

Moderate Alcohol Consumption Increases the Risk of Clinical Relapse in Male Depressed Patients Treated with Serotonin-Norepinephrine Reuptake Inhibitors


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
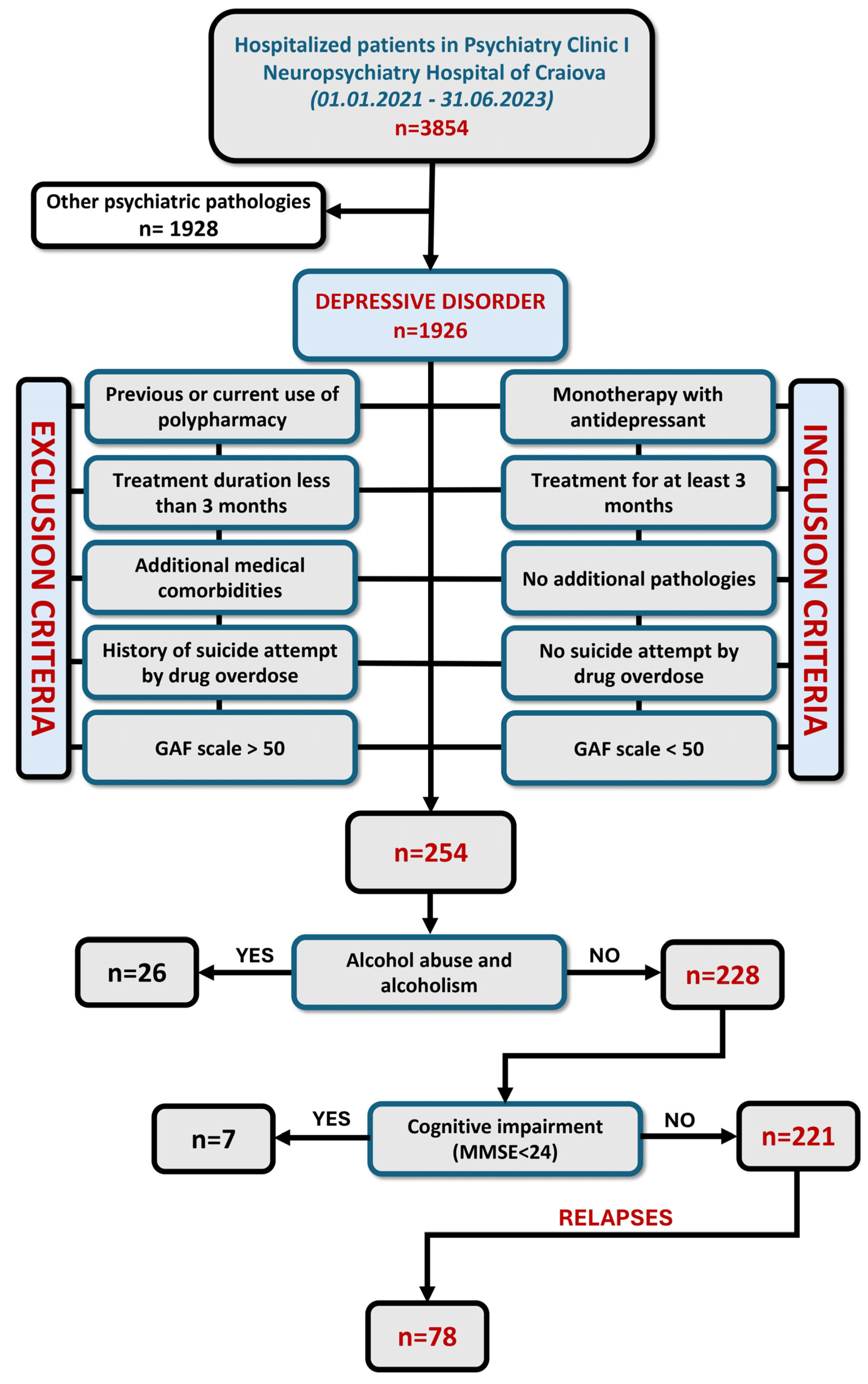
2.1. Sample
2.2. Inclusion and Exclusion Criteria
2.3. Antidepressant Treatment
2.4. Clinical and Biochemical Evaluations
2.5. Statistical Analysis
3. Results
3.1. No Differences in Relapse Were Observed in Depressive Patients, Regardless of Liver Enzyme Levels
3.2. SNRI Treatment Should Be Avoided in Patients with Any Type of Alcohol Consumption
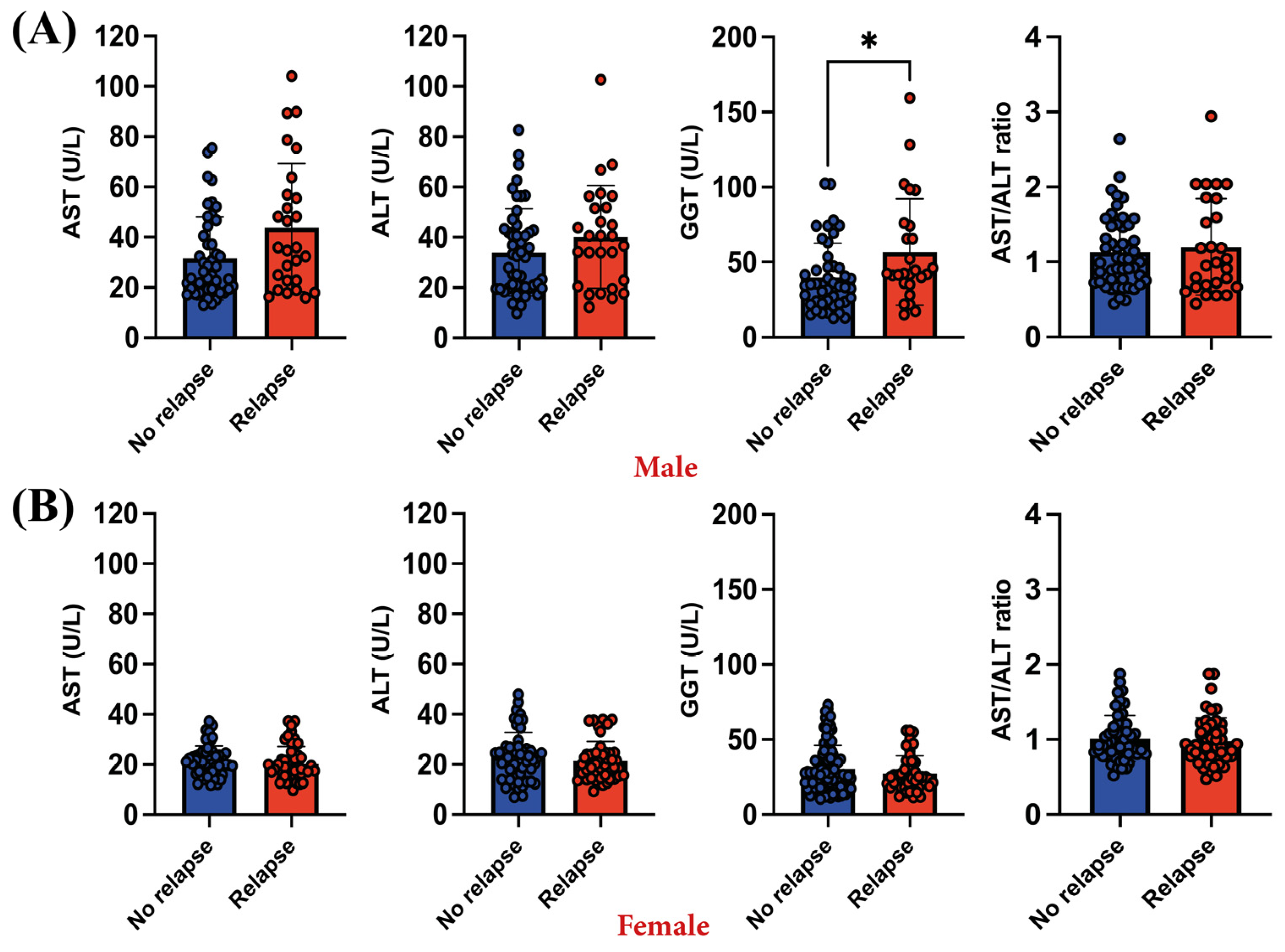
3.3. Relapsing Male Patients Exhibid Higher GGT Levels Compared to Those without Any Relapse Episode
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Carney, R.M.; Freedland, K.E.; Miller, G.E.; Jaffe, A.S. Depression as a risk factor for cardiac mortality and morbidity: A review of potential mechanisms. J. Psychosom. Res. 2002, 53, 897–902. [Google Scholar] [CrossRef] [PubMed]
- Mora, C.; Zonca, V.; Riva, M.A.; Cattaneo, A. Blood biomarkers and treatment response in major depression. Expert. Rev. Mol. Diagn. 2018, 18, 513–529. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.H.; Yen, Y.C.; Chen, M.C.; Chen, C.C. Depression and pain impair daily functioning and quality of life in patients with major depressive disorder. J. Affect. Disord. 2014, 166, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Lerner, D.; Adler, D.A.; Rogers, W.H.; Chang, H.; Lapitsky, L.; McLaughlin, T.; Reed, J. Work performance of employees with depression: The impact of work stressors. Am. J. Health Promot. 2010, 24, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Goodman, R.J.; Samek, D.R.; Wilson, S.; Iacono, W.G.; McGue, M. Close relationships and depression: A developmental cascade approach. Dev. Psychopathol. 2019, 31, 1451–1465. [Google Scholar] [CrossRef]
- Cho, Y.; Lee, J.K.; Kim, D.H.; Park, J.H.; Choi, M.; Kim, H.J.; Nam, M.J.; Lee, K.U.; Han, K.; Park, Y.G. Factors associated with quality of life in patients with depression: A nationwide population-based study. PLoS ONE 2019, 14, e0219455. [Google Scholar] [CrossRef] [PubMed]
- Orsolini, L.; Latini, R.; Pompili, M.; Serafini, G.; Volpe, U.; Vellante, F.; Fornaro, M.; Valchera, A.; Tomasetti, C.; Fraticelli, S.; et al. Understanding the Complex of Suicide in Depression: From Research to Clinics. Psychiatry Investig. 2020, 17, 207–221. [Google Scholar] [CrossRef] [PubMed]
- Cai, H.; Xie, X.M.; Zhang, Q.; Cui, X.; Lin, J.X.; Sim, K.; Ungvari, G.S.; Zhang, L.; Xiang, Y.T. Prevalence of Suicidality in Major Depressive Disorder: A Systematic Review and Meta-Analysis of Comparative Studies. Front. Psychiatry 2021, 12, 690130. [Google Scholar] [CrossRef]
- Nock, M.K.; Hwang, I.; Sampson, N.A.; Kessler, R.C. Mental disorders, comorbidity and suicidal behavior: Results from the National Comorbidity Survey Replication. Mol. Psychiatry 2010, 15, 868–876. [Google Scholar] [CrossRef]
- Rubio-Guerra, A.F.; Rodriguez-Lopez, L.; Vargas-Ayala, G.; Huerta-Ramirez, S.; Serna, D.C.; Lozano-Nuevo, J.J. Depression increases the risk for uncontrolled hypertension. Exp. Clin. Cardiol. 2013, 18, 10–12. [Google Scholar]
