Abstract
We present a case of a 59-year-old male diagnosed with polycythemia vera (PV) for many years, who presented with a relatively abrupt onset of heavy constitutional symptoms, including fatigue, night sweats, and a 10% weight loss over 6 weeks. Despite the known initial diagnosis of PV, the presence of profound B-symptoms prompted further investigation. A positron emission tomography/computed tomography (PET/CT) scan with 18F-Fluorodeoxyglucose ([18F]FDG) was performed to exclude malignant diseases. The [18F]FDG PET/CT revealed intense metabolic activity in the bone marrow of the proximal extremities and trunk skeleton, as well as a massively enlarged spleen with increased metabolic activity. Histopathologically, a transformation to myelofibrosis was revealed on a bone marrow biopsy. The case intends to serve as an exemplification for [18F]FDG PET/CT in PV with transformation to myelofibrosis (post-PV myelofibrosis).
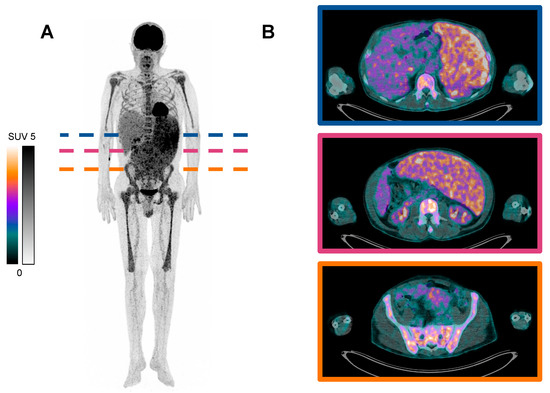
Figure 1.
18F-Fluorodeoxyglucose ([18F]FDG) targeted positron emission tomography/computed tomography (PET/CT) scan of a patient with advanced polycythemia vera (PV) and transformation to myelofibrosis. A 59-year-old male with a known history of PV presented with newly developed profound constitutional symptoms, including fatigue, night sweats, and a 10% weight loss over 6 weeks. Despite the known initial diagnosis of PV, the abrupt deterioration of his general condition and new onset of B-symptoms prompted further investigation, and the patient was referred to the nuclear medicine department for further diagnostics regarding malignancy. Subsequently, a [18F]FDG PET/CT (acquired 65 min post-injection of 225 MBq) was performed: (A) maximum intensity projection (MIP), and (B) three transversal slices of [18F]FDG PET/CT, showing intense metabolic activity in the bone marrow of the proximal extremities and trunk skeleton, as well as an enlarged spleen with increased metabolic activity. (B) shows the specific extent of splenomegaly from the upper abdominal to the pelvic region with increased metabolic activity. No evidence of a secondary malignancy was found. Bone marrow biopsy was conducted, and histopathological examination revealed hypercellularity with increased erythroid, myeloid, and thromboid lineages with grade 2 fibrosis (MF-2 according to European consensus grading [1]). Additional molecular studies detected JAK2 V617F mutation. Thereby, the diagnosis of advanced PV with transformation to post-PV myelofibrosis was determined. Polycythemia vera (PV) is a clonal myeloproliferative neoplasm (MPN) characterized by erythrocytosis, often accompanied by leukocytosis and/or thrombocytosis. It belongs to the group of chronic myeloproliferative neoplasms (MPN), according to WHO/ICC 2022 [2]. Genetic alterations of the hematopoietic stem cell are the underlying pathomechanism, causing a clonal proliferation of one or more terminally differentiated cell lineages in the peripheral blood. Major diagnostic criteria for the diagnosis of PV include elevated hemoglobin concentration and/or hematocrit, the presence of JAK2 V617F or JAK2 exon 12 mutations, and trilineage hyperplasia (panmyelosis) on a bone marrow biopsy [3]. PV can evolve into myelofibrosis (post-PV myelofibrosis) or acute myeloid leukemia (AML) [4]. Approximately 50% of patients will progress to post-PV myelofibrosis 20 years after disease onset. In some cases, patients may present with profound B-symptoms, leading to concerns about an independent second underlying malignancy. In this scenario [18F], FDG PET/CT imaging has a high differential diagnostic value by identifying metabolic abnormalities in tissue as malignancy [5,6] or, as in this case, aiding in the detection of the shift to spent-phase PV with subsequent myelofibrosis [7]. The potential of [18F]FDG in the management of PV was only reported for a limited number of patients [8,9,10] and is not established as a standard imaging modality. Depending on the severity of PV, different levels of uptake in the bone marrow and spleen are reported and may be characteristic [10,11,12,13]. The heightened metabolic activity PV is primarily attributed to the increased cellular turnover and proliferation within the bone marrow, as well as the enlarged spleen, which is actively involved in hematopoiesis and sequestration of blood cells. The case intends to serve as an exemplification for [18F]FDG PET/CT in PV with transformation to myelofibrosis (post-PV myelofibrosis). Future studies, ideally in prospective settings, should be performed evaluating the value of [18F]FDG PET/CT in clinical practice, i.e., diagnostic and treatment of PV.
