
Relevance of Volumetric Parameters Applied to [68Ga]Ga-DOTATOC PET/CT in NET Patients Treated with PRRT

 , , ,
, , ,  , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Therapy Protocol
2.3. Images Acquisition and Evaluation
2.4. Early Clinical Response Evaluation and Follow-Up
2.5. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
3.2. Volumetric Parameters and Early Clinical Response
3.2.1. Total Tumor Burden Analysis
3.2.2. Liver Tumor Burden Analysis
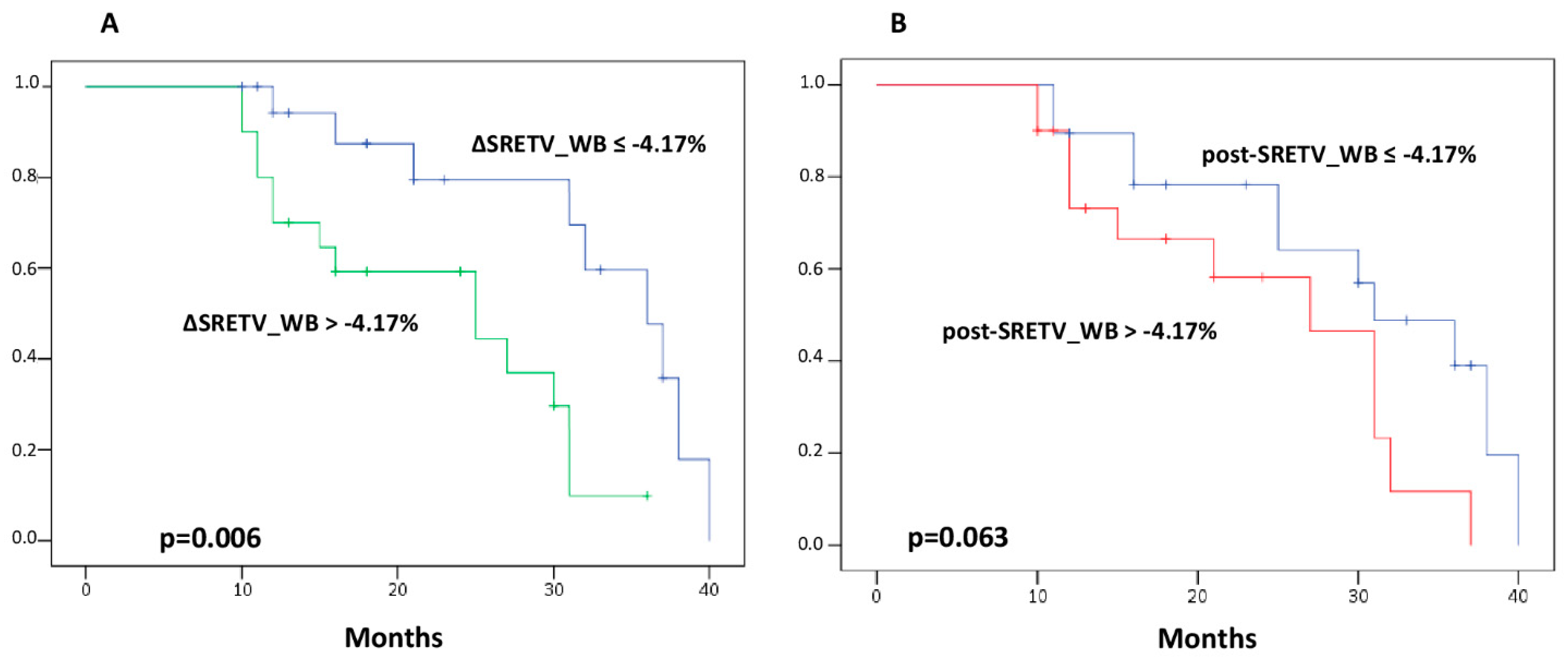
3.3. Volumetric Parameters and Clinical Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Oh, S.; Prasad, V.; Lee, D.S.; Baum, R.P. Effect of Peptide Receptor Radionuclide Therapy on Somatostatin Receptor Status and Glucose Metabolism in Neuroendocrine Tumors: Intraindividual Comparison of Ga-68 DOTANOC PET/CT and F-18 FDG PET/CT. Int. J. Mol. Imaging 2011, 2011, 524130. [Google Scholar] [CrossRef]
- Paganelli, G.; Sansovini, M.; Nicolini, S.; Grassi, I.; Ibrahim, T.; Amadori, E.; Di Iorio, V.; Monti, M.; Scarpi, E.; Bongiovanni, A.; et al. 177Lu-PRRT in advanced gastrointestinal neuroendocrine tumors: 10-year follow-up of the IRST phase II prospective study. Eur. J. Nucl. Med. Mol. Imaging 2020, 48, 152–160. [Google Scholar] [CrossRef] [PubMed]
- Reubi, J.; Waser, B.; Schaer, J.-C.; Laissue, J.A. Somatostatin receptor sst1–sst5 expression in normal and neoplastic human tissues using receptor autoradiography with subtype-selective ligands. Eur. J. Nucl. Med. 2001, 28, 836–846. [Google Scholar] [CrossRef] [PubMed]
- Reubi, J.C.; Schär, J.-C.; Waser, B.; Wenger, S.; Heppeler, A.; Schmitt, J.S.; Mäcke, H.R. Affinity profiles for human somatostatin receptor subtypes SST1–SST5 of somatostatin radiotracers selected for scintigraphic and radiotherapeutic use. Eur. J. Nucl. Med. 2000, 27, 273–282. [Google Scholar] [CrossRef] [PubMed]
- Maecke, H.R.; Reubi, J.C. Somatostatin Receptors as Targets for Nuclear Medicine Imaging and Radionuclide Treatment. J. Nucl. Med. 2011, 52, 841–844. [Google Scholar] [CrossRef]
- Werner, R.A.; Bluemel, C.; Allen-Auerbach, M.S.; Higuchi, T.; Herrmann, K. 68Gallium- and 90Yttrium-/177Lutetium: “theranostic twins” for diagnosis and treatment of NETs. Ann. Nucl. Med. 2014, 29, 1–7. [Google Scholar] [CrossRef]
- Squires, M.H.; Volkan Adsay, N.; Schuster, D.M.; Russell, M.C.; Cardona, K.; Delman, K.A.; Winer, J.H.; Altinel, D.; Sarmiento, J.M.; El-Rayes, B.; et al. Octreoscan Versus FDG-PET for Neuroendocrine Tumor Staging: A Biological Approach. Ann. Surg. Oncol. 2015, 22, 2295–2301. [Google Scholar] [CrossRef]
