


New Insights on Molecular Autopsy in Sudden Death: A Systematic Review
 , , , ,
, , , ,  ,
,  ,
,  and
and
Abstract
:1. Introduction
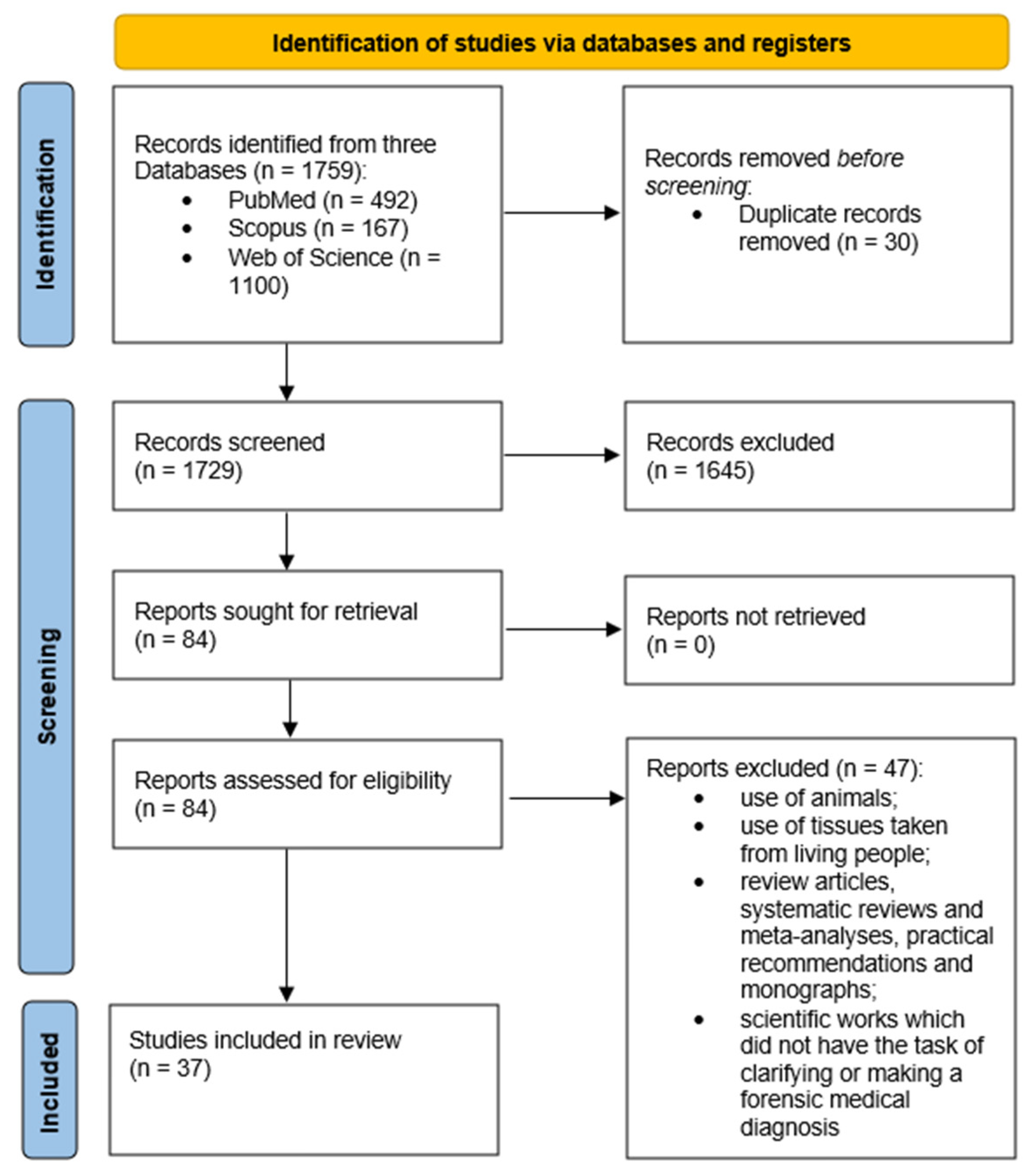
2. Materials and Methods
- Original articles or case studies;
- Non-violent deaths;
- Post-mortem genetic testing;
- Study of human tissues;
- Studies in which the purpose was to clarify or formulate a postmortem forensic diagnosis;
- Cases inclusive of sudden death in infants below 1 year of age (SIDS) and sudden death in infants between 1 and 5 years of age (SUDI) and SCD and SUDY, without specification of the number of each category, were included.
- Studies focused exclusively on SIDS—sudden death in infants below 1 year of age;
- Studies focused exclusively on SUDI—sudden death in infants between 1 and 5 years of age;
- Genetic studies performed on tissues taken from living people;
- Genetic studies on animal tissues;
- Genetic studies whose results were obtained in vitro, even if a database of post-mortem material from earlier studies was used to obtain them;
- Genetic studies aimed at identifying the DNA or RNA of infectious agents;
- Scientific works aimed at improving the technical approach to the use of the genetic testing method without the task of clarifying or making a forensic medical diagnosis;
- Review articles, systematic reviews, meta-analyses, practical recommendations, monographs, and commentary articles on previous research.
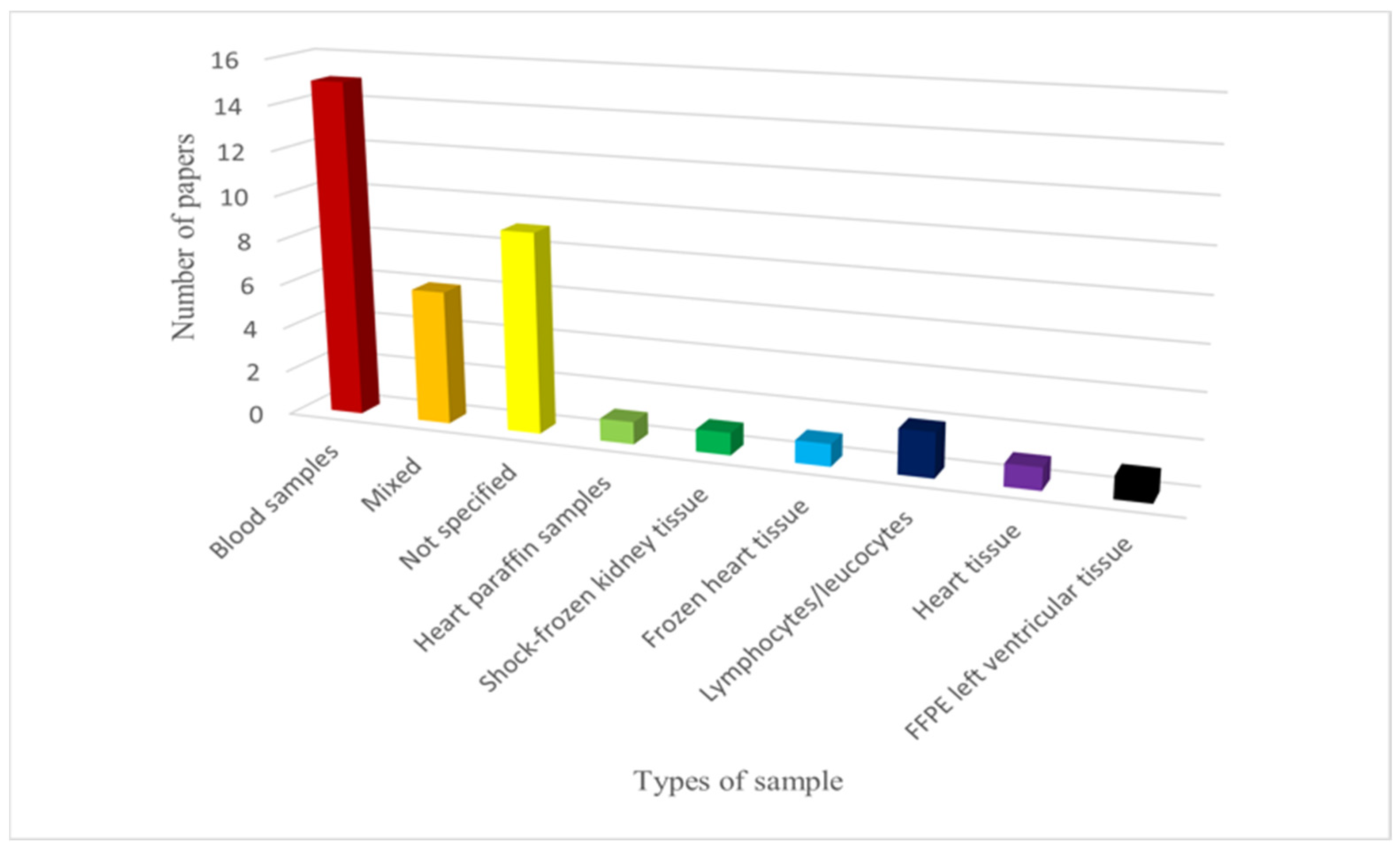
3. Results
4. Discussion
Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hauck, F.R.; Tanabe, K.O. International trends in sudden infant death syndrome: Stabilization of rates requires further action. Pediatrics 2008, 122, 660–666. [Google Scholar] [CrossRef] [PubMed]
- Heathfield, L.J.; Martin, L.J.; Ramesar, R. A Systematic Review of Molecular Autopsy Studies in Sudden Infant Death Cases. J. Pediatr. Genet. 2018, 7, 143–149. [Google Scholar] [PubMed]
- Basso, C.; Aguilera, B.; Banner, J.; Cohle, S.; d’Amati, G.; de Gouveia, R.H.; di Gioia, C.; Fabre, A.; Gallagher, P.J.; Leone, O.; et al. Guidelines for autopsy investigation of sudden cardiac death: 2017 update from the Association for European Cardiovascular Pathology. Virchows Arch. 2017, 471, 691–705. [Google Scholar] [CrossRef] [PubMed]
- Isbister, J.C.; Semsarian, C. The role of the molecular autopsy in sudden cardiac death in young individuals. Nat. Rev. Cardiol. 2024, 21, 215–216. [Google Scholar] [CrossRef]
- Lee, A.; Ackerman, M.J. Sudden unexplained death: Evaluation of those left behind. Lancet 2003, 362, 1429–1431. [Google Scholar] [CrossRef]
- Semsarian, C.; Ingles, J.; Wilde, A.A.M. Sudden cardiac death in the young: The molecular autopsy and a practical approach to surviving relatives. Eur. Heart J. 2015, 36, 1290–1296. [Google Scholar] [CrossRef]
- Semsarian, C.; Ingles, J. Molecular autopsy in victims of inherited arrhythmias. J. Arrhythm. 2016, 32, 359–365. [Google Scholar] [CrossRef]
- Paratz, E.D.; Rowsell, L.; Zentner, D.; Parsons, S.; Morgan, N.; Thompson, T.; James, P.; Pflaumer, A.; Semsarian, C.; Smith, K.; et al. Cardiac arrest and sudden cardiac death registries: A systematic review of global coverage. Open Heart 2020, 7, e001195. [Google Scholar] [CrossRef] [PubMed]
- Campuzano, O.; Sarquella-Brugada, G. Molecular autopsy in sudden cardiac death. Glob. Cardiol. Sci. Pract. 2023, 2023, e202308. [Google Scholar] [CrossRef]
- Chahal, C.A.A.; Salloum, M.N.; Alahdab, F.; Gottwald, J.A.; Tester, D.J.; Anwer, L.A.; So, E.L.; Murad, M.H.; Louis, E.K.S.; Ackerman, M.J.; et al. Systematic Review of the Genetics of Sudden Unexpected Death in Epilepsy: Potential Overlap With Sudden Cardiac Death and Arrhythmia-Related Genes. J. Am. Heart Assoc. 2020, 9, e012264. [Google Scholar] [CrossRef]
- Zhen, X.; Zhao, W.; Wang, J.; Li, L.; He, Y.; Zhang, J.; Li, C.; Zhang, S.; Luo, B.; Huang, J.; et al. Androgen receptor (CAG)n repeat polymorphism contributes to risk of sudden cardiac death originated from coronary artery disease with sex discrepancy. Forensic Sci. Int. 2023, 343, 111563. [Google Scholar] [CrossRef] [PubMed]
- Neubauer, J.; Kissel, C.K.; Bolliger, S.A.; Barbon, D.; Thali, M.J.; Kloiber, D.; Bode, P.K.; Kovacs, B.; Graf, U.; Maspoli, A.; et al. Benefits and outcomes of a new multidisciplinary approach for the management and financing of sudden unexplained death cases in a forensic setting in Switzerland. Forensic Sci. Int. 2022, 334, 111240. [Google Scholar] [CrossRef] [PubMed]
- Alhassani, S.; Deif, B.; Conacher, S.; Cunningham, K.S.; Roberts, J.D. A large familial pathogenic Plakophilin-2 gene (PKP2) deletion manifesting with sudden cardiac death and lone atrial fibrillation: Evidence for alternating atrial and ventricular phenotypes. HeartRhythm Case Rep. 2018, 4, 486–489. [Google Scholar] [CrossRef] [PubMed]
