
Comparison between the Friedewald, Martin and Sampson Equations and LDL-C Quantification by Ultracentrifugation in a Mexican Population

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Population
2.2. Blood Sampling
2.3. Laboratory Analysis
2.4. Dyslipidemia Definition
2.5. Sample Preparation
2.6. Ultracentrifugation Phase I: Removal of Chylomicrons, Very Low-Density Lipoproteins (VLDL), and Intermediate-Density Lipoproteins (IDL)
2.7. Isolation of LDL
2.8. LDL Wash and Dialysis
2.9. LDL Quantitation
2.10. Statistical Analysis
2.11. Ethics Committee
3. Results
3.1. Characteristics of the Study Population
3.2. LDL-C Levels Estimated with the 3 Equations and Quantified after Ultracentrifugation Isolation
3.3. Correlation Test
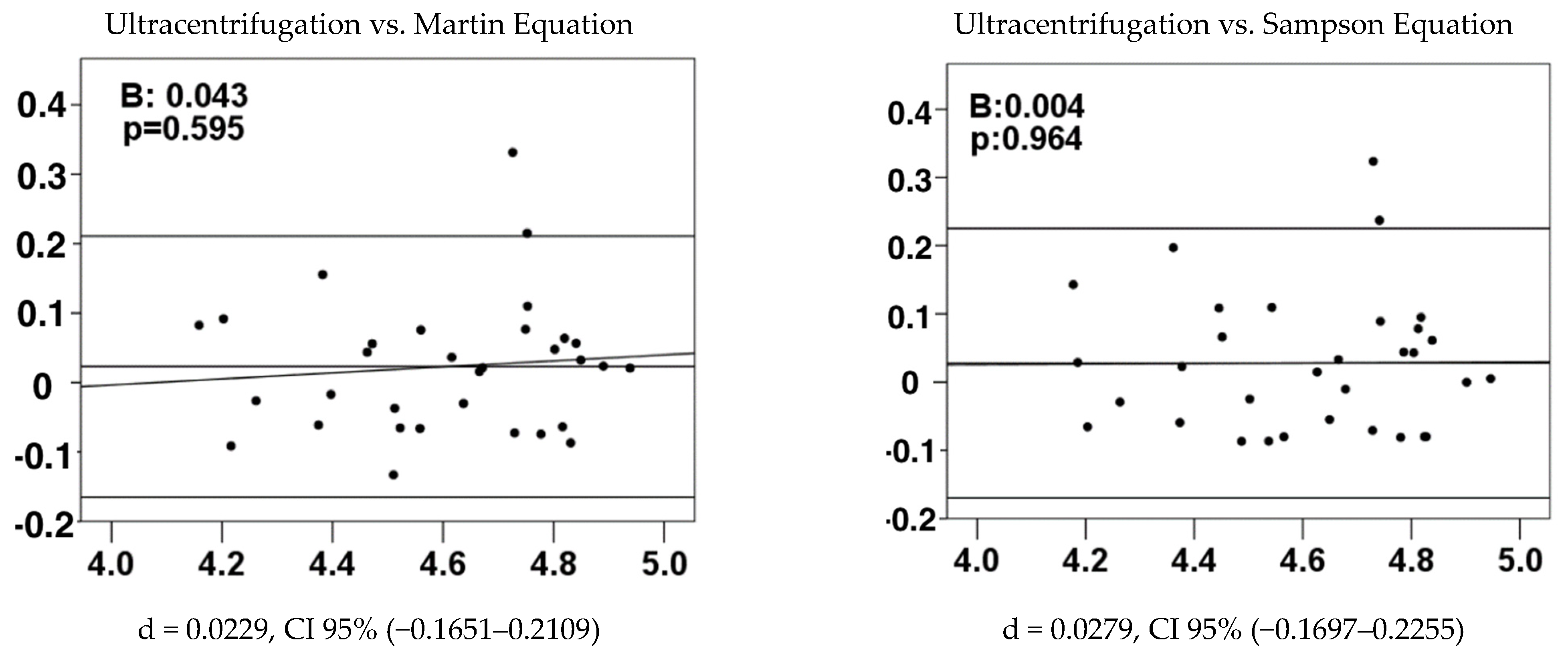
3.4. Concordance Test
4. Discussion
- Non-Dyslipidemic Controls:
- Dyslipidemic Controls:
- Coronary Artery Disease (CAD) Group:
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jeong, S.; Choi, S.; Kim, K.; Kim, S.M.; Lee, G.; Park, S.Y.; Kim, Y.; Son, J.S.; Yun, J.; Park, S.M. Effect of Change in Total Cholesterol Levels on Cardiovascular Disease Among Young Adults. J. Am. Heart Assoc. 2018, 7, e008819. [Google Scholar] [CrossRef] [PubMed]
- Elshourbagy, N.A.; Meyers, H.V.; Abdel-Meguid, S.S. Cholesterol: The Good, the Bad, and the Ugly—Therapeutic Targets for the Treatment of Dyslipidemia. Med. Princ. Pract. 2014, 23, 99–111. [Google Scholar] [CrossRef] [PubMed]
- Du, Z.; Qin, Y. Dyslipidemia and Cardiovascular Disease: Current Knowledge, Existing Challenges, and New Opportunities for Management Strategies. J. Clin. Med. 2023, 12, 363. [Google Scholar] [CrossRef] [PubMed]
- Berberich, A.J.; Hegele, R.A. A Modern Approach to Dyslipidemia. Endocr. Rev. 2022, 43, 611–653. [Google Scholar] [CrossRef]
- Pavía-López, A.A.; Alcocer-Gamba, M.A.; Ruiz-Gastélum, E.D.; Mayorga-Butrón, J.L.; Mehta, R.; Díaz-Aragón, F.A.; Aldrete-Velasco, J.A.; López-Juárez, N.; Cruz-Bautista, I.; Chávez-Mendoza, A.; et al. Guía de práctica clínica mexicana para el diagnóstico y tratamiento de las dislipidemias y enfermedad cardiovascular aterosclerótica. Arch. Cardiol. Mex. 2022, 92, 1–62. [Google Scholar] [CrossRef]
- Mexican Official Norm NOM-037-SSA2-2012. For the prevention, treatment and control of dyslipidemias. Rev. Mex. Cardiol. 2012, 23, 91–124.
- Friedewald, W.T.; I Levy, R.; Fredrickson, D.S. Estimation of the Concentration of Low-Density Lipoprotein Cholesterol in Plasma, Without Use of the Preparative Ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef]
- Martin, S.S.; Blaha, M.J.; Elshazly, M.B.; Toth, P.P.; Kwiterovich, P.O.; Blumenthal, R.S.; Jones, S.R. Comparison of a Novel Method vs the Friedewald Equation for Estimating Low-Density Lipoprotein Cholesterol Levels From the Standard Lipid Profile. JAMA 2013, 310, 2061. [Google Scholar] [CrossRef] [PubMed]
