 | Gamma | [20] |
| Sample collection (early recall 3) | Both | 21.37 | 19.23 | 23.51 | Gamma | [20] |
| hrHPV testing | Both | 16.57 | 14.91 | 18.23 | Gamma | [20] |
| LBC (routine screen 2) | LBC | 26.99 | 24.29 | 29.69 | Gamma | [20] |
| LBC (early recall 3) | LBC | 34.92 | 31.43 | 38.41 | Gamma | [20] |
| Self-sampling | ||||||
| Self-sampling kit | Both | 10.98 | 9.88 | 12.08 | Gamma | [20] |
| Sample collection (early recall 3) | Both | 20.08 | 18.07 | 22.09 | Gamma | [20] |
| hrHPV testing | Both | 15.16 | 13.64 | 16.68 | Gamma | [20] |
| LBC (routine screen 2) | LBC | 43.92 | 39.53 | 48.31 | Gamma | [20] |
| LBC (early recall 3) | LBC | 34.92 | 31.43 | 38.41 | Gamma | [20] |
| All sampling strategies | ||||||
| Colposcopy 5 | Both | 545.00 | 490.50 | 599.50 | Gamma | [21] |
| Organisational costs 6 | Both | 10.93 | 14.79 | 9.93 | Gamma | Supplementary Table S6 |
| DNA methylation | DNA methylation | 29.44 | 27.02 | 42.02 | Gamma | Estimate, Supplementary Table S5 |
| Probabilities using annual surveillance data [18,19] | ||||||
| Clinician-collected sampling | ||||||
| Clinician-collected sampling | Both | 77.90% | 80.11% | 75.69% | Beta | [18] |
| Attends sample collection appointment | Both | 91.39% | 82.25% | 100.00% | Beta | [19] |
| hrHPV-positive result | Both | 9.96% | 8.97% | 10.96% | Beta | [19] |
| LTFU at colposcopy referral (routine screen 2) | Both | 28.51% | 35.66% | 21.36% | Beta | [19] |
| LTFU at colposcopy referral (early recall 3) | Both | 42.52% | 51.15% | 33.90% | Beta | [19] |
| LTFU at early recall (early recall 3) | Both | 3.44% | 0.00% | 3.78% | Beta | [19] |
| Self-sampling | ||||||
| hrHPV-positive result | Both | 8.38% | 7.54% | 9.22% | Beta | [19] |
| Returns for sample collection appointment | LBC | 79.25% | 71.33% | 87.18% | Beta | [19] |
| LTFU at colposcopy referral (routine screen 2) | Both | 20.75% | 14.52% | 26.97% | Beta | [19] |
| LTFU at colposcopy referral (early recall 3) | Both | 76.19% | 78.57% | 40.48% | Beta | [19] |
| LTFU at early recall (early recall 3) | Both | 3.47% | 0.00% | 3.81% | Beta | [19] |
| Scenario 1: LBC has higher sensitivity and specificity than DNA methylation testing [23] | ||||||
| Clinician-collected sampling | ||||||
| LBC abnormal (routine screen 2) | LBC | 28.33% | 25.50% | 31.17% | Beta | Supplementary Table S15 |
| LBC abnormal (early recall 3) | LBC | 7.18% | 6.47% | 7.90% | Beta | Supplementary Table S15 |
| DNA methylation positive (routine screen 2) | DNA methylation | 28.57% | 25.72% | 31.43% | Beta | Supplementary Table S15 |
| DNA methylation positive (early recall 3) | DNA methylation | 7.25% | 6.52% | 7.97% | Beta | Supplementary Table S15 |
| Self-sampling | ||||||
| LBC abnormal (routine screen 2) | LBC | 30.16% | 27.14% | 33.18% | Beta | Supplementary Table S15 |
| LBC abnormal (early recall 3) | LBC | 2.60% | 2.34% | 2.86% | Beta | Supplementary Table S15 |
| DNA methylation positive (routine screen 2) | DNA methylation | 32.20% | 28.98% | 35.42% | Beta | Supplementary Table S15 |
| DNA methylation positive (early recall 3 | DNA methylation | 2.78% | 2.50% | 3.05% | Beta | Supplementary Table S15 |
| Scenario 2 DNA methylation testing has higher sensitivity and specificity than LBC 7 [24] | ||||||
| Clinician-collected sampling | ||||||
| LBC abnormal (routine screen 2) | LBC | 56.78% | 51.10% | 62.46% | Beta | Supplementary Table S15 |
| LBC abnormal (early recall 3) | LBC | 7.18% | 6.47% | 7.90% | Beta | Supplementary Table S15 |
| DNA methylation positive (routine screen 2) | DNA methylation | 46.61% | 41.95% | 51.27% | Beta | Supplementary Table S15 |
| DNA methylation positive (early recall 3) | DNA methylation | 5.90% | 5.31% | 6.49% | Beta | Supplementary Table S15 |
