
Transition from Transrectal to Transperineal MRI-Fusion Prostate Biopsy Does Not Comprise Detection Rates of Clinically Significant Prostate Cancer at a Tertiary Care Center

 , , ,
, , ,
Abstract
:1. Introduction
2. Material and Methods
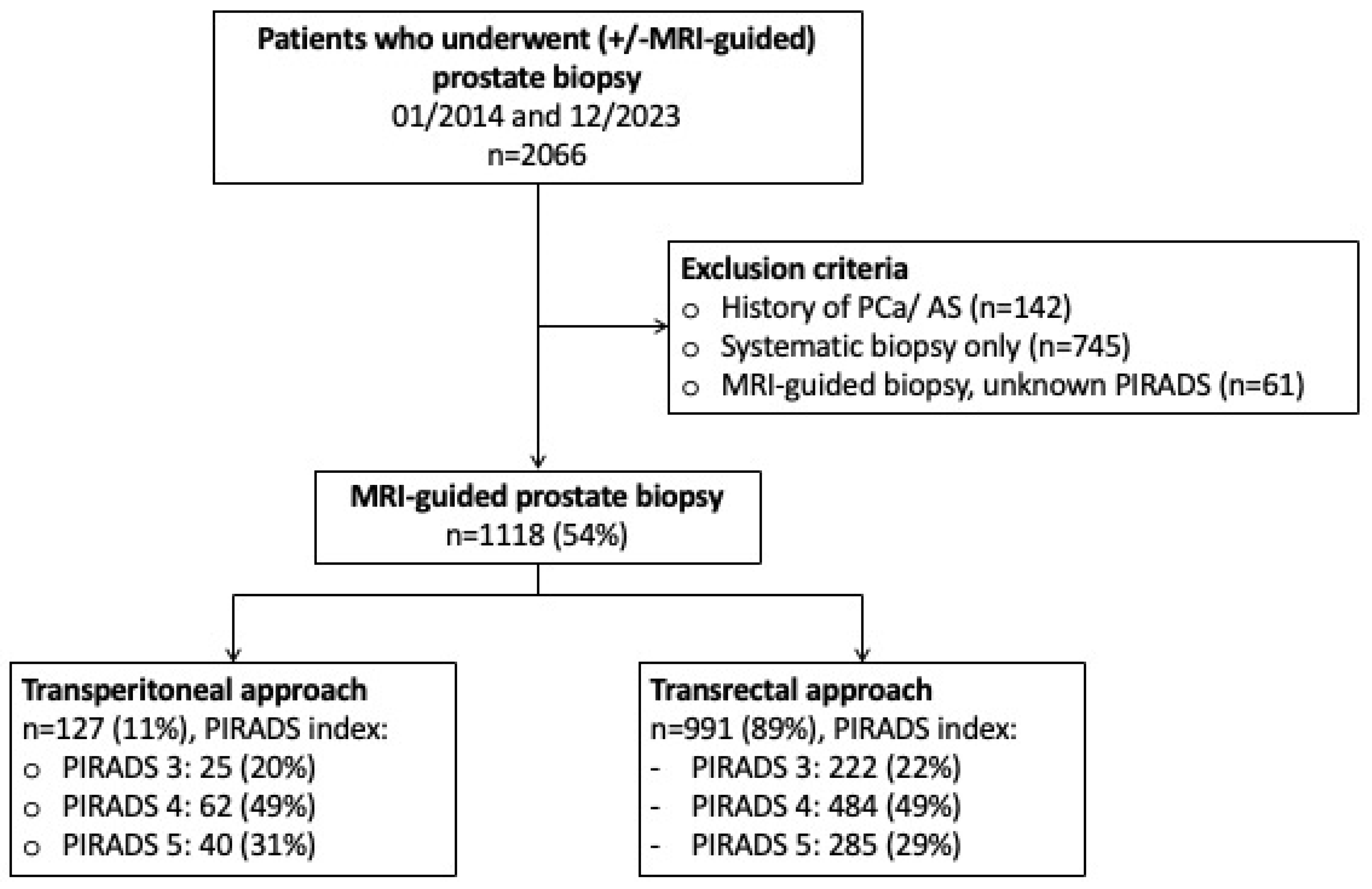
2.1. Study Population
2.2. Outcome Measurement
2.3. Statistical Analyses
3. Results
3.1. Descriptive Characteristics of the Study Population
3.2. Detection Rates of Clinically Significant Prostate Cancer
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Culp, M.B.; Soerjomataram, I.; Efstathiou, J.A.; Bray, F.; Jemal, A. Recent Global Patterns in Prostate Cancer Incidence and Mortality Rates. Eur. Urol. 2020, 77, 38–52. [Google Scholar] [CrossRef] [PubMed]
- Cornford, P.; Tilki, D.; Van Den Bergh, R.C.N. EAU Guidelines. Edn. Presented at the EAU Annual Congress Paris April 2024. ISBN 978-94-92671-23-3. Published online 2024. Available online: http://uroweb.org/guidelines/compilations-of-all-guidelines/ (accessed on 15 May 2024).