- Sampson, M.; Ling, C.; Sun, Q.; Harb, R.; Ashmaig, M.; Warnick, R.; Sethi, A.; Fleming, J.K.; Otvos, J.D.; Meeusen, J.W.; et al. A New Equation for Calculation of Low-Density Lipoprotein Cholesterol in Patients With Normolipidemia and/or Hypertriglyceridemia. JAMA Cardiol. 2020, 5, 540. [Google Scholar] [CrossRef]
- Samuel, C.; Park, J.; Sajja, A.; Michos, E.D.; Blumenthal, R.S.; Jones, S.R.; Martin, S.S. Accuracy of 23 Equations for Estimating LDL Cholesterol in a Clinical Laboratory Database of 5,051,467 Patients. Glob. Hear. 2023, 18, 36. [Google Scholar] [CrossRef]
- Coverdell, T.C.; Sampson, M.; Zubirán, R.; Wolska, A.; Donato, L.J.; Meeusen, J.W.; Jaffe, A.S.; Remaley, A.T. An improved method for estimating low LDL-C based on the enhanced Sampson-NIH equation. Lipids Health Dis. 2024, 23, 43. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Xin, Y.; Li, J.; Meng, M.; Zhou, L.; Qiu, H.; Chen, H.; Li, H. Evaluation of Sampson equation for LDL-C in acute coronary syndrome patients: A Chinese population-based cohort study. Lipids Health Dis. 2022, 21, 39. [Google Scholar] [CrossRef] [PubMed]
- Mhaimeed, O.; A Burney, Z.; Schott, S.L.; Kohli, P.; A Marvel, F.; Martin, S.S. The importance of LDL-C lowering in atherosclerotic cardiovascular disease prevention: Lower for longer is better. Am. J. Prev. Cardiol. 2024, 18, 100649. [Google Scholar] [CrossRef]
- Ference, B.A.; Ginsberg, H.N.; Graham, I.; Ray, K.K.; Packard, C.J.; Bruckert, E.; Hegele, R.A.; Krauss, R.M.; Raal, F.J.; Schunkert, H.; et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European Atherosclerosis Society Consensus Panel. Eur. Heart J. 2017, 38, 2459–2472. [Google Scholar] [CrossRef]
- Aguilar-Salinas, C.A.; Olaiz, G.; Valles, V.; Torres, J.M.R.; Pérez, F.J.G.; Rull, J.A.; Rojas, R.; Franco, A.; Sepulveda, J. High prevalence of low HDL cholesterol concentrations and mixed hyperlipidemia in a Mexican nationwide survey. J. Lipid Res. 2001, 42, 1298–1307. [Google Scholar] [CrossRef] [PubMed]
- Howard, W.J.; Russell, M.; Fleg, J.L.; Mete, M.; Ali, T.; Devereux, R.B.; Galloway, J.M.; Otvos, J.D.; Ratner, R.E.; Roman, M.J.; et al. Prevention of atherosclerosis with low-density lipoprotein cholesterol lowering—Lipoprotein changes and interactions: The SANDS study. J. Clin. Lipidol. 2009, 3, 322–331. [Google Scholar] [CrossRef] [PubMed]
- A Ference, B.; Mahajan, N. The Role of Early LDL Lowering to Prevent the Onset of Atherosclerotic Disease. Curr. Atheroscler. Rep. 2013, 15, 312. [Google Scholar] [CrossRef] [PubMed]
- Krishnaveni, P. Assessing the Validity of Friedewald’s Formula and Anandraja’s Formula For Serum L DL -Cholesterol Calculation. J. Clin. Diagn. Res. 2015, 9, BC01–BC04. [Google Scholar] [CrossRef] [PubMed]
