1. Introduction
The aging of the world population is a proven fact, and in fact, it is estimated that, between 2015 and 2050, the proportion of people over 60 years will rise from 12% to 22% [
1]. The term sarcopenia was initially used to describe the loss in muscle mass with advancing age [
2]. Since then, new diagnostic criteria have been added to the definition of sarcopenia, such as muscle strength and physical performance, and it was recognized as a disease by the International Classification of Diseases, Tenth Revision, Clinical Modification (code M62.84) [
3].
Currently, there are several definitions of sarcopenia according to the different study groups that consider different criteria and cutoff values. Some of the most commonly used diagnostic criteria are those proposed by the European Working Group on Sarcopenia in Older People, in 2010 (EWGSOP1) [
4], and updated in 2018 (EWGSOP2) [
5]. In 2014, the Asian Working Group on Sarcopenia (AWGS) [
6] proposed a diagnostic algorithm based on Asian data which was updated in 2019 (AWGS-2019) [
7]. There are also criteria proposed for sarcopenia diagnostic by the International Working Group on Sarcopenia (IWGS) [
8], or the Foundation for the National Institutes of Health (FNIH) Sarcopenia Project [
9]. It has been estimated that the prevalence of sarcopenia worldwide ranges from 10–16% of the older adults [
10], but it may vary depending on the definition criteria or the studies analyzed [
11].
Sarcopenia has been related to numerous adverse outcomes, including poor health-related quality of life, cognitive decline or hypertension and cardio-cerebrovascular disease or even increased mortality [
12,
13,
14,
15,
16,
17]. Moreover, sarcopenia has been associated with higher intensive care unit admission and increased hospital stays, severity of disease and risk of mortality among COVID-19 patients [
18].
The diagnosis of sarcopenia in daily clinical practice is not easy, since, in many cases, the time and specific equipment required is not available [
19]. Therefore, it is necessary to develop simple, easy-to-use, validated tools that allow for rapid screening for sarcopenia.
The SARC-F (strength, assistance in walking, rise from a chair, climb stairs, and falls) questionnaire is valid and internally consistent for screening persons at risk for adverse outcomes from sarcopenia [
20,
21], and it stands as one of the best tools to evaluate sarcopenia in every day practice [
22]. The EWGSOP2 recommends the SARC-F as a way to introduce the assessment and treatment of sarcopenia into clinical practice, and it can be easily administered in community healthcare and other clinical settings [
5].
The SARC-F was originally developed in English, and to the date, it has been translated and validated for many languages and populations [
23,
24,
25,
26]. A translation of the Portuguese versions of the SARC-F, together with the FRAIL Scale, were performed in 2021 [
27], but to the best of our knowledge, the analysis of the reliability and clinical validity of the cross-culturally adapted Portuguese version of the SARC-F has not been carried out. This questionnaire has been validated for the Brazilian Portuguese spoken population [
28], but despite the fact that Portugal and Brazil share a common language, several cultural and dialectal differences must be taken into consideration.
In view of the above, the objective of this study was to perform the translation and cross-cultural adaptation of the Portuguese version of the SAC-F and evaluate its clinical validity in Portuguese community-dwelling adults aged 65 years or older.