- Uccelli, L.; Boschi, A.; Cittanti, C.; Martini, P.; Panareo, S.; Tonini, E.; Nieri, A.; Urso, L.; Caracciolo, M.; Lodi, L.; et al. 90Y/177Lu-DOTATOC: From Preclinical Studies to Application in Humans. Pharmaceutics 2021, 13, 1463. [Google Scholar] [CrossRef]
- Baum, R.P.; Kluge, A.W.; Kulkarni, H.; Schorr-Neufing, U.; Niepsch, K.; Bitterlich, N.; van Echteld, C.J.A. [177Lu-DOTA]0-D-Phe1-Tyr3-Octreotide (177Lu-DOTA TOC) for peptide receptor radiotherapy in patients with advanced neuroendocrine tumours: A Phase-II study. Theranostics 2016, 6, 501–510. [Google Scholar] [CrossRef]
- Urso, L.; Nieri, A.; Rambaldi, I.; Castello, A.; Uccelli, L.; Cittanti, C.; Panareo, S.; Gagliardi, I.; Ambrosio, M.R.; Zatelli, M.C.; et al. Radioligand therapy (RLT) as neoadjuvant treatment for inoperable pancreatic neuroendocrine tumors: A literature review. Endocr. 2022, 78, 255–261. [Google Scholar] [CrossRef]
- Pattison, D.A.; Hofman, M.S. Role of fluorodeoxyglucose PET/computed tomography in targeted radionuclide therapy for endocrine malignancies. PET Clin. 2015, 10, 461–476. [Google Scholar] [CrossRef]
- Binderup, T.; Knigge, U.; Johnbeck, C.B.; Loft, A.; Berthelsen, A.K.; Oturai, P.; Mortensen, J.; Federspiel, B.; Langer, S.W.; Kjaer, A. 18F-FDG-PET is superior to WHO grading as prognostic tool in neuroendocrine neoplasms and useful in guiding peptide receptor radionuclide therapy: A prospective 10-year follow-up study of 166 patients. J. Nucl. Med. 2020, 62, 808–815. [Google Scholar] [CrossRef] [PubMed]
- Magi, L.; Prosperi, D.; Lamberti, G.; Marasco, M.; Ambrosini, V.; Rinzivillo, M.; Campana, D.; Gentiloni, G.; Annibale, B.; Signore, A.; et al. Role of [18F]FDG PET/CT in the management of G1 gastro-entero-pancreatic neuroendocrine tumors. Endocrine 2022, 76, 484. [Google Scholar] [CrossRef] [PubMed]
- Urso, L.; Panareo, S.; Castello, A.; Ambrosio, M.R.; Zatelli, M.C.; Caracciolo, M.; Tonini, E.; Valpiani, G.; Boschi, A.; Uccelli, L.; et al. Glucose Metabolism Modification Induced by Radioligand Therapy with [177Lu]Lu/[90Y]Y-DOTATOC in Advanced Neuroendocrine Neoplasms: A Prospective Pilot Study within FENET-2016 Trial. Pharmaceutics 2022, 14, 2009. [Google Scholar] [CrossRef]
- Ambrosini, V.; Kunikowska, J.; Baudin, E.; Bodei, L.; Bouvier, C.; Capdevila, J.; Cremonesi, M.; de Herder, W.W.; Dromain, C.; Falconi, M.; et al. Consensus on molecular imaging and theranostics in neuroendocrine neoplasms. Eur. J. Cancer 2021, 146, 56–73. [Google Scholar] [CrossRef]
- Shah, R.; Garg, R.; Majmundar, M.; Purandare, N.; Malhotra, G.; Patil, V.; Ramteke-Jadhav, S.; Lila, A.; Shah, N.; Bandgar, T. Exendin-4-based imaging in insulinoma localization: Systematic review and meta-analysis. Clin. Endocrinol. 2021, 95, 354–364. [Google Scholar] [CrossRef] [PubMed]
