
Changes in CT-Based Morphological Features of the Kidney with Declining Glomerular Filtration Rate in Chronic Kidney Disease
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Image Preprocessing and Feature Extraction
2.3. Statistical Analyses
3. Results
3.1. Patient Characteristics and Feature Summary
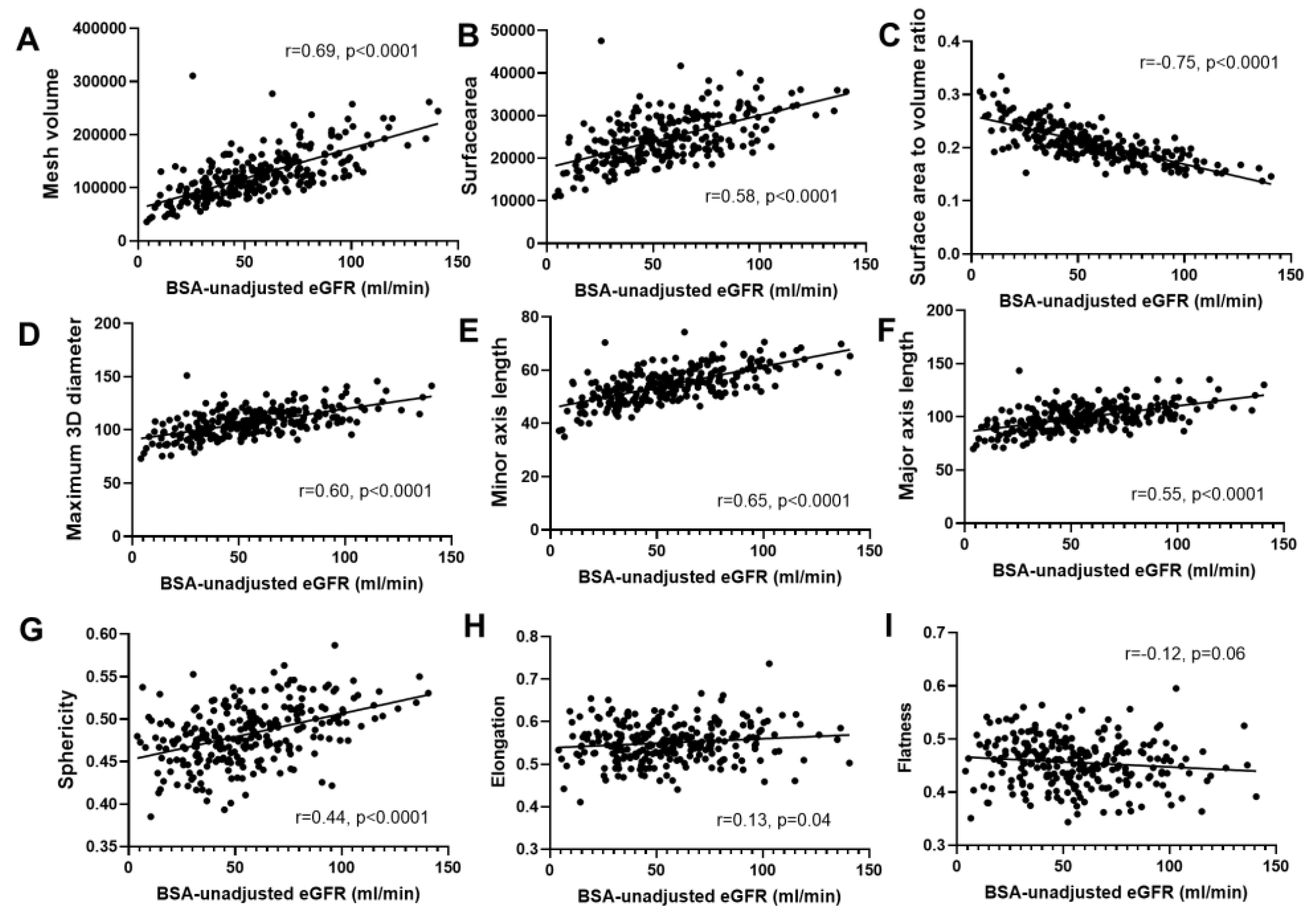
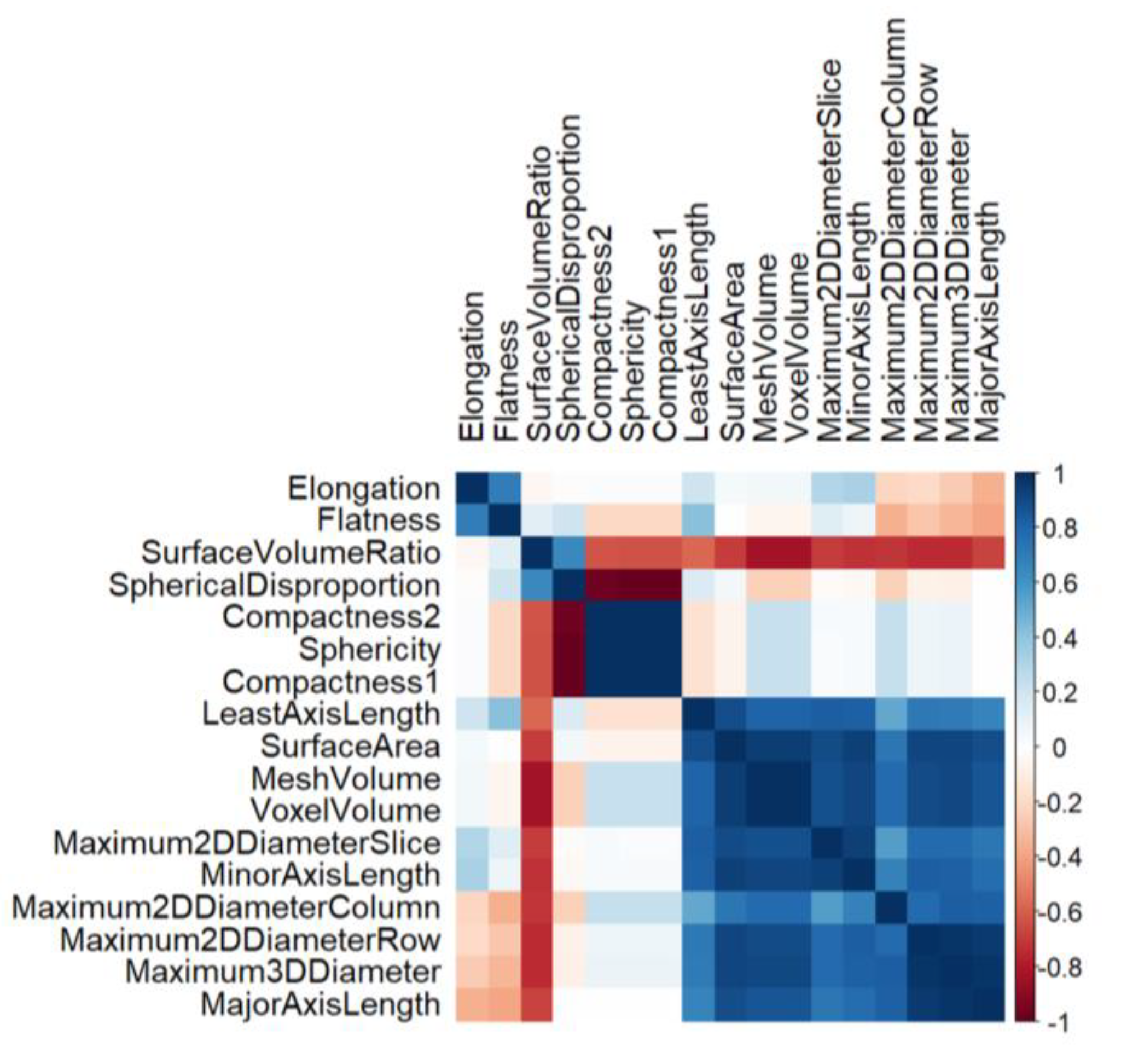
3.2. Correlation Analysis
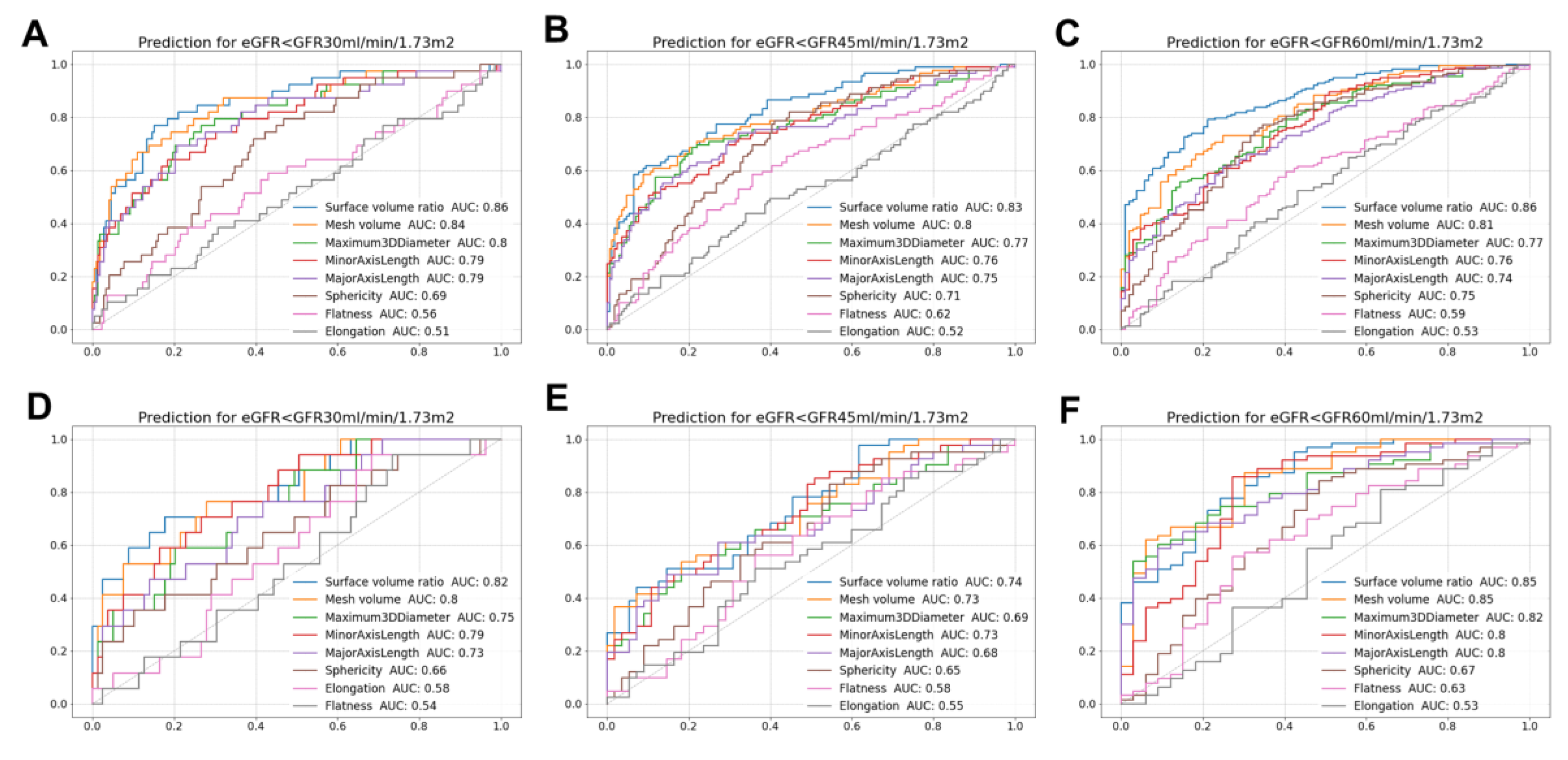
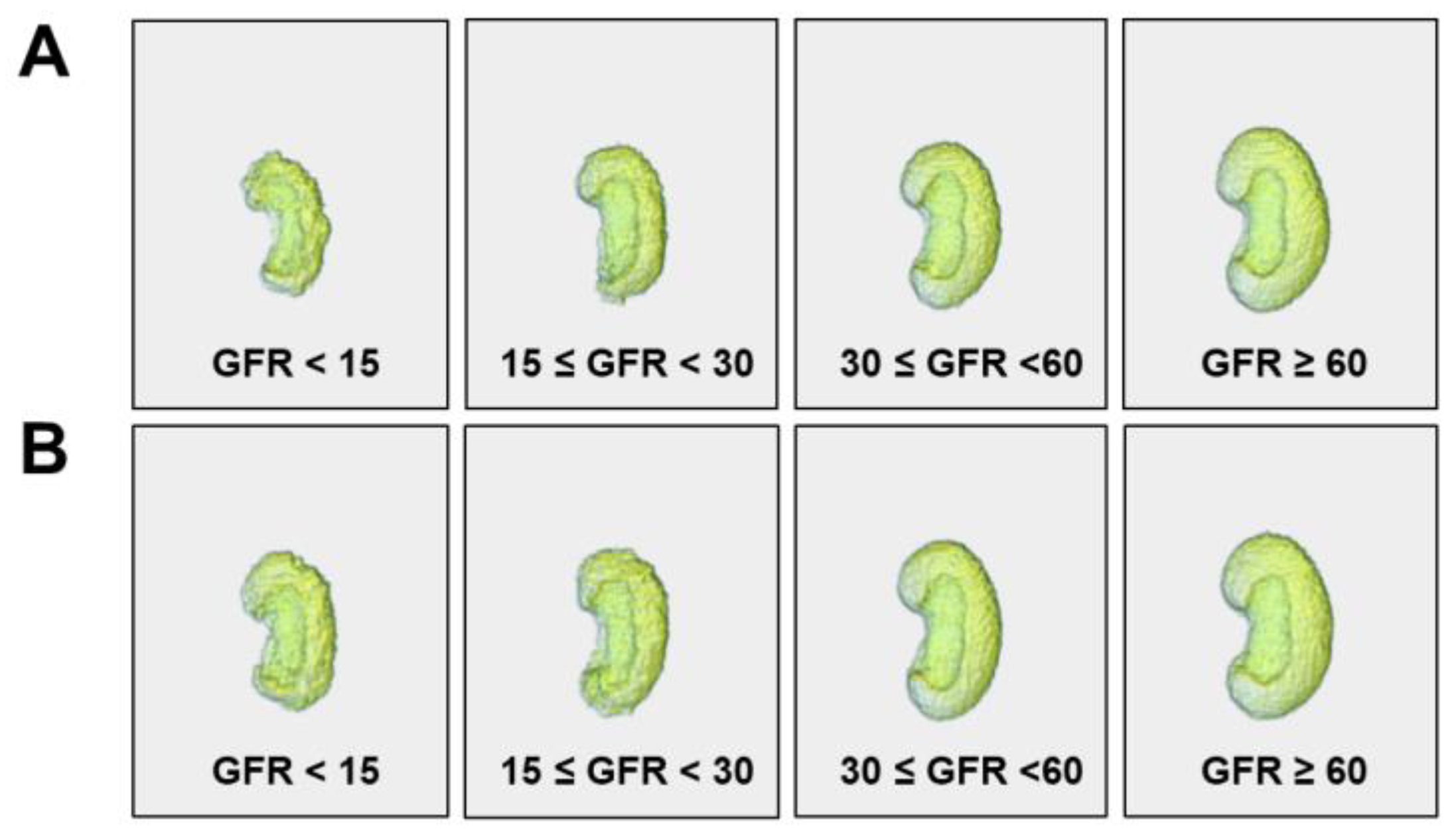
3.3. Diagnostic Value of Features and 3D Visualization
3.4. Determinants of Surface-Area-to-Volume Ratio
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD Chronic Kidney Disease Collaboration. Global, regional, and national burden of chronic kidney disease, 1990-2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 