3. Results
The descriptive characteristics of the 100 participants (73% women) are displayed in
Table 2. The mean age was 77.07 ± 7.36 years, most of the participants had a basic education level (77%) and were married (66%). As for the body composition and sarcopenia-related parameters, women had a significantly higher fat-mass percentage (
p < 0.001), while men had significantly greater values of handgrip strength, ALMI-height
2, and ALMI-BMI (all
p < 0.001). According to the SARC-F total score, 27% of the participants were at risk of sarcopenia (SARC-F ≥ 4), and women a had significantly greater SARC-F total score (
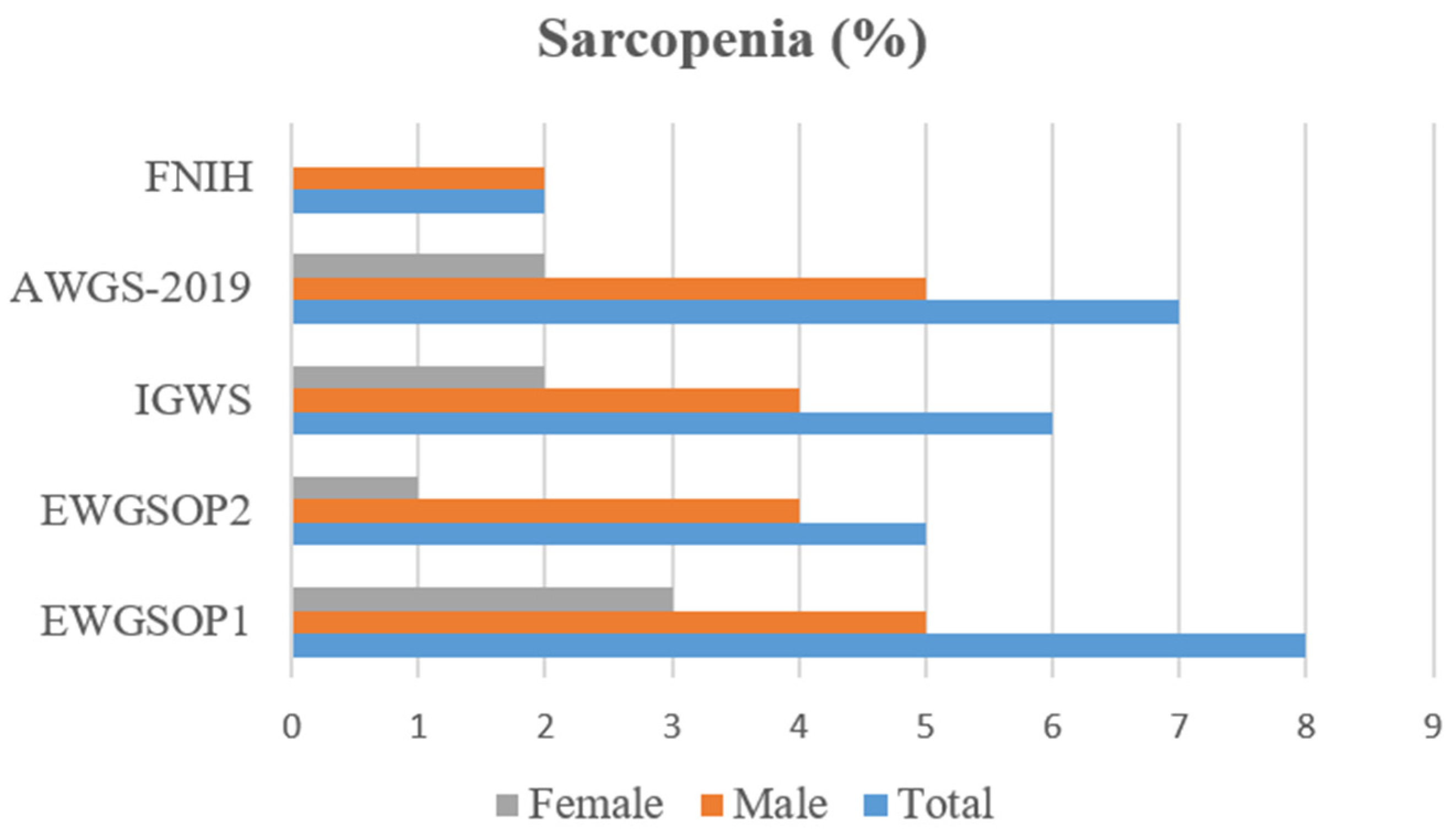
p < 0.001). When analyzing the prevalence of sarcopenia (
Figure 1), the highest and lowest percentages were seen in the diagnosis according to EWGSOP1 (8%) and FNIH (2%), respectively. In our sample, men had a higher rate of sarcopenia regardless of the diagnostic criteria.
3.1. Reliability
As for the internal consistency, the analysis showed a Cronbach α value of 0.82 for the total score of the Portuguese SARC-F, which determines an acceptable level of internal consistency (Cronbach α ≥ 0.7). Item-to-total score correlation was also performed (
Table 3) and showed significant positive correlations (all
p < 0.001), with Spearman’s coefficient values ranging from 0.63 (item 5) to 0.87 (item 4).