- Treglia, G.; Sadeghi, R.; Giovinazzo, F.; Galiandro, F.; Annunziata, S.; Muoio, B.; Kroiss, A.S. Pet with different radiopharmaceuticals in neuroendocrine neoplasms: An umbrella review of published meta-analyses. Cancers 2021, 13, 5172. [Google Scholar] [CrossRef] [PubMed]
- Bozkurt, M.F.; Virgolini, I.; Balogova, S.; Beheshti, M.; Rubello, D.; Decristoforo, C.; Ambrosini, V.; Kjaer, A.; Delgado-Bolton, R.; Kunikowska, J.; et al. Guideline for PET/CT imaging of neuroendocrine neoplasms with 68Ga-DOTA-conjugated somatostatin receptor targeting peptides and 18F–DOPA. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 1588–1601. [Google Scholar] [CrossRef]
- Taïeb, D.; Garrigue, P.; Bardiès, M.; Abdullah, A.E.; Pacak, K. Application and dosimetric requirements for Gallium-68-labeled somatostatin analogues in targeted radionuclide therapy for gastroenteropancreatic neuroendocrine tumors. PET Clin. 2015, 10, 477–486. [Google Scholar] [CrossRef]
- Treglia, G.; Castaldi, P.; Rindi, G.; Giordano, A.; Rufini, V. Diagnostic performance of Gallium-68 somatostatin receptor PET and PET/CT in patients with thoracic and gastroenteropancreatic neuroendocrine tumours: A meta-analysis. Endocrine 2012, 42, 80–87. [Google Scholar] [CrossRef]
- Garcia-Carbonero, R.; Sorbye, H.; Baudin, E.; Raymond, E.; Wiedenmann, B.; Niederle, B.; Sedlackova, E.; Toumpanakis, C.; Anlauf, M.; Cwikla, J.B.; et al. ENETS consensus guidelines for high-grade gastroenteropancreatic neuroendocrine tumors and neuroendocrine carcinomas. Neuroendocrinology 2016, 103, 186–194. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Brabander, T.; van der Zwan, W.A.; Teunissen, J.J.; Kam, B.L.; de Herder, W.W.; Feelders, R.A.; Krenning, E.P.; Kwekkeboom, D.J. Pitfalls in the response evaluation after Peptide Receptor Radionuclide Therapy with [177Lu-DOTA0, Tyr3] octreotate. Endocr. Relat. Cancer 2017, 24, 243–251. [Google Scholar] [CrossRef]
- Zhang, J.; Kulkarni, H.R.; Singh, A.; Baum, R.P. Delayed Response (Partial Remission) 3 Years after Peptide Receptor Radionuclide Therapy in a Patient Participating in the NETTER-1 Trial. Clin. Nucl. Med. 2019, 44, 223–226. [Google Scholar] [CrossRef] [PubMed]
- Pauwels, E.; Van Binnebeek, S.; Vandecaveye, V.; Baete, K.; Vanbilloen, H.; Koole, M.; Mottaghy, F.M.; Haustermans, K.; Clement, P.M.; Nackaerts, K.; et al. Inflammation-Based Index and 68Ga-DOTATOC PET–Derived Uptake and Volumetric Parameters Predict Outcome in Neuroendocrine Tumor Patients Treated with 90Y-DOTATOC. J. Nucl. Med. 2020, 61, 1014–1020. [Google Scholar] [CrossRef] [PubMed]