- Rifai, N.; Warnick, G.R.; McNamara, J.R.; Belcher, J.D.; Grinstead, G.F.; Frantz, I.D. Measurement of low-density-lipoprotein cholesterol in serum: A status report. Clin. Chem. 1992, 38, 150–160. [Google Scholar] [CrossRef]
- Kapoor, R.; Chakraborty, M.; Singh, N. A Leap above Friedewald Formula for Calculation of Low-Density Lipoprotein-Cholesterol. J. Lab. Physicians 2015, 7, 011–016. [Google Scholar] [CrossRef]
- Stroes, E. Statins and LDL-cholesterol lowering: An overview. Curr. Med Res. Opin. 2005, 21, S9–S16. [Google Scholar] [CrossRef] [PubMed]
- Cholesterol Treatment Trialists’ (CTT) Collaborators. The effects of lowering LDL cholesterol with statin therapy in people at low risk of vascular disease: Meta-analysis of individual data from 27 randomised trials. Lancet 2012, 380, 581–590. [Google Scholar] [CrossRef] [PubMed]
- Nawrocki, J.W.; Weiss, S.R.; Davidson, M.H.; Sprecher, D.L.; Schwartz, S.L.; Lupien, P.-J.; Jones, P.H.; Haber, H.E.; Black, D.M. Reduction of LDL Cholesterol by 25% to 60% in Patients With Primary Hypercholesterolemia by Atorvastatin, a New HMG-CoA Reductase Inhibitor. Arter. Thromb. Vasc. Biol. 1995, 15, 678–682. [Google Scholar] [CrossRef] [PubMed]
- Mortensen, M.B.; Dzaye, O.; Bøtker, H.E.; Jensen, J.M.; Maeng, M.; Bentzon, J.F.; Kanstrup, H.; Sørensen, H.T.; Leipsic, J.; Blankstein, R.; et al. Low-Density Lipoprotein Cholesterol Is Predominantly Associated With Atherosclerotic Cardiovascular Disease Events in Patients With Evidence of Coronary Atherosclerosis: The Western Denmark Heart Registry. Circulation 2023, 147, 1053–1063. [Google Scholar] [CrossRef] [PubMed]
- Bolli, A.; Di Domenico, P.; Pastorino, R.; Busby, G.B.; Bottà, G. Risk of Coronary Artery Disease Conferred by Low-Density Lipoprotein Cholesterol Depends on Polygenic Background. Circulation 2021, 143, 1452–1454. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Hao, D.; Che, Y.; Zhang, L.; Zhang, S. Structural Basis and Functional Mechanism of Lipoprotein in Cholesterol Transport. In Cholesterol—Good, Bad and the Heart; InTech: Houston, TX, USA, 2018. [Google Scholar] [CrossRef]
- Chapman, M.J.; Ginsberg, H.N.; Amarenco, P.; Andreotti, F.; Borén, J.; Catapano, A.L.; Descamps, O.S.; Fisher, E.; Kovanen, P.T.; Kuivenhoven, J.A.; et al. Triglyceride-rich lipoproteins and high-density lipoprotein cholesterol in patients at high risk of cardiovascular disease: Evidence and guidance for management. Eur. Heart J. 2011, 32, 1345–1361. [Google Scholar] [CrossRef] [PubMed]
- Morofuji, Y.; Nakagawa, S.; Ujifuku, K.; Fujimoto, T.; Otsuka, K.; Niwa, M.; Tsutsumi, K. Beyond Lipid-Lowering: Effects of Statins on Cardiovascular and Cerebrovascular Diseases and Cancer. Pharmaceuticals 2022, 15, 151. [Google Scholar] [CrossRef] [PubMed]