- Ariza, J.A.; Rocha, A.H.M.; Pérez, R.C.; Bermudez-Santana, C.I. Next-generation sequencing of postmortem molecular markers to support for medicolegal autopsy. Forensic Sci. Int. 2022, 6, 100300. [Google Scholar] [CrossRef]
- Marey, I.; Fressart, V.; Rambaud, C.; Fornes, P.; Martin, L.; Grotto, S.; Alembik, Y.; Gorka, H.; Millat, G.; Gandjbakhch, E.; et al. Clinical impact of post-mortem genetic testing in cardiac death and cardiomyopathy. Open Med. 2020, 15, 435–446. [Google Scholar] [CrossRef] [PubMed]
- Siskind, T.; Williams, N.; Sebastin, M.; Marion, R.; McDonald, T.V.; Walsh, C.; Sampson, B.; Tang, Y.; Clark, B.C. Genetic screening of relatives of decedents experiencing sudden unexpected death: Medical examiner’s office referrals to a multi-disciplinary cardiogenetics program. J. Community Genet. 2022, 13, 629–639. [Google Scholar] [CrossRef] [PubMed]
- Clemens, D.J.; Gray, B.; Bagnall, R.D.; Tester, D.J.; Dotzler, S.M.; Giudicessi, J.R.; Matthews, E.; Semsarian, C.; Behr, E.R.; Ackerman, M.J. Triadin Knockout Syndrome Is Absent in a Multi-Center Molecular Autopsy Cohort of Sudden Infant Death Syndrome and Sudden Unexplained Death in the Young and Is Extremely Rare in the General Population. Circ. Genom. Precis. Med. 2020, 13, e002731. [Google Scholar] [CrossRef] [PubMed]
- Marziliano, N.; Medoro, A.; Mignogna, D.; Saccon, G.; Folzani, S.; Reverberi, C.; Russo, C.; Intrieri, M. Sudden Cardiac Death Caused by a Fatal Association of Hypertrophic Cardiomyopathy (MYH7, p.Arg719Trp), Heterozygous Familial Hypercholesterolemia (LDLR, p.Gly343Lys) and SARS-CoV-2 B.1.1.7 Infection. Diagnostics 2021, 11, 1229. [Google Scholar] [CrossRef] [PubMed]
- Beccacece, L.; Abondio, P.; Giorgetti, A.; Bini, C.; Pelletti, G.; Luiselli, D.; Pelotti, S. A Genome-Wide Analysis of a Sudden Cardiac Death Cohort: Identifying Novel Target Variants in the Era of Molecular Autopsy. Genes 2023, 14, 1265. [Google Scholar] [CrossRef]
- Iglesias, M.; Ripoll-Vera, T.; Perez-Luengo, C.; García, A.B.; Moyano, S.; Canos, J.C.; Borondo, J.C.; Alvarez, J.; Heine-Suñer, D.; Barcelo, B. Diagnostic Yield of Genetic Testing in Sudden Cardiac Death with Autopsy Findings of Uncertain Significance. J. Clin. Med. 2021, 10, 1806. [Google Scholar] [CrossRef]
- Larsen, M.K.; Christiansen, S.L.; Hertz, C.L.; Frank-Hansen, R.; Jensen, H.K.; Banner, J.; Morling, N. Targeted molecular genetic testing in young sudden cardiac death victims from Western Denmark. Int. J. Leg. Med. 2020, 134, 111–121. [Google Scholar] [CrossRef] [PubMed]
- Girolami, F.; Spinelli, V.; Maurizi, N.; Focardi, M.; Nesi, G.; Maio, V.; Grifoni, R.; Albora, G.; Bertaccini, B.; Targetti, M.; et al. Genetic characterization of juvenile sudden cardiac arrest and death in Tuscany: The ToRSADE registry. Front. Cardiovasc. Med. 2022, 9, 1080608. [Google Scholar] [CrossRef]
- Neubauer, J.; Wang, S.; Russo, G.; Haas, C. Re-evaluation of single nucleotide variants and identification of structural variants in a cohort of 45 sudden unexplained death cases. Int. J. Leg. Med. 2021, 135, 1341–1349. [Google Scholar] [CrossRef] [PubMed]
- Scheiper-Welling, S.; Tabunscik, M.; Gross, T.E.; Jenewein, T.; Beckmann, B.M.; Niess, C.; Gradhand, E.; Wunder, C.; Schneider, P.M.; Rothschild, M.A.; et al. Variant interpretation in molecular autopsy: A useful dilemma. Int. J. Leg. Med. 2022, 136, 475–482. [Google Scholar] [CrossRef] [PubMed]
- Fadoni, J.; Santos, A.; Cainé, L. Post-mortem genetic investigation in sudden cardiac death victims: Complete exon sequencing of forty genes using next-generation sequencing. Int. J. Leg. Med. 2022, 136, 483–491. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Barrios, E.; Sarquella-Brugada, G.; Perez-Serra, A.; Fernandez-Falgueras, A.; Cesar, S.; Alcalde, M.; Coll, M.; Puigmulé, M.; Iglesias, A.; Ferrer-Costa, C.; et al. Reevaluation of ambiguous genetic variants in sudden unexplained deaths of a young cohort. Int. J. Leg. Med. 2023, 137, 345–351. [Google Scholar] [CrossRef] [PubMed]
- Tuveng, J.M.; Berling, B.M.; Bunford, G.; Vanoye, C.G.; Welch, R.C.; Leren, T.P.; George, A.L.; Rognum, T.O. Long QT syndrome KCNH2 mutation with sequential fetal and maternal sudden death. Forensic Sci. Med. Pathol. 2018, 14, 367–371. [Google Scholar] [CrossRef] [PubMed]
- Kraoua, L.; Jaouadi, H.; Allouche, M.; Achour, A.; Kaouther, H.; Ahmed, H.B.; Chaker, L.; Maazoul, F.; Ouarda, F.; Zaffran, S.; et al. Molecular autopsy and clinical family screening in a case of sudden cardiac death reveals ACTN2 mutation related to hypertrophic/dilated cardiomyopathy and a novel LZTR1 variant associated with Noonan syndrome. Mol. Genet. Genom. Med. 2022, 10, e1954. [Google Scholar] [CrossRef]
- Gélinas, R.; Leach, E.; Horvath, G.; Laksman, Z. Molecular Autopsy Implicates Primary Carnitine Deficiency in Sudden Unexplained Death and Reversible Short QT Syndrome. Can. J. Cardiol. 2019, 35, 1256.e1–1256.e2. [Google Scholar] [CrossRef]