- Durmo, R.; Filice, A.; Fioroni, F.; Cervati, V.; Finocchiaro, D.; Coruzzi, C.; Besutti, G.; Fanello, S.; Frasoldati, A.; Versari, A. Predictive and Prognostic Role of Pre-Therapy and Interim 68Ga-DOTATOC PET/CT Parameters in Metastatic Advanced Neuroendocrine Tumor Patients Treated with PRRT. Cancers 2022, 14, 592. [Google Scholar] [CrossRef] [PubMed]
- Opalińska, M.; Morawiec-Sławek, K.; Kania-Kuc, A.; Al Maraih, I.; Sowa-Staszczak, A.; Hubalewska-Dydejczyk, A. Potential value of pre- and post-therapy [68Ga]Ga-DOTA-TATE PET/CT in the prognosis of response to PRRT in disseminated neuroendocrine tumors. Front. Endocrinol. 2022, 13, 929391. [Google Scholar] [CrossRef]
- Ohlendorf, F.; Henkenberens, C.; Brunkhorst, T.; Ross, T.L.; Christiansen, H.; Bengel, F.M.; Derlin, T. Volumetric 68Ga-DOTA-TATE PET/CT for assessment of whole-body tumor burden as a quantitative imaging biomarker in patients with metastatic gastroenteropancreatic neuroendocrine tumors. Q. J. Nucl. Med. Mol. Imaging 2020, 66, 361–371. [Google Scholar] [CrossRef] [PubMed]
- Evangelista, L.; Urso, L.; Caracciolo, M.; Stracuzzi, F.; Panareo, S.; Cistaro, A.; Catalano, O. FDG PET/CT Volume-Based Quantitative Data and Survival Analysis in Breast Cancer Patients: A Systematic Review of the Literature. Curr. Med. Imaging Former. Curr. Med. Imaging Rev. 2022, 18. [Google Scholar] [CrossRef]
- Jung, A.R.; Roh, J.L.; Kim, J.S.; Choi, S.H.; Nam, S.Y.; Kim, S.Y. Post-treatment 18F-FDG PET/CT for predicting survival and recurrence in patients with advanced-stage head and neck cancer undergoing curative surgery. Oral Oncol. 2020, 107, 104750. [Google Scholar] [CrossRef]
- Abdulrezzak, U.; Kurt, Y.K.; Kula, M.; Tutus, A. Combined imaging with 68Ga-DOTA-TATE and 18F-FDG PET/CT on the basis of volumetric parameters in neuroendocrine tumors. Nucl. Med. Commun. 2016, 37, 874–881. [Google Scholar] [CrossRef]
- Toriihara, A.; Baratto, L.; Nobashi, T.; Park, S.; Hatami, N.; Davidzon, G.; Kunz, P.L.; Iagaru, A. Prognostic value of somatostatin receptor expressing tumor volume calculated from 68Ga-DOTATATE PET/CT in patients with well-differentiated neuroendocrine tumors. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 2244–2251. [Google Scholar] [CrossRef]
- Wang, L.F.; Lin, L.; Wang, M.J.; Li, Y. The therapeutic efficacy of 177Lu-DOTATATE/DOTATOC in advanced neuroendocrine tumors: A meta-analysis. Medicine 2020, 99, e19304. [Google Scholar] [CrossRef]