- Shi, B.; Wang, H.-Y.; Liu, J.; Cai, Z.; Song, C.; Jia, L.; Yin, D.; Wang, H.; Dou, K.-F.; Song, W. Directly Measured vs. Calculated Low-Density Lipoprotein Cholesterol Does Not Identify Additional Individuals With Coronary Artery Disease and Diabetes at Higher Risk of Adverse Events: Insight From a Large Percutaneous Coronary Intervention Cohort in Asia. Front. Cardiovasc. Med. 2022, 9, 932878. [Google Scholar] [CrossRef] [PubMed]
- Sajja, A.; Park, J.; Sathiyakumar, V.; Varghese, B.; Pallazola, V.A.; Marvel, F.A.; Kulkarni, K.; Muthukumar, A.; Joshi, P.H.; Gianos, E.; et al. Comparison of Methods to Estimate Low-Density Lipoprotein Cholesterol in Patients With High Triglyceride Levels. JAMA Netw. Open 2021, 4, e2128817. [Google Scholar] [CrossRef]
- White, K.T.; Moorthy, M.; O Akinkuolie, A.; Demler, O.; Ridker, P.M.; Cook, N.R.; Mora, S. Identifying an Optimal Cutpoint for the Diagnosis of Hypertriglyceridemia in the Nonfasting State. Clin. Chem. 2015, 61, 1156–1163. [Google Scholar] [CrossRef]
- Nordestgaard, B.G. Triglyceride-Rich Lipoproteins and Atherosclerotic Cardiovascular Disease. Circ. Res. 2016, 118, 547–563. [Google Scholar] [CrossRef] [PubMed]
- Berglund, L.; Brunzell, J.D.; Goldberg, A.C.; Goldberg, I.J.; Sacks, F.; Murad, M.H.; Stalenhoef, A.F.H. Evaluation and Treatment of Hypertriglyceridemia: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2012, 97, 2969–2989. [Google Scholar] [CrossRef] [PubMed]
- Martin, S.S.; Martin, S.S.; Ditmarsch, M.; Ditmarsch, M.; Simmons, M.; Simmons, M.; Alp, N.; Alp, N.; Turner, T.; Turner, T.; et al. Comparison of low-density lipoprotein cholesterol equations in patients with dyslipidaemia receiving cholesterol ester transfer protein inhibition. Eur. Heart J.-Cardiovasc. Pharmacother. 2022, 9, 148–155. [Google Scholar] [CrossRef]
- Chung, S. Correlation of extended Martin/Hopkins equation with a direct homogeneous assay in assessing low-density lipoprotein cholesterol in patients with hypertriglyceridemia. J. Clin. Lab. Anal. 2023, 37, e24963. [Google Scholar] [CrossRef] [PubMed]
- Shiri, H.; Sagha, A.; Nasri, H.; Mehdeipour, S.; Fooladi, S.; Mehrabani, M.; Farhadi, S.; Kharazmi, S.; Nematollahi, M.H. Lithium and zinc levels along with oxidative status in myocardial infarction: A case-control study. Heliyon 2023, 9, e21875. [Google Scholar] [CrossRef] [PubMed]
- Wolska, A.; Remaley, A.T. Measuring LDL-cholesterol: What is the best way to do it? Curr. Opin. Cardiol. 2020, 35, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Zubirán, R.; Vargas-Vazquez, A.; Olvera, F.D.R.; Cruz-Bautista, I.; Martagón-Rosado, A.; Sampson, M.; Remaley, A.T.; Aguilar-Salinas, C.A. Performance of the enhanced Sampson-NIH equation for VLDL-C and LDL-C in a population with familial combined hyperlipidemia. Atherosclerosis 2023, 386, 117364. [Google Scholar] [CrossRef] [PubMed]