- Takahashi, Y.; Fukuda, H.; Hayakawa, A.; Sano, R.; Kubo, R.; Kawabata-Iwakawa, R.; Nakajima, T.; Ishige, T.; Tokue, H.; Asano, K.; et al. Postmortem genetic analysis of 17 sudden cardiac deaths identified nonsense and frameshift variants in two cases of arrhythmogenic cardiomyopathy. Int. J. Leg. Med. 2023, 137, 1927–1937. [Google Scholar] [CrossRef]
- Yamamoto, T.; Miura, A.; Itoh, K.; Takeshima, Y.; Nishio, H. RNA sequencing reveals abnormal LDB3 splicing in sudden cardiac death. Forensic Sci. Int. 2019, 302, 109906. [Google Scholar] [CrossRef] [PubMed]
- Grassi, S.; Vidal, M.C.; Campuzano, O.; Arena, V.; Alfonsetti, A.; Rossi, S.S.; Scarnicci, F.; Iglesias, A.; Brugada, R.; Oliva, A. Sudden Death without a Clear Cause after Comprehensive Investigation: An Example of Forensic Approach to Atypical/Uncertain Findings. Diagnostics 2021, 11, 886. [Google Scholar] [CrossRef] [PubMed]
- Modena, M.; Castiglione, V.; Aretini, P.; Mazzanti, C.M.; Chiti, E.; Giannoni, A.; Emdin, M.; Di Paolo, M. Unveiling a sudden unexplained death case by whole exome sequencing and bioinformatic analysis. Mol. Genet. Genom. Med. 2020, 8, e1182. [Google Scholar] [CrossRef] [PubMed]
- Shanks, G.W.; Tester, D.J.; Ackerman, J.P.; Simpson, M.A.; Behr, E.R.; White, S.M.; Ackerman, M.J. Importance of Variant Interpretation in Whole-Exome Molecular Autopsy. Circulation 2018, 137, 2705–2715. [Google Scholar] [CrossRef] [PubMed]
- Marcondes, L.; Crawford, J.; Earle, N.; Smith, W.; Hayes, I.; Morrow, P.; Donoghue, T.; Graham, A.; Love, D.; Skinner, J.R.; et al. Long QT molecular autopsy in sudden unexplained death in the young (1–40 years old): Lessons learnt from an eight year experience in New Zealand. PLoS ONE 2018, 13, e0196078. [Google Scholar] [CrossRef] [PubMed]
- Jenewein, T.; Neumann, T.; Erkapic, D.; Kuniss, M.; Verhoff, M.A.; Thiel, G.; Kauferstein, S. Influence of genetic modifiers on sudden cardiac death cases. Int. J. Leg. Med. 2018, 132, 379–385. [Google Scholar] [CrossRef]
- Neubauer, J.; Lecca, M.R.; Russo, G.; Bartsch, C.; Medeiros-Domingo, A.; Berger, W.; Haas, C. Exome analysis in 34 sudden unexplained death (SUD) victims mainly identified variants in channelopathy-associated genes. Int. J. Leg. Med. 2018, 132, 1057–1065. [Google Scholar] [CrossRef] [PubMed]
- Andersen, J.D.; Jacobsen, S.B.; Trudsø, L.C.; Kampmann, M.L.; Banner, J.; Morling, N. Whole genome and transcriptome sequencing of post-mortem cardiac tissues from sudden cardiac death victims identifies a gene regulatory variant in NEXN. Int. J. Leg. Med. 2019, 133, 1699–1709. [Google Scholar] [CrossRef]
- Raju, H.; Ware, J.S.; Skinner, J.R.; Hedley, P.L.; Arno, G.; Love, D.R.; van der Werf, C.; Tfelt-Hansen, J.; Winkel, B.G.; Cohen, M.C.; et al. Next-generation sequencing using microfluidic PCR enrichment for molecular autopsy. BMC Cardiovasc. Disord. 2019, 19, 174. [Google Scholar] [CrossRef]
- Graziosi, M.; Leone, O.; Foà, A.; Agostini, V.; Ditaranto, R.; Foroni, M.; Rossi, C.; Lovato, L.; Seri, M.; Rapezzi, C. Postmortem diagnosis of left dominant arrhythmogenic cardiomyopathy: The importance of a multidisciplinary network for sudden death victims. “HIC mors gaudet succurere vitae”. Cardiovasc. Pathol. 2020, 44, 107157. [Google Scholar] [CrossRef]
- Simons, E.; Labro, A.; Saenen, J.; Nijak, A.; Sieliwonczyk, E.; Vandendriessche, B.; Dąbrowska, M.; Van Craenenbroeck, E.M.; Schepers, D.; Van Laer, L.; et al. Molecular autopsy and subsequent functional analysis reveal de novo DSG2 mutation as cause of sudden death. Eur. J. Med. Genet. 2021, 64, 104322. [Google Scholar] [CrossRef]
- Gaertner-Rommel, A.; Tiesmeier, J.; Jakob, T.; Strickmann, B.; Veit, G.; Bachmann-Mennenga, B.; Paluszkiewicz, L.; Klingel, K.; Schulz, U.; Laser, K.T.; et al. Molecular autopsy and family screening in a young case of sudden cardiac death reveals an unusually severe case of FHL1 related hypertrophic cardiomyopathy. Mol. Genet. Genom. Med. 2019, 7, e841. [Google Scholar] [CrossRef] [PubMed]
- Mahlke, N.; Dittmann, S.; Schulze-Bahr, E.; Ritz-Timme, S.; Hartung, B. Sudden unexpected cardiac death and postmortem identification of a novel RYR2 gene mutation. Int. J. Leg. Med. 2019, 133, 1835–1838. [Google Scholar] [CrossRef]
- Neubauer, J.; Wang, Z.; Rougier, J.S.; Abriel, H.; Rieubland, C.; Bartholdi, D.; Haas, C.; Medeiros-Domingo, A. Functional characterization of a novel SCN5A variant associated with long QT syndrome and sudden cardiac death. Int. J. Leg. Med. 2019, 133, 1733–1742. [Google Scholar] [CrossRef] [PubMed]
- Foti, F.; De-Giorgio, F.; Vetrugno, G.; Basso, C.; Pilichou, K. A de novo ryanodine receptor 2 gene variant in a case of sudden cardiac death. Int. J. Leg. Med. 2020, 134, 619–623. [Google Scholar] [CrossRef]
- Manzanilla-Romero, H.H.; Schermer, E.; Mayr, A.; Rudnik-Schöneborn, S. Only one beer can be mortal: A case report of two sisters with cardiac arrest due to a homozygous mutation in PPA2 gene. Eur. J. Pediatr. 2023, 182, 3785–3788. [Google Scholar] [CrossRef] [PubMed]