709–733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lv, J.C.; Zhang, L.X. Prevalence and Disease Burden of Chronic Kidney Disease. Adv. Exp. Med. Biol. 2019, 1165, 3–15. [Google Scholar] [CrossRef] [PubMed]
- Chang, A.; Gibson, I.W.; Cohen, A.H.; Weening, J.W.; Jennette, J.C.; Fogo, A.B.; Renal Pathology Society. A position paper on standardizing the nonneoplastic kidney biopsy report. Hum. Pathol. 2012, 43, 1192–1196. [Google Scholar] [CrossRef]
- Sethi, S.; Haas, M.; Markowitz, G.S.; D’Agati, V.D.; Rennke, H.G.; Jennette, J.C.; Bajema, I.M.; Alpers, C.E.; Chang, A.; Cornell, L.D.; et al. Mayo Clinic/Renal Pathology Society Consensus Report on Pathologic Classification, Diagnosis, and Reporting of GN. J. Am. Soc. Nephrol. 2016, 27, 1278–1287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Srivastava, A.; Palsson, R.; Kaze, A.D.; Chen, M.E.; Palacios, P.; Sabbisetti, V.; Betensky, R.A.; Steinman, T.I.; Thadhani, R.I.; McMahon, G.M.; et al. The Prognostic Value of Histopathologic Lesions in Native Kidney Biopsy Specimens: Results from the Boston Kidney Biopsy Cohort Study. J. Am. Soc. Nephrol. 2018, 29, 2213–2224. [Google Scholar] [CrossRef] [Green Version]
- Fufaa, G.D.; Weil, E.J.; Lemley, K.V.; Knowler, W.C.; Brosius, F.C., 3rd; Yee, B.; Mauer, M.; Nelson, R.G. Structural Predictors of Loss of Renal Function in American Indians with Type 2 Diabetes. Clin. J. Am. Soc. Nephrol. 2016, 11, 254–261. [Google Scholar] [CrossRef] [Green Version]
- Bjorneklett, R.; Sriskandarajah, S.; Bostad, L. Prognostic Value of Histologic Classification of ANCA-Associated Glomerulonephritis. Clin. J. Am. Soc. Nephrol. 2016, 11, 2159–2167. [Google Scholar] [CrossRef] [Green Version]