- Iczkowski, K.A.; van Leenders, G.J.L.H.; van der Kwast, T.H. The 2019 International Society of Urological Pathology (ISUP) Consensus Conference on Grading of Prostatic Carcinoma. Am. J. Surg. Pathol. 2021, 45, 1007. [Google Scholar] [CrossRef] [PubMed]
- Kasivisvanathan, V.; Rannikko, A.S.; Borghi, M.; Panebianco, V.; Mynderse, L.A.; Vaarala, M.H.; Briganti, A.; Budäus, L.; Hellawell, G.; Hindley, R.G.; et al. MRI-Targeted or Standard Biopsy for Prostate-Cancer Diagnosis. N. Engl. J. Med. 2018, 378, 1767–1777. [Google Scholar] [CrossRef] [PubMed]
- Rouvière, O.; Puech, P.; Renard-Penna, R.; Claudon, M.; Roy, C.; Mège-Lechevallier, F.; Decaussin-Petrucci, M.; Dubreuil-Chambardel, M.; Magaud, L.; Remontet, L.; et al. Use of prostate systematic and targeted biopsy on the basis of multiparametric MRI in biopsy-naive patients (MRI-FIRST): A prospective, multicentre, paired diagnostic study. Lancet Oncol. 2019, 20, 100–109. [Google Scholar] [CrossRef] [PubMed]
- Klotz, L.; Chin, J.; Black, P.C.; Finelli, A.; Anidjar, M.; Bladou, F.; Mercado, A.; Levental, M.; Ghai, S.; Chang, S.D.; et al. Comparison of Multiparametric Magnetic Resonance Imaging–Targeted Biopsy With Systematic Transrectal Ultrasonography Biopsy for Biopsy-Naive Men at Risk for Prostate Cancer: A Phase 3 Randomized Clinical Trial. JAMA Oncol. 2021, 7, 534. [Google Scholar] [CrossRef] [PubMed]
- Drost, F.-J.H.; Osses, D.F.; Nieboer, D.; Steyerberg, E.W.; Bangma, C.H.; Roobol, M.J.; Schoots, I.G. Prostate MRI, with or without MRI-targeted biopsy, and systematic biopsy for detecting prostate cancer. Cochrane Database Syst. Rev. 2019, 4, CD012663. [Google Scholar] [CrossRef] [PubMed]
- Cornford, M.; van der Berg, R.C.H. EAU Guidelines. Edn. Presented at the EAU Annual Congress Milan 2023. 2023. ISBN 978-94-92671-19-6. Available online: http://uroweb.org/guidelines/compilations-of-all-guidelines (accessed on 4 January 2024).