- Ripoll-Vera, T.; Pérez Luengo, C.; Borondo Alcázar, J.C.; García Ruiz, A.B.; Sánchez Del Valle, N.; Barceló Martín, B.; García, J.L.P.; Buitrago, G.G.; Martínez, C.D.; Villena, J.C.C.; et al. Sudden cardiac death in persons aged 50 years or younger: Diagnostic yield of a regional molecular autopsy program using massive sequencing. Rev. Esp. Cardiol. 2021, 74, 402–413. [Google Scholar] [CrossRef]
- Fellmann, F.; van El, C.G.; Charron, P.; Michaud, K.; Howard, H.C.; Boers, S.N.; Clarke, A.J.; Duguet, A.-M.; Forzano, F.; Kauferstein, S.; et al. European recommendations integrating genetic testing into multidisciplinary management of sudden cardiac death. Eur. J. Hum. Genet. 2019, 27, 1763–1773. [Google Scholar] [CrossRef] [PubMed]
- Orland, K.M.; Anderson, K.B. Molecular Autopsy for Sudden Cardiac Death: Current State and Considerations. Curr. Genet. Med. Rep. 2019, 7, 145–152. [Google Scholar] [CrossRef]
- Yazdanfard, P.D.; Christensen, A.H.; Tfelt-Hansen, J.; Bundgaard, H.; Winkel, B.G. Non-diagnostic autopsy findings in sudden unexplained death victims. BMC Cardiovasc. Disord. 2020, 20, 58. [Google Scholar] [CrossRef]
- Votýpka, P.; Krebsová, A.; Norambuena-Poustková, P.; Peldová, P.; Pohlová Kučerová, Š.; Kulvajtová, M.; Dohnalová, P.; Bílek, M.; Stufka, V.; Rücklová, K.; et al. Post-mortem genetic testing in sudden cardiac death and genetic screening of relatives at risk: Lessons learned from a Czech pilot multidisciplinary study. Int. J. Leg. Med. 2023, 137, 1787–1801. [Google Scholar] [CrossRef] [PubMed]
- Orlíčková, J.; Zeman, M.; Vojtíšek, T.; Slabý, O. The importance of molecular autopsy in forensic medicine. Cas. Lek. Cesk. 2022, 161, 207–211. [Google Scholar] [PubMed]
- Ko, T.; Morita, H. Molecular Genomic Autopsy-Clues to Preventing Further Tragedy? Circ. J. 2022, 87, 120–122. [Google Scholar] [CrossRef]
- Kristina, R.; Markéta, K.; Alice, K.; Martin, D.; Jana, P. Molecular autopsy and sudden cardiac death in the young. Soud. Lek. 2020, 65, 2–6. [Google Scholar] [PubMed]
- Brion, M.; Sobrino, B.; Martinez, M.; Blanco-Verea, A.; Carracedo, A. Massive parallel sequencing applied to the molecular autopsy in sudden cardiac death in the young. Forensic Sci. Int. Genet. 2015, 18, 160–170. [Google Scholar] [CrossRef] [PubMed]
- Basso, C.; Burke, M.; Fornes, P.; Gallagher, P.J.; de Gouveia, R.H.; Sheppard, M.; Thiene, G.; van der Wal, A. Guidelines for autopsy investigation of sudden cardiac death. Virchows Arch. 2008, 452, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Moher, D. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Bmj 2021, 372, n71. [Google Scholar] [CrossRef]
- Kumar, S.; Peters, S.; Thompson, T.; Morgan, N.; Maccicoca, I.; Trainer, A.; Zentner, D.; Kalman, J.M.; Winship, I.; Vohra, J.K. Familial cardiological and targeted genetic evaluation: Low yield in sudden unexplained death and high yield in unexplained cardiac arrest syndromes. Heart Rhythm 2013, 10, 1653–1660. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Authors and Year of Publication | Gene(s) Examined | Heart Disease | Sample Number and Type of Death |
|---|---|---|---|
| Zhen X. et al. (2023) [11] | 1 gene (CAG)n repeat polymorphism within Androgen Receptor (AR) gene | Coronary heart disease | 564 healthy controls and 182 cases of SCD |
| Neubauer J. et al. (2022) [12] | 393 cardiovascular and metabolic disease genes | Not specified | 39 cases of SCD |
| Alhassani S. et al. (2018) [13] | 30 genes (AKAP9, ANK2, CACNA1C, CACNB2, CASQ2, CAV3, DSC2, DSG2, DSP, GPD1L, HCN4, JUP, KCNE1, KCNE2, KCNE3, KCNH2, KCNJ2, KCNJ5, KCNJ8, KCNQ1, NKX2.5, PKP2, RANGRF, RYR2, SCN1B, SCN3B, SCN4B, SCN5A, SNTA1, TMEM43) | Not specified | A case of SUDY and his family |
| Ariza J.A. et al. (2022) [14] | 4834 clinically relevant genes | Cardiac channelopathy | A case of SUDY |
| Marey I. et al. (2020) [15] | 15 genes (MYH7, MYBPC3, TNNT2, TNNI3, MYL2, PKP2, DSP, DSG2, LMNA, TTR, and five major sarcomeric genes in DCM) | Not specified | 35 cases of SCD |
| Siskind T. et al. (2022) [16] | 94 genes (ABCC9, ACTC1, ACTN2, AKAP9, AKAP10, ANK2, ANKRD1, ARHGAP24, BAG3, BCAT1, CACNA1C, CACNA2D1, CACNB2, CALM1, CAML2, CASQ2, CAV1, CAV3, CDKN1A, CRYAB, CSRP3, CTF1, DES, DPP6, DSC2, DSG2, DSP, DTNA, EMD, FHL2, FLRT2, GATAD1, GLA, GPD1L, HAND1, HCN4, JUP, KCNA5, KCND3, KCNE1, KCNE1L, KCNE2, KCNE3, KCNE4, KCNH2, KCNJ2, KCNJ5, KCNJ8, KCNQ1, LAMA4, LAMP2, LDB3, LMNA, MYB, MYBPC3, MYH6, MYH7, MYL2, MYL3, MYLK2, MYOZ2, MYPN, NEBL, NEXN, NOS1AP, PC3, PKP2, PLN, PRKAG2, RANGRF, RBM20, RyR2, SCN10A, SCN1B, SCN2B, SCN3B, SCN4B, SCN5A, SGCD, SNTA1, STRN, TAZ, TCAP, TGFB3, TMEM43, TMPO, TNNC1, TNNI3, TNNT2, TPM, TPM1, TRPM4, TTR, and VCL) | Not specified | 5 cases of SCD and 6 cases of SUDY |
| Clemens D.J. (2020) [17] | 1 gene (TRDN) | Triadine knockout syndrome (TKOS) | 258 cases of SUDY |