- Working Group of the International IgA Nephropathy Network and the Renal Pathology Society; Roberts, I.S.; Cook, H.T.; Troyanov, S.; Alpers, C.E.; Amore, A.; Barratt, J.; Berthoux, F.; Bonsib, S.; Brujin, J.A.; et al. The Oxford classification of IgA nephropathy: Pathology definitions, correlations, and reproducibility. Kidney Int. 2009, 76, 546–556. [Google Scholar] [CrossRef] [Green Version]
- Levin, A.S.; Bilous, R.W.; Coresh, J. Chapter 1: Definition and classification of CKD. Kidney Int. Suppl. 2013, 3, 19–62. [Google Scholar] [CrossRef] [Green Version]
- Araujo, N.C.; Rebelo, M.A.P.; da Silveira Rioja, L.; Suassuna, J.H.R. Sonographically determined kidney measurements are better able to predict histological changes and a low CKD-EPI eGFR when weighted towards cortical echogenicity. BMC Nephrol. 2020, 21, 123. [Google Scholar] [CrossRef]
- Nakazato, T.; Ikehira, H.; Imasawa, T. Determinants of renal shape in chronic kidney disease patients. Clin. Exp. Nephrol. 2016, 20, 748–756. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Zwanenburg, A.; Vallieres, M.; Abdalah, M.A.; Aerts, H.; Andrearczyk, V.; Apte, A.; Ashrafinia, S.; Bakas, S.; Beukinga, R.J.; Boellaard, R.; et al. The Image Biomarker Standardization Initiative: Standardized Quantitative Radiomics for High-Throughput Image-based Phenotyping. Radiology 2020, 295, 328–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pyradiomics Community. Pyradiomics. Available online: https://pyradiomics.readthedocs.io/ (accessed on 30 November 2022).