- Vargas-Vázquez, A.; Bello-Chavolla, O.Y.; Antonio-Villa, N.E.; Mehta, R.; Cruz-Bautista, I.; Aguilar-Salinas, C.A. Comparative assessment of LDL-C and VLDL-C estimation in familial combined hyperlipidemia using Sampson’s, Martin’s and Friedewald’s equations. Lipids Health Dis. 2021, 20, 46. [Google Scholar] [CrossRef] [PubMed]
- Bello-Chavolla, O.Y.; Aguilar-Salinas, C.A. Factors Influencing Achievement of Low-Density Lipoprotein Cholesterol Goals in Mexico: The International Cholesterol Management Practice Study. Rev. Investig. Clin. 2020, 71, 408–416. [Google Scholar] [CrossRef]
- Shiffman, D.; Louie, J.Z.; Caulfield, M.P.; Nilsson, P.M.; Devlin, J.J.; Melander, O. LDL subfractions are associated with incident cardiovascular disease in the Malmö Prevention Project Study. Atherosclerosis 2017, 263, 287–292. [Google Scholar] [CrossRef]
- Chary, A.; Hedayati, M. Review of Laboratory Methods to Determine HDL and LDL Subclasses and Their Clinical Importance. Rev. Cardiovasc. Med. 2022, 23, 147. [Google Scholar] [CrossRef]
- Tsigalou, C.; Panopoulou, M.; Papadopoulos, C.; Karvelas, A.; Tsairidis, D.; Anagnostopoulos, K. Estimation of low-density lipoprotein cholesterol by machine learning methods. Clin. Chim. Acta 2021, 517, 108–116. [Google Scholar] [CrossRef] [PubMed]
- Joven, J.; Villabona, C.; Vilella, E.; Masana, L.; Albertí, R.; Vallés, M. Abnormalities of Lipoprotein Metabolism in Patients with the Nephrotic Syndrome. N. Engl. J. Med. 1990, 323, 579–584. [Google Scholar] [CrossRef]
- Rubiés-Prat, J.; Reverter, J.L.; Sentí, M.; Pedro-Botet, J.; Salinas, I.; Lucas, A.; Nogués, X.; Sanmartí, A. Calculated Low-Density Lipoprotein Cholesterol Should Not Be Used for Management of Lipoprotein Abnormalities in Patients With Diabetes Mellitus. Diabetes Care 1993, 16, 1081–1086. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Variable | Controls n = 59 | CAD n = 54 | p |
|---|---|---|---|
| Sex (%M/%F) | 55.9%/44.1% | 88.9%/11.1% | - |
| Age (years) | 47 (44–51) | 62 (57–69) | <0.001 |
| BMI (kg/m2) | 27.7 (25.4–29.8) | 26.2 (24.4–27.8) | 0.015 |
| TC (mmol/L) | 4.50 (3.98–5.02) | 3.37 (2.80–4.22) | <0.001 |
| HDL-C (mmol/L) | 1.09 (0.98–1.29) | 0.85 (0.70–0.93) | <0.001 |
| Non-HDL-C (mmol/L) | 3.29 (2.90–3.91) | 2.69 (1.99–3.31) | <0.001 |
| LDL-C (mmol/L) | 2.82 (1.68–5.31) | 2.07 (1.53–2.90) | <0.001 |
| Triglycerides (mmol/L) | 1.33 (1.05–1.95) | 1.47 (1.17–2.13) | 0.300 |
| Glucose (mmol/L) | 5.27 (4.8–5.49) | 5.661 (5.21–6.77) | <0.001 |
| Statins (%) | 0% | 100% | - |
| Smoking (%) | 10.5% | 17.1% | - |
| Alcoholism (%) | 0% | 2.4% | - |
| Variable | Controls (n = 59) | CAD Dyslipidemia (n = 54) | p1 | p2 | |
|---|---|---|---|---|---|
| Non-Dyslipidemia (n = 32) | Dyslipidemia (n = 27) | ||||
| Sex (%M/%F) | 53.3%/43.7% | 60.7%/39.3% | 88.9%/11.1% | - | - |
| Age (years) | 48 (44–53) | 47 (44–50) | 62 (57–69) | 0.393 | <0.001 * |
| BMI (kg/m2) | 26.8 (25.4–28.7) | 28.9 (26.1–31.3) | 26.0 (24.1–27.7) | 0.055 | 0.138 |