| Marzialiano N. et al. (2019) [18] | 60 genes (ACTC1, ACVRL1, APOB, BAG3, BMPR2, BRAF, CACNA1C, CASQ2, DES, DMD, DSC2, DSG2, DSP, ELN, EMD, ENG, FBN1, FLNC, GATA4, GLA, JAG1, JUP, KCNE1, KCNE2, KCNH2, KCNJ2, KCNJ8, KCNQ1, KRAS, LAMP2, LDLR, LDLRAP1, LMNA, MYBPC3, MYH7, MYL2, MYL3, NF1, NKX2-5, PKP2, PLN, PRKAG2, PCSK9, PTPN11, RAF1, RBM20, RYR2, SCN1B, SCN5A, SOS1, SOS2, TAZ, TGFBR2, TMEM43, TNNC1, TNNI3, TNNT2, TPM1, TTN, and TTR) | Hypertrophic cardiomyopathy and heterozygous familial hypercholesterolemia | A case of SUDY |
| Beccacece L. et al. (2023) [19] | The DNA was genotyped for about 720,000 genetic markers | Not specified | 30 cases of SCD |
| Iglesias M. et al. (2021) [20] | From 194 to 380 genes | Not specified | 31 cases of SUDI, SUDY and SCD (unspecified number) |
| Larsen M.K. et al. (2020) [21] | 104 genes (ABCC9f, ACTC1a,g, ACTN2l, AKAP9, ANK2, ANKRD1l, BAG3, CACNA1Cc, CACNA1D, CACNB2, CALM1h,n, CALM2h,n, CALM3h,n, CALR3, CASQ2, CAV3c, CRYAB, CSRP3a, CTF1, DESk, DMD, DPP6, DSC2, DSG2a, DSPa, DTNA, EYA4, FHL2, FKTN, GAAa, GJA5i,j, GLAl, GPD1Ld, HCN1e, HCN4e,f,g, ILK, JPH2f, JUP, KCNA5, KCND3f, KCNE1f, KCNE2f, KCNE3f, KCNE4f, KCNE5f, KCNH2f,o, KCNJ2f,o, KCNJ5f, KCNJ8f,h, KCNQ1e,h,o, LAMA4, LAMP2, LDB3g,l, lHCM, LMNAf,g,k, MOG1, MYBPC3a,g, MYH6a,e, MYH7a,g, MYL2, MYL3, MYLK2, MYOZ2, MYPNl, NEBL, NEXNl, NPPA, PKP2b, PLNk,l, PRDM16g, PRKAG2f,m, PSEN1, PSEN2, RANGRFb, RBM20, RPS7, RPSA, RYR2f,k, SCN1Bf,i, SCN2Bb, SCN3Bf, SCN4Bf, SCN5Aa,c,e,f,g,h,i,j,k, SDHA, SGCD, SLC22A5, SLC25A4, SNTA1, STARD3, TAZg, TCAPl, TGFB3, TMEM43, TMPO, TNNC1l, TNNI3l, TNNT2a,g, TPM1a,g, TRPM4i,j, TTNa,k, and VCLa) | Hypertrophic cardiomyopathy (HCM), dilated cardiomyopathy (DCM), arrhythmogenic right ventricular | 70 cases of SUDI, SUDY and SCD |
| Girolami F. et al. (2022) [22] | 174 genes (ABCC9, ABCG5, ABCG8, ACTA1, ACTA2, ACTC1, ACTN2, AKAP9, ALMS1, ANK2, ANKRD1, APOA4, APOA5, APOB, APOC2, APOE, BAG3, BRAF, CACNA1C, CACNA2D1, CACNB2, CALM1, CALR3, CASQ2, CAV3, CBL, CBS, CETP, COL3A1, COL5A1, COL5A2, COX15, CREB3L3, CRELD1, CRYAB, CSRP3, CTF1, DES, DMD, DNAJC19, DOLK, DPP6, DSC2, DSG2, DSP, DTNA, EFEMP2, ELN, EMD, EYA4, FBN1, FBN2, FHL1, FHL2, FKRP, FKTN, FXN, GAA, GATAD1, GCKR, GJA5, GLA, GPD1L, GPIHBP1, HADHA, HCN4, HFE, HRAS, HSPB8, ILK, JAG1, JPH2, JUP, KCNA5, KCND3, KCNE1, KCNE2, KCNE3, KCNH2, KCNJ2, KCNJ5, KCNJ8, KCNQ1, KLF10, KRAS, LAMA2, LAMA4, LAMP2, LDB3, LDLR, LDLRAP1, LMF1, LMNA, LPL, LTBP2, MAP2K1, MAP2K2, MIB1, MURC, MYBPC3, MYH11, MYH6, MYH7, MYL2, MYL3, MYLK, MYLK2, MYO6, MYOZ2, MYPN, NEXN, NKX25, NODAL, NPPA, NRAS, PCSK9, PDLIM3, PKP2, PLN, PRDM16, PRKAG2, PRKAR1A, PTPN11, RAF1, RANGRF, RBM20, RYR1, RYR2, SALL4, SCN1B, SCN2B, SCN3B, SCN4B, SCN5A, SCO2, SDHA, SEPN1, SGCB, SGCD, SHOC2, SLC25A4, SLC2A10, SMAD3, SMAD4, SNTA1, SOS1, SREBF2, TAZ, TBX20, TBX3, TBX5, TCAP, TGFB2, TGFB3, TGFBR1, TGFBR2, TMEM43, TMPO, TNNC1, TNNI3, TNNT2, TPM1, TRDN, TRIM63, TRPM4, TTN, TTR, TXNRD2, VCL, ZBTB17, ZHX3, ZIC3) | Not specified | 14 cases of SCD |
| Neubauer J. et al. (2021) [23] | 244 (ABCC8, ABCC9, ACAD9, ACADM, ACADS, ACADVL, ACTA2, ACTC1, ACTN2, ACVRL1, ADAMTS10, AGL, AKAP9, ALG10, ALMS1, ANK2, ANKRD1, ASCL1, ATP5F1E, BAG3, BDNF, BMPR1B, BMPR2, BRAF, CACNA1C, CACNA2D1, CACNB2, CALM1, CALM2, CALM3, CALR3, CAMK2G, CASQ2, CAV1, CAV3, CAVIN4, CBL, CDH2, CHRM2, CLCA2, COA5, COL3A1, COL5A1, COL5A2, COL6A1, COL6A2, CPT1A, CPT2, CRYAB, CSRP3, CTF1, CTGF, CTNNA3, DCHS1, DES, DLG1, DMD, DMPK, DNAJC19, DNM1L, DOLK, DPP6, DSC2, DSG2, DSP, DTNA, ECE1, EDN3, EFEMP2, ELN, EMD, ENG, ETFA, ETFB, ETFDH, EYA4, FBN1, FBN2, FGF12, FHL1, FHL2, FHOD3, FKRP, FKTN, FLNA, FLNC, FXN, G6PC, GAA, GATA4, GATA5, GATA6, GATAD1, GDNF, GJA1, GJA5, GJD4, GK, GLA, GLB1, GLRA1, GPD1L, GUSB, HADH, HADHA, HADHB, HCN2, HCN4, HEY2, HFE, HMGCL, HMGCS2, HRAS, HTR2C, ILK, JPH2, JUP, KCNA5, KCND2, KCND3, KCNE1, KCNE2, KCNE3, KCNE5, KCNH2, KCNJ2, KCNJ5, KCNJ8, KCNK17, KCNQ1, KLF10, KRAS, LAMA4, LAMP2, LDB3, LMNA, LRP5, LRRC10, LZTR1, MAOA, MAP2K1, MAP2K2, MED12, MED23, MOG, MRPL3, MT-TI, MT-TL1, MYBPC3, MYH11, MYH6, MYH7, MYL2, MYL3, MYLK, MYLK2, MYO6, MYOM1, MYOZ2, MYPN, NEBL, NEXN, NKX2-5, NOS1AP, NOTCH1, NPPA, NPPA, NRAS, PDLIM3, PDSS2, PHOX2B, PKP2, PLEKHM2, PLN, PPA2, PPP1R13L, PRDM16, PRKAG2, PRKG1, PSEN1, PSEN2, PTPN11, RAB3GAP1, RAF1, RANGRF, RBM20, RET, RYR2, SCN10A, SCN1B, SCN2B, SCN3B, SCN4B, SCN5A, SCO2, SDHA, SEMA3A, SGCD, SHOC2, SKI, SLC22A5, SLC25A10, SLC25A3, SLC37A4, SLC4A3, SLC6A4, SLMAP, SMAD3, SMAD9, SNTA1, SOS1, SYNE1, SYNE2, TAZ, TBX1, TBX20, TBX3, TBX5, TCAP, TGFB2, TGFB3, TGFBR1, TGFBR2, TMEM43, TMEM70, TMPO, TNNC1, TNNI3, TNNI3K, TNNT2, TP63, TPM1, TRDN, TRIM63, TRPM4, TRPM7, TSFM, TSPYL1, TTN, TTR, TXNRD2, VCL, XK, and ZNF365) | Not specified | 45 cases of SCD |
| Scheiper-Welling S. et al. (2022) [24] | 93 genes with known cardiac associations | Arrhythmic heart disease | 56 cases of SUDY |