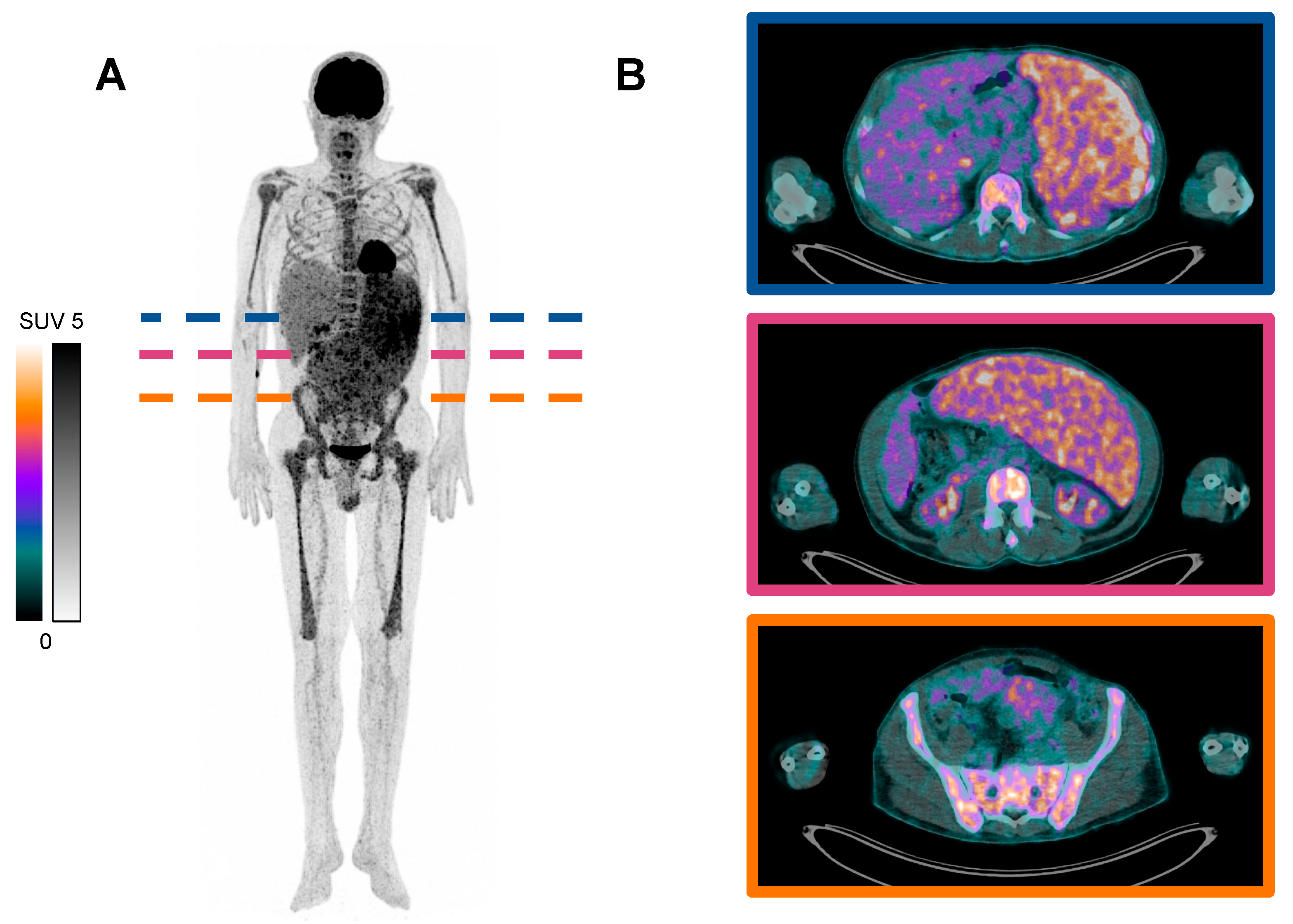
Figure 1.