- Bodei, L.; Kidd, M.S.; Singh, A.; van der Zwan, W.A.; Severi, S.; Drozdov, I.A.; Cwikla, J.; Baum, R.P.; Kwekkeboom, D.J.; Paganelli, G.; et al. PRRT genomic signature in blood for prediction of 177Lu-octreotate efficacy. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 1155–1169. [Google Scholar] [CrossRef] [PubMed]
- Hou, J.; Yang, Y.; Chen, N.; Chen, D.; Hu, S. Prognostic Value of Volume-Based Parameters Measured by SSTR PET/CT in Neuroendocrine Tumors: A Systematic Review and Meta-Analysis. Front. Med. 2021, 8, 771912. [Google Scholar] [CrossRef] [PubMed]
- Tirosh, A.; Papadakis, G.Z.; Millo, C.; Hammoud, D.; Sadowski, S.M.; Herscovitch, P.; Pacak, K.; Marx, S.J.; Yang, L.; Nockel, P.; et al. Prognostic Utility of Total 68Ga-DOTATATE-Avid Tumor Volume in Patients With Neuroendocrine Tumors. Gastroenterology 2018, 154, 998–1008.e1. [Google Scholar] [CrossRef] [PubMed]
- Thuillier, P.; Liberini, V.; Grimaldi, S.; Rampado, O.; Gallio, E.; De Santi, B.; Arvat, E.; Piovesan, A.; Filippi, R.; Abgral, R.; et al. Prognostic Value of Whole-Body PET Volumetric Parameters Extracted from 68Ga-DOTATOC PET/CT in Well-Differentiated Neuroendocrine Tumors. J. Nucl. Med. 2022, 63, 1014–1020. [Google Scholar] [CrossRef] [PubMed]
- Ezziddin, S.; Attassi, M.; Yong-Hing, C.J.; Ahmadzadehfar, H.; Willinek, W.; Grünwald, F.; Guhlke, S.; Biersack, H.J.; Sabet, A. Predictors of long-term outcome in patients with well-differentiated gastroenteropancreatic neuroendocrine tumors after peptide receptor radionuclide therapy with 177Lu-octreotate. J. Nucl. Med. 2014, 55, 183–190. [Google Scholar] [CrossRef]
- Gabriel, M.; Oberauer, A.; Dobrozemsky, G.; Decristoforo, C.; Putzer, D.; Kendler, D.; Uprimny, C.; Kovacs, P.; Bale, R.; Virgolini, I.J. 68Ga-DOTA-Tyr3-Octreotide PET for Assessing Response to Somatostatin-Receptor–Mediated Radionuclide Therapy. J. Nucl. Med. 2009, 50, 1427–1434. [Google Scholar] [CrossRef]
- Shi, H.; Jiang, C.; Zhang, Q.; Qi, C.; Yao, H.; Lin, R. Clinicopathological heterogeneity between primary and metastatic sites of gastroenteropancreatic neuroendocrine neoplasm. Diagn. Pathol. 2020, 15, 108. [Google Scholar] [CrossRef]
- Yang, Z.; Tang, L.H.; Klimstra, D.S. Effect of tumor heterogeneity on the assessment of Ki67 labeling index in well-differentiated neuroendocrine tumors metastatic to the liver: Implications for prognostic stratification. Am. J. Surg. Pathol. 2011, 35, 853–860. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients | Feature | N (%) | |
|---|---|---|---|
| Gender, n(%) | Male | 21 (53.8) | |
| Female | 18 (46.2) | ||
| Age, median | 60.7 [25–80 y] | ||
| Primary origin | Midgut | 7 (17.9) | |
| Pancreatic | 19 (48.7) | ||
| Cerebral | 1 (2.6) | ||
| Bronchial | 6 (15.4) | ||
| CUP | 5 (12.8) | ||
| Pheocromocytoma | 1 (2.6) | ||