- Bădescu, S.V.; Tătaru, C.; Kobylinska, L.; Georgescu, E.L.; Zahiu, D.M.; Zăgrean, A.M.; Zăgrean, L. The association between Diabetes mellitus and Depression. J. Med. Life 2016, 9, 120–125. [Google Scholar] [PubMed]
- Ma, H.; Wang, Y.; Xue, Y.; Huang, D.; Kong, Y.; Zhao, X.; Zhang, M. The effect of Xinkeshu tablets on depression and anxiety symptoms in patients with coronary artery disease: Results from a double-blind, randomized, placebo-controlled study. Biomed. Pharmacother. 2019, 112, 108639. [Google Scholar] [CrossRef] [PubMed]
- Xiao, J.; Lim, L.K.E.; Ng, C.H.; Tan, D.J.H.; Lim, W.H.; Ho, C.S.H.; Tan, E.X.X.; Sanyal, A.J.; Muthiah, M.D. Is Fatty Liver Associated With Depression? A Meta-Analysis and Systematic Review on the Prevalence, Risk Factors, and Outcomes of Depression and Non-alcoholic Fatty Liver Disease. Front. Med. 2021, 8, 691696. [Google Scholar] [CrossRef]
- Ng, C.H.; Xiao, J.; Chew, N.W.S.; Chin, Y.H.; Chan, K.E.; Quek, J.; Lim, W.H.; Tan, D.J.H.; Loke, R.W.K.; Tan, C.; et al. Depression in non-alcoholic fatty liver disease is associated with an increased risk of complications and mortality. Front. Med. 2022, 9, 985803. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Park, S.H. Association between depression and nonalcoholic fatty liver disease: Contributions of insulin resistance and inflammation. J. Affect. Disord. 2021, 278, 259–263. [Google Scholar] [CrossRef] [PubMed]
- Ueberberg, B.; Frommberger, U.; Messer, T.; Zwanzger, P.; Kuhn, J.; Anghelescu, I.; Ackermann, K.; Assion, H.J. Drug-Induced Liver Injury (DILI) in Patients with Depression Treated with Antidepressants: A Retrospective Multicenter Study. Pharmacopsychiatry 2020, 53, 60–64. [Google Scholar] [CrossRef] [PubMed]
- Voican, C.S.; Corruble, E.; Naveau, S.; Perlemuter, G. Antidepressant-induced liver injury: A review for clinicians. Am. J. Psychiatry 2014, 171, 404–415. [Google Scholar] [CrossRef] [PubMed]
- Park, S.H.; Ishino, R. Liver injury associated with antidepressants. Curr. Drug Saf. 2013, 8, 207–223. [Google Scholar] [CrossRef] [PubMed]
- Todorović Vukotić, N.; Đorđević, J.; Pejić, S.; Đorđević, N.; Pajović, S.B. Antidepressants- and antipsychotics-induced hepatotoxicity. Arch. Toxicol. 2021, 95, 767–789. [Google Scholar] [CrossRef]
- Fang, L.; Wang, S.; Cao, L.; Yao, K. Early intervention of acute liver injury related to venlafaxine: A case report. Medicine 2021, 100, e28140. [Google Scholar] [CrossRef]
- Voican, C.S.; Martin, S.; Verstuyft, C.; Corruble, E.; Perlemuter, G.; Colle, R. Liver Function Test Abnormalities in Depressed Patients Treated with Antidepressants: A Real-World Systematic Observational Study in Psychiatric Settings. PLoS ONE 2016, 11, e0155234. [Google Scholar] [CrossRef] [PubMed]
- Qiu, J.; Kuang, M.; He, S.; Yu, C.; Wang, C.; Huang, X.; Sheng, G.; Zou, Y. Gender perspective on the association between liver enzyme markers and non-alcoholic fatty liver disease: Insights from the general population. Front. Endocrinol. 2023, 14, 1302322. [Google Scholar] [CrossRef] [PubMed]