| Fadoni J. et al. (2022) [25] | 40 genes (MYBPC3, MYH7, TNNI3, TNNT2, ACTC1, TPM1, MYL2, MYL3, MYH6, TNNC1, VCL, CAV3, MYLK2, JPH2, CSRP3, ANKRD1, DES, ACTN2, MYL4, NEXN, CRYAB, DSG2, HSPB1, HSPD1, MYO6, GPD1L, KCNE2, NME1, MYC, POMC, SCN5A, TP53, ACAD9, GAA, PRKAG2, LAMP2, NDUFS1, RAF1, SCO2, and SCL25A4) | Hypertrophic cardiomyopathy (HCM) | 16 cases of SUDY and SCD |
| Martínez-Barrios E. et al. (2023) [26] | 113 genes (ABCC9, ACTA2, ACTC1, ACTN2, AKAP9, ANK2, BAG3, CACNA1C, CACNA1G, CACNA1H, CACNA1I, CACNB2, CASQ2, CAV3, CHRM2, COL3A1, CRYAB, CSRP3, CTF1, DES, DMD, DMPK, DSC2, DSG2, DSP, ECE1, EMD, EN1, EYA4, FBN1, FHL2, FKTN, GJA7, GLA, GPD1L, HCN1, HCN2, HCN4, ILK, JPH2, JUP, KCNA4, KCNA5, KCND2, KCND3, KCNE1, KCNE2, KCNE3, KCNH2, KCNJ2, KCNJ3, KCNJ5, KCNK4, KCNQ1, LAMA4, LAMP2, LDB3, LMNA, MYBPC3, MYH6, MYH7, MYL2, MYL3, MYLK2, MYOZ2, MYPN, NEBL, NEXN, NOS1AP, NOTCH1, NPPA, NUP155, PDLIM3, PHOX2A, PHOX2B, PKP2, PLN, PRKAG2, PSEN1, PSEN2, RBM20, RET, RYR2, SCN10A, SCN1B, SCN2B, SCN3B, SCN4B, SCN5A, SGCA, SGCB, SGCD, SIRT3, SLC25A4, SLC6A4, SLC8A1, SLMAP, SNTA1, TAZ, TCAP, TGFB3, TGFBR1, TGFBR2, TLX3, TMEM43, TMPO, TNNC1, TNNI3, TNNT2, TPM1, TTN, and VCL) | Not specified | 51 cases of SIDS, SUDI and SUDY (unspecified number) |
| Tuveng Jon M. et al. (2018) [27] | 5 genes (KCNQ1, KCNH2, SCN5A, KCNE1, KCNE2 | Not specified | A case of SUDY |
| Kraoua L. et al. (2012) [28] | Whole genome | Hypertrophic/dilatated cardiomyopathy | A case of SUDY |
| Gélinas R. et al. (2019) [29] | 184 genes (AARS2, ABCC6, ABCC9, ACAD9, ACADVL, ACTA1, ACTA2, ACTC1, ACTN2, AGK, AGL, AKAP9, ALMS1, ALPK3, ANK2, ANO5, APOA1, BAG3, BRAF, CACNA1C, CACNB2, CALM1, CALM2, CALM3, CALR3, CAPN3, CASQ2, CAV3, CBL, CDH2, COX15, CPT2, CRYAB, CSRP3, CTNNA3, DBH, DES, DMD, DNAJC19, DOLK, DSC2, DSG2, DSP, DTNA, DYSF, EEF1A2, ELAC2, EMD, ENPP1, EPG5, ETFA, ETFB, ETFDH, FBXO32, FHL1, FKRP, FKTN, FLNC, FOXD4, FOXRED1, FXN, GAA, GATA5, GATA6, GATAD1, GBE1, GFM1, GLA, GLB1, GMPPB, GTPBP3, GUSB, HADHA, HAND1, HCN4, HFE, HRAS, ISPD, JPH2, JUP, KCNA5, KCNE1, KCNE2, KCNH2, KCNJ2, KCNJ5, KCNQ1, KRAS, LAMA2, LAMP2, LARGE, LDB3, LMNA, LRRC10, LZTR1, MAP2K1, MAP2K2, MLYCD, MTO1, MYBPC3, MYBPHL, MYH6, MYH7, MYL2, MYL3, MYL4, MYOT, MYPN, NDUFAF2, NEXN, NF1, NKX2-5, NOS1AP, NRAS, NUP155, PCCA, PCCB, PKP2, PLEC, PLEKHM2, PLN, PNPLA2, POMT1, PPA2, PPP1CB, PRDM16, PRKAG2, PTPN11, RAF1, RASA2, RBCK1, RBM20, RIT1, RMND1, RRAS, RYR2, SALL4, SCN10A, SCN1B, SCN3B, SCN5A, SCNN1B, SCNN1G, SCO2, SDHA, SELENON, SGCA, SGCB, SGCD, SGCG, SHOC2, SLC22A5, SLC25A20, SLC25A4, SMCHD1, SOS1, SOS2, SPEG, SPRED1, TAB2, TAZ, TBX20, TBX5, TCAP, TECRL, TGFB3, TMEM43, TMEM70, TNNC1, TNNI3, TNNI3K, TNNT2, TOR1AIP1, TPM1, TRDN, TRIM32, TRPM4, TSFM, TTN, TTR, VCL, VCP, VPS13A, and XK) | Not specified | A case of SUDY |
| Takahashi Y. et al. (2023) [30] | 72 genes (ABCC9, ACTC1, ACTN2, AKAP9, ANK2, CACNA1C, CACNA2D1, CACNB2, CALM1, CALM2, CASQ2, CAV3, CSRP3, DES, DPP6, DSC2, DSG2, DSP, GJA5, GPD1L, HCN4, HEY2, IRX3, JUP, KCNA5, KCND3, KCNE1, KCNE2, KCNE3, KCNE5, KCNH2, KCNJ2, KCNJ3,CNJ5, KCNJ8, KCNQ1, LDB3, LMNA, MYBPC3, MYH6, MYH7, MYL2, MYL3, MYL4, MYOZ2, NEXN, PKP2, PLN, RANGRF, RBM20, RYR2, SCN10A, SCN1B, SCN3B, SCN4B, SCN5A, SGCD, SNTA, TAZ, TBX5, TCAP, TGFB3, TMEM43, TNNC1, TNNI3, TNNT2, TPM1, TRDN, TRPM4, TTN, TTR) | Not specified | 17 cases of SCD |
| Yamamoto T. et al. (2019) [31] | Clinical exome | Myotonic dystrophy type 1 (DM1) | A case of SUDY |
| Grassi S. et al. (2021) [32] | 82 genes (ABCC9, ACTC1, ACTN2, AKAP9, ANK2, BAG3, CACNA1C, CACNA2D1, CACNB2, CASQ2, CAV3, CRYAB, CSRP3, DES, DMD, DMPK, DSC2, DSG2, DSP, EMD, FKTN, FLNC, GLA, GPD1L, HCN4, JPH2, JUP, KCND3, KCNE1, KCNE2, KCNE3, KCNE5, KCNH2, KCNJ2, KCNJ5, KCNJ8, KCNQ1, LAMP2, LDB3, LMNA, MYBPC3, MYH6, MYH7, MYL2, MYL3, MYOZ2, MYPN, NEBL, NEXN, NOS1AP, PDLIM3, PKP2, PLN, PRKAG2, RANGRF, RBM20, RYR2, SCN1B, SCN2B, SCN3B, SCN4B, SCN5A, SCN10A, SGCD, SLMAP, SNTA1, TAZ, TCAP, TGFB3, TMEM43, TMPO, TNNC1, TNNI3, TNNT2, TP63, TPM1, TRDN, TRIM63, TRPM4, TTN, TTR, VCL) | Not specified | A case of SUDY |
| Modena M. et al. (2019) [33] | Whole exome | Not specified | A case of SCD |
| Shanks G.W. et al. (2018) [34] | 99 sudden death-susceptibility genes | Not specified | 25 cases of SUDY |
| Marcondes L. et al. (2018) [35] | Not specified, but the following genes are mentioned: SCN5A, KCNH2, KCNQ1, KCNE2, KCNE1, and KCNJ2 | Long QT syndrome (LQTS) | 365 cases of SUDY |
| Jenewein T. et al. (2018) [36] | 13 genes (DSC2, DSG2, DSP, HCN4, KCNJ2, KCNQ1, KCNH2, SCN5A, KCNE1, KCNE2, PKP2, RyR2, and SCN4B) | Not specified | A case of SUDY |