18F-Fluorodeoxyglucose ([18F]FDG) targeted positron emission tomography/computed tomography (PET/CT) scan of a patient with advanced polycythemia vera (PV) and transformation to myelofibrosis. A 59-year-old male with a known history of PV presented with newly developed profound constitutional symptoms, including fatigue, night sweats, and a 10% weight loss over 6 weeks. Despite the known initial diagnosis of PV, the abrupt deterioration of his general condition and new onset of B-symptoms prompted further investigation, and the patient was referred to the nuclear medicine department for further diagnostics regarding malignancy. Subsequently, a [18F]FDG PET/CT (acquired 65 min post-injection of 225 MBq) was performed: (A) maximum intensity projection (MIP), and (B) three transversal slices of [18F]FDG PET/CT, showing intense metabolic activity in the bone marrow of the proximal extremities and trunk skeleton, as well as an enlarged spleen with increased metabolic activity. (B) shows the specific extent of splenomegaly from the upper abdominal to the pelvic region with increased metabolic activity. No evidence of a secondary malignancy was found. Bone marrow biopsy was conducted, and histopathological examination revealed hypercellularity with increased erythroid, myeloid, and thromboid lineages with grade 2 fibrosis (MF-2 according to European consensus grading [1]). Additional molecular studies detected JAK2 V617F mutation. Thereby, the diagnosis of advanced PV with transformation to post-PV myelofibrosis was determined. Polycythemia vera (PV) is a clonal myeloproliferative neoplasm (MPN) characterized by erythrocytosis, often accompanied by leukocytosis and/or thrombocytosis. It belongs to the group of chronic myeloproliferative neoplasms (MPN), according to WHO/ICC 2022 [2]. Genetic alterations of the hematopoietic stem cell are the underlying pathomechanism, causing a clonal proliferation of one or more terminally differentiated cell lineages in the peripheral blood. Major diagnostic criteria for the diagnosis of PV include elevated hemoglobin concentration and/or hematocrit, the presence of JAK2 V617F or JAK2 exon 12 mutations, and trilineage hyperplasia (panmyelosis) on a bone marrow biopsy [3]. PV can evolve into myelofibrosis (post-PV myelofibrosis) or acute myeloid leukemia (AML) [4]. Approximately 50% of patients will progress to post-PV myelofibrosis 20 years after disease onset. In some cases, patients may present with profound B-symptoms, leading to concerns about an independent second underlying malignancy. In this scenario [18F], FDG PET/CT imaging has a high differential diagnostic value by identifying metabolic abnormalities in tissue as malignancy [5,6] or, as in this case, aiding in the detection of the shift to spent-phase PV with subsequent myelofibrosis [7]. The potential of [18F]FDG in the management of PV was only reported for a limited number of patients [8,9,10] and is not established as a standard imaging modality. Depending on the severity of PV, different levels of uptake in the bone marrow and spleen are reported and may be characteristic [10,11,12,13]. The heightened metabolic activity PV is primarily attributed to the increased cellular turnover and proliferation within the bone marrow, as well as the enlarged spleen, which is actively involved in hematopoiesis and sequestration of blood cells. The case intends to serve as an exemplification for [18F]FDG PET/CT in PV with transformation to myelofibrosis (post-PV myelofibrosis). Future studies, ideally in prospective settings, should be performed evaluating the value of [18F]FDG PET/CT in clinical practice, i.e., diagnostic and treatment of PV.
Author Contributions
Conceptualization: M.B.B., C.B., F.R. and S.E.; investigation: M.B.B., C.B., S.E., O.F., K.C. and F.R.; writing—original draft preparation: M.B.B., A.B., C.B. and F.R.; writing—review and editing: M.B.B., O.F. and K.C.; visualization: A.B.; supervision: S.E. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
An ethical review and approval were waived for this report, as it is a retrospective case description that has no retroactive influence on the patient’s treatment.
Informed Consent Statement
Written informed consent has been obtained from the patient to publish this paper.