| TC (mmol/L) | 4.40 (3.96–4.71) | 4.76 (4.04–5.46) | 3.37 (2.67–4.27) | 0.059 | <0.001 * |
| HDL-C (mmol/L) | 1.22 (1.04–1.40) | 0.96 (0.85–1.16) | 0.78 (0.67–0.90) | <0.001 * | <0.001 * |
| Non-HDL-C (mmol/L) | 3.16 (2.56–3.57) | 3.73 (3.21–4.24) | 2.68 (1.94–3.39) | 0.002 * | 0.033 * |
| Triglycerides (mmol/L) | 1.12 (0.92–1.33) | 2.15 (1.66–2.48) | 1.67 (1.29–2.31) | <0.001 * | <0.001 * |
| Glucose (mmol/L) | 5.27 (4.88–5.49) | 5.66 (5.21–6.77) | 5.85 (5.28–7.89) | 0.831 | <0.001 * |
| Statins (%) | - | - | 100% | - | - |
| Method (mmol/L) | Controls (n = 59) | CAD Dyslipidemia (n = 54) | p1 | p2 | |
|---|---|---|---|---|---|
| Non-Dyslipidemia (n = 32) | Dyslipidemia (n = 27) | ||||
| Ultracentrifugation | 2.72 (2.25–3.21) | 2.82 (2.64–3.35) | 2.07 (1.53–2.90) | 0.206 | 0.009 * |
| Friedewald | 2.61 (2.09–3.01) | 2.67 (2.21–3.17) | 1.74 (1.24–2.35) | 0.438 | <0.001 * |
| Martin | 2.61 (2.21–3.13) | 2.68 (2.35–3.46) | 1.85 (1.40–2.51) | 0.632 | 0.001 * |
| Sampson | 2.61 (2.11–3.09) | 2.86 (2.36–3.50) | 1.82 (1.33–2.45) | 0.193 | 0.001 * |
| Equation | Ultracentrifugation | ||
|---|---|---|---|
| Control (n = 59) | CAD Dyslipidemia (n = 54) | ||
| Dyslipidemia (n = 32) | Non-Dyslipidemia (n = 27) | ||
| Friedewald | 0.023 | <0.001 * | <0.001 * |
| Martin | 0.187 | 0.002 * | <0.001 * |
| Sampson | 0.128 | 0.032 * | <0.001 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fuentevilla-Álvarez, G.; Soto, M.E.; Valdivia, J.A.G.; Torres-Paz, Y.E.; Sámano, R.; Perez-Torres, I.; Gamboa-Ávila, R.; Huesca-Gómez, C. Comparison between the Friedewald, Martin and Sampson Equations and LDL-C Quantification by Ultracentrifugation in a Mexican Population. Diagnostics 2024, 14, 1241. https://doi.org/10.3390/diagnostics14121241
Fuentevilla-Álvarez G, Soto ME, Valdivia JAG, Torres-Paz YE, Sámano R, Perez-Torres I, Gamboa-Ávila R, Huesca-Gómez C. Comparison between the Friedewald, Martin and Sampson Equations and LDL-C Quantification by Ultracentrifugation in a Mexican Population. Diagnostics. 2024; 14(12):1241. https://doi.org/10.3390/diagnostics14121241
Chicago/Turabian StyleFuentevilla-Álvarez, Giovanny, María Elena Soto, José Antonio García Valdivia, Yazmín Estela Torres-Paz, Reyna Sámano, Israel Perez-Torres, Ricardo Gamboa-Ávila, and Claudia Huesca-Gómez. 2024. "Comparison between the Friedewald, Martin and Sampson Equations and LDL-C Quantification by Ultracentrifugation in a Mexican Population" Diagnostics 14, no. 12: 1241. https://doi.org/10.3390/diagnostics14121241
APA StyleFuentevilla-Álvarez, G., Soto, M. E., Valdivia, J. A. G., Torres-Paz, Y. E., Sámano, R., Perez-Torres, I., Gamboa-Ávila, R., & Huesca-Gómez, C. (2024). Comparison between the Friedewald, Martin and Sampson Equations and LDL-C Quantification by Ultracentrifugation in a Mexican Population. Diagnostics, 14(12), 1241. https://doi.org/10.3390/diagnostics14121241