- Buturovic-Ponikvar, J.; Visnar-Perovic, A. Ultrasonography in chronic renal failure. Eur. J. Radiol. 2003, 46, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Sanusi, A.A.; Arogundade, F.A.; Famurewa, O.C.; Akintomide, A.O.; Soyinka, F.O.; Ojo, O.E.; Akinsola, A. Relationship of ultrasonographically determined kidney volume with measured GFR, calculated creatinine clearance and other parameters in chronic kidney disease (CKD). Nephrol. Dial. Transplant. 2009, 24, 1690–1694. [Google Scholar] [CrossRef] [Green Version]
- Lucisano, G.; Comi, N.; Pelagi, E.; Cianfrone, P.; Fuiano, L.; Fuiano, G. Can renal sonography be a reliable diagnostic tool in the assessment of chronic kidney disease? J. Ultrasound Med. 2015, 34, 299–306. [Google Scholar] [CrossRef]
- Jovanovic, D.; Gasic, B.; Pavlovic, S.; Naumovic, R. Correlation of kidney size with kidney function and anthropometric parameters in healthy subjects and patients with chronic kidney diseases. Ren. Fail. 2013, 35, 896–900. [Google Scholar] [CrossRef]
- Shin, H.S.; Chung, B.H.; Lee, S.E.; Kim, W.J.; Ha, H.I.; Yang, C.W. Measurement of kidney volume with multi-detector computed tomography scanning in young Korean. Yonsei Med. J. 2009, 50, 262–265. [Google Scholar] [CrossRef] [Green Version]
- Johnson, S.; Rishi, R.; Andone, A.; Khawandi, W.; Al-Said, J.; Gletsu-Miller, N.; Lin, E.; Baumgarten, D.A.; O’Neill, W.C. Determinants and functional significance of renal parenchymal volume in adults. Clin. J. Am. Soc. Nephrol. 2011, 6, 70–76. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.K. Sonographic Dimensions of Normal Kidney in Korean Male. Ultrasonography 1996, 15, 63–69. [Google Scholar]
- Mazzotta, L.; Sarteschi, L.M.; Carlini, A.; Antonelli, A. Comparison of renal ultrasonographic and functional biometry in healthy patients and in patients with chronic renal failure. Arch. Ital. Urol. Androl. 2002, 74, 206–209. [Google Scholar] [PubMed]
- Tarnovski, L.; Brinar, I.V.; Kirhmajer, M.V.; Vrkic, T.Z.; Laganovic, M. Sex Differences in Cardiovascular Risk Factors and Renal Function among Young Adults after Intrauterine Growth Restriction. Acta Clin. Croat. 2021, 60, 164–172. [Google Scholar] [CrossRef]
- Hostetter, T.H. Hypertrophy and hyperfunction of the diabetic kidney. J. Clin. Investig. 2001, 107, 161–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christiansen, J.S.; Gammelgaard, J.; Frandsen, M.; Parving, H.H. Increased kidney size, glomerular filtration rate and renal plasma flow in short-term insulin-dependent diabetics. Diabetologia 1981, 20, 451–456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamada, H.; Hishida, A.; Kumagai, H.; Nishi, S. Effects of age, renal diseases and diabetes mellitus on the renal size reduction accompanied by the decrease of renal function. Nihon Jinzo Gakkai Shi 1992, 34, 1071–1075. [Google Scholar]