Data Availability Statement
The datasets, including the DICOM image file used and analyzed in this paper, are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Thiele, J.; Kvasnicka, H.M.; Facchetti, F.; Franco, V.; van der Walt, J.; Orazi, A. European consensus on grading bone marrow fibrosis and assessment of cellularity. Haematologica 2005, 90, 1128–1132. [Google Scholar] [PubMed]
- Arber, D.A.; Orazi, A.; Hasserjian, R.P.; Borowitz, M.J.; Calvo, K.R.; Kvasnicka, H.-M.; Wang, S.A.; Bagg, A.; Barbui, T.; Branford, S.; et al. International Consensus Classification of Myeloid Neoplasms and Acute Leukemias: Integrating morphologic, clinical, and genomic data. Blood 2022, 140, 1200–1228. [Google Scholar] [CrossRef] [PubMed]
- Khoury, J.D.; Solary, E.; Abla, O.; Akkari, Y.; Alaggio, R.; Apperley, J.F.; Bejar, R.; Berti, E.; Busque, L.; Chan, J.K.C.; et al. The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Myeloid and Histiocytic/Dendritic Neoplasms. Leukemia 2022, 36, 1703–1719. [Google Scholar] [CrossRef]
- Tefferi, A.; Barbui, T. Polycythemia vera: 2024 update on diagnosis, risk-stratification, and management. Am. J. Hematol. 2023, 98, 1465–1487. [Google Scholar] [CrossRef]
- Kouijzer, I.J.; Mulders-Manders, C.M.; Bleeker-Rovers, C.P.; Oyen, W.J. Fever of Unknown Origin: The Value of FDG-PET/CT. Semin. Nucl. Med. 2018, 48, 100–107. [Google Scholar] [CrossRef] [PubMed]
- El-Galaly, T.C.; Gormsen, L.C.; Hutchings, M. PET/CT for Staging; Past, Present, and Future. Semin. Nucl. Med. 2018, 48, 4–16. [Google Scholar] [CrossRef] [PubMed]
- Barosi, G.; Mesa, R.A.; Thiele, J.; Cervantes, F.; Campbell, P.J.; Verstovsek, S.; Dupriez, B.; Levine, R.L.; Passamonti, F.; Gotlib, J.; et al. Proposed criteria for the diagnosis of post-polycythemia vera and post-essential thrombocythemia myelofibrosis: A consensus statement from the international working group for myelofibrosis research and treatment. Leukemia 2008, 22, 437–438. [Google Scholar] [CrossRef] [PubMed]
- Basu, S.; Asopa, R.; Peshwe, H.; Mohandas, K.M. Diffuse intense FDG uptake in the bone marrow in gastrointestinal stromal tumor with coexistent polycythemia rubra vera. Clin. Nucl. Med. 2008, 33, 782–783. [Google Scholar] [CrossRef]
- Quarles van Ufford, H.M.E.; de Jong, J.A.F.; Baarslag, H.J.; de Haas, M.J.; Oud, K.; de Klerk, J.M.H. F-18 FDG PET in a patient with polycythemia vera. Clin. Nucl. Med. 2008, 33, 780–781. [Google Scholar] [CrossRef] [PubMed]
- Ayubcha, C.; Hosoya, H.; Seraj, S.M.; Zadeh, M.Z.; Werner, T.; Alavi, A. A Pilot Study of FDG-PET/CT in Polycythemia Vera Using Global Analysis Techniques. Asia Ocean. J. Nucl. Med. Biol. 2020, 8, 64–68. [Google Scholar] [CrossRef]
- Slot, S.; van de Donk, N.W.C.J.; Otten, R.H.J.; Boden, B.J.H.; Zijlstra, J.; Raijmakers, P.G.H.M.; Zweegman, S. The value of bone marrow, liver, and spleen imaging in diagnosis, prognostication, and follow-up monitoring of myeloproliferative neoplasms: A systematic review. Cancer Imaging 2021, 21, 36. [Google Scholar] [CrossRef] [PubMed]
- Agool, A.; Glaudemans, A.W.J.M.; Boersma, H.H.; Dierckx, R.A.J.O.; Vellenga, E.; Slart, R.H.J.A. Radionuclide imaging of bone marrow disorders. Eur. J. Nucl. Med. Mol. Imaging 2011, 38, 166–178. [Google Scholar] [CrossRef] [PubMed]
- Fujimi, A.; Kanisawa, Y.; Minami, S.; Kamihara, Y.; Iwasaki, S. Focal 18F-FDG uptake in bone marrow on PET/CT in a patient with JAK2 mutation without overt myeloproliferative neoplasm. Int. J. Hematol. 2014, 99, 1–3. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).