Regarding reliability, the inter-rater reliability analysis was carried out on 20 different participants (76 ± 6.32 years, 50% women), and we obtained an ICC value of 0.96 for the SARC-F total score, which indicate an excellent inter-rater reliability. The test–retest reliability analysis revealed substantial ICC values for item 3 (ICC = 0.81), item 1 (ICC = 0.83), item 5 (ICC = 0.85), and the total score (ICC = 0.89), while excellent correlations were observed for items 4 (ICC = 0.93) and 2 (ICC = 1).
3.2. Clinical Validity
The specificity of the Portuguese SARC-F according to the different diagnostic criteria of sarcopenia were similar (
Table 4), ranging from 72.5% (FNIH) to 73.4 (IGWS), while negative predictive values went from 91.78% (EWGSOP1) to 97.3% (FNIH). On the other hand, low scores were observed with respect to sensitivity, with percentages ranging from 0 to 33.3% (for FNIH and IGWS, respectively) and positive predictive values, ranging from 0% (FNIH) to 7.41% (EWGSOP1, IGWS, and AWGS-2019). Accuracy levels were similar (69–71%), and the values regarding the area under the ROC curve went from 0.52 (FNIH) to 0.634 (IGWS).
Concerning the associations between the total score of Portuguese of the SARC-F and sarcopenia-related parameters (
Table 5), our findings revealed significant (all
p < 0.001) and good correlations with handgrip strength, gait speed, and the TUG test (Rho Spearman’s Correlation Coefficients of −0.40, −0.68, and 0.62, respectively). As for muscle mass, no significant correlations were observed with ALMI. However, calf diameter was correlated to the SARC-F total score (rho = 0.26,
p = 0.01). When the multivariate linear regression analysis was performed (
Table 6), muscle strength (which indicates probable sarcopenia according EWGSOP2) and gait speed (severity of sarcopenia) showed independent associations, with an adjusted-R
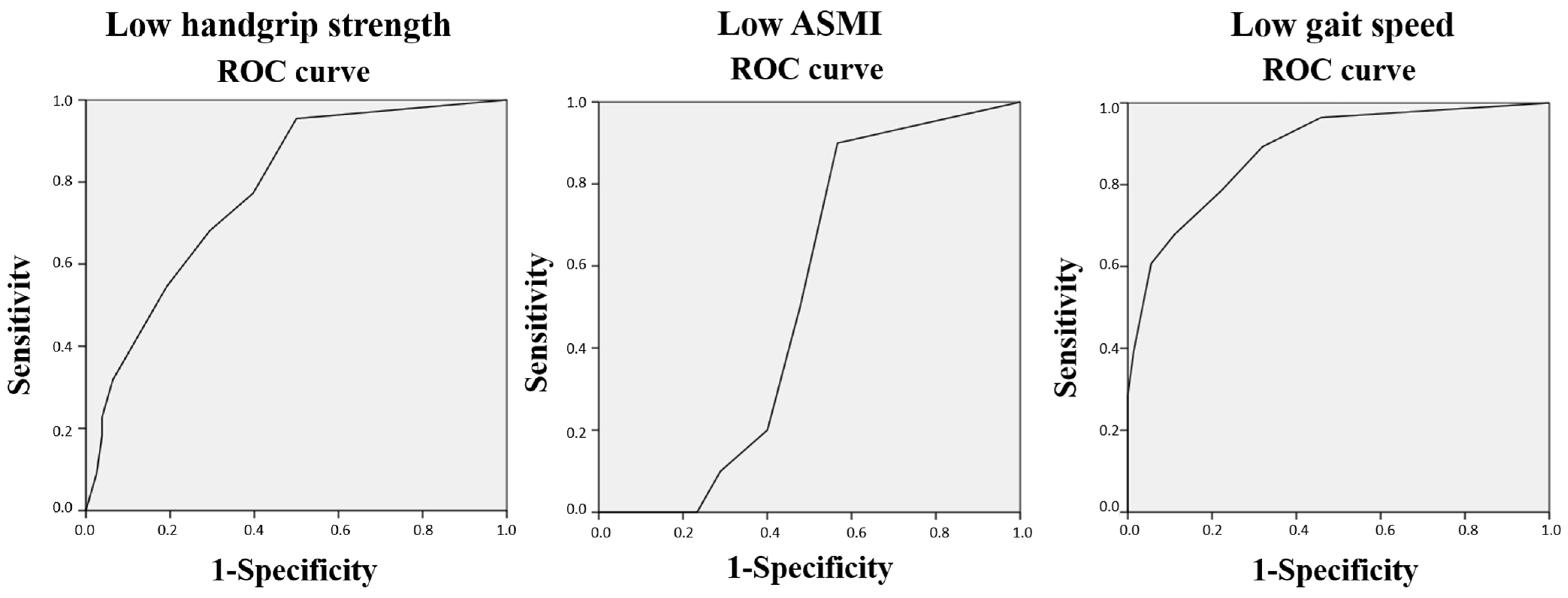
2 of 0.50 for the model, which indicated a large effect size. In the analysis of the discriminative ability of the Portuguese SARC-F total score with respect to sarcopenia-related parameters according to the EWGSOP2 (
Figure 2), our results showed that the AUC for low handgrip strength (22% of the sample, 63.4% women) and low gait speed (28% of the participants, 75% women) were 0.78 (95% confidence interval = 0.68–0.88) and 0.89 (95% confidence interval = 0.81–0.96), respectively, while for low ASMI (10% of the participants, 40% women), it was 0.52 (95% confidence interval = 0.40–0.64).
4. Discussion