| Self-sampling | ||||||
| LBC abnormal (routine screen 2) | LBC | 60.16% | 54.15% | 66.18% | Beta | Supplementary Table S15 |
| LBC abnormal (early recall 3) | LBC | 2.60% | 2.34% | 2.86% | Beta | Supplementary Table S15 |
| DNA methylation positive (routine screen 2) | DNA methylation | 51.04% | 45.93% | 56.14% | Beta | Supplementary Table S15 |
| DNA methylation positive (early recall 3) | DNA methylation | 2.21% | 1.99% | 2.43% | Beta | Supplementary Table S15 |
| Outcome | LBC | DNA Methylation | % Change 1 | Incremental Difference 2 (95% CI) * |
|---|---|---|---|---|
| Scenario 1: base-case results | ||||
| Number of complete screens | 415,483 | 416,888 | 0.3% | 1405 |
| Number LTFU | 6766 | 5361 | −20.8% | −1405 |
| Number of ≤CIN1 diagnoses | 4369 | 5746 | 31.5% | 1376 (1208; 1551) |
| Number of CIN2+ diagnoses | 4369 | 3509 | −19.7% | −860 |
| Number of CIN3+ diagnoses | 2470 | 2233 | −9.6% | −236 (−353; −117) |
| Total screening costs (EUR) | 41,099,596 | 40,895,452 | −0.5% | −204,144 |
| Costs related to sample collection (EUR) 3 | 9,738,670 | 9,338,105 | −4.1% | −400,565 |
| Costs related to laboratory testing (EUR) 4 | 8,946,292 | 8,861,200 | −1.0% | −85,092 |
| Costs related to colposcopy (EUR) 5 | 4,762,298 | 5,043,811 | 5.9% | 281,513 |
| Cost per complete screen (EUR) 6 | 98.92 | 98.10 | −0.8% | −0.82 (−1.78; 0.15) |
| Cost per CIN2+ diagnosis (EUR) 7 | 9407 | 11,654 | 23.9% | 2247 |
| Cost per CIN3+ diagnosis (EUR) 8 | 16,642 | 18,312 | 10.0% | 1671 |
| Scenario 2: base-case results | ||||
| Number of complete screens | 412,859 | 415,244 | 0.6% | 2385 |
| Number LTFU | 9389 | 7004 | −25.4% | −2385 |
| Number of ≤CIN1 diagnoses | 7880 | 6690 | −15.1% | −1191 (−1409; −929) |
| Number of CIN2+ diagnoses | 8294 | 7345 | −11.4% | −949 |
| Number of CIN3+ diagnoses | 4693 | 5169 | 10.1% | 475 (275; 713) |
| Total screening costs (EUR) | 44,547,572 | 43,212,775 | −3.0% | −1,334,797 |
| Costs related to sample collection (EUR) 3 | 9,509,079 | 9,259,968 | −2.6% | −249,111 |
| Costs related to laboratory testing (EUR) 4 | 8,571,124 | 8,651,684 | 0.9% | 80,560 |
| Costs related to colposcopy (EUR) 5 | 8,815,033 | 7,648,787 | −13.2% | −1,166,247 |
| Cost per complete screen (EUR) 6 | 107.90 | 104.07 | −3.6% | −3.83 (−4.80; 2.77) |
| Cost per CIN2+ diagnosis (EUR) 7 | 5371 | 5883 | 9.5% | 512 |
| Cost per CIN3+ diagnosis (EUR) 8 | 9492 | 8361 | −11.9% | −1131 |
| Scenario | Number of People LTFU | Number of ≤CIN1 Diagnoses | Number of CIN3+ Diagnoses | Total Cost of Screening (EUR) | Cost per Complete Screen (EUR) |
|---|---|---|---|---|---|
| Scenario 1: LBC has higher sensitivity and specificity than DNA methylation testing [23] | |||||
| Scenario 1.1: 100% clinician-collected sampling, 0% self-sampling | |||||
| LBC | 5215 | 4913 | 2530 | 42,603,221 | 104.31 |
| DNA methylation test | 5245 | 6240 | 2173 | 42,289,928 | 103.55 |
| Incremental 1 | 29 | 1327 | −357 | −313,293 | −0.76 |
| Scenario 1.2: 75% clinician-collected sampling, 25% self-sampling | |||||
| LBC | 10,477 | 3068 | 2326 | 37,499,862 | 86.73 |
| DNA methylation test | 5638 | 4562 | 2378 | 37,557,026 | 85.90 |
| Incremental | −4839 | 1494 | 52 | 57,164 | −0.83 |
| Scenario 1.3: 50% clinician-collected sampling, 50% self-sampling | |||||
| LBC | 8723 | 3683 | 2394 | 39,200,982 | 92.37 |
| DNA methylation test | 5507 | 5121 | 2309 | 39,134,660 | 91.52 |
| Incremental | −3216 | 1438 | −84 | −66,322 | −0.85 |
| Scenario 1.4: 25% clinician-collected sampling, 75% self-sampling | |||||
| LBC | 6969 | 4298 | 2462 | 40,902,101 | 98.23 |
| DNA methylation test | 5376 | 5681 | 2241 | 40,712,294 | 97.40 |