- Xue, C.; Yuan, J.; Lo, G.G.; Chang, A.T.Y.; Poon, D.M.C.; Wong, O.L.; Zhou, Y.; Chu, W.C.W. Radiomics feature reliability assessed by intraclass correlation coefficient: A systematic review. Quant. Imaging Med. Surg. 2021, 11, 4431–4460. [Google Scholar] [CrossRef]
- Lin, Z.; Cui, Y.; Liu, J.; Sun, Z.; Ma, S.; Zhang, X.; Wang, X. Automated segmentation of kidney and renal mass and automated detection of renal mass in CT urography using 3D U-Net-based deep convolutional neural network. Eur. Radiol. 2021, 31, 5021–5031. [Google Scholar] [CrossRef]
- Li, D.; Xiao, C.; Liu, Y.; Chen, Z.; Hassan, H.; Su, L.; Liu, J.; Li, H.; Xie, W.; Zhong, W.; et al. Deep Segmentation Networks for Segmenting Kidneys and Detecting Kidney Stones in Unenhanced Abdominal CT Images. Diagnostics 2022, 12, 1788. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics (n = 257) | |
|---|---|
| Male sex, n (%) | 143 (55.6%) |
| Age, median [range], yr | 71.0 [19.0–89.0] |
| BMI, median [IQR], kg/m2 | 24.1 [21.8–26.8] |
| BSA, mean ± SD, m2 | 1.7 ± 0.2 |
| Comorbidity, n (%) | |
| Diabetes | 96 (37.4%) |
| Hypertension | 158 (61.5%) |
| Coronary artery disease | 27 (10.5%) |
| Serum creatinine, median [IQR], mg/dL | 1.2 [0.9–1.6] |
| Estimated GFR, mean ± SD, mL/min/1.73 m2 | 57.2 ± 26.3 |
| CKD stage (eGFR range), n (%) | |
| Stage 1 (≥90 mL/min/1.73 m2) | 39 (15.2%) |
| Stage 2 (60–90 mL/min/1.73 m2) | 65 (25.3%) |
| Stage 3 (30–60 mL/min/1.73 m2) | 114 (44.4%) |
| Stage 4 (15–30 mL/min/1.73 m2) | 27 (10.5%) |
| Stage 5 (<15 mL/min/1.73 m2) | 12 (4.7%) |
| Hemoglobin, mean ± SD, g/dL | 11.3 ± 2.2 |
| Albumin, median [IQR], g/dL | 3.7 [3.2–4.1] |
| Features | Total (n = 257) | Patients without Diabetes (n = 161) | Patients with Diabetes (n = 96) | |||
|---|---|---|---|---|---|---|
| r | p-Value | r | p-Value | r | p-Value | |
| Surface-area-to-volume ratio | −0.747 | <0.0001 | −0.779 | <0.0001 | −0.702 | <0.0001 |
| Mesh volume | 0.686 | <0.0001 | 0.684 | <0.0001 | 0.717 | <0.0001 |
| Voxel volume | 0.686 | <0.0001 | 0.684 | <0.0001 | 0.712 | <0.0001 |
| Minor axis length | 0.652 | <0.0001 | 0.672 | <0.0001 | 0.637 | <0.0001 |
| Maximum 3D diameter | 0.603 | <0.0001 | 0.629 | <0.0001 | 0.593 | <0.0001 |
| Maximum 2D diameter (coronal view) | 0.605 | <0.0001 | 0.634 | <0.0001 | 0.566 | <0.0001 |
| Maximum 2D diameter (axial view) | 0.586 | <0.0001 | 0.593 | <0.0001 | 0.603 | <0.0001 |