The objective of this study was to perform the cross-cultural adaptation and clinical validation of the Portuguese version of the SARC-F for a population of community-dwelling Portuguese older adults. Our findings show that the Portuguese SARC-F showed adequate reliability and clinical validity to be employed for the screening of sarcopenia in Portuguese older adults. It is also a valid instrument to identify people with low handgrip strength and gait speed.
The SARC-F total score of the present study was 2.25 ± 2.61, with 27% of the participants at risk of sarcopenia (SARC-F ≥ 4), values that are between those described in previous validation articles such as those of Tsekoura et al. [
25] in Greek people (2.8 ± 1.9 and 32.3%), or Parra-Rodríguez et al. [
19] in Mexican people (1.95 ± 1.9 and 19.5%). On the other hand, 4.58% and 3.38% of the participants with a SARC-F total score ≥ 4 were described in the Thai [
40] and Japanese [
23] validations, respectively, where lower values could be explained by cultural and lifestyle factors. Our analysis also showed that women had a significantly higher SARC-F total score, which is in line with the findings described by Krzymińska-Siemaszko et al. [
41] and Perna et al. [
26] in the in the Polish and Italian validations, respectively.
The lowest prevalence of sarcopenia was observed according to the FNIH criteria (2%), which was expected given that the three diagnostic criteria are required (low values of muscle mass, strength, and physical performance). The other prevalence values were ranging from 5% (EWGSOP2) to 8% (EWGSOP1). As mentioned, low muscle mass, muscle strength, and physical fitness are the three parameters usually evaluated for sarcopenia diagnosis proposed by the different international working groups, but there are several variations regarding the diagnostic tools, cut-off points, or diagnostic criteria. For instance, Liu et al. [
42] found that, in Chinese adults ≥ 50 years, the prevalence of sarcopenia according to different operational definitions were 11.8% (EWGSOP2), 18.1% (FNIH), 22.8% (AWGS 2019), 24.1% (IWGS), and 57.1% (EWGSOP1). However, there are other factors such as age group, gender, geographical areas, ethnicities, or locations that may affect the prevalence of sarcopenia [
43,
44]. A meta-analysis published by Petermann-Rocha et al. [
45] described that the prevalence of sarcopenia varied from 10% to 27% in adults aged 60 years and over, where the highest prevalence was found in Oceania (EWGSOP1) and the lowest in Europe (EWGSOP2). Women had a higher prevalence according the IWGS (17% vs. 12%), and men when employing the EWGSOP2 (11% vs. 2%). Our study found that men showed a higher prevalence of sarcopenia under all the operational diagnostic criteria, and the greater difference was observed when EWGSOP2 (4% vs. 4%) and AWGS-2019 (5% vs. 2%) were followed.