- Berridge, C.; Omer, A.; Lopez, F.; Bryant, R.J.; Lamb, A.D. Perspectives on technology—Prostate cancer: Is local anaesthetic transperineal prostate biopsy really better than transrectal biopsy? BJU Int. 2024. [Google Scholar] [CrossRef]
- Ploussard, G.; Barret, E.; Fiard, G.; Lenfant, L.; Malavaud, B.; Giannarini, G.; Almeras, C.; Aziza, R.; Renard-Penna, R.; Descotes, J.-L.; et al. Transperineal Versus Transrectal Magnetic Resonance Imaging–targeted Biopsies for Prostate Cancer Diagnosis: Final Results of the Randomized PERFECT trial (CCAFU-PR1). Eur. Urol. Oncol. 2024. [Google Scholar] [CrossRef] [PubMed]
- Rai, B.P.; Mayerhofer, C.; Somani, B.K.; Kallidonis, P.; Nagele, U.; Tokas, T. Magnetic Resonance Imaging/Ultrasound Fusion-guided Transperineal Versus Magnetic Resonance Imaging/Ultrasound Fusion-guided Transrectal Prostate Biopsy—A Systematic Review. Eur. Urol. Oncol. 2021, 4, 904–913. [Google Scholar] [CrossRef]
- Lenfant, L.; Barret, E.; Rouprêt, M.; Rozet, F.; Ploussard, G.; Mozer, P. Transperineal Prostate Biopsy Is the New Black: What Are the Next Targets? Eur. Urol. 2022, 82, 3–5. [Google Scholar] [CrossRef]
- Wu, Q.; Tu, X.; Zhang, C.; Ye, J.; Lin, T.; Liu, Z.; Yang, L.; Qiu, S.; Bao, Y.; Wei, Q. Transperineal magnetic resonance imaging targeted biopsy versus transrectal route in the detection of prostate cancer: A systematic review and meta-analysis. Prostate Cancer Prostatic Dis. 2024, 27, 212–221. [Google Scholar] [CrossRef] [PubMed]
- Diamand, R.; Guenzel, K.; Mjaess, G.; Lefebvre, Y.; Ferriero, M.; Simone, G.; Fourcade, A.; Fournier, G.; Bui, A.-P.; Taha, F.; et al. Transperineal or Transrectal Magnetic Resonance Imaging–targeted Biopsy for Prostate Cancer Detection. Eur. Urol. Focus 2024. [Google Scholar] [CrossRef] [PubMed]
- El-Achkar, A.; Heidar, N.A.; Labban, M.; Al-Moussawy, M.; Moukaddem, H.; Nasr, R.; Khauli, R.; El-Hajj, A.; Bulbul, M. MRI/US fusion transperineal versus transrectral biopsy of prostate cancer: Outcomes and complication rates, a tertiary medical center experience in the Middle East. Turk. J. Urol. 2022, 48, 98–105. [Google Scholar] [CrossRef] [PubMed]
- Uleri, A.; Baboudjian, M.; Tedde, A.; Gallioli, A.; Long-Depaquit, T.; Palou, J.; Basile, G.; Gaya, J.M.; Sanguedolce, F.; Lughezzani, G.; et al. Is There an Impact of Transperineal Versus Transrectal Magnetic Resonance Imaging–targeted Biopsy in Clinically Significant Prostate Cancer Detection Rate? A Systematic Review and Meta-analysis. Eur. Urol. Oncol. 2023, 6, 621–628. [Google Scholar] [CrossRef] [PubMed]
- Weinreb, J.C.; Barentsz, J.O.; Choyke, P.L.; Cornud, F.; Haider, M.A.; Macura, K.J.; Margolis, D.; Schnall, M.D.; Shtern, F.; Tempany, C.M.; et al. PI-RADS Prostate Imaging—Reporting and Data System: 2015, Version 2. Eur. Urol. 2016, 69, 16–40. [Google Scholar] [CrossRef] [PubMed]
- Turkbey, B.; Rosenkrantz, A.B.; Haider, M.A.; Padhani, A.R.; Villeirs, G.; Macura, K.J.; Tempany, C.M.; Choyke, P.L.; Cornud, F.; Margolis, D.J.; et al. Prostate Imaging Reporting and Data System Version 2.1: 2019 Update of Prostate Imaging Reporting and Data System Version 2. Eur. Urol. 2019, 76, 340–351. [Google Scholar] [CrossRef] [PubMed]
- Humke, C.; Hoeh, B.; Preisser, F.; Wenzel, M.; Welte, M.N.; Theissen, L.; Bodelle, B.; Koellermann, J.; Steuber, T.; Haese, A.; et al. Concordance between Preoperative mpMRI and Pathological Stage and Its Influence on Nerve-Sparing Surgery in Patients with High-Risk Prostate Cancer. Curr. Oncol. 2022, 29, 2385–2394. [Google Scholar] [CrossRef] [PubMed]