| Maximum 2D diameter (sagittal view) | 0.584 | <0.0001 | 0.612 | <0.0001 | 0.58 | <0.0001 |
| Surface area | 0.583 | <0.0001 | 0.58 | <0.0001 | 0.629 | <0.0001 |
| Major axis length | 0.551 | <0.0001 | 0.561 | <0.0001 | 0.564 | <0.0001 |
| Least axis length | 0.454 | <0.0001 | 0.461 | <0.0001 | 0.515 | <0.0001 |
| Compactness2 | 0.439 | <0.0001 | 0.486 | <0.0001 | 0.336 | <0.0001 |
| Compactness1 | 0.437 | <0.0001 | 0.484 | <0.0001 | 0.336 | <0.0001 |
| Sphericity | 0.435 | <0.0001 | 0.482 | <0.0001 | 0.335 | <0.0001 |
| Spherical disproportion | −0.426 | <0.0001 | −0.471 | <0.0001 | −0.33 | <0.0001 |
| Elongation | 0.129 | 0.039 | 0.157 | 0.047 | 0.076 | 0.463 |
| Flatness | −0.117 | 0.062 | −0.126 | 0.112 | −0.077 | 0.456 |
| Variables | Univariable | Multivariable | ||
|---|---|---|---|---|
| Beta Coefficient | p-Value | Beta Coefficient | p-Value | |
| Sex | −0.012 | 0.004 | −0.011 | 0.0001 |
| Age | 0.001 | <0.0001 | 0.0004 | 0.0002 |
| BMI | −0.001 | 0.004 | −0.002 | <0.0001 |
| Diabetes | −0.001 | 0.739 | ||
| Hypertension | 0.005 | 0.251 | ||
| Coronary artery disease | 0.012 | 0.069 | ||
| eGFR | −0.001 | <0.0001 | −0.001 | < 0.0001 |
| Hemoglobin | −0.004 | <0.0001 | 0.001 | 0.107 |
| Albumin | 0.005 | 0.099 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, Y.H.; Jo, S.; Lee, R.W.; Kim, J.-E.; Paek, J.H.; Kim, B.; Shin, S.-Y.; Hwang, S.D.; Lee, S.W.; Song, J.H.; et al. Changes in CT-Based Morphological Features of the Kidney with Declining Glomerular Filtration Rate in Chronic Kidney Disease. Diagnostics 2023, 13, 402. https://doi.org/10.3390/diagnostics13030402
Choi YH, Jo S, Lee RW, Kim J-E, Paek JH, Kim B, Shin S-Y, Hwang SD, Lee SW, Song JH, et al. Changes in CT-Based Morphological Features of the Kidney with Declining Glomerular Filtration Rate in Chronic Kidney Disease. Diagnostics. 2023; 13(3):402. https://doi.org/10.3390/diagnostics13030402
Chicago/Turabian StyleChoi, Yoon Ho, Seongho Jo, Ro Woon Lee, Ji-Eun Kim, Jin Hyuk Paek, Byoungje Kim, Soo-Yong Shin, Seun Deuk Hwang, Seoung Woo Lee, Joon Ho Song, and et al. 2023. "Changes in CT-Based Morphological Features of the Kidney with Declining Glomerular Filtration Rate in Chronic Kidney Disease" Diagnostics 13, no. 3: 402. https://doi.org/10.3390/diagnostics13030402
APA StyleChoi, Y. H., Jo, S., Lee, R. W., Kim, J.-E., Paek, J. H., Kim, B., Shin, S.-Y., Hwang, S. D., Lee, S. W., Song, J. H., & Kim, K. (2023). Changes in CT-Based Morphological Features of the Kidney with Declining Glomerular Filtration Rate in Chronic Kidney Disease. Diagnostics, 13(3), 402. https://doi.org/10.3390/diagnostics13030402