| Incremental | −1593 | 1383 | −221 | −189,807 | −0.83 |
| Scenario 1.5: 0% clinician-collected sampling, 100% self-sampling | |||||
| LBC | 12,230 | 2453 | 2258 | 35,798,743 | 81.29 |
| DNA methylation test | 5769 | 4002 | 2446 | 35,979,392 | 80.52 |
| Incremental | −6462 | 1550 | 188 | 180,650 | −0.77 |
| Scenario 1.6: same test performance for LBC and DNA methylation test 2 | |||||
| LBC | 6766 | 4369 | 2470 | 41,099,596 | 98.92 |
| DNA methylation test | 5279 | 4511 | 2600 | 40,811,627 | 97.88 |
| Incremental | −1487 | 142 | 131 | −287,970 | −1.04 |
| Scenario 2: DNA methylation testing has higher sensitivity and specificity than LBC [24] | |||||
| Scenario 2.1: 100% clinician-collected sampling, 0% self-sampling | |||||
| LBC | 7810 | 8748 | 4766 | 46,278,868 | 114.04 |
| DNA methylation test | 6766 | 7186 | 4983 | 44,643,326 | 109.72 |
| Incremental | −1043 | −1562 | 217 | −1,635,542 | −4.31 |
| Scenario 2.2: 75% clinician-collected sampling, 25% self-sampling | |||||
| LBC | 13,171 | 5803 | 4518 | 40,402,785 | 94.02 |
| DNA methylation test | 7574 | 5501 | 5612 | 39,787,981 | 91.40 |
| Incremental | −5598 | −302 | 1094 | −614,804 | −2.62 |
| Scenario 2.3: 50% clinician-collected sampling, 50% self-sampling | |||||
| LBC | 11,384 | 6785 | 4601 | 42,361,479 | 100.44 |
| DNA methylation test | 7304 | 6063 | 5402 | 41,406,429 | 97.24 |
| Incremental | −4080 | −722 | 802 | −955,050 | −3.21 |
| Scenario 2.4: 25% clinician-collected sampling, 75% self-sampling | |||||
| LBC | 9597 | 7766 | 4684 | 44,320,173 | 107.11 |
| DNA methylation test | 7035 | 6624 | 5193 | 43,024,878 | 103.34 |
| Incremental | −2562 | −1142 | 509 | −1,295,296 | −3.77 |
| Scenario 2.5: 0% clinician-collected sampling, 100% self-sampling | |||||
| LBC | 14,959 | 4821 | 4435 | 38,444,090 | 87.84 |
| DNA methylation test | 7843 | 4939 | 5821 | 38,169,532 | 85.82 |
| Incremental | −7116 | 118 | 1387 | −274,558 | −2.02 |
| Scenario 2.6: same test performance for LBC and DNA methylation 2 | |||||
| LBC | 9389 | 7880 | 4693 | 44,547,572 | 107.90 |
| DNA methylation test | 8060 | 8159 | 4950 | 44,591,104 | 107.66 |
| Incremental | −1329 | 279 | 257 | 43,532 | −0.24 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Puri Sudhir, K.; Kagenaar, E.; Meijer, M.; Hesselink, A.T.; Adams, E.; Turner, K.M.E.; Huntington, S. Comparing the Costs and Diagnostic Outcomes of Replacing Cytology with the QIAsure DNA Methylation Test as a Triage within HPV Primary Cervical Cancer Screening in The Netherlands. Diagnostics 2023, 13, 3612. https://doi.org/10.3390/diagnostics13243612
Puri Sudhir K, Kagenaar E, Meijer M, Hesselink AT, Adams E, Turner KME, Huntington S. Comparing the Costs and Diagnostic Outcomes of Replacing Cytology with the QIAsure DNA Methylation Test as a Triage within HPV Primary Cervical Cancer Screening in The Netherlands. Diagnostics. 2023; 13(24):3612. https://doi.org/10.3390/diagnostics13243612
Chicago/Turabian StylePuri Sudhir, Krishnan, Eva Kagenaar, Michelle Meijer, Albertus T. Hesselink, Elisabeth Adams, Katy M. E. Turner, and Susie Huntington. 2023. "Comparing the Costs and Diagnostic Outcomes of Replacing Cytology with the QIAsure DNA Methylation Test as a Triage within HPV Primary Cervical Cancer Screening in The Netherlands" Diagnostics 13, no. 24: 3612. https://doi.org/10.3390/diagnostics13243612
APA StylePuri Sudhir, K., Kagenaar, E., Meijer, M., Hesselink, A. T., Adams, E., Turner, K. M. E., & Huntington, S. (2023). Comparing the Costs and Diagnostic Outcomes of Replacing Cytology with the QIAsure DNA Methylation Test as a Triage within HPV Primary Cervical Cancer Screening in The Netherlands. Diagnostics, 13(24), 3612. https://doi.org/10.3390/diagnostics13243612