- Aithal, G.P.; Watkins, P.B.; Andrade, R.J.; Larrey, D.; Molokhia, M.; Takikawa, H.; Hunt, C.M.; Wilke, R.A.; Avigan, M.; Kaplowitz, N.; et al. Case definition and phenotype standardization in drug-induced liver injury. Clin. Pharmacol. Ther. 2011, 89, 806–815. [Google Scholar] [CrossRef] [PubMed]
- Conigrave, K.M.; Degenhardt, L.J.; Whitfield, J.B.; Saunders, J.B.; Helander, A.; Tabakoff, B. CDT, GGT, and AST as markers of alcohol use: The WHO/ISBRA collaborative project. Alcohol. Clin. Exp. Res. 2002, 26, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Whitfield, J.B. Gamma glutamyl transferase. Crit. Rev. Clin. Lab. Sci. 2001, 38, 263–355. [Google Scholar] [CrossRef]
- Ghosh, S.; Jain, R.; Rao, R.; Jhanjee, S.; Mishra, A.K. Alcohol Biomarkers and their Relevance in Detection of Alcohol Consumption in Clinical Settings. Int. Arch. Subst. Abus. Rehabil. 2019, 1, 1–8. [Google Scholar] [CrossRef]
- Young-Wolff, K.C.; Kendler, K.S.; Sintov, N.D.; Prescott, C.A. Mood-related drinking motives mediate the familial association between major depression and alcohol dependence. Alcohol. Clin. Exp. Res. 2009, 33, 1476–1486. [Google Scholar] [CrossRef] [PubMed]
- Turner, S.; Mota, N.; Bolton, J.; Sareen, J. Self-medication with alcohol or drugs for mood and anxiety disorders: A narrative review of the epidemiological literature. Depress. Anxiety 2018, 35, 851–860. [Google Scholar] [CrossRef]
- Driessen, M.; Meier, S.; Hill, A.; Wetterling, T.; Lange, W.; Junghanns, K. The course of anxiety, depression and drinking behaviours after completed detoxification in alcoholics with and without comorbid anxiety and depressive disorders. Alcohol. Alcohol. 2001, 36, 249–255. [Google Scholar] [CrossRef]
- Kuehner, C. Why is depression more common among women than among men? Lancet Psychiatry 2017, 4, 146–158. [Google Scholar] [CrossRef]
- White, A.M. Gender Differences in the Epidemiology of Alcohol Use and Related Harms in the United States. Alcohol. Res. 2020, 40, 1. [Google Scholar] [CrossRef] [PubMed]
- Al-Rousan, T.; Moore, A.A.; Han, B.H.; Ko, R.; Palamar, J.J. Trends in binge drinking prevalence among older U.S. men and women, 2015 to 2019. J. Am. Geriatr. Soc. 2022, 70, 812–819. [Google Scholar] [CrossRef] [PubMed]
- Kawaida, K.; Yoshimoto, H.; Morita, N.; Ogai, Y.; Saito, T. The Prevalence of Binge Drinking and Alcohol-Related Consequences and their Relationship among Japanese College Students. Tohoku J. Exp. Med. 2021, 254, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Erol, A.; Karpyak, V.M. Sex and gender-related differences in alcohol use and its consequences: Contemporary knowledge and future research considerations. Drug Alcohol. Depend. 2015, 156, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Mitkin, N.A.; Unguryanu, T.N.; Malyutina, S.; Kudryavtsev, A.V. Association between Alcohol Consumption and Body Composition in Russian Adults and Patients Treated for Alcohol-Related Disorders: The Know Your Heart Cross-Sectional Study. Int. J. Environ. Res. Public. Health 2023, 20, 2905. [Google Scholar] [CrossRef] [PubMed]
- Thomasson, H. Gender Differences in Alcohol Metabolism; Springer: Berlin/Heidelberg, Germany, 2002; pp. 163–179. [Google Scholar]