| Neubauer J. et al. (2018) [37] | 189 genes (ABCC8, ABCC9, ACAD9, ACADM, ACADS, ACADVL, ACTA2, ACTC1, ACTN2, ACVRL1, ADAMTS10, AGL, AKAP9, ANK2, ANKRD1, ASCL1, ATP5E, BAG3, BMPR1B, BMPR2, BRAF, CACNA1C, CACNA2D1, CACNB2, CALM1, CALM2, CALM3, CALR3, CAMK2G, CASQ2, CAV1, CAV3, CBL, COA5, COL3A1, COL5A1, COL5A2, CPT1A, CPT2, CRYAB, CSRP3, CTF1, CTGF, CTNNA3, DCHS1, DES, DLG1, DMD, DMPK, DNAJC, DNM1L, DOLK, DPP6, DSC2, DSG2, DSP, DTNA, ECE1, EFEMP2, ELN, EMD, ENG, ETFA, ETFB, ETFDH, EYA4, FBN1, FBN2, FHL2, FKRP, FKTN, FLNA, FOXRED1, G6PC, GAA, GATA4, GATA5, GATA6, GATA6, GATAD1, GJA1, GJA5, GJD4, GK, GLA, GLB1, GPD1L, GUSB, HADH, HADHA, HADHB, HCN2, HCN4, HEY2, HFE, HMGCL, HMGCS2, ILK, JPH2, JUP, KCNA5, KCND3, KCNE1, KCNE1L, KCNE2, KCNE3, KCNE5, KCNH2, KCNJ2, KCNJ5, KCNJ8, KCNQ1, LAMA4, LAMP2, LDB3, LMNA, MAP2K1, MAP2K2, MED23, MRPL3, MYBPC3, MYH11, MYH6, MYH7, MYL2, MYL3, MYLK, MYLK2, MYOM1, MYOZ2, MYPN, NEBL, NEXN, Nkx2-5, NOS1AP, NOTCH1, PDLIM3, PKP2, PLN, PRKAG2, PRKG1, PSEN1, PSEN2, RAF1, RANGRF, RBM20, RYR2, SCN10A, SCN1B, SCN2B, SCN3B, SCN4B, SCN5A, SCO2, SDHA, SEMA3A, SGCD, SLC22A5, SLC25A3, SLC37A4, SLMAP, SMAD3, SMAD9, SNTA1, SYNE1, SYNE2, TAZ, TBX5, TCAP, TGFβ2, TGFβ3, TGFβR1, TGFβR2, TMEM43, TMPO, TNNC1, TNNI3, TNNT2, TPM1, TRDN, TRPM4, TRPM7, TSFM, TTN, TTR, VCL, XK, ZASP, and ZNF365) | Not specified | 34 cases of SCD |
| Andersen J.D. et al. (2019) [38] | Whole genome sequencing | Not specified | 9 cases of SCD |
| Raju H. et al. (2019) [39] | 6 genes (KCNE1, KCNE2, KCNQ1, KCNH2, SCN5A, and RYR2) | Long QT syndrome (LQTS), Brugada syndrome (BrS), and catecholaminergic polymorphic ventricular tachycardia (CPVT) | 197 cases of SUDI, SUDY and SCD (unspecified number) |
| Graziosi M. et al. (2020) [40] | 174 genes (ABCC9, ABCG5, ABCG8, ACTA1, ACTA2, ACTC1, ACTN2, AKAP9, ALMS1, ANK2, ANKRD1, APOA4, APOA5, APOB, APOC2, APOE, BAG3, BRAF, CACNA1C, CACNA2D1, CACNB2, CALM1, CALR3, CASQ2, CAV3, CBL, CBS, CETP, COL3A1, COL5A1, COL5A2, COX15, CREB3L3, CRELD1, CRYAB, CSRP3, CTF1, DES, DMD, DNAJC19 DOLK, DPP6, DSC2, DSG2, DSP, DTNA, EFEMP2, ELN, EMD, EYA4, FBN1, FBN2, FHL1, FHL2, FKRP, FKTN, FXN, GAA, GATAD1, GCKR, GJA5, GLA, GPD1L, GPIHBP1, HADHA, HCN4, HFE, HRAS, HSPB8, ILK, JAG1, JPH2, JUP, KCNA5, KCND3, KCNE1, KCNE2, KCNE3, KCNH2, KCNJ2, KCNJ5, KCNJ8, KCNQ1, KLF10, KRAS, LAMA2, LAMA4, LAMP2, LDB3, LDLR, LDLRAP1, LMF1, LMNA, LPL, LTBP2, MAP2K1, MAP2K2, MIB1, MURC, MYBPC3, MYH11, MYH6, MYH7, MYL2, MYL3, MYLK, MYLK2, MYO6, MYOZ2, MYPN, NEXN, NKX2-5, NODAL, NOTCH1, NPPA, NRAS, PCSK9, PDLIM3, PKP2, PLN, PRDM16, PRKAG2, PRKAR1A, PTPN11, RAF1, RANGRF, RBM20, RYR1, RYR2, SALL4, SCN1B, SCN2B, SCN3B, SCN4B, SCN5A, SCO2, SDHA, SEPN1, SGCB, SGCD, SGCG, SHOC2, SLC25A4, SLC2A10, SMAD3, SMAD4, SNTA1, SOS1, SREBF2, TAZ, TBX20, TBX3, TBX5, TCAP, TGFB2, TGFB3, TGFBR1, TGFBR2, TMEM43, TMPO, TNNC1, TNNI3, TNNT2, TPM1, TRDN, TRIM63, TRPM4, TTN, TTR, TXNRD2, VCL, ZBTB17, ZHX3, and ZIC3) | Arrhythmogenic left ventricular cardiomyopathy (ALVC) | A case of SCD |
| Simons E. et al. (2021) [41] | 61 genes (ABCC9, AKAP9, ANK2, CACNA1C, CACNA2D1, CACNB2, CALM1, CASQ2, CAV3, CTNNA3, DES, DPP6, DSC2, DSG2, DSP, GJA1 (CX43), GJA5 (CX40), GPD1L, HCN4, JUP, KCNA5, KCND3, KCNE1, KCNE2, KCNE3, KCNE5 (KCNE1L), KCNH2, KCNJ2, KCNJ5 (GIRK4), KCNJ8, KCNQ1 (excl. exon 9), LMNA, NKX2-5 (NKX2E), NOS1AP, NPPA, PKP2, PLN, PRKAG2, RANGRF (MOG1), RYR2, SCN1B, SCN2B, SCN3B, SCN4B, SCN5A, SLMAP, SNTA1, TGFB3, TMEM43, TRDN, and TRPM4) | Long QT syndrome type 1 (LQTS1) | A case of SCD |
| Gaertner-Rommel A. et al. (2019) [42] | 174 genes associated with inherited cardiac conditions | Hypertrophic cardiomyopathy (HCM) | A case of SUDY |
| Mahlke N. et al. (2019) [43] | 74 genes associated with inherited cardiovascular conditions | Catecholaminergic polymorphic ventricular tachycardia (CPVT) | A case of SUDY |
| Neubauer J. et al. (2019) [44] | Whole exome | Not specified | A case of SUDY |
| Foti F. et al. (2020) [45] | 174 genes | Arrhythmic heart disease | A case of SUDY |
| Manzanilla-Romero H.H. et al. (2023) [46] | 48 genes for arrhythmias and then whole exome | Myocarditis | A case of SUDY |
| Ripoll-Vera et al. (2020) [47] | Between 194 and 380 genes | Not specified | 62 cases of SCD |
| Mutation | Evaluation | Pathology | Reference |
|---|---|---|---|
| ACTN2: c.355G>A p.(Ala119Thr) | Pathogenic | HCM, DCM | Kraoua L. et al. (2022) [24] |
| CACNA1C c.2573G>A p.(Arg858His) | Pathogenic | LQTS | Larsen M.K. et al. (2020) [21] |
| CALR3 c.387dup p.(Ile130Tyrfs*11) | Pathogenic | Familial HCM, ARVC | Neubauer J. et al. (2021) [23] |
| DSG2 c.2979G>T p.(Gln993His) | Likely pathogenic | ARDV | Simons E. et al. (2021) [41] |
| KCNE1 c.292C>T p.(Arg98Trp) | Likely pathogenic | LQTS | Marcondes L. et al. (2018) [35] |
| KCNH2 c.87C>A p.(Phe29Leu) | Pathogenic | LQTS | Larsen M.K. et al. (2020) [21] |
| KCNH2 c.211G>C p.(Gly71Arg) | Pathogenic | Congenital LQTS | Raju H. et al. (2019) [39] |
| KCNH2 c.1591C>T p.(Arg531Trp) | Likely pathogenic | LQTS type 2 | Scheiper-Welling S. et al. (2022) [24] |
| KCNH2 c.1600C>T p.(Arg534Cys) | Pathogenic | LQTS | Scheiper-Welling S. et al. (2022) [24] |
| KCNH2 c.1682C>T p.(Ala561Val) | Pathogenic/likely pathogenic | LQTS | Marcondes L. et al. (2018) [35] |
| KCNJ2 c.199C>T p.(Arg67Trp) | Pathogenic | LQTS | Marcondes L. et al. (2018) [35] |
| KCNQ1 c.287C>G p.(Thr96Arg) | Likely pathogenic | LQTS | Marcondes L. et al. (2018) [35] |