| Grading (%) | Median 8% [1–40%] | G1 | 4 (19.3) |
| G2 | 31 (77.4) | ||
| G3 | 3 (3.3) | ||
| NET Syndrome | Functioning | 9 (23.1) | |
| Nonfunctioning | 30 (76.9) | ||
| PRRT Scheme | MONO | 23 (59) | |
| DUO | 16 (41) | ||
| Univariate Analysis | Multivariate Analysis | ||||||
|---|---|---|---|---|---|---|---|
| HR | 95% CI | p Value | HR | 95% CI | p Value | ||
| Progression-free survival (PFS) | |||||||
| Age | per year | 0.981 | 0.945–1.018 | 0.310 | |||
| Gender | Male vs. Female | 1.056 | 0.448–2.490 | 0.901 | |||
| Primary origin | Pancreas vs. others | 1.726 | 0.722–4.124 | 0.219 | |||
| NET syndrome | Functioning vs. nonfunctioning | 1.147 | 0.657–2.001 | 0.630 | |||
| Median Ki-67 | <8 vs. ≥8 | 2.418 | 1.051–6.148 | 0.064 | 0.223 | 0.192–1.468 | 0.223 |
| Grading | G1 vs. G2 vs. G3 | 3.020 | 0.289–31.51 | 0.356 | |||
| 0.378 | 0.060–2.387 | 0.301 | |||||
| 0.931 | 0.266–3.266 | 0.911 | |||||
| PRRT scheme | Mono vs. Duo | 0.962 | 0.630–1.470 | 0.858 | |||
| post-SRETV_WB | ≤34.8 vs. >34.8 | 0.452 | 0.187–1.092 | 0.078 | 0.422 | 0.164–1.092 | 0.075 |
| post-SRETV_L | ≤35.1 vs. >35.1 | 0.680 | 0.284–1.632 | 0.389 | |||
| ΔSRETV_WB | ≤−4.17 vs. >−4.17 | 0.275 | 0.102–0.744 | 0.011 | 0.295 | 0.107–0.817 | 0.019 |
| ΔSRETV_L | ≤20.1 vs. >20.1 | 0.770 | 0.324–1.830 | 0.554 | |||
| post-TLSRE_WB | ≤763.3 vs. >763.3 | 0.519 | 0.235–1.722 | 0.155 | |||
| post-TLSRE_L | ≤585.2 vs. >585.2 | 0.680 | 0.284–1.632 | 0.389 | |||
| ΔTLSRE_WB | ≤−2.38 vs. >−2.38 | 0.489 | 0.205–1.166 | 0.107 | |||
| ΔTLSRE_L | ≤12.6 vs. >12.6 | 0.489 | 0.205–1.166 | 0.630 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Urso, L.; Castello, A.; Treglia, G.; Panareo, S.; Nieri, A.; Rambaldi, I.; Caracciolo, M.; Ortolan, N.; Uccelli, L.; Cittanti, C.; et al. Relevance of Volumetric Parameters Applied to [68Ga]Ga-DOTATOC PET/CT in NET Patients Treated with PRRT. Diagnostics 2023, 13, 606. https://doi.org/10.3390/diagnostics13040606
Urso L, Castello A, Treglia G, Panareo S, Nieri A, Rambaldi I, Caracciolo M, Ortolan N, Uccelli L, Cittanti C, et al. Relevance of Volumetric Parameters Applied to [68Ga]Ga-DOTATOC PET/CT in NET Patients Treated with PRRT. Diagnostics. 2023; 13(4):606. https://doi.org/10.3390/diagnostics13040606
Chicago/Turabian StyleUrso, Luca, Angelo Castello, Giorgio Treglia, Stefano Panareo, Alberto Nieri, Ilaria Rambaldi, Matteo Caracciolo, Naima Ortolan, Licia Uccelli, Corrado Cittanti, and et al. 2023. "Relevance of Volumetric Parameters Applied to [68Ga]Ga-DOTATOC PET/CT in NET Patients Treated with PRRT" Diagnostics 13, no. 4: 606. https://doi.org/10.3390/diagnostics13040606