- Sudhinaraset, M.; Wigglesworth, C.; Takeuchi, D.T. Social and Cultural Contexts of Alcohol Use: Influences in a Social-Ecological Framework. Alcohol. Res. 2016, 38, 35–45. [Google Scholar] [PubMed]
- Alsheikh, A.M.; Elemam, M.O.; El-Bahnasawi, M. Treatment of Depression With Alcohol and Substance Dependence: A Systematic Review. Cureus 2020, 12, e11168. [Google Scholar] [CrossRef] [PubMed]
- Cornelius, J.R.; Chung, T.; Douaihy, A.B.; Kirisci, L.; Glance, J.; Kmiec, J.; FitzGerald, D.; Wesesky, M.A.; Salloum, I. Mirtazapine in comorbid major depression and an alcohol use disorder: A double-blind placebo-controlled pilot trial. Psychiatry Res. 2016, 242, 326–330. [Google Scholar] [CrossRef] [PubMed]
- Liappas, J.; Paparrigopoulos, T.; Tzavellas, E.; Rabavilas, A. Mirtazapine and venlafaxine in the management of collateral psychopathology during alcohol detoxification. Prog. Neuropsychopharmacol. Biol. Psychiatry 2005, 29, 55–60. [Google Scholar] [CrossRef]
- Le Bon, O.; Murphy, J.R.; Staner, L.; Hoffmann, G.; Kormoss, N.; Kentos, M.; Dupont, P.; Lion, K.; Pelc, I.; Verbanck, P. Double-blind, placebo-controlled study of the efficacy of trazodone in alcohol post-withdrawal syndrome: Polysomnographic and clinical evaluations. J. Clin. Psychopharmacol. 2003, 23, 377–383. [Google Scholar] [CrossRef]
- Friedmann, P.D.; Rose, J.S.; Swift, R.; Stout, R.L.; Millman, R.P.; Stein, M.D. Trazodone for sleep disturbance after alcohol detoxification: A double-blind, placebo-controlled trial. Alcohol. Clin. Exp. Res. 2008, 32, 1652–1660. [Google Scholar] [CrossRef]
- Book, S.W.; Thomas, S.E.; Randall, P.K.; Randall, C.L. Paroxetine reduces social anxiety in individuals with a co-occurring alcohol use disorder. J. Anxiety Disord. 2008, 22, 310–318. [Google Scholar] [CrossRef] [PubMed]
- Cornelius, J.R.; Bukstein, O.G.; Birmaher, B.; Salloum, I.M.; Lynch, K.; Pollock, N.K.; Gershon, S.; Clark, D. Fluoxetine in adolescents with major depression and an alcohol use disorder: An open-label trial. Addict. Behav. 2001, 26, 735–739. [Google Scholar] [CrossRef] [PubMed]
- Pettinati, H.M.; Volpicelli, J.R.; Kranzler, H.R.; Luck, G.; Rukstalis, M.R.; Cnaan, A. Sertraline treatment for alcohol dependence: Interactive effects of medication and alcoholic subtype. Alcohol. Clin. Exp. Res. 2000, 24, 1041–1049. [Google Scholar] [CrossRef] [PubMed]
- Kranzler, H.R.; Burleson, J.A.; Brown, J.; Babor, T.F. Fluoxetine treatment seems to reduce the beneficial effects of cognitive-behavioral therapy in type B alcoholics. Alcohol. Clin. Exp. Res. 1996, 20, 1534–1541. [Google Scholar] [CrossRef]
- Moriarty, A.S.; Castleton, J.; Gilbody, S.; McMillan, D.; Ali, S.; Riley, R.D.; Chew-Graham, C.A. Predicting and preventing relapse of depression in primary care. Br. J. Gen. Pract. 2020, 70, 54–55. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The ICD-10 Classification of Mental and Behavioural Disorders: Clinical Descriptions and Diagnostic Guidelines; World Health Organization: Geneva, Switzerland, 1992; Available online: https://www.who.int/publications/i/item/9241544228 (accessed on 8 April 2024).
- Dufour, M.C. What is moderate drinking? Defining “drinks” and drinking levels. Alcohol. Res. Health 1999, 23, 5–14. [Google Scholar] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Arevalo-Rodriguez, I.; Smailagic, N.; Roqué-Figuls, M.; Ciapponi, A.; Sanchez-Perez, E.; Giannakou, A.; Pedraza, O.L.; Bonfill Cosp, X.; Cullum, S. Mini-Mental State Examination (MMSE) for the early detection of dementia in people with mild cognitive impairment (MCI). Cochrane Database Syst. Rev. 2021, 7, Cd010783. [Google Scholar] [CrossRef] [PubMed]
- Aas, I.H.M.; Sonesson, O.; Torp, S. A Qualitative Study of Clinicians Experience with Rating of the Global Assessment of Functioning (GAF) Scale. Community Ment. Health J. 2018, 54, 107–116. [Google Scholar] [CrossRef]
- Nuggerud-Galeas, S.; Sáez-Benito Suescun, L.; Berenguer Torrijo, N.; Sáez-Benito Suescun, A.; Aguilar-Latorre, A.; Magallón Botaya, R.; Oliván Blázquez, B. Analysis of depressive episodes, their recurrence and pharmacologic treatment in primary care patients: A retrospective descriptive study. PLoS ONE 2020, 15, e0233454. [Google Scholar] [CrossRef] [PubMed]
- Burcusa, S.L.; Iacono, W.G. Risk for recurrence in depression. Clin. Psychol. Rev. 2007, 27, 959–985. [Google Scholar] [CrossRef] [PubMed]
- Poikolainen, K. Underestimation of recalled alcohol intake in relation to actual consumption. Br. J. Addict. 1985, 80, 215–216. [Google Scholar] [CrossRef] [PubMed]
- Gilligan, C.; Anderson, K.G.; Ladd, B.O.; Yong, Y.M.; David, M. Inaccuracies in survey reporting of alcohol consumption. BMC Public. Health 2019, 19, 1639. [Google Scholar] [CrossRef] [PubMed]
- Embree, B.G.; Whitehead, P.C. Validity and reliability of self-reported drinking behavior: Dealing with the problem of response bias. J. Stud. Alcohol. 1993, 54, 334–344. [Google Scholar] [CrossRef] [PubMed]
- Grüner Nielsen, D.; Andersen, K.; Søgaard Nielsen, A.; Juhl, C.; Mellentin, A. Consistency between self-reported alcohol consumption and biological markers among patients with alcohol use disorder—A systematic review. Neurosci. Biobehav. Rev. 2021, 124, 370–385. [Google Scholar] [CrossRef] [PubMed]
- Del Boca, F.K.; Darkes, J. The validity of self-reports of alcohol consumption: State of the science and challenges for research. Addiction 2003, 98 (Suppl. S2), 1–12. [Google Scholar] [CrossRef] [PubMed]
- Archer, M.; Kampman, O.; Bloigu, A.; Bloigu, R.; Luoto, K.; Kultti, J.; Hämäläinen, M.; Moilanen, E.; Leinonen, E.; Niemelä, O. Assessment of alcohol consumption in depression follow-up using self-reports and blood measures including inflammatory biomarkers. Alcohol. Alcohol. 2019, 54, 243–250. [Google Scholar] [CrossRef]
- Niederhofer, H.; Staffen, W.; Mair, A. Tianeptine may be a useful adjunct in the treatment of alcohol dependence of adolescents. Alcohol. Clin. Exp. Res. 2003, 27, 136. [Google Scholar] [CrossRef]
- Lôo, H.; Malka, R.; Defrance, R.; Barrucand, D.; Benard, J.Y.; Niox-Rivière, H.; Raab, A.; Sarda, A.; Vachonfrance, G.; Kamoun, A. Tianeptine and amitriptyline. Controlled double-blind trial in depressed alcoholic patients. Neuropsychobiology 1988, 19, 79–85. [Google Scholar] [CrossRef]
- Vuković, O.; Marić, N.P.; Britvić, D.; Cvetić, T.; Damjanović, A.; Prostran, M.; Jasović-Gasić, M. Efficacy, tolerability and safety of tianeptine in special populations of depressive patients. Psychiatr. Danub. 2009, 21, 194–198. [Google Scholar] [PubMed]
- Correia, J.P.; Alves, P.S.; Camilo, E.A. SGOT-SGPT ratios. Dig. Dis. Sci. 1981, 26, 284. [Google Scholar] [CrossRef] [PubMed]
- Salaspuro, M. Use of enzymes for the diagnosis of alcohol-related organ damage. Enzyme 1987, 37, 87–107. [Google Scholar] [CrossRef] [PubMed]
- Graham, K.; Massak, A. Alcohol consumption and the use of antidepressants. Can. Med Assoc. J. 2007, 176, 633–637. [Google Scholar] [CrossRef] [PubMed]
- Liappas, I.A.; Piperi, C.; Malitas, P.N.; Tzavellas, E.O.; Liappas, A.I.; Boufidou, F.; Kalofoutis, C.A.; Bagos, P.; Rabavilas, A.; Kalofoutis, A. Correlation of liver dysfunction biological markers to the mood status of alcohol-dependent individuals. Int. J. Psychiatry Clin. Pract. 2006, 10, 166–173. [Google Scholar] [CrossRef] [PubMed]
- Savage, K.; Porter, C.; Bunnett, E.; Hana, M.; Keegan, A.; Ogden, E.; Stough, C.; Pipingas, A. Liver and inflammatory biomarker relationships to depression symptoms in healthy older adults. Exp. Gerontol. 2023, 177, 112186. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Mao, Y.; Zhu, S.; Ma, J.; Gao, S.; Jin, X.; Wei, Z.; Geng, Y. Relationship between depressive disorders and biochemical indicators in adult men and women. BMC Psychiatry 2023, 23, 49. [Google Scholar] [CrossRef] [PubMed]
- McIntyre, R.S.; Panjwani, Z.D.; Nguyen, H.T.; Woldeyohannes, H.O.; Alsuwaidan, M.; Soczynska, J.K.; Lourenco, M.T.; Konarski, J.Z.; Kennedy, S.H. The hepatic safety profile of duloxetine: A review. Expert. Opin. Drug Metab. Toxicol. 2008, 4, 281–285. [Google Scholar] [CrossRef] [PubMed]
- Wernicke, J.; Acharya, N.; Strombom, I.; Gahimer, J.L.; D’Souza, D.N.; DiPietro, N.; Uetrecht, J.P. Hepatic effects of duloxetine-II: Spontaneous reports and epidemiology of hepatic events. Curr. Drug Saf. 2008, 3, 143–153. [Google Scholar] [CrossRef]
- Wernicke, J.; Pangallo, B.; Wang, F.; Murray, I.; Henck, J.W.; Knadler, M.P.; D’Souza, D.N.; Uetrecht, J.P. Hepatic effects of duloxetine-I: Non-clinical and clinical trial data. Curr. Drug Saf. 2008, 3, 132–142. [Google Scholar] [CrossRef]
- Friedrich, M.E.; Akimova, E.; Huf, W.; Konstantinidis, A.; Papageorgiou, K.; Winkler, D.; Toto, S.; Greil, W.; Grohmann, R.; Kasper, S. Drug-Induced Liver Injury during Antidepressant Treatment: Results of AMSP, a Drug Surveillance Program. Int. J. Neuropsychopharmacol. 2016, 19, pyv126. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, A.F.; Sharma, M.S.; Brunoni, A.R.; Vieta, E.; Fava, G.A. The Safety, Tolerability and Risks Associated with the Use of Newer Generation Antidepressant Drugs: A Critical Review of the Literature. Psychother. Psychosom. 2016, 85, 270–288. [Google Scholar] [CrossRef] [PubMed]
- Janiri, L.; Hadjichristos, A.; Buonanno, A.; Rago, R.; Mannelli, P.; de Risio, S. Adjuvant trazodone in the treatment of alcoholism: An open study. Alcohol. Alcohol. 1998, 33, 362–365. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Lv, T.; Wu, J.; Lyu, Y. Trazodone changed the polysomnographic sleep architecture in insomnia disorder: A systematic review and meta-analysis. Sci. Rep. 2022, 12, 14453. [Google Scholar] [CrossRef]
- Peterson, M.J.; Benca, R.M. Sleep in mood disorders. Psychiatr. Clin. North. Am. 2006, 29, 1009–1032. [Google Scholar] [CrossRef] [PubMed]
- Baglioni, C.; Battagliese, G.; Feige, B.; Spiegelhalder, K.; Nissen, C.; Voderholzer, U.; Lombardo, C.; Riemann, D. Insomnia as a predictor of depression: A meta-analytic evaluation of longitudinal epidemiological studies. J. Affect. Disord. 2011, 135, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Brower, K.J. Alcohol’s effects on sleep in alcoholics. Alcohol. Res. Health 2001, 25, 110–125. [Google Scholar] [PubMed]
- Roehrs, T.; Roth, T. Sleep, sleepiness, and alcohol use. Alcohol. Res. Health 2001, 25, 101–109. [Google Scholar] [PubMed]
- Borras, L.; de Timary, P.; Constant, E.L.; Huguelet, P.; Eytan, A. Successful treatment of alcohol withdrawal with trazodone. Pharmacopsychiatry 2006, 39, 232. [Google Scholar] [CrossRef]
- Noble, R.E. Depression in women. Metabolism 2005, 54, 49–52. [Google Scholar] [CrossRef]
- Albert, P.R. Why is depression more prevalent in women? J. Psychiatry Neurosci. 2015, 40, 219–221. [Google Scholar] [CrossRef] [PubMed]
- Yuan, W.; Hesketh, T. Intimate Partner Violence and Depression in Women in China. J. Interpers. Violence 2021, 36, Np12016–Np12040. [Google Scholar] [CrossRef] [PubMed]