| KCNQ1 c.568C>T p.(Arg190Trp) | Pathogenic/likely pathogenic | LQTS | Larsen M.K. et al. (2020) [21] |
| KCNQ1 c.727C>T p.(Arg243Cys) | Pathogenic | LQTS | Marcondes L. et al. (2018) [35] |
| KCNQ1 c.969G>A p.(Trp323Ter) | Pathogenic | LQTS | Raju H. et al. (2019) [39] |
| KCNQ1 c.1363C>T p.(His455Tyr) | Pathogenic | LQTS | Marcondes L. et al. (2018) [35] |
| LMNA c.568 C>T p.(Arg190Trp) | Pathogenic | DCM | Marey I. et al. (2020) [15] |
| LMNA c.1412G>A p.(Arg471His) | Pathogenic/likely pathogenic | DCM | Larsen M.K. et al. (2020) [21] |
| LMNA c.1579C>T p. (Arg527Cys) | Pathogenic/likely pathogenic | DCM | Neubauer J. et al. (2018) [37] |
| MYBPC3 c.884delT p.(Phe295fs) | Pathogenic/likely pathogenic | HCM | Siskind T. et al. (2022) [12] |
| MYBPC3 c.2441_2443del p.(Lys814del) | Likely pathogenic | HCM | Girolami F. et al. (2022) [22] |
| MYBPC3 c.2670dup p.(Arg891fs) | Likely pathogenic | HCM | Iglesias M. et al. (2021) [20] |
| MYBPC3 c.2864_2865del p.(PRO955fs) | Pathogenic/likely pathogenic | HCM | Marey I. et al. (2020) [15] |
| MYBPC3 c.2905C>T p.(Gln969Ter) | Pathogenic | HCM | Siskind T. et al. (2022) [12] |
| MYH7 c.1325G>A p.(Arg442His) | Pathogenic/likely pathogenic | HCM | Larsen M.K. et al. (2020) [21] |
| MYH7 c.1955G>A (p.Arg652Lys) | Pathogenic | HCM | Ripoll-Vera T. et al. (2020) [47] |
| MYH7 c.1988G>A p.(Arg663His) | Pathogenic | HCM | Marey I. et al. (2020) [15] |
| MYH7 c.2011C>T p.Arg671Cys | Likely pathogenic | HCM | Martínez-Barrios E. et al. (2023) [26] |
| MYH7 c.2105T>A p.(Ile702Asn) | Pathogenic/likely pathogenic | HCM | Marey I. et al. (2020) [15] |
| MYH7 c.2155C>T p.(Arg719Trp) | Pathogenic | HCM | Marziliano N. et al. (2019) [18] |
| MYH7 c.2606G>A p.(Arg869His) | Likely pathogenic | HCM and DCM | Siskind T. et al. (2022) [16] |
| PKP2 c.235C>T p.(Arg79Ter) | Pathogenic | ARVD | Larsen M.K. et al. (2020) [21] |
| PKP2 c.1237C>T (p.Arg413Ter) | Pathogenic | ARVD | Martínez-Barrios E. et al. (2023) [26] |
| PPA2 c.514G>A (p.Glu172Lys) | Pathogenic | PPA2-related mitochondriopathy | Ripoll-Vera T. et al. (2020) [28] |
| PPA2 c.683C > T p.(Pro228Leu) | Pathogenic | PPA2-related mitochondriopathy | Manzanilla-Romero H.H. et al. (2023) [46] |
| SCN5A c.127C>T p.(Arg43Ter) | Pathogenic | BrS, LQTS type 3 | Scheiper-Welling S. et al. (2022) [24] |
| SCN5A c.1231G>A p.(Val411Met) | Pathogenic | LQTS type 3 | Siskind T. et al. (2022) [16] |
| SCN5A c.2254G>A p.(Gly752Arg) | Pathogenic/likely pathogenic | BrS | Larsen M.K. et al. (2020) [21] |
| RYR2 c.1259G>A p.(Arg420Gln) | Pathogenic | LQTS | Raju H. et al. (2019) [39] |
| RYR2 c.11836G>A p.(Gly3946Ser) | Pathogenic | CPVT | Raju H. et al. (2019) [39] |
| RYR2 c.13735C>T p.(His4579Tyr) | Likely pathogenic | CPVT | Larsen M.K. et al. (2020) [21] |
| RYR2 c.13823G>A p.(Arg4608Gln) | Pathogenic/likely pathogenic | CPVT | Raju H. et al. (2019) [39] |
| RYR2 c.14288A>G p.(Asn4763Ser) | Likely pathogenic | CPVT | Shanks G.W. et al. (2018) [34] |
| TCAP c.360_361del p.(Glu120Aspfs*15) | Likely pathogenic | HCM | Girolami F. et al. (2022) [22] |
| TTN c.94344_94347del p.(Lys31448fs) | Likely pathogenic | DCM | Neubauer J. et al. (2018) [37] |
| TNNI3 c.407G>A p.(Arg136Gln) | Likely pathogenic | HCM | Marey I. et al. (2020) [15] |
| TNNI3 c.509G>A p.(Arg170Gln) | Pathogenic | HCM | Marey I. et al. (2020) [15] |
| TNNI3 c.611G>A p.(Arg204His) | Pathogenic/likely pathogenic | HCM | Martínez-Barrios E. et al. (2023) [26] |
| TNNT2 c.275 G>A p.(Arg92Gln) | Likely pathogenic | HCM and LVNC | Marey I. et al. (2020) [15] |
| TNNT2 c.421C>T p.(Arg141Trp) | Likely pathogenic | HCM-DCM | Marey I. et al. (2020) [15] |
| TNNT2 c.517_519del p.(Glu173del) | Pathogenic/Likely pathogenic | HCM | Girolami F. et al. (2022) [22] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tomassini, L.; Ricchezze, G.; Fedeli, P.; Lancia, M.; Gambelunghe, C.; De Micco, F.; Cingolani, M.; Scendoni, R. New Insights on Molecular Autopsy in Sudden Death: A Systematic Review. Diagnostics 2024, 14, 1151. https://doi.org/10.3390/diagnostics14111151
Tomassini L, Ricchezze G, Fedeli P, Lancia M, Gambelunghe C, De Micco F, Cingolani M, Scendoni R. New Insights on Molecular Autopsy in Sudden Death: A Systematic Review. Diagnostics. 2024; 14(11):1151. https://doi.org/10.3390/diagnostics14111151
Chicago/Turabian StyleTomassini, Luca, Giulia Ricchezze, Piergiorgio Fedeli, Massimo Lancia, Cristiana Gambelunghe, Francesco De Micco, Mariano Cingolani, and Roberto Scendoni. 2024. "New Insights on Molecular Autopsy in Sudden Death: A Systematic Review" Diagnostics 14, no. 11: 1151. https://doi.org/10.3390/diagnostics14111151
APA StyleTomassini, L., Ricchezze, G., Fedeli, P., Lancia, M., Gambelunghe, C., De Micco, F., Cingolani, M., & Scendoni, R. (2024). New Insights on Molecular Autopsy in Sudden Death: A Systematic Review. Diagnostics, 14(11), 1151. https://doi.org/10.3390/diagnostics14111151