- Mandel, P.; Wenzel, M.; Hoeh, B.; Welte, M.N.; Preisser, F.; Inam, T.; Wittler, C.; Humke, C.; Köllermann, J.; Wild, P.; et al. Immunohistochemistry for Prostate Biopsy—Impact on Histological Prostate Cancer Diagnoses and Clinical Decision Making. Curr. Oncol. 2021, 28, 2123–2133. [Google Scholar] [CrossRef] [PubMed]
- Cindolo, L.; Bertolo, R.; Minervini, A.; Sessa, F.; Muto, G.; Bove, P.; Vittori, M.; Bozzini, G.; Castellan, P.; Mugavero, F.; et al. External validation of Cormio nomogram for predicting all prostate cancers and clinically significant prostate cancers. World J. Urol. 2020, 38, 2555–2561. [Google Scholar] [CrossRef]
- Hu, J.C.; Assel, M.; Allaf, M.E.; Ehdaie, B.; Vickers, A.J.; Cohen, A.J.; Ristau, B.T.; Green, D.A.; Han, M.; Rezaee, M.E.; et al. Transperineal Versus Transrectal Magnetic Resonance Imaging–targeted and Systematic Prostate Biopsy to Prevent Infectious Complications: The PREVENT Randomized Trial. Eur. Urol. 2024. [Google Scholar] [CrossRef]
- Mian, B.M.; Feustel, P.J.; Aziz, A.; Kaufman, R.P.; Bernstein, A.; Avulova, S.; Fisher, H.A. Complications Following Transrectal and Transperineal Prostate Biopsy: Results of the ProBE-PC Randomized Clinical Trial. J. Urol. 2024, 211, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Bonkat, G.; Pilatz, A.; Wagenlehner, F. Time to Adapt Our Practice? The European Commission Has Restricted the Use of Fluoroquinolones since March 2019. Eur. Urol. 2019, 76, 273–275. [Google Scholar] [CrossRef] [PubMed]
- Wenzel, M.; von Hardenberg, J.; Welte, M.N.; Doryumu, S.; Hoeh, B.; Wittler, C.; Höfner, T.; Kriegmair, M.C.; Michel, M.S.; Chun, F.K.H.; et al. Monoprophylaxis With Cephalosporins for Transrectal Prostate Biopsy After the Fluoroquinolone-Era: A Multi-Institutional Comparison of Severe Infectious Complications. Front. Oncol. 2021, 11, 684144. [Google Scholar] [CrossRef] [PubMed]
- Alidjanov, J.F.; Cai, T.; Bartoletti, R.; Bonkat, G.; Bruyère, F.; Köves, B.; Kulchavenya, E.; Medina-Polo, J.; Naber, K.; Perepanova, T.; et al. The negative aftermath of prostate biopsy: Prophylaxis, complications and antimicrobial stewardship: Results of the global prevalence study of infections in urology 2010–2019. World J. Urol. 2021, 39, 3423–3432. [Google Scholar] [CrossRef] [PubMed]
- Sigle, A.; Borkowetz, A.; von Hardenberg, J.; Drerup, M.; Kornienko, K.; Kwe, J.; Wenzel, M.; Mandel, P.; Westhoff, N.; Rieger, C.; et al. Prediction of Significant Prostate Cancer in Equivocal Magnetic Resonance Imaging Lesions: A High-volume International Multicenter Study. Eur. Urol. Focus 2023, 9, 606–613. [Google Scholar] [CrossRef]
- Park, K.J.; Choi, S.H.; Lee, J.S.; Kim, J.K.; Kim, M. Interreader Agreement with Prostate Imaging Reporting and Data System Version 2 for Prostate Cancer Detection: A Systematic Review and Meta-Analysis. J. Urol. 2020, 204, 661–670. [Google Scholar] [CrossRef]

{kind=link}
| N | Overall, n = 1118 | Transrectal Biopsy, n = 991 (89%) | Transperineal Biopsy, n = 127 (11%) | p-Value | |
|---|---|---|---|---|---|
| Age at biopsy [years] Median (IQR) | 1118 | 66 (60, 72) | 66 (60, 72) | 67 (60, 72) | 0.2 |
| Prostate-specific antigen [ng/mL] Median (IQR) | 1117 | 7 (5, 10) | 7 (5, 10) | 7 (5, 10) | 0.2 |
| Prostate volume [mL] Median (IQR) | 1097 | 48 (35, 70) | 50 (36, 70) | 45 (35, 60) | 0.087 |
| Total number of cores Median (IQR) | 1113 | 15 (13, 17) | 14 (13, 17) | 17 (16, 19) | <0.001 |
| Number of cores: Systematic Median (IQR) | 1113 | 12 (12, 12) | 12 (12, 12) | 12 (12, 12) | 0.4 |