- Lövestad, S.; Löve, J.; Vaez, M.; Krantz, G. Prevalence of intimate partner violence and its association with symptoms of depression; a cross-sectional study based on a female population sample in Sweden. BMC Public. Health 2017, 17, 335. [Google Scholar] [CrossRef]
- Kundakovic, M.; Rocks, D. Sex hormone fluctuation and increased female risk for depression and anxiety disorders: From clinical evidence to molecular mechanisms. Front. Neuroendocrinol. 2022, 66, 101010. [Google Scholar] [CrossRef] [PubMed]
- Kelmendi, K.; Jemini-Gashi, L. An Exploratory Study of Gender Role Stress and Psychological Distress of Women in Kosovo. Womens Health 2022, 18, 17455057221097823. [Google Scholar] [CrossRef] [PubMed]
- Livingston, M.; Callinan, S. Underreporting in Alcohol Surveys: Whose Drinking Is Underestimated? J. Stud. Alcohol Drugs 2015, 76, 158–167. [Google Scholar] [CrossRef] [PubMed]
- Mușat, M.I.; Militaru, F.; Udriștoiu, I.; Mitran, S.I.; Cătălin, B. Alcohol Consumption Is a Coping Mechanism for Male Patients with Severe Anxiety Disorders Treated with Antidepressants Monotherapy. J. Clin. Med. 2024, 13, 2723. [Google Scholar] [CrossRef] [PubMed]
- Osborne, A.K.; Wilson-Menzfeld, G.; McGill, G.; Kiernan, M.D. Military service and alcohol use: A systematic narrative review. Occup. Med. 2022, 72, 313–323. [Google Scholar] [CrossRef] [PubMed]
- D’Aquino, S.; Callinan, S. Drinking to cope as a mediator of the relationship between stress and alcohol outcomes. Drugs Educ. Prev. Policy 2023, 1–8. [Google Scholar] [CrossRef]
- Foster, D.W.; Young, C.M.; Steers, M.; Quist, M.C.; Bryan, J.L.; Neighbors, C. Tears in your beer: Gender differences in coping drinking motives, depressive symptoms and drinking. Int. J. Ment. Health Addict. 2014, 12, 730–746. [Google Scholar] [CrossRef]
- Poustchi, H.; George, J.; Esmaili, S.; Esna-Ashari, F.; Ardalan, G.; Sepanlou, S.G.; Alavian, S.M. Gender differences in healthy ranges for serum alanine aminotransferase levels in adolescence. PLoS ONE 2011, 6, e21178. [Google Scholar] [CrossRef] [PubMed]
- Balakrishnan, M.; Patel, P.; Dunn-Valadez, S.; Dao, C.; Khan, V.; Ali, H.; El-Serag, L.; Hernaez, R.; Sisson, A.; Thrift, A.P.; et al. Women Have a Lower Risk of Nonalcoholic Fatty Liver Disease but a Higher Risk of Progression vs Men: A Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2021, 19, 61–71.e15. [Google Scholar] [CrossRef] [PubMed]
- Eng, P.C.; Forlano, R.; Tan, T.; Manousou, P.; Dhillo, W.S.; Izzi-Engbeaya, C. Non-alcoholic fatty liver disease in women—Current knowledge and emerging concepts. JHEP Rep. 2023, 5, 100835. [Google Scholar] [CrossRef] [PubMed]
- Berlanga, C.; Flores-Ramos, M. Different gender response to serotonergic and noradrenergic antidepressants. A comparative study of the efficacy of citalopram and reboxetine. J. Affect. Disord. 2006, 95, 119–123. [Google Scholar] [CrossRef] [PubMed]
- Kornstein, S.G.; Wohlreich, M.M.; Mallinckrodt, C.H.; Watkin, J.G.; Stewart, D.E. Duloxetine efficacy for major depressive disorder in male vs. female patients: Data from 7 randomized, double-blind, placebo-controlled trials. J. Clin. Psychiatry 2006, 67, 761–770. [Google Scholar] [CrossRef] [PubMed]
- Entsuah, A.R.; Huang, H.; Thase, M.E. Response and remission rates in different subpopulations with major depressive disorder administered venlafaxine, selective serotonin reuptake inhibitors, or placebo. J. Clin. Psychiatry 2001, 62, 869–877. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, S.J.; Hilmer, S.N. Drug-induced liver injury in older adults. Ther. Adv. Drug Saf. 2010, 1, 65–77. [Google Scholar] [CrossRef] [PubMed]
- Boschloo, L.; Vogelzangs, N.; van den Brink, W.; Smit, J.H.; Veltman, D.J.; Beekman, A.T.; Penninx, B.W. Alcohol use disorders and the course of depressive and anxiety disorders. Br. J. Psychiatry 2012, 200, 476–484. [Google Scholar] [CrossRef] [PubMed]
