
Diagnostic Challenges in Difficult-to-Localize Insulinomas: A Case Report and Review of Literature


Abstract
:1. Introduction
2. Case Description
2.1. Initial Presentation
2.2. Further Investigations
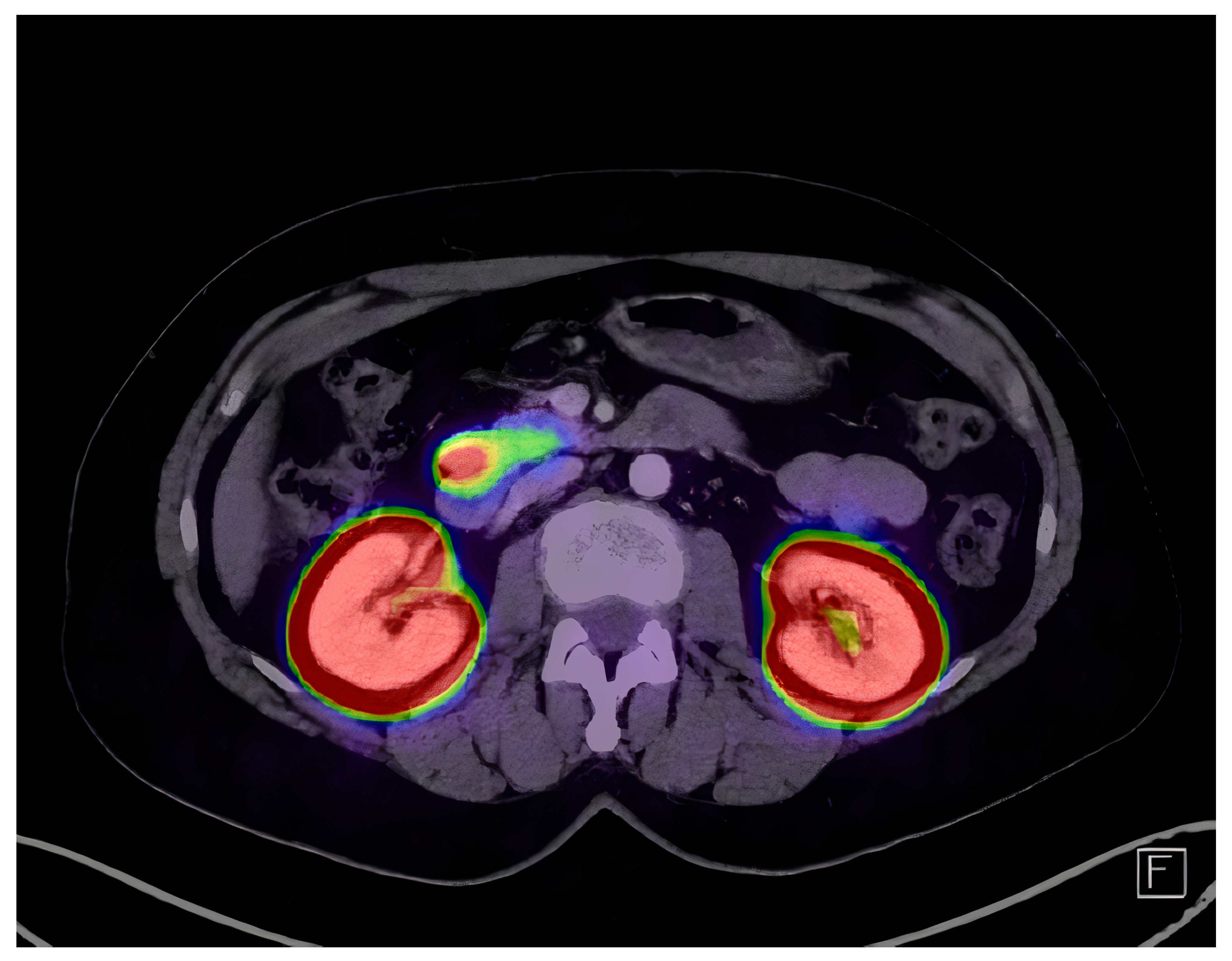
2.3. Imaging and Localization
2.4. Treatment and Outcome
3. Discussion
3.1. Clinical Considerations
3.2. Clinical Diagnosis
3.3. Lesion Localization
3.4. Surgical Treatment
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Service, F.J.; Dale, A.J.; Elveback, L.R.; Jiang, N.S. Insulinoma: Clinical and diagnostic features of 60 consecutive cases. Mayo Clin. Proc. 1976, 51, 417–429. [Google Scholar] [PubMed]
- Grant, C.S. Insulinoma. Best Pract. Res. Clin. Gastroenterol. 2005, 19, 783–798. [Google Scholar] [CrossRef] [PubMed]
- Service, F.J.; McMahon, M.M.; O’Brien, P.C.; Ballard, D.J. Functioning insulinoma–incidence, recurrence, and long-term survival of patients: A 60-year study. Mayo Clin. Proc. 1991, 66, 711–719. [Google Scholar] [CrossRef] [PubMed]
- Placzkowski, K.A.; Vella, A.; Thompson, G.B.; Grant, C.S.; Reading, C.C.; Charboneau, J.W.; Andrews, J.C.; Lloyd, R.V.; Service, F.J. Secular trends in the presentation and management of functioning insulinoma at the Mayo Clinic, 1987-2007. J. Clin. Endocrinol. Metab. 2009, 94, 1069–1073. [Google Scholar] [CrossRef] [PubMed]
- Lewis, M.A.; Thompson, G.B.; Young, W.F. Preoperative Assessment of the Pancreas in Multiple Endocrine Neoplasia Type 1. World J. Surg. 2012, 36, 1375–1381. [Google Scholar] [CrossRef]
- Falconi, M.; Eriksson, B.; Kaltsas, G.; Bartsch, D.; Capdevila, J.; Caplin, M.; Kos-Kudla, B.; Kwekkeboom, D.; Rindi, G.; Klöppel, G.; et al. ENETS Consensus Guidelines Update for the Management of Patients with Functional Pancreatic Neuroendocrine Tumors and Non-Functional Pancreatic Neuroendocrine Tumors. Neuroendocrinology 2016, 103, 153–171. [Google Scholar] [CrossRef]
- Sharma, P.; Arora, S.; Karunanithi, S.; Khadgