
MRI Findings in Axial Psoriatic Spondylarthritis

 , , ,
, , , 
Abstract
:1. Introduction
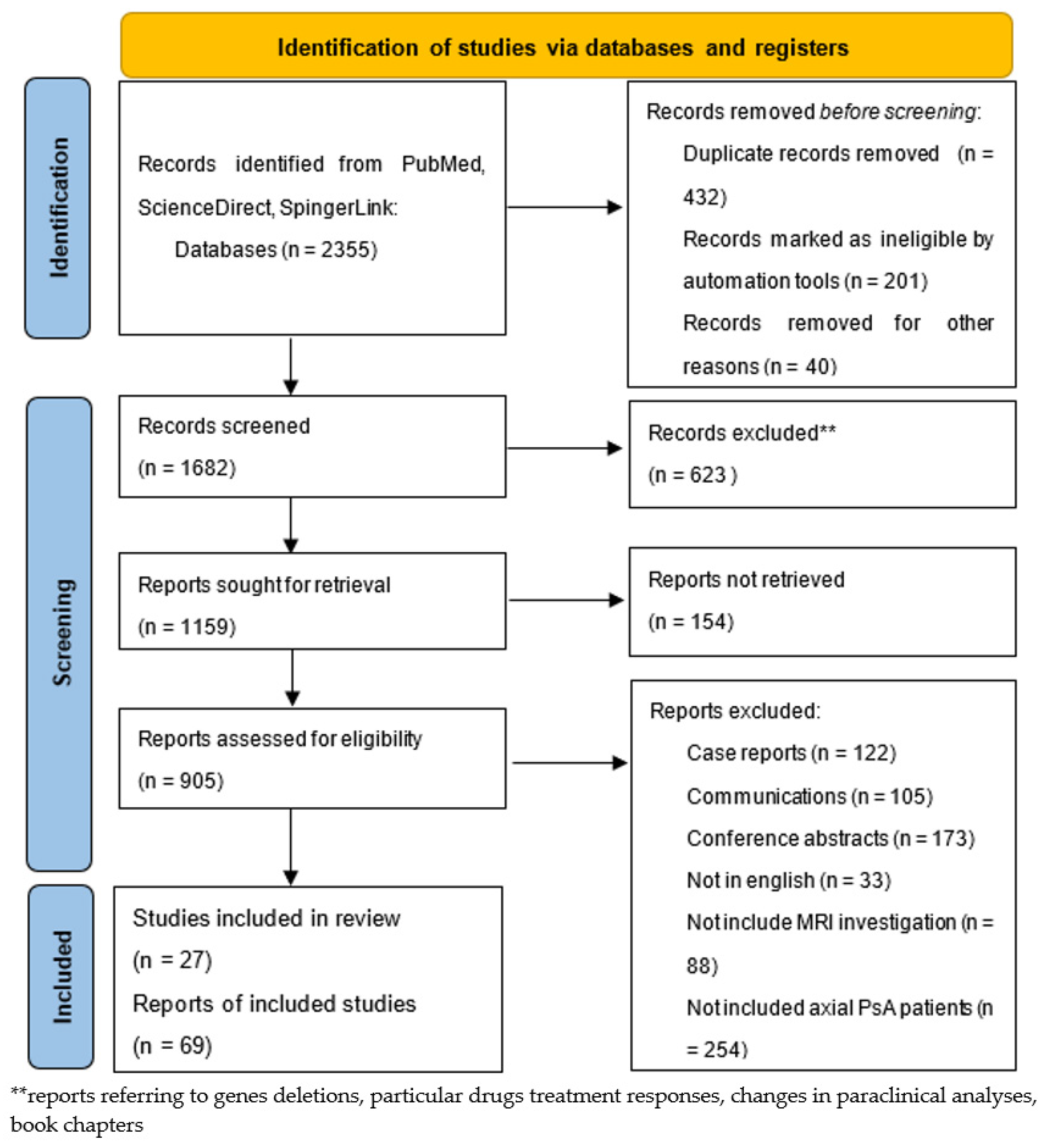
2. Materials and Methods
3. Results
3.1. Clinical Manifestations

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pain Features | IBP | MBP |
|---|---|---|
| Age | <40 yo | >50 yo |
| Onset | Insidious | Variable |
| Timing | During the night, can wake the patient. | Daytime |
| Improvement | With physical activity, no improvement at rest. | With rest, movement may worsen the pain. |
| Diagnosis | NO history of back injury or heavy work load; Alternating buttock pain; Favorable response to NSAIDs. | History of back injury or heavy work load; No or minimal response to NSAIDs *. |
| Duration | >3 months | <4 weeks; persisting pain needs additional tests and imaging (HLA-B27, acute phase reactants, MRI, clinical examination). |
| Location | Anywhere; the proximal/distal third or the posterior region are highly suggestive. | Anterior mid-third of sacroiliac joints, often bilateral. |
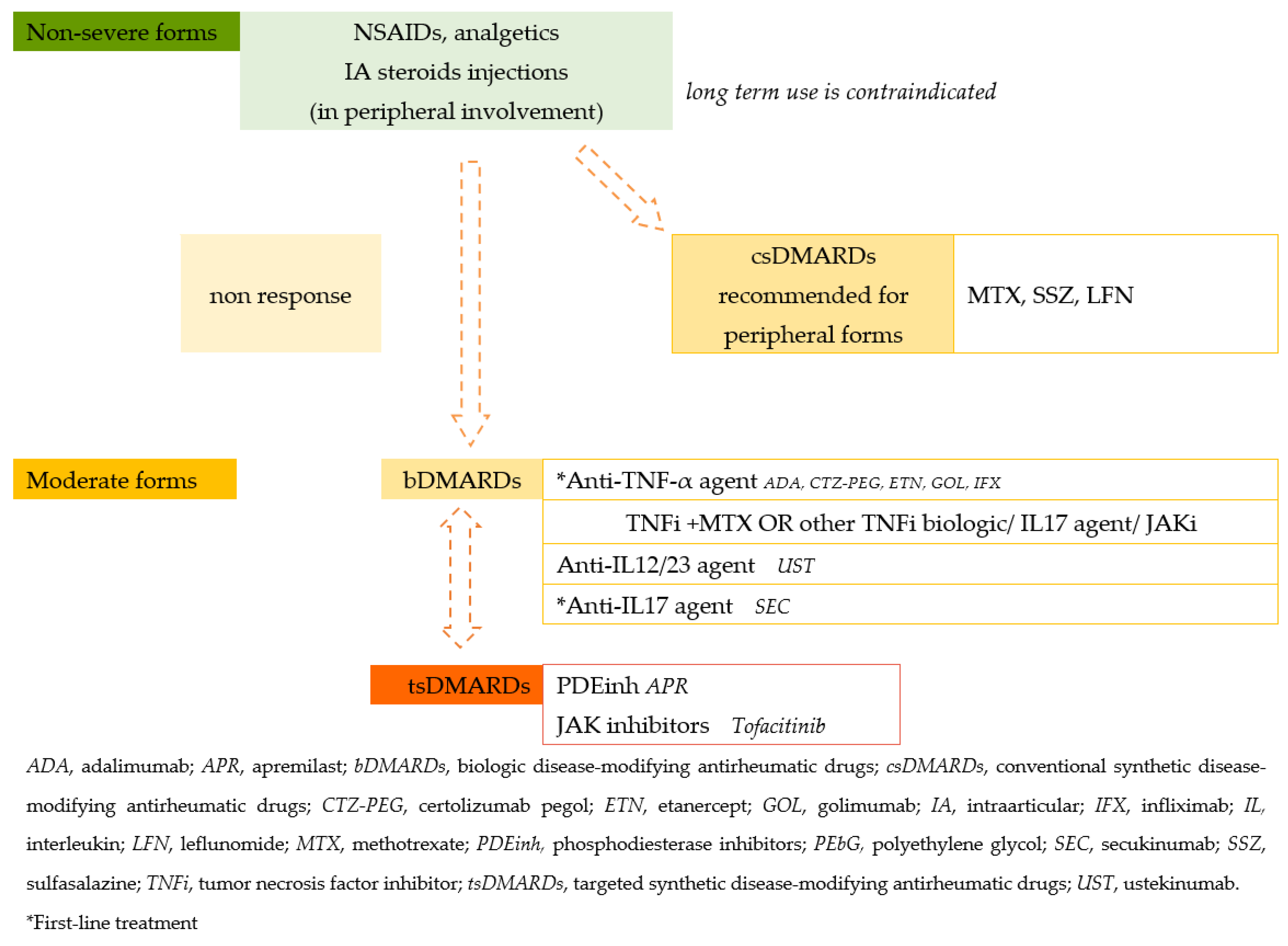
| Treatment | See Figure 2. | Physiotherapy, NSAIDs, corticosteroids, when necessary. |

- Systemic arthritis;
- Olygoarthritis (persistent/extended);
- Polyarthritis RF-negative;
- Polyarthritis RF-positive;
- Psoriatic arthritis;
- Enthesitis-related arthritis (ERA);
- Undifferentiated arthritis (UA).
3.2. Imaging Protocols
3.2.1. Axial PsA
- -
- Sagittal T1-weighted (T1w) sequences—best for the characterization of fat content or to assess structural bone lesions.
- -
- Sagittal T2-weighted Fat-Sat fast spin echo sequences and short tau inversion recovery (STIR) sequences (short tau inversion recovery) sequences in two planes for water content evaluation/BMO.
- -
- For a better assessment of the costovertebral and costotransverse joints and the facet joints, coronal sequences can be added to the protocol [58].
- -
- Sagittal T1w Fat-Sat sequences with gadolinium enhancement—used for the detection of osteitis; increased perfusion; rarely used, in cases of doubt and high suspicion, to differentiate exudate from synovitis or to assess the activity of bone erosions [59].
3.2.2. Sacroiliac Joints Sequences
- -
- T1-weighted axial oblique and semi-coronal sequences.
- -
- T1-weighted Fat-Sat (TIWFS) spin echo/T1 Dixon/3D gradient echo such as VIBE—for the better evaluation of erosions; VIBE sequences showed a better ability to detect cartilage erosions before extending to the underlying bone [60].
- -
- Axial oblique semi-coronal STIR and T2-weighted fat-suppressed (T2WFS) sequences (coronal plane tilted parallel to the long axis of the sacroiliac joint) with 4-mm slice thickness.
- -
- Apparent diffusion coefficient (ADC) map—STIR or T2WFS sequences may be substituted or supplemented for the better assessment of SIJ inflammation.
- -
- Coronal and axial oblique T1w Fat-Sat with gadolinium—detects osteitis; increased perfusion; recommended in cases of doubt and high suspicion; T1WFS pre- and postcontrast administration can differentiate active inflammation from a simple fluid.
3.3. MRI Findings
3.3.1. Vertebral Findings (Similar to Spa Findings)
- Inflammation of the vertebral body superior or inferior corners, identified in the early stages as a low signal in T1w, a high signal in T2w and STIR, due to bone marrow edema and later, a high signal in T1w and T2w due to fatty bone marrow degeneration, known as the “shiny corner sign” or “Romanus lesions” (Figure 3). This is also found in ankylosing spondylitis.
- Spondylodiscitis—inflammation of the whole vertebral end plate, involving the adjacent intervertebral disc (Andersson lesion) and soft tissue, identified on low signal T1w in both the intervertebral disc and adjacent end plates due to inflammation and bone marrow edema; on high signal T2w Fat-Sat and STIR in the disc space, adjacent endplates, and paravertebral soft tissue, also involving the psoas muscle, with the loss of the endplate cortex signal. Normally, muscle tissue has an intermediary signal in both T1w and T2w sequences, while inflammation leads to an increased signal in both sequences. A T1w-sequence with gadolinium shows enhancement of the vertebral endplates and paravertebral soft tissue and peripheral enhancement in the case of collections. DWI sequences distinguish the acute and chronic stages (high signal vs. low signal). It is described also as a complication in the evolution of advanced SpA, mostly in the lumbar spine [64,65].
- Facet joint inflammation—generated mostly by articular degeneration, usually associated with BME within the spinal pedicles, and common in most arthropathies.
- Inflammation of the posterior and lateral elements—including the costovertebral joints, transverse and spinous processes, and the adjacent soft tissue
- Bone erosion—best visualized on T1-weighted sequences as cortical (dark appearance) bone defects, contour irregularities, and the loss of the normal bright appearance of the adjacent bone marrow.
- Bulky new bone formation—bone productions in high signal T1w; marginal and paramarginal vertical syndesmophytes distributed asymmetrically along the spine, with a peculiar feature of late PsA, while in SpA, syndesmophytes are typically bilateral and symmetrical, with only a marginal distribution and evolution from caudal to cranial [66]. In axial PsA, syndesmophytes extend towards the adjacent vertebra, while in AS, they are continuous from adjacent vertebra, with a tendency to the formation of osteophytic bridges and further evolution to the bamboo spine [67]. The vertebral joint spaces are preserved until the late stages of the disease.
- Enthesitis—involving the supraspinal ligament, interspinal ligaments, and ligamentum flavum; normally, tendons have a homogenous low signal in all sequences [65].
3.3.2. Sacroiliac Joints Findings
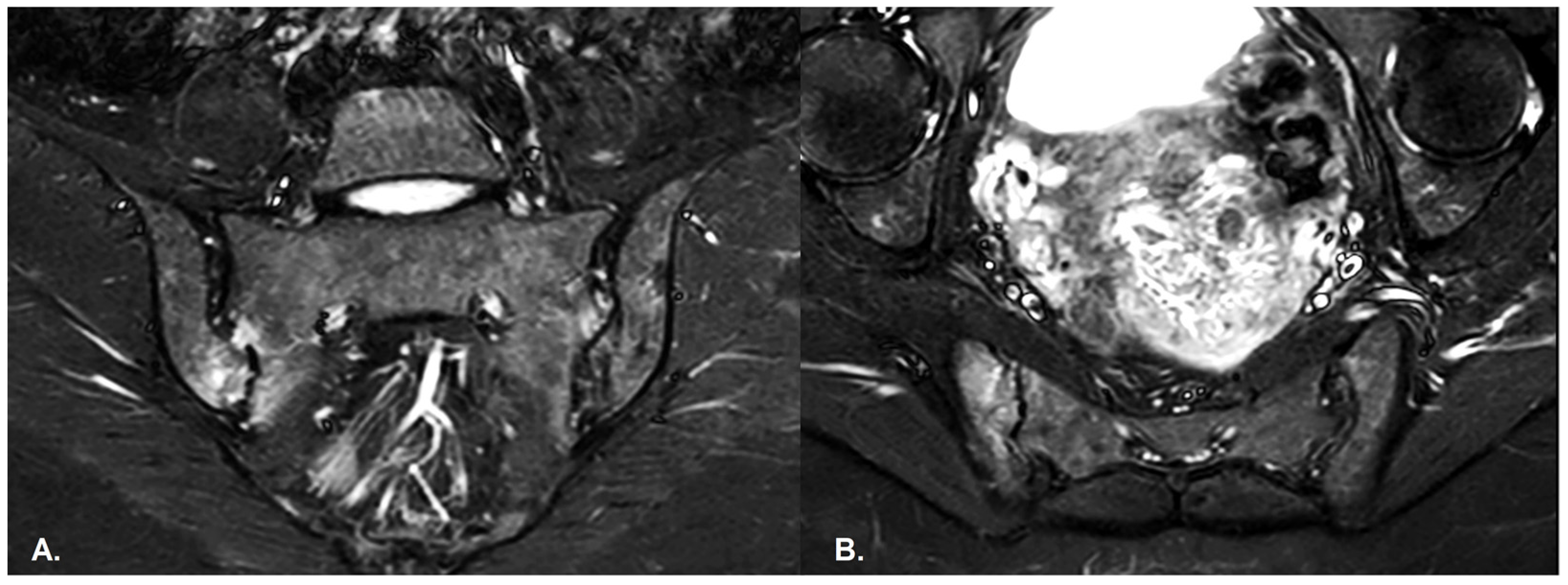
- BME is evident in low signal T1w, hyper signal T2w, STIR images and +C T1w Fat-Sat, similar to blood vessels and spinal fluid; the signal intensity is directly proportional to the inflammation activity. It is usually located periarticular to or on the subchondral bone surfaces and it is an indicator of disease activity (Figure 4) [65].
- Capsular inflammation—increased signal on T2w GRE and STIR sequences.
- Enthesitis—entheses are normally seen as hypointense structures, whereas inflammation leads to an increase in signal; best visualized on T2w Fat-Sat and STIR sequences. There are similar findings in both PsA and SpA [65].
- Joint space fluid.
- Joint space enhancement.
- Erosions–initially focal, later they will converge and will have a pseudo-enlargement aspect of the sacroiliac joint. In T1w images there is a loss of cortical bone signal (normally hypointense) and bone marrow fat (normally hyperintense).
- Inflammation at the site of erosion.
- Fat metaplasia in an erosion cavity or ‘backfill’ [65].
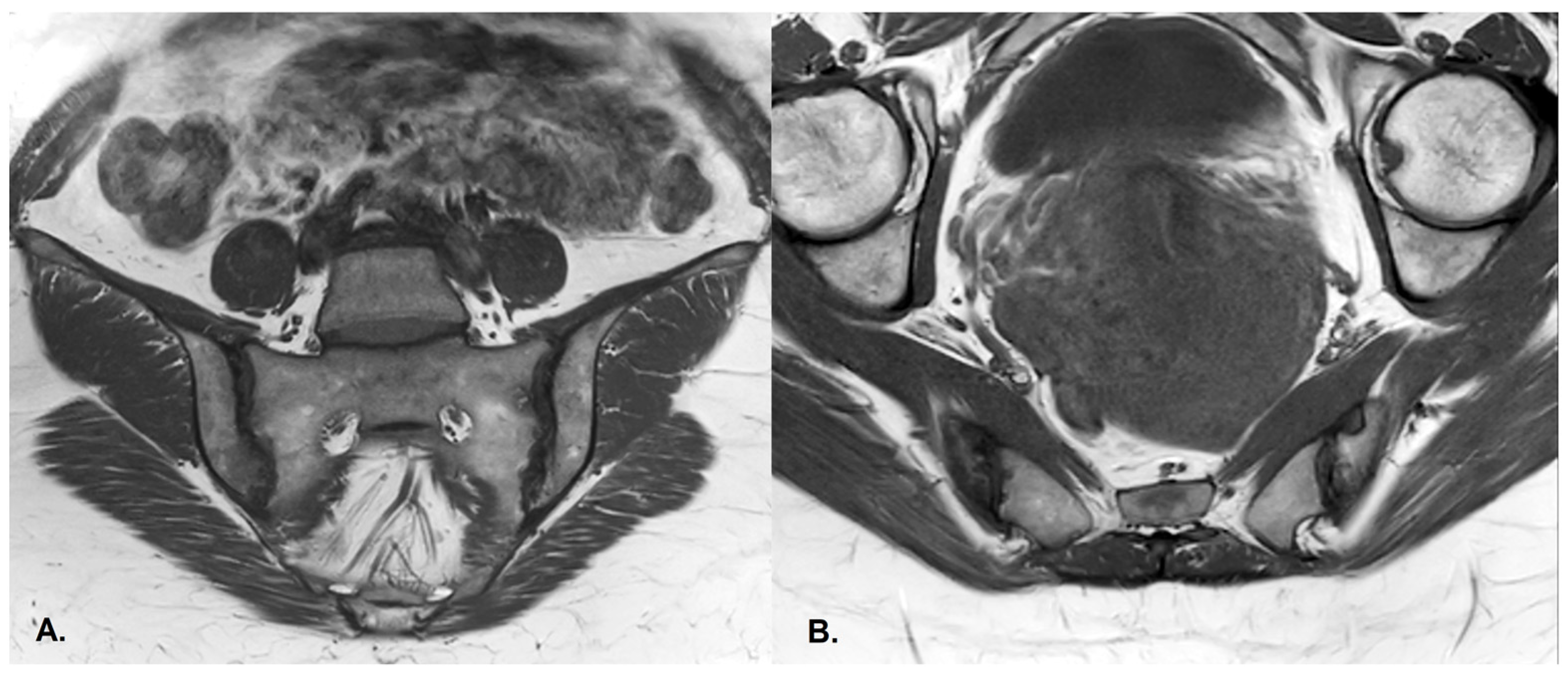
- Sclerosis—better visualized on an X-ray or CT scan; a subchondral or periarticular area with a low signal compared to normal bone marrow on T1, T1FS (SPIR), and STIR sequences (Figure 5).Slight: <25% of the subcortical bone area.Moderate: 25% to <50% of the subcortical bone area.Severe: >50% of the subcortical bone area [29].
- Ankylosis [65]Partial: Partial osseous bridging across the joint space.Total: Fusion of the joint facets [29].
- -
- DWI has the advantage of not necessitating gadolinium administration and is helpful in the early detection of spinal cord damage. ADC discriminates between active-inactive juvenile inflammatory arthritis, a better diagnosis of SpA, and mechanical versus inflammatory back pain.
- -
- CSE-MRI helps detect active inflammation and structural damage.
- -
- DCE-MRI is useful in the evaluation of inflammation activity, detecting early disease from periarticular soft tissue inflammation, even in the absence of synovitis [81]. It is also helpful in distinguishing synovitis between RA and PsA.
- -
- T2- and T1p-mapping—providing insight into early biochemical cartilage changes and evidence of atlantoaxial instability, and does not require contrast agent administration.
- -
- DGEMRIC (delayed gadolinium-enhanced MRI of cartilage)—recommended for peripheral disease; useful in uncovering early biochemical cartilage disturbances; requires long acquisition protocols.
3.3.3. Specific Features of Juvenile Psoriatic Arthritis [88]
- -
- Early disease—periarticular osteopenia, effusion, juxta-synovial soft-tissue swelling;
- -
- Intermediate disease—narrowing of the spaces between joints, cortical erosions, epiphyseal overgrowth;
- -
- Late disease—ankylosis, joint angular deformities, contractures, muscle atrophy.
- 1.
- The 2–5 years age group displays the phenotypic and pathophysiological features of common autoimmune diseases, including:
- -
- Female predominance, positive anti-nuclear antibodies (ANA), higher predisposition of chronic uveitis.
- -
- Similar features to oligo- and polyarticular JIA or early-onset ANA-positive JIA.
- -
- Arthritis, often involving the knee and ankle; the involvement of dactylitis and distal interphalangeal joints is highly suggestive of jPsA. Dactylitis is present in 20–40% of patients and is the first musculoskeletal finding at presentation in about 15% of cases; moreover, it has been observed a long time before skin psoriasis [70].
- -
- Higher incidence of small joint and wrist involvement.
- -
- 2.
- The 9–12 years age group have features of autoinflammation that emerge as enthesopathy, including:
- -
- Relative equal sex distribution, with a little male predisposition;
- -
- Resembles adult PsA features;
- -
- Enthesitis in up to 60% of patients [91];
- -
- Axial involvement, sacroiliitis;
- -
- HLA-B27 positivity, but some of these cases will be diagnosed as ERA or UA by the ILAR criteria.
- -
- Systemic JIA corresponds to adult-onset Still’s disease;
- -
- RF-positive polyarticular JIA is equivalent to RF-positive RA;
- -
- ERA has adult-equivalent undifferentiated SpA.
3.4. Other Diagnostic Tools
3.5. Pharmacological Therapy
3.5.1. Treatment Recommendations and Responses
3.5.2. DMARDs Side Effects
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zeidler, H.K. Psoriatic Spondylitis: A Disease Manifestation in Debate: Evidences to Know for the Clinical Rheumatologist. J. Clin. Rheumatol. 2022, 28, 38–43. [Google Scholar] [CrossRef]
- Crespo-Rodríguez, A.M.; Sanz Sanz, J.; Freites, D.; Rosales, Z.; Abasolo, L.; Arrazola, J. Role of Diagnostic Imaging in Psoriatic Arthritis: How, When, and Why. Insights Imaging 2021, 12, 121. [Google Scholar] [CrossRef]
- Alinaghi, F.; Calov, M.; Kristensen, L.E.; Gladman, D.D.; Coates, L.C.; Jullien, D.; Gottlieb, A.B.; Gisondi, P.; Wu, J.J.; Thyssen, J.P.; et al. Prevalence of Psoriatic Arthritis in Patients with Psoriasis: A Systematic Review and Meta-Analysis of Observational and Clinical Studies. J. Am. Acad. Dermatol. 2019, 80, 251–265.e19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopez-Medina, C.; Ziade, N. Axial Disease in Psoriatic Arthritis: How Can We Define It, and Does It Have an Impact on Treatment? Mediterr. J. Rheumatol. 2022, 33, 142–149. [Google Scholar] [CrossRef] [PubMed]
- Helliwell, P.S.; Helliwell, P.S. Axial Disease in Psoriatic Arthritis. Rheumatology (UK) 2020, 59, 1193–1195. [Google Scholar] [CrossRef] [Green Version]
- Gubar, E.E.; Loginova, E.Y.; Korotaeva, T.V.; Glukhova, S.I.; Nasonov, E.L. Comparative Characteristics of Early Psoriatic Arthritis with and without Axial Skeleton Injury (a Subanalysis of the All-Russian Registry of Patients with Psoriatic Arthritis). Rheumatol. Sci. Pract. 2019, 57, 636–641. [Google Scholar] [CrossRef]
- Feld, J.; Chandran, V.; Haroon, N.; Inman, R.; Gladman, D. Axial Disease in Psoriatic Arthritis and Ankylosing Spondylitis: A Critical Comparison. Nat. Rev. Rheumatol. 2018, 14, 363–371. [Google Scholar] [CrossRef]
- Sankowski, A.J.; Łebkowska, U.M.; Ćwikła, J.; Walecka, I.; Walecki, J. Psoriatic Arthritis. Pol. J. Radiol. 2013, 78, 7–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christophers, E.; Barker, J.; Griffiths, C.; Daudén, E.; Milligan, G.; Molta, C.; Sato, R.; Boggs, R. The Risk of Psoriatic Arthritis Remains Constant Following Initial Diagnosis of Psoriasis among Patients Seen in European Dermatology Clinics. J. Eur. Acad. Dermatol. Venereol. 2010, 24, 548–554. [Google Scholar] [CrossRef] [PubMed]
- Brunello, F.; Tirelli, F.; Pegoraro, L.; Dell’Apa, F.; Alfisi, A.; Calzamatta, G.; Folisi, C.; Zulian, F. New Insights on Juvenile Psoriatic Arthritis. Front. Pediatr. 2022, 10, 884727. [Google Scholar] [CrossRef]
- Brandon, T.G.; Manos, C.K.; Xiao, R.; Ogdie, A.; Weiss, P.F. Pediatric Psoriatic Arthritis: A Population-Based Cohort Study of Risk Factors for Onset and Subsequent Risk of Inflammatory Comorbidities. J. Psoriasis Psoriatic Arthritis 2018, 3, 131–136. [Google Scholar] [CrossRef]
- Carvalho, A.L.; Hedrich, C.M. The Molecular Pathophysiology of Psoriatic Arthritis—The Complex Interplay Between Genetic Predisposition, Epigenetics Factors, and the Microbiome. Front. Mol. Biosci. 2021, 8, 662047. [Google Scholar] [CrossRef] [PubMed]
- Kiil, R.M.; Mistegaard, C.E.; Loft, A.G.; Zejden, A.; Hendricks, O.; Jurik, A.G. Differences in Topographical Location of Sacroiliac Joint MRI Lesions in Patients with Early Axial Spondyloarthritis and Mechanical Back Pain. Arthritis Res. Ther. 2022, 24, 75. [Google Scholar] [CrossRef]
- Maksymowych, W.P.; Østergaard, M. Magnetic Resonance Imaging of Axial and Peripheral Disease in Psoriatic Arthritis: A Report From the 2020 GRAPPA Annual Meeting. J. Rheumatol. 2021, 97, 50–54. [Google Scholar] [CrossRef] [PubMed]
- Giovannini, I.; Zabotti, A.; Cicciò, C.; Salgarello, M.; Cereser, L.; de Vita, S.; Tinazzi, I. Clinical Medicine Axial Psoriatic Disease: Clinical and Imaging Assessment of an Underdiagnosed Condition. J. Clin. Med. 2021, 10, 2845. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, A.B.; Bakewell, C.; Merola, J.F. Musculoskeletal Imaging for Dermatologists: Techniques in the Diagnosis and Management of Psoriatic Arthritis. Dermatol. Ther. (Heidelb.) 2021, 11, 1199–1216. [Google Scholar] [CrossRef]
- Braga, M.V.; de Oliveira, S.C.; Vasconcelos, A.H.C.; Lopes, J.R.; de Macedo Filho, C.L.; Ramos, L.M.A.; Rodrigues, C.E.M. Prevalence of Sacroiliitis and Acute and Structural Changes on MRI in Patients with Psoriatic Arthritis. Sci. Rep. 2020, 10, 11580. [Google Scholar] [CrossRef]
- Benavent, D.; Plasencia, C.; Poddubnyy, D.; Kishimoto, M.; Proft, F.; Sawada, H.; López-Medina, C.; Dougados, M.; Navarro-Compán, V. Unveiling Axial Involvement in Psoriatic Arthritis: An Ancillary Analysis of the ASAS-PerSpA Study. Semin. Arthritis. Rheum. 2021, 51, 766–774. [Google Scholar] [CrossRef]
- Feld, J.; Ye, J.Y.; Chandran, V.; Inman, R.D.; Haroon, N.; Cook, R.; Gladman, D.D. Axial Disease in Psoriatic Arthritis: The Presence and Progression of Unilateral Grade 2 Sacroiliitis in a Psoriatic Arthritis Cohort. Semin. Arthritis. Rheum 2021, 51, 464–468. [Google Scholar] [CrossRef]
- Furer, V.; Levartovsky, D.; Wollman, J.; Wigler, I.; Paran, D.; Kaufman, I.; Elalouf, O.; Borok, S.; Anouk, M.; Maman, H.S.; et al. Prevalence of Nonradiographic Sacroiliitis in Patients with Psoriatic Arthritis: A Real-Life Observational Study. J. Rheumatol. 2021, 48, 1014–1021. [Google Scholar] [CrossRef]
- Diaz, P.; Feld, J.; Eshed, I.; Eder, L. Characterising Axial Psoriatic Arthritis: Correlation between Whole Spine MRI Abnormalities and Clinical, Laboratory and Radiographic Findings. RMD Open 2022, 8, e002011. [Google Scholar] [CrossRef] [PubMed]
- Castillo-Gallego, C.; Aydin, S.Z.; Emery, P.; McGonagle, D.G.; Marzo-Ortega, H. Magnetic Resonance Imaging Assessment of Axial Psoriatic Arthritis: Extent of Disease Relates to HLA-B27. Arthritis Rheum. 2013, 65, 2274–2278. [Google Scholar] [CrossRef] [PubMed]
- Ye, L.; Liu, Y.; Xiao, Q.; Dong, L.; Wen, C.; Zhang, Z.; Jin, M.; Brown, M.A.; Chen, D. MRI Compared with Low-Dose CT Scanning in the Diagnosis of Axial Spondyloarthritis. Clin. Rheumatol. 2020, 39, 1295–1303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poggenborg, R.P.; Pedersen, S.J.; Eshed, I.; Sørensen, I.J.; Møller, J.M.; Madsen, O.R.; Thomsen, H.S.; Østergaard, M. Head-to-Toe Whole-Body MRI in Psoriatic Arthritis, Axial Spondyloarthritis and Healthy Subjects: First Steps towards Global Inflammation and Damage Scores of Peripheral and Axial Joints. Rheumatology (UK) 2015, 54, 1039–1049. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jadon, D.R.; Sengupta, R.; Nightingale, A.; Lindsay, M.; Korendowych, E.; Robinson, G.; Jobling, A.; Shaddick, G.; Bi, J.; Winchester, R.; et al. Axial Disease in Psoriatic Arthritis Study: Defining the Clinical and Radiographic Phenotype of Psoriatic Spondyloarthritis. Ann. Rheum. Dis. 2017, 76, 701–707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gensler, L.; Szumski, A.; Jones, H.; Baraliakos, X.; Gensler, L.S.; Szumski, A.; Heather Jones, M.E.; Xenofon Baraliakos, R. Does Psoriatic Axial Spondyloarthritis Phenotype Correlate with Imaging Morphotype? Clin. Exp. Rheumatol. 2020, 38, 329–332. [Google Scholar] [CrossRef]
- Salinas, R.G.; Prado, E.S.; Ruta, S. Axial Involvement in Psoriatic Arthritis: Effect on Peripheral Arthritis and Differential Features with Axial Spondyloarthritis in South America. J. Rheumatol. 2021, 48, 1346–1348. [Google Scholar] [CrossRef]
- Abdelaziz, M.M.; Ismail, N.; Gamal, A.M.; Lafy, R.; El-Adly, W. Comparative Analysis between Ankylosing Spondylitis and Axial Psoriatic Arthritis Patients. Egypt. Rheumatol. 2022, 44, 25–29. [Google Scholar] [CrossRef]
- Arnbak, B.; Jensen, T.S.; Egund, N.; Zejden, A.; Hørslev-Petersen, K.; Manniche, C.; Jurik, A.G. Prevalence of Degenerative and Spondyloarthritis-Related Magnetic Resonance Imaging Findings in the Spine and Sacroiliac Joints in Patients with Persistent Low Back Pain. Eur. Radiol. 2016, 26, 1191–1203. [Google Scholar] [CrossRef]
- Yap, K.S.; Ye, J.Y.; Li, S.; Gladman, D.D.; Chandran, V. Back Pain in Psoriatic Arthritis: Defining Prevalence, Characteristics and Performance of Inflammatory Back Pain Criteria in Psoriatic Arthritis. Ann. Rheum. Dis. 2018, 77, 1573–1577. [Google Scholar] [CrossRef]
- Aydin, S.Z.; Kilic, L.; Kucuksahin, O.; Ureyen, S.B.; Kalyoncu, U. Performances of Inflammatory Back Pain Criteria in Axial Psoriatic Arthritis. Rheumatology (Oxford) 2017, 56, 2031–2032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kivity, S.; Gofrit, S.G.; Baker, F.A.; Leibushor, N.; Tavor, S.; Lidar, M.; Eshed, I. Association between Inflammatory Back Pain Features, Acute and Structural Sacroiliitis on MRI, and the Diagnosis of Spondyloarthritis. Clin. Rheumatol. 2019, 38, 1579–1585. [Google Scholar] [CrossRef] [PubMed]
- Zisman, D.; Gladman, D.D.; Stoll, M.L.; Strand, V.; Lavi, I.; Hsu, J.J.; Mellins, E.D. The Juvenile Psoriatic Arthritis Cohort in the CARRA Registry: Clinical Characteristics, Classification, and Outcomes. J. Rheumatol. 2017, 44, 342–351. [Google Scholar] [CrossRef]
- Ekelund, M.; Aalto, K.; Fasth, A.; Herlin, T.; Nielsen, S.; Nordal, E.; Peltoniemi, S.; Rygg, M.; Zak, M.; Berntson, L. Psoriasis and Associated Variables in Classification and Outcome of Juvenile Idiopathic Arthritis—An Eight-Year Follow-up Study. Pediatr. Rheumatol. 2017, 15, 13. [Google Scholar] [CrossRef] [Green Version]
- Lamot, L.; Miler, M.; Vukojević, R.; Vidović, M.; Lamot, M.; Trutin, I.; Gabaj, N.N.; Harjaček, M. The Increased Levels of Fecal Calprotectin in Children With Active Enthesitis Related Arthritis and MRI Signs of Sacroiliitis: The Results of a Single Center Cross-Sectional Exploratory Study in Juvenile Idiopathic Arthritis Patients. Front. Med. (Lausanne) 2021, 8, 650619. [Google Scholar] [CrossRef]
- Jawad, I.I.; Nisar, M.K. How Well Are Biologic and Conventional DMARDs Tolerated in Psoriatic Arthritis: A Real World Study. Eur. J. Rheumatol. 2022, 9, 100–103. [Google Scholar] [CrossRef] [PubMed]
- Grinnell-Merrick, L.L.; Lydon, E.J.; Mixon, A.M.; Saalfeld, W. Evaluating Inflammatory Versus Mechanical Back Pain in Individuals with Psoriatic Arthritis: A Review of the Literature. Rheumatol. Ther. 2020, 7, 667–684. [Google Scholar] [CrossRef]
- Poddubnyy, D.; Jadon, D.R.; Van den Bosch, F.; Mease, P.J.; Gladman, D.D. Axial Involvement in Psoriatic Arthritis: An Update for Rheumatologists. Semin. Arthritis Rheum 2021, 51, 880–887. [Google Scholar] [CrossRef]
- Akgul, O.; Ozgocmen, S. Classification Criteria for Spondyloarthropathies. World J. Orthop. 2011, 2, 107–115. [Google Scholar] [CrossRef]
- D’Angelo, S.; Palazzi, C.; Gilio, M.; Leccese, P.; Padula, A.; Olivieri, I. Improvements in Diagnostic Tools for Early Detection of Psoriatic Arthritis. Expert Rev. Clin. Immunol. 2016, 12, 1209–1215. [Google Scholar] [CrossRef]
- Poddubnyy, D.; Baraliakos, X.; van den Bosch, F.; Braun, J.; Coates, L.C.; Chandran, V.; Diekhoff, T.; van Gaalen, F.A.; Gensler, L.S.; Goel, N.; et al. Axial Involvement in Psoriatic Arthritis Cohort (AXIS): The Protocol of a Joint Project of the Assessment of SpondyloArthritis International Society (ASAS) and the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA). Ther. Adv. Musculoskelet. Dis. 2021, 13, 1759720X211057975. [Google Scholar] [CrossRef]
- Gubar, E.; Korotaeva, T.; Loginova, E.; Korsakova, Y.; Glukhova, S. Pos0310 do axial psoriatic arthritis patients meet asas classification criteria for axial spondyloarthritis? Ann. Rheum. Dis. 2022, 81, 405. [Google Scholar] [CrossRef]
- Poddubnyy, D. Classification vs Diagnostic Criteria: The Challenge of Diagnosing Axial Spondyloarthritis. Rheumatology (UK) 2020, 59, IV6–IV17. [Google Scholar] [CrossRef]
- Wallman, J.; Alenius, G.-M.; Klingberg, E.; Sigurdardottir, V.; Wedrén, S.; Exarchou, S.; Lindström, U.; di Giuseppe, D.; Askling, J.; Jacobsson, L. Validity of Clinical Psoriatic Arthritis Diagnoses Made by Rheumatologists in the Swedish National Patient Register. Scand. J. Rheumatol. 2022, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Nas, K.; Karkucak, M.; Durmuş, B.; Ulu, M.A.; Karatay, S.; Çapkin, E.; Ulusoy, H.; Gülkesen, A.; Sula, B.; Akgöl, G.; et al. The Performance of Psoriatic Arthritis Classification Criteria in Turkish Patients with Psoriatic Arthritis. Int. J. Rheum. Dis. 2017, 20, 985–989. [Google Scholar] [CrossRef] [PubMed]
- Carneiro, S.; Palominos, P.E.; Anti, S.M.A.; Assad, R.L.; Gonçalves, R.S.G.; Chiereghin, A.; Lyrio, A.M.; Ximenes, A.C.; Saad, C.G.; Gonçalves, C.R.; et al. Brazilian Society of Rheumatology 2020 Guidelines for Psoriatic Arthritis. Adv. Rheumatol. 2021, 61, 69. [Google Scholar] [CrossRef]
- Petty, R.E.; Southwood, T.R.; Manners, P.; Glass, D.N.; Goldenberg, J.; He, X.; Maldonado-Cocco, J.; Orozco-Alcala, J.; Prieur, A.-M. International League of Associations for Rheumatology Classification of Juvenile Idiopathic Arthritis: Second Revision, Edmonton, 2001. J. Rheumatol. 2004, 31, 390–392. [Google Scholar]
- Gottlieb, A.B.; Wells, A.F.; Merola, J.F. Telemedicine and Psoriatic Arthritis: Best Practices and Considerations for Dermatologists and Rheumatologists. Clin. Rheumatol. 2022, 41, 1271–1283. [Google Scholar] [CrossRef] [PubMed]
- Novelli, L.; Motta, F.; Ceribelli, A.; Guidelli, G.M.; Luciano, N.; Isailovic, N.; Vecellio, M.; Caprioli, M.; Clementi, N.; Clementi, M.; et al. A Case of Psoriatic Arthritis Triggered by SARS-CoV-2 Infection. Rheumatology (UK) 2021, 60, E21–E23. [Google Scholar] [CrossRef]
- Colatutto, D.; Sonaglia, A.; Zabotti, A.; Cereser, L.; Girometti, R.; Quartuccio, L. Post-Covid-19 Arthritis and Sacroiliitis: Natural History with Longitudinal Magnetic Resonance Imaging Study in Two Cases and Review of the Literature. Viruses 2021, 13, 1558. [Google Scholar] [CrossRef]
- Bardazzi, F.; Sacchelli, L.; Loi, C.; Filippi, F.; Guglielmo, A. Reply to “Dermatoses Caused by Face Mask Wearing during the COVID-19 Pandemic”. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e425–e427. [Google Scholar] [CrossRef]
- Fassio, A.; Matzneller, P.; Idolazzi, L. Recent Advances in Imaging for Diagnosis, Monitoring, and Prognosis of Psoriatic Arthritis. Front. Med. (Lausanne) 2020, 7, 551684. [Google Scholar] [CrossRef]
- Galluzzo, E.; Lischi, D.M.; Taglione, E.; Lombardini, F.; Pasero, G.; Perri, G.; Riente, L. Sonographic Analysis of the Ankle in Patients with Psoriatic Arthritis. Scand J. Rheumatol. 2000, 29, 52–55. [Google Scholar] [PubMed]
- Wiell, C.; Szkudlarek, M.; Hasselquist, M.; Møller, J.M.; Vestergaard, A.; Nørregaard, J.; Terslev, L.; Østergaard, M. Ultrasonography, Magnetic Resonance Imaging, Radiography, and Clinical Assessment of Inflammatory and Destructive Changes in Fingers and Toes of Patients with Psoriatic Arthritis. Arthritis Res. Ther. 2007, 9, R119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milosavljevic, J.; Lindqvist, U.; Elvin, A. Ultrasound and Power Doppler Evaluation of the Hand and Wrist in Patients with Psoriatic Arthritis. Acta. Radiol. 2005, 46, 374–385. [Google Scholar] [CrossRef] [PubMed]
- Poggenborg, R.P.; Terslev, L.; Pedersen, S.J.; Østergaard, M. Recent Advances in Imaging in Psoriatic Arthritis. Ther. Adv. Musculoskelet. Dis. 2011, 3, 43–53. [Google Scholar] [CrossRef] [Green Version]
- Mathew, A.J.; Østergaard, M.; Eder, L. Imaging in Psoriatic Arthritis: Status and Recent Advances. Best Pract. Res. Clin. Rheumatol. 2021, 35, 101690. [Google Scholar] [CrossRef] [PubMed]
- Sieper, J.; Rudwaleit, M.; Baraliakos, X.; Brandt, J.; Braun, J.; Burgos-Vargas, R.; Dougados, M.; Hermann, K.G.; Landewe, R.; Maksymowych, W.; et al. The Assessment of SpondyloArthritis International Society (ASAS) Handbook: A Guide to Assess Spondyloarthritis. Ann. Rheum. Dis. 2009, 68, ii1–ii44. [Google Scholar] [CrossRef]
- Sudoł-Szopinska, I.; Urbanik, A. Diagnostic Imaging of Sacroiliac Joints and the Spine in the Course of Spondyloarthropathies. Pol. J. Radiol. 2013, 78, 43–49. [Google Scholar] [CrossRef] [Green Version]
- Baraliakos, X.; Hoffmann, F.; Deng, X.; Wang, Y.Y.; Huang, F.; Braun, J. Detection of Erosions in Sacroiliac Joints of Patients with Axial Spondyloarthritis Using the Magnetic Resonance Imaging Volumetric Interpolated Breath-Hold Examination. J. Rheumatol. 2019, 46, 1445–1449. [Google Scholar] [CrossRef]
- Lukas, C.; Braun, J.; van der Heijde, D.; Hermann, K.-G.A.; Rudwaleit, M.; Østergaard, M.; Oostveen, A.; O’connor, P.; Maksymowych, W.P.; Lambert, R.G.W.; et al. Scoring Inflammatory Activity of the Spine ByMagnetic Resonance Imaging in AnkylosingSpondylitis: A Multireader Experiment. J. Rheumatol. 2007, 34, 862–870. [Google Scholar] [PubMed]
- Her, M.; Kavanaugh, A. A Review of Disease Activity Measures for Psoriatic Arthritis: What Is the Best Approach? Expert Rev. Clin. Immunol. 2014, 10, 1241–1254. [Google Scholar] [CrossRef] [PubMed]
- Krabbe, S.; Østergaard, M.; Pedersen, S.J.; Weber, U.; Kröber, G.; Makysmowych, W.; Lambert, R.G.W. Canada-Denmark MRI Scoring System of the Spine in Patients with Axial Spondyloarthritis: Updated Definitions, Scoring Rules and Inter-Reader Reliability in a Multiple Reader Setting. RMD Open. 2019, 5, e001057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waldburger, M. Forme Particulière de Spondylarthrite Ankylosante Avec Spondylodiscite. Rev. Med. Suisse. 2005, 9, 1646. [Google Scholar]
- Canella, C.; Schau, B.; Ribeiro, E.; Sbaffi, B.; Marchiori, E. MRI in Seronegative Spondyloarthritis: Imaging Features and Differential Diagnosis in the Spine and Sacroiliac Joints. Am. J. Roentgenol. 2013, 200, 149–157. [Google Scholar] [CrossRef] [PubMed]
- Caso, F.; Costa, L.; Peluso, R.; Del Puente, A.; Scarpa, R. Psoriatic Arthritis. In Mosaic of Autoimmunity: The Novel Factors of Autoimmune Diseases; Elsevier: Amsterdam, The Netherlands, 2019; pp. 527–540. ISBN 9780128143087. [Google Scholar]
- Poggenborg, R.P.; Glinatsi, D.; Østergaard, M. Magnetic Resonance Imaging in Psoriatic Arthritis. In Psoriatic Arthritis and Psoriasis: Pathology and Clinical Aspects; Springer International Publishing: Berlin/Heidelberg, Germany, 2016; pp. 199–208. ISBN 9783319195308. [Google Scholar]
- Sudoł-Szopińska, I.; Giraudo, C.; Oei, E.H.G.; Jans, L. Imaging Update in Inflammatory Arthritis. J. Clin. Orthop. Trauma. 2021, 20, 101491. [Google Scholar] [CrossRef] [PubMed]
- Gazel, U.; Ayan, G.; Solmaz, D.; Bakirci, S.; Karsh, J.; Sampaio, M.; Jibri, Z.; Aydin, S.Z. Limited Added Value of Whole Spine MRI in Spondyloarthritis for Disease Activity Assessment. Clin. Rheumatol. 2021, 40, 4909–4913. [Google Scholar] [CrossRef]
- Stoll, M.L.; Punaro, M. Psoriatic Juvenile Idiopathic Arthritis: A Tale of Two Subgroups. Curr. Opin. Rheumatol. 2011, 23, 437–443. [Google Scholar] [CrossRef]
- Garrido-Castro, J.L.; Calvo-Gutierrez, J.; Gonzalez-Navas, C.; Font-Ugalde, P.; Castro-Villegas, M.D.C.; Collantes-Estevez, E. FRI0218 Structural Damage Distribution at Vertebral Level in Patients with Axial Spondyloarthritis. Ann. Rheum. Dis. 2015, 74, 503. [Google Scholar] [CrossRef]
- Chimenti, M.S.; Alten, R.; D’Agostino, M.A.; Gremese, E.; Kiltz, U.; Lubrano, E.; Moreno, M.; Pham, T.; Ramonda, R.; Spinelli, F.R.; et al. Sex-Associated and Gender-Associated Differences in the Diagnosis and Management of Axial Spondyloarthritis: Addressing the Unmet Needs of Female Patients. RMD Open 2021, 7, e001681. [Google Scholar] [CrossRef]
- Fragoulis, G.E.; Evangelatos, G.; Konsta, M.; Iliopoulos, A. Anterior Chest Wall Involvement in Psoriatic Arthritis: A Forgotten Entity? Rheumatology (UK) 2020, 59, 3113–3114. [Google Scholar] [CrossRef] [PubMed]
- Queiro, R.; Tejón, P.; Alonso, S.; Alperi, M.; Ballina, J. Erosive Discovertebral Lesion (Andersson Lesion) as the First Sign of Disease in Axial Psoriatic Arthritis. Scand. J. Rheumatol. 2013, 42, 220–225. [Google Scholar] [CrossRef]
- Renson, T. Identifying Pitfalls and Opportunities of Magnetic Resonance Imaging in Spondyloarthritis. Belg. J. Paediatr. 2022, 24, 238–239. [Google Scholar]
- Regierer, A.; Weiß, A.; Baraliakos, X.; Behrens, F.; Poddubnny, D.; Schett, G.; Lorenz, H.M.; Worsch, M.; Strangfeld, A. Comparison of patients with axial psa and patients with axspa and concomitant. Ann. Rheum. Dis. 2022, 81, 864–865. [Google Scholar] [CrossRef]
- Badr, S.; Jacques, T.; Lefebvre, G.; Boulil, Y.; Diwan, R.A.; Cotten, A. Main Diagnostic Pitfalls in Reading the Sacroiliac Joints on Mri. Diagnostics 2021, 11, 2001. [Google Scholar] [CrossRef] [PubMed]
- Caetano, A.P.; Mascarenhas, V.V.; Machado, P.M. Axial Spondyloarthritis: Mimics and Pitfalls of Imaging Assessment. Front. Med. (Lausanne) 2021, 8, 658538. [Google Scholar] [CrossRef] [PubMed]
- Slobodin, G.; Lidar, M.; Eshed, I. Clinical and Imaging Mimickers of Axial Spondyloarthritis. Semin. Arthritis Rheum 2017, 47, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Gao, Z.; Zhong, Y.; Meng, Q. Osteitis Condensans Ilii May Demonstrate Bone Marrow Edema on Sacroiliac Joint Magnetic Resonance Imaging. Int. J. Rheum. Dis. 2018, 21, 299–307. [Google Scholar] [CrossRef] [Green Version]
- Chabros, P.; Pietrzak, A.; Gągała, J.; Kandzierski, G.; Krasowska, D. Psoriatic Arthritis—Classification, Diagnostic and Clinical Aspects. Przegl. Dermatol. 2020, 107, 32–43. [Google Scholar] [CrossRef]
- Li, S.-S.; Du, N.; He, S.-H.; Liang, X.; Li, T.-F. Dactylitis Is Associated with More Severe Axial Joint Damage and Higher Disease Activity in Axial Psoriatic Arthritis. J. Rheumatol. 2022, 49, 1012–1019. [Google Scholar] [CrossRef]
- Guo, Z.K.; Zhang, Y.M.; Kong, C.Y.; Liu, Y.; Ji, X.D.; Zhan, Y.; Qi, W.F.; Lei, X.W. Whole-Body Magnetic Resonance Imaging vs. Clinical Evaluation of Enthesitis in Patients with Spondyloarthritis. Chin. Med. J. (Engl.) 2021, 134, 2638–2640. [Google Scholar] [CrossRef]
- Ren, C.; Zhu, Q.; Yuan, H. Mono-Exponential and Bi-Exponential Model-Based Diffusion-Weighted MR Imaging and IDEAL-IQ Sequence for Quantitative Evaluation of Sacroiliitis in Patients with Ankylosing Spondylitis. Clin. Rheumatol. 2018, 37, 3069–3076. [Google Scholar] [CrossRef]
- Sarbu, M.I.; Sarbu, N.; Ene, D.C.; Corche, D.; Baz, R.; Negru, D.; Nechita, A.; Fotea, S.; Anghel, L.; Tatu, A.L. New Perspectives on Diagnosing Psoriatic Arthritis by Imaging Techniques. Open Access Rheumatol. 2021, 13, 343–352. [Google Scholar] [CrossRef]
- Latest News and Advancements Within the Areas of Axial Spondyloarthritis and Psoriatic Arthritis Featured at EULAR 2021. EMJ Rheumatol. 2021, 8, 2–10.
- Mandl, P.; Navarro-Compán, V.; Terslev, L.; Aegerter, P.; van der Heijde, D.; D’Agostino, M.A.; Baraliakos, X.; Pedersen, S.J.; Jurik, A.G.; Naredo, E.; et al. EULAR Recommendations for the Use of Imaging in the Diagnosis and Management of Spondyloarthritis in Clinical Practice. Ann. Rheum. Dis. 2015, 74, 1327–1339. [Google Scholar] [CrossRef]
- Kan, J.H. Juvenile Idiopathic Arthritis and Enthesitis-Related Arthropathies. Pediatr. Radiol. 2013, 43, 172–180. [Google Scholar] [CrossRef]
- Pradsgaard, D.Ø.; Spannow, A.H.; Heuck, C.; Herlin, T. Decreased Cartilage Thickness in Juvenile Idiopathic Arthritis Assessed by Ultrasonography. J. Rheumatol. 2013, 40, 1596–1603. [Google Scholar] [CrossRef] [PubMed]
- Gelfand, J.M.; Weinstein, R.; Neimann, A.L.; Berlin, J.A.; Margolis, D.J. Prevalence and Treatment of Psoriasis in the United Kingdom A Population-Based Study. Arch. Dermatol. 2005, 141, 1537–1541. [Google Scholar] [CrossRef] [PubMed]
- Tuttle, K.S.L.; Vargas, S.O.; Callahan, M.J.; Bae, D.S.; Nigrovic, P.A. Enthesitis as a Component of Dactylitis in Psoriatic Juvenile Idiopathic Arthritis: Histology of an Established Clinical Entity. Pediatr. Rheumatol. 2015, 13, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ravelli, A.; Consolaro, A.; Schiappapietra, B.; Martini, A. The Conundrum of Juvenile Psoriatic Arthritis. Clin. Exp. Rheumatol. 2015, 33 (Suppl. S93), S40–S43. [Google Scholar]
- Martini, A.; Ravelli, A.; Avcin, T.; Beresford, M.W.; Burgos-Vargas, R.; Cuttica, R.; Ilowite, N.T.; Khubchandani, R.; Laxer, R.M.; Lovell, D.J.; et al. Toward New Classification Criteria for Juvenile Idiopathic Arthritis: First Steps, Pediatric Rheumatology International Trials Organization International Consensus. J. Rheumatol. 2019, 46, 190–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Debrach, A.C.; Rougelot, A.; Beaumel, A.; Cabrera, N.; Belot, A.; Duquesne, A.; Aubry-Rozier, B.; Hofer, M.; Couret, M.; Larbre, J.P.; et al. Comparison of Paediatric and Adult Classification Criteria in Juvenile Idiopathic Arthritis during the Transition from Paediatric to Adult Care. Jt. Bone Spine 2021, 88, 105047. [Google Scholar] [CrossRef] [PubMed]
- Guillaume-Czitrom, S.; Sibilia, J.; Nordal, E. Growing up with Chronic Arthritis: The Confusing Matter of Classification. RMD Open 2017, 3, e000417. [Google Scholar] [CrossRef] [PubMed]
- Stoll, M.L.; Zurakowski, D.; Nigrovic, L.E.; Nichols, D.P.; Sundel, R.P.; Nigrovic, P.A. Patients with Juvenile Psoriatic Arthritis Comprise Two Distinct Populations. Arthritis Rheum 2006, 54, 3564–3572. [Google Scholar] [CrossRef] [PubMed]
- Nusman, C.M.; Hemke, R.; Lavini, C.; Schonenberg-Meinema, D.; van Rossum, M.A.J.; Dolman, K.M.; van den Berg, J.M.; Maas, M.; Kuijpers, T.W. Dynamic Contrast-Enhanced Magnetic Resonance Imaging Can Play a Role in Predicting Flare in Juvenile Idiopathic Arthritis. Eur. J. Radiol. 2017, 88, 77–81. [Google Scholar] [CrossRef]
- Murata, N.; Murata, K.; Gonzalez-Cuyar, L.F.; Maravilla, K.R. Gadolinium Tissue Deposition in Brain and Bone. Magn. Reason. Imaging 2016, 34, 1359–1365. [Google Scholar] [CrossRef]
- Kruithof, E.; Baeten, D.; de Rycke, L.; Vandooren, B.; Foell, D.; Roth, J.; Cañete, J.D.; Boots, A.M.; Veys, E.M.; de Keyser, F. Open Access Synovial Histopathology of Psoriatic Arthritis, Both Oligo-and Polyarticular, Resembles Spondyloarthropathy More than It Does Rheumatoid Arthritis. Arthritis Res. Ther. 2005, 7, 569–580. [Google Scholar] [CrossRef] [Green Version]
- Bolt, J.W.; van Ansenwoude, C.M.J.; Hammoura, I.; van de Sande, M.G.; van Baarsen, L.G.M. Translational Research Studies Unraveling the Origins of Psoriatic Arthritis: Moving Beyond Skin and Joints. Front. Med. (Lausanne) 2021, 8, 711823. [Google Scholar] [CrossRef]
- van Kuijk, A.W.R.; Reinders-Blankert, P.; Smeets, T.J.M.; Dijkmans, B.A.C.; Tak, P.P. Detailed Analysis of the Cell Infiltrate and the Expression of Mediators of Synovial Inflammation and Joint Destruction in the Synovium of Patients with Psoriatic Arthritis: Implications for Treatment. Ann. Rheum. Dis. 2006, 65, 1551–1557. [Google Scholar] [CrossRef] [Green Version]
- Reece, R.J.; Canete, J.D.; Parsons, W.J.; Emery, P.; Veale, D.J. Distinct vascular patterns of early synovitis in psoriatic, reactive, and rheumatoid arthritis. Arthritis Rheum. 1999, 42, 1481–1484. [Google Scholar] [CrossRef]
- Tenazinha, C.; Barros, R.; Fonseca, J.E.; Vieira-Sousa, E. Histopathology of Psoriatic Arthritis Synovium—A Narrative Review. Front. Med. (Lausanne) 2022, 9, 860813. [Google Scholar] [CrossRef] [PubMed]
- Ingegnoli, F.; Coletto, L.A.; Scotti, I.; Compagnoni, R.; Randelli, P.S.; Caporali, R. The Crucial Questions on Synovial Biopsy: When, Why, Who, What, Where, and How? Front. Med. (Lausanne) 2021, 8, 705382. [Google Scholar] [CrossRef] [PubMed]
- Ramwadhdoebe, T.H.; Hahnlein, J.; van Kuijk, B.J.; Choi, I.Y.; van Boven, L.J.; Gerlag, D.M.; Tak, P.P.; van Baarsen, L.G. Human Lymph-Node CD8+ T Cells Display an Altered Phenotype during Systemic Autoimmunity. Clin. Transl. Immunol. 2016, 5, e67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehta, S.; Singal, A.; Singh, N.; Nath Bhattacharya, S.; Bhattacharya, N. A Study of Clinicohistopathological Correlation in A Study of Clinicohistopathological Correlation in Patients of Psoriasis and Psoriasiform Dermatitis Patients of Psoriasis and Psoriasiform Dermatitis. Indian J. Dermatol. Venereol. Leprol. 2009, 75, 100. [Google Scholar]
- Karouzakis, E.; Hähnlein, J.; Grasso, C.; Semmelink, J.F.; Tak, P.P.; Gerlag, D.M.; Gay, S.; Ospelt, C.; van Baarsen, L.G.M. Molecular Characterization of Human Lymph Node Stromal Cells during the Earliest Phases of Rheumatoid Arthritis. Front. Immunol. 2019, 10, 1863. [Google Scholar] [CrossRef] [Green Version]
- Ramwadhdoebe, T.H.; Hähnlein, J.; Maijer, K.I.; van Boven, L.J.; Gerlag, D.M.; Tak, P.P.; van Baarsen, L.G.M. Lymph Node Biopsy Analysis Reveals an Altered Immunoregulatory Balance Already during the At-Risk Phase of Autoantibody Positive Rheumatoid Arthritis. Eur. J. Immunol. 2016, 46, 2812–2821. [Google Scholar] [CrossRef]
- van Baarsen, L.G.M.; de Hair, M.J.H.; Ramwadhdoebe, T.H.; Zijlstra, I.J.A.J.; Maas, M.; Gerlag, D.M.; Tak, P.P. The Cellular Composition of Lymph Nodes in the Earliest Phase of Inflammatory Arthritis. Ann. Rheum. Dis. 2013, 72, 1420–1424. [Google Scholar] [CrossRef]
- Proft, F.; Torgutalp, M.; Muche, B.; Rios Rodriguez, V.; Verba, M.; Poddubnyy, D. Efficacy of Tofacitinib in Reduction of Inflammation Detected on MRI in Patients with Psoriatic ArthritiS PresenTing with Axial Involvement (PASTOR): Protocol of a Randomised, Double-Blind, Placebo-Controlled, Multicentre Trial. BMJ Open. 2021, 11, e048647. [Google Scholar] [CrossRef] [PubMed]
- Acosta Felquer, M.L.; LoGiudice, L.; Galimberti, M.L.; Rosa, J.; Mazzuoccolo, L.; Soriano, E.R. Treating the Skin with Biologics in Patients with Psoriasis Decreases the Incidence of Psoriatic Arthritis. Ann. Rheum. Dis. 2022, 81, 74–79. [Google Scholar] [CrossRef]
- Menter, A.; Krueger, G.G.; Paek, S.Y.; Kivelevitch, D.; Adamopoulos, I.E.; Langley, R.G. Interleukin-17 and Interleukin-23: A Narrative Review of Mechanisms of Action in Psoriasis and Associated Comorbidities. Dermatol. Ther. (Heidelb.) 2021, 11, 385–400. [Google Scholar] [CrossRef]
- Aouad, K.; El-Zorkany, B. Treat-to-Target in Axial Spondyloarthritis: Are We There Yet? Mediterr. J. Rheumatol. 2022, 33, 137–141. [Google Scholar] [CrossRef]
- Hioki, T.; Komine, M.; Ohtsuki, M. Diagnosis and Intervention in Early Psoriatic Arthritis. J. Clin. Med. 2022, 11, 2051. [Google Scholar] [CrossRef]
- Ogdie, A.; Coates, L.C.; Gladman, D.D. Treatment Guidelines in Psoriatic Arthritis. Rheumatology (UK) 2021, 59, I37–I46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milutinovic, S.; Veljkovic, K.; Zlatanovic, M.; Radunovic, G.; Damjanov, N. Depression/Anxiety Symptoms in Axial Spondyloarthritis and Psoriatic Arthritis Patients in Serbia: A Pilot Study. Rheumatol. Int. 2019, 39, 1595–1605. [Google Scholar] [CrossRef] [PubMed]
- Singh, J.A.; Guyatt, G.; Ogdie, A.; Gladman, D.D.; Deal, C.; Deodhar, A.; Dubreuil, M.; Dunham, J.; Husni, M.E.; Kenny, S.; et al. Special Article: 2018 American College of Rheumatology/National Psoriasis Foundation Guideline for the Treatment of Psoriatic Arthritis. Arthritis Rheumatol. 2019, 71, 5–32. [Google Scholar] [CrossRef] [Green Version]
- Advancements in Psoriatic Arthritis Management: Updated GRAPPA Treatment Recommendations. In Proceedings of the GRAPPA Annual Meeting and Trainee Symposium 2022, Brooklyn, NY, USA, 14–16 July 2022.