- McHugh, R.K.; Weiss, R.D. Alcohol Use Disorder and Depressive Disorders. Alcohol. Res. 2019, 40, 1–8. [Google Scholar] [CrossRef]
- Upadhyaya, H.P.; Brady, K.T.; Sethuraman, G.; Sonne, S.C.; Malcolm, R. Venlafaxine treatment of patients with comorbid alcohol/cocaine abuse and attention-deficit/hyperactivity disorder: A pilot study. J. Clin. Psychopharmacol. 2001, 21, 116–118. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| AST Blood Levels | ALT Blood Levels | AST/ALT Ratio | GGT Blood Levels | ||
|---|---|---|---|---|---|
| Normal Values | 1–40 U/L | 1–41 U/L | <1.1 | 1–38 U/L | |
| Descriptive statistics of the studied population | Mean | 29.24 | 28.75 | 1.07 | 40.93 |
| Std. Deviation | 20.1 | 16.4 | 0.4 | 32.1 | |
| Minimum | 9.8 | 5.5 | 0.4 | 10.4 | |
| Maximum | 116.5 | 102.7 | 3.2 | 180.2 | |
| Range | 106.7 | 97.2 | 2.8 | 169.8 | |
| Skewness | 2.2 | 1.4 | 1.6 | 2.2 | |
| Kurtosis | 4.9 | 2.5 | 3.7 | 5.5 | |
| Test for normal distribution D’Agostino & Pearson test | K2 | 110.9 | 64.6 | 79.4 | 114.5 |
| p value | <0.0001 | <0.0001 | <0.0001 | <0.0001 | |
| Passed normality test (alpha = 0.05)? | No | No | No | No | |
| Total | SSRI | SNRI | TCA | SARI | NaSSA | ||
|---|---|---|---|---|---|---|---|
| Included patients | No. of patients | 221 | 72 | 40 | 34 | 61 | 14 |
| Mean age (years) | 53.99 ± 8.94 | 53.19 ± 8.15 | 54.58 ± 8.93 | 51.50 ± 9.37 | 54.97 ± 9.72 | 58.14 ± 6.87 | |
| Gender Distribution (M:F) | 76:145 | 13:59 | 18:22 | 18:16 | 23:38 | 4:10 | |
| No relapse | No. of patients | 143 | 44 | 23 | 21 | 45 | 10 |
| Mean age (years) | 53.52 ± 9.68 | 54.32 ± 7.60 | 54.17 ± 10.50 | 49.33 ± 10.56 | 53.87 ± 10.75 | 58.10 ± 7.34 | |
| Gender Distribution (M:F) | 49:94 | 10:34 | 9:14 | 10:11 | 18:27 | 2:8 | |
| Relapse episodes | No. of patients | 78 | 28 | 17 | 13 | 16 | 4 |
| Mean age (years) | 54.83 ± 7.36 | 51.46 ± 8.79 | 56.35 ± 6.04 | 55.00 ± 5.87 | 58.06 ± 5.05 | 58.50 ± 6.55 | |
| Gender Distribution (M:F) | 27:51 | 3:25 | 9:8 | 8:5 | 5:11 | 2:2 | |
| SSRI | SNRI | TCA | NaSSA | SARI | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| OR | p Value | OR | p Value | OR | p Value | OR | p Value | OR | p Value | |
| Elevated AST | 0.936 | 0.932 | 9.167 | 0.028 | 1.016 | 0.983 | INC. | INC. | 1.253 | 0.767 |
| Elevated ALT | 1.442 | 0.553 | 2.778 | 0.201 | 0.593 | 0.481 | INC. | INC. | 0.433 | 0.445 |
| Elevated GGT | 1.015 | 0.977 | 5.344 | 0.018 | 3.000 | 0.134 | INC. | INC. | 0.622 | 0.440 |
| Elevated AST/ALT | 0.889 | 0.831 | 1.545 | 0.530 | 0.467 | 0.297 | 0.778 | 0.852 | 0.750 | 0.630 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mușat, M.I.; Militaru, F.; Gheorman, V.; Udriștoiu, I.; Mitran, S.I.; Cătălin, B. Moderate Alcohol Consumption Increases the Risk of Clinical Relapse in Male Depressed Patients Treated with Serotonin-Norepinephrine Reuptake Inhibitors. Diagnostics 2024, 14, 1140. https://doi.org/10.3390/diagnostics14111140
Mușat MI, Militaru F, Gheorman V, Udriștoiu I, Mitran SI, Cătălin B. Moderate Alcohol Consumption Increases the Risk of Clinical Relapse in Male Depressed Patients Treated with Serotonin-Norepinephrine Reuptake Inhibitors. Diagnostics. 2024; 14(11):1140. https://doi.org/10.3390/diagnostics14111140
Chicago/Turabian StyleMușat, Mădălina Iuliana, Felicia Militaru, Victor Gheorman, Ion Udriștoiu, Smaranda Ioana Mitran, and Bogdan Cătălin. 2024. "Moderate Alcohol Consumption Increases the Risk of Clinical Relapse in Male Depressed Patients Treated with Serotonin-Norepinephrine Reuptake Inhibitors" Diagnostics 14, no. 11: 1140. https://doi.org/10.3390/diagnostics14111140
APA StyleMușat, M. I., Militaru, F., Gheorman, V., Udriștoiu, I., Mitran, S. I., & Cătălin, B. (2024). Moderate Alcohol Consumption Increases the Risk of Clinical Relapse in Male Depressed Patients Treated with Serotonin-Norepinephrine Reuptake Inhibitors. Diagnostics, 14(11), 1140. https://doi.org/10.3390/diagnostics14111140