The Portuguese SARC-F showed acceptable internal consistency (Cronbach α value = 0.82), which is in line with those described by other validations such as the Spanish [
29], the Romanian [
46], or the Polish versions [
41] (Cronbach α values of 0.78, 0.76, and 0.7, respectively), while on the other hand, lower internal consistency was obtained in the Italian [
26] or the Japanese [
23] versions of the SARC-F (Cronbach α values of 0.67 and 0.61, respectively). Previous SARC-F validations have found significant item-to-total correlations, with the items 2 (assistance with walking) and 1 (strength) showing the lowest and the highest correlations, respectively [
19,
41]. In the present study, the analysis showed that all the questions of the SARC-F significantly correlated with the total score, where a higher correlation was observed for the question 4 (climbing stairs) and lower correlations for questions 2 (assistance with walking) and 5 (falls).
In order to assess test–retest reliability, the Portuguese SARC-F was administered again to a subsample of 20 participants after two weeks. This time interval was recommended by the EuGMS [
22] and used in previous SARC-F validations. Our analysis revealed substantial to excellent ICC values for the SARC-F questions, with an ICC of 0.89 for the SARC-F total score. These findings are similar but slightly lower than the values described by Krzymińska-Siemaszko et al. [
41] in the Polish validation (ICC = 0.923), but higher than those indicated by Parra-Rodríguez et al. [
19] in the Spanish validation for Mexican population, and by Beaudart et al. [
47] in the French version (ICC values of 0.80 and 0.86, respectively). Our findings also revealed an excellent inter-rater reliability for the Portuguese SARC-F total score, which is in agreement with other validation studies [
25,
41].
With regard to the clinical validation of the Portuguese SARC-F, our results showed lower values of sensitivity but greater specificity in the diagnosis of sarcopenia under the five diagnosis criteria. Additionally, weak positive predictive values were found, as well as high negative predictive values. These results are in agreement with the findings described in previous validation studies [
19,
25,
41,
47] and confirm the Portuguese SARC-F as a valid and capable tool for determining the absence of sarcopenia. The Portuguese SARC-F scores could be considered as low, especially in men, where all total scores were <4, and regarding the items, the highest score observed was two and only on one occasion (item 4, climb stairs). This could be due to the high level of physical functioning of the participants, which may also influence the low prevalence of sarcopenia and may have an effect on our results.
As for the comparison between the SARC-F total score and other parameters related to sarcopenia and body composition, significant correlations have been described [
24]. Our results are in line with those described by Kera et al. [
23] and by Krzymińska-Siemaszko et al. [
41] in the Japanese and Polish study validations, respectively, and showed significant correlations with all the studied variables, except for the ASMI values. When analyzing the discriminant ability of the SARC-F with low muscle mass (according the EWGSOP2 criteria), the AUC was low (0.52), which could be explained by the low percentage of participants with low ASMI (10%). But on the other hand, our results showed that the Portuguese SARC-F was able to distinguish between people with low handgrip strength (probable sarcopenia) and low gait speed (which indicates severity) with AUC of 0.78 and 0.89, respectively, which indicate moderate accuracy level. These results could be influenced by the proportion of men and women in this study, given that significant gender-related differences regarding handgrip strength, muscle mass, and fat-mass percentage were observed.
Some limitations of the present study should be considered. Bioelectrical impedance analysis, although it is supported by study groups such as the EWGSOP 1 and 2 or the AGWS, is not the most accurate method to determine muscle mass as compared to magnetic resonance imaging, computed tomography, or dual-energy X-ray absorptiometry, but it is recommended in the usual clinical care for its affordability and portability [
5]. On the other hand, since the study was conducted on older adults from a specific geographical location, with only 27% of men, and thus, any generalization of these findings should be limited to people with similar characteristics, and future studies should be carried out on a general sample with a more balanced ratio between men and women from different geographical regions.

 ,
, 



{kind=link}
{kind=link}