- Wervers, K.; Vis, M.; Tchetveriko, I.; Gerards, A.H.; Kok, M.R.; Appels, C.W.Y.; van der Graaff, W.L.; van Groenendael, J.H.L.M.; Korswagen, L.A.; Veris-van Dieren, J.J.; et al. Burden of Psoriatic Arthritis According to Different Definitions of Disease Activity: Comparing Minimal Disease Activity and the Disease Activity Index for Psoriatic Arthritis. Arthritis Care. Res. (Hoboken) 2018, 70, 1764–1770. [Google Scholar] [CrossRef] [Green Version]
- Haque, N.; Lories, R.J.; de Vlam, K. Orthopaedic Interventions in Patients with Psoriatic Arthritis: A Descriptive Report from the SPAR Cohort. RMD Open. 2016, 2, e000293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mekhail, C.; Chouk, M.; Prati, C.; Wendling, D.; Verhoeven, F. Prognostic Factors of Good Response to DMARDs in Psoriatic Arthritis: A Narrative Review. Expert Rev. Clin. Pharmacol. 2020, 13, 505–519. [Google Scholar] [CrossRef] [PubMed]
- Koutsompina, M.L.; Pappa, M.; Sakellariou, S.; Gialouri, C.G.; Fragoulis, G.E.; Androutsakos, T. Methotrexate-Related Liver Cirrhosis in Psoriatic Arthritis: A Case Report and Review of the Literature. Mediterr. J. Rheumatol. 2021, 32, 264–272. [Google Scholar] [CrossRef] [PubMed]
- Roy, A.; Darapureddy, A.; Kumar, Y. Noninvasive Assessment of Liver Fibrosis by Magnetic Resonance Elastography in Patients with Rheumatic Disease on Long-Term Methotrexate Treatment. Indian J. Rheumatol. 2023, 18, 54–60. [Google Scholar] [CrossRef]
- Hoganson, D.D.; Chen, J.; Ehman, R.L.; Talwalkar, J.A.; Michet, C.J.; Yin, M.; Crowson, C.S.; Matteson, E.L. Magnetic Resonance Elastography for Liver Fibrosis in Methotrexate Treatment. Open J. Rheumatol. Autoimmune. Dis 2012, 02, 6–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mease, P.J.; Armstrong, A.W. Managing Patients with Psoriatic Disease: The Diagnosis and Pharmacologic Treatment of Psoriatic Arthritis in Patients with Psoriasis. Drugs 2014, 74, 423–441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahmood, F.; Helliwell, P. Psoriatic Arthritis: A Review. EMJ Reumatol. 2016, 3, 114–117. [Google Scholar]




| Author | Year | Study Population | Provided Information |
|---|---|---|---|
| Braga et al. [17] | 2020 | 45 patients | MRI sacroiliitis evaluation |
| Benavent et al. [18] | 2021 | 3684 patients | |
| Feld et al. [19] | 2021 | 1354 patients | |
| Furer et al. [20] | 2021 | 107 patients | |
| Diaz et al. [21] | 2022 | 93 patients | |
| Castillo-Gallego et al. [22] | 2013 | 76 patientes | Assement of inflammatory and structural damage |
| Ye et al. [23] | 2019 | 121 patients | |
| Poggenborg et al. [24] | 2015 | 48 patients | Comparison with other SpA entities |
| Jadon et al. [25] | 2017 | 402 patients | |
| Gensler et al. [26] | 2020 | 203 patients | |
| Salinas et al. [27] | 2021 | 139 patients | |
| Abdelaziz et al. [28] | 2021 | 100 patients | |
| Arnbak et al. [29] | 2016 | 1037 patients | Inflammatory back pain prevalence, MRI findings, and clinical correlations |
| Yap et al. [30] | 2018 | 171 patients | |
| Aydin et al. [31] | 2017 | 1195 patients | |
| Kivity et al. [32] | 2018 | 224 patients | |
| Zisman et al. [33] | 2017 | 361 patients | Juvenile idiopatic arthritis, risks of psoriasis association, and other comorbidities |
| Ekelund et al. [34] | 2017 | 440 patients | |
| Brandon et al. [11] | 2018 | 26710 patients | |
| Lamot et al. [35] | 2021 | 71 patients | |
| Jawad et al. [36] | 2022 | 335 patients | Treatment side effects |
| Classification | Details | Pros | Cons |
|---|---|---|---|
| CASPAR | Inflammatory arthritis of joint/spine/enthesis + ≥3 points from the following:
|
|
|
| Moll and Wright | Arthritis + Psoriasis + Negative rheumatoid factor. Divides PsA into five categories: - DIP joint only; - Asymmetrical oligoarthritis; - Polyarthritis; - Spondylitis; - Arthritis mutilans. | Historically, it was the simplest and most used criteria. |
|
| ESSG (European SpA Study Group) | Synovitis/inflammatory back pain + Current psoriasis or personal history. Other features: - Arthritis; - Buttock pain; - Enthesitis; - Sacroiliitis; - Inflammatory bowel disease; - Episodes of acute diarrhea; - Urethritis [8]. |
| Lower sensitivity. |
| Vasey and Espinoza | Psoriasis/psoriatic nail dystrophy +
|
|
|
| ASAS | Sacroiliitis in imaging studies (active inflammatory lesions in an MRI examination or X-ray changes defined according to the modified New York criteria) + ≥1 sign of spondyloarthropathy, or HLA-B27 antigen present + ≥2 signs of spondyloarthropathy SpA features: - Inflammatory back pain (IBP) - Arthritis - Enthesitis (heel) - Uveitis - Dactylitis - Psoriasis - Crohn’s disease/colitis - Good response to NSAIDs - Family history of SpA - HLA-B27 - Elevated CRP |
| Low specificity (77%) for PsA, as it has common features with other axSpA. |
| ILAR [47] | Definite jPsA. Arthritis and psoriasis or Arthritis with at least two of the following: - Dactylitis; - Nail pitting or onycholysis; - Psoriasis in a first-degree relative. Exclusion criteria: - Arthritis in an HLA-B27-positive male with arthritis onset after 6 years of age; - Ankylosing spondylitis, enthesitis-related arthritis, sacroiliitis with IBD, Reiter’s syndrome, or acute anterior uveitis in a first-degree relative; - Presence of the IgM rheumatoid factor on at least two occasions more than 3 months apart; - Presence of systemic JIA. Definite ERA. Arthritis and enthesitis, or arthritis or enthesitis with at least two of the following: - Presence or history of sacroiliac joint tenderness and/or inflammatory lumbosacral pain; - Presence of the HLA-B27 antigen; - Onset of arthritis in a male over 6 years of age; - Acute (symptomatic) anterior uveitis; - History of ankylosing spondylitis, enthesitis-related arthritis, sacroiliitis with inflammatory bowel disease, Reiter’s syndrome, or acute anterior uveitis in a first-degree relative. Exclusion criteria: - Psoriasis or a history of psoriasis in the patient or a first-degree relative; - Presence of an IgM rheumatoid factor on at least two occasions at least 3 months apart; - Presence of systemic JIA in the patient. |
|
|
| axPsA | AS | |
|---|---|---|
| 44% HLA-B27-positive | 90% HLA-B27-positive | |
| Cervical spine | Facet joints fusion—more frequent | |
| Dorsal spine | Non-marginal syndesmophytes (spinal ligament origin) Asymmetrical Cranial to caudal evolution | Marginal syndesmophytes Symmetrical Caudal to cranial Paravertebral ossification |
| Lumbar spine | Facet joints fusion—more frequent | |
| Sacroiliac | Less severe sacroiliitis Asymmetrical sacroiliitis Syndesmophytes extend into SIJ space Syndesmophytes may be observed in the absence of sacroiliitis | Severe sacroiliitis Symmetrical Syndesmophytes pass across the SIJ space |
| BME | Lower score in spine and SIJ | Higher score |
| Fat metaplasia | Less severe | More severe |
| Erosions | Less severe | More severe |
| Peripheral involvement Enthesitis | More often dactylitis, nail dystrophy Similar to AS | Less often Similar to PsA |
| Uveitis | Rare | Frequent |
| Inflammatory bowel disease | Similar prevalence | Similar prevalence |
| Condition | Characteristic Location of BME |
|---|---|
| axSpA | Posterior lower quadrant of the ilium |
| Dorsal-cartilaginous segment of the SIJ | |
| Healthy individuals | Lower iliac bone |
| Sports individuals | Overlaps with axSpA |
| Posterior lower quadrant of the ilium | |
| Anterior upper quadrant of the sacrum | |
| Postpartum | Overlaps with axSpA |
| Typically, no structural changes | |
| Degenerative | Anterior and middle thirds |
| Ligamentous segment of the SIJ | |
| Associated with the degeneration of the pubic symphysis |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pascu, L.S.; Sârbu, N.; Brădeanu, A.V.; Jicman, D.; Matei, M.N.; Sârbu, M.I.; Voinescu, D.C.; Nechita, A.; Tatu, A.L. MRI Findings in Axial Psoriatic Spondylarthritis. Diagnostics 2023, 13, 1342. https://doi.org/10.3390/diagnostics13071342
Pascu LS, Sârbu N, Brădeanu AV, Jicman D, Matei MN, Sârbu MI, Voinescu DC, Nechita A, Tatu AL. MRI Findings in Axial Psoriatic Spondylarthritis. Diagnostics. 2023; 13(7):1342. https://doi.org/10.3390/diagnostics13071342
Chicago/Turabian StylePascu, Loredana Sabina, Nicolae Sârbu, Andrei Vlad Brădeanu, Daniela Jicman (Stan), Madalina Nicoleta Matei, Mihaela Ionela Sârbu, Doina Carina Voinescu, Aurel Nechita, and Alin Laurențiu Tatu. 2023. "MRI Findings in Axial Psoriatic Spondylarthritis" Diagnostics 13, no. 7: 1342. https://doi.org/10.3390/diagnostics13071342
APA StylePascu, L. S., Sârbu, N., Brădeanu, A. V., Jicman, D., Matei, M. N., Sârbu, M. I., Voinescu, D. C., Nechita, A., & Tatu, A. L. (2023). MRI Findings in Axial Psoriatic Spondylarthritis. Diagnostics, 13(7), 1342. https://doi.org/10.3390/diagnostics13071342