| Number of cores: PIRADS Median (IQR) | 1114 | 3 (1, 5) | 2 (1, 5) | 5 (4, 7) | <0.001 |
| Digital rectal examination n (%) | 1118 | 0.057 | |||
| Suspicous | 250 (22%) | 230 (23%) | 20 (16%) | ||
| Non-suspicous | 868 (78%) | 761 (77%) | 107 (84%) | ||
| Number of prior (negative) biopsies n (%) | 1118 | 0.008 | |||
| 0 | 865 (77%) | 753 (76%) | 112 (88%) | ||
| 1 | 193 (17%) | 181 (18%) | 12 (9.4%) | ||
| ≥2 | 60 (5.4%) | 57 (5.8%) | 3 (2.4%) | ||
| Index PIRADS lesion n (%) | 1118 | 0.7 | |||
| 3 | 247 (22%) | 222 (22%) | 25 (20%) | ||
| 4 | 546 (49%) | 484 (49%) | 62 (49%) | ||
| 5 | 325 (29%) | 285 (29%) | 40 (31%) | ||
| Number of PIRADS lesions n (%) | 1118 | 0.075 | |||
| 1 | 800 (72%) | 718 (72%) | 82 (65%) | ||
| ≥2 | 318 (28%) | 273 (28%) | 45 (35%) |
| Overall Cohort | PIRADS 3 | PIRADS 4 | PIRADS 5 | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Overall | TR n = 991 (89%) | TP n = 127 (11%) | p-Value | Overall, n = 247 | TR n = 222 (90%) | TP n = 25 (10%) | p-Value | Overall, n = 546 | TR n = 484 (89%) | TP n = 62 (11%) | p-Value | Overall, n = 325 | TR n = 285 (88%) | TP n = 40 (12%) | p-Value | |
| ISUP or GS at biopsy n (%) | 0.8 | >0.9 | 0.9 | >0.9 | ||||||||||||
| No PCa | 358 (32%) | 319 (32%) | 39 (31%) | 134 (54%) | 121 (55%) | 13 (52%) | 174 (32%) | 154 (32%) | 20 (32%) | 50 (15%) | 44 (15%) | 6 (15%) | ||||
| ISUP 1 or GS 3 + 3 | 179 (16%) | 156 (16%) | 23 (18%) | 56 (23%) | 50 (23%) | 6 (24%) | 95 (17%) | 83 (17%) | 12 (19%) | 28 (8.6%) | 23 (8.1%) | 5 (12%) | ||||
| ISUP ≥ 2 or GS ≥ 3 + 4 | 581 (52%) | 516 (52%) | 65 (51%) | 57 (23%) | 51 (23%) | 6 (24%) | 277 (51%) | 247 (51%) | 30 (48%) | 247 (76%) | 218 (76%) | 29 (72%) | ||||
| Univariable | Multivariable * | ||||||
|---|---|---|---|---|---|---|---|
| Odds Ratio | 95%-CI | p-Value | Odds Ratio | 95%-CI | p-Value | ||
| PIRADS 3 | Biopsy approach | ||||||
| Transrectal | ref. | ref. | |||||
| Transperineal | 1.06 | 0.37–2.66 | 0.91 | 0.64 | 0.17–2.11 | 0.49 | |
| PIRADS 4 | Biopsy approach | ||||||
| Transrectal | ref. | ref. | |||||
| Transperineal | 0.90 | 0.53–1.53 | 0.69 | 0.82 | 0.44–1.52 | 0.52 | |
| PIRADS 5 | Biopsy approach | ||||||
| Transrectal | ref. | ref. | |||||
| Transperineal | 0.81 | 0.39–1.77 | 0.58 | 0.63 | 0.24–1.71 | 0.35 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hoeh, B.; Wenzel, M.; Humke, C.; Cano Garcia, C.; Siech, C.; Schneider, M.; Lange, C.; Traumann, M.; Köllermann, J.; Preisser, F.; et al. Transition from Transrectal to Transperineal MRI-Fusion Prostate Biopsy Does Not Comprise Detection Rates of Clinically Significant Prostate Cancer at a Tertiary Care Center. Diagnostics 2024, 14, 1184. https://doi.org/10.3390/diagnostics14111184
Hoeh B, Wenzel M, Humke C, Cano Garcia C, Siech C, Schneider M, Lange C, Traumann M, Köllermann J, Preisser F, et al. Transition from Transrectal to Transperineal MRI-Fusion Prostate Biopsy Does Not Comprise Detection Rates of Clinically Significant Prostate Cancer at a Tertiary Care Center. Diagnostics. 2024; 14(11):1184. https://doi.org/10.3390/diagnostics14111184
Chicago/Turabian StyleHoeh, Benedikt, Mike Wenzel, Clara Humke, Cristina Cano Garcia, Carolin Siech, Melissa Schneider, Carsten Lange, Miriam Traumann, Jens Köllermann, Felix Preisser, and et al. 2024. "Transition from Transrectal to Transperineal MRI-Fusion Prostate Biopsy Does Not Comprise Detection Rates of Clinically Significant Prostate Cancer at a Tertiary Care Center" Diagnostics 14, no. 11: 1184. https://doi.org/10.3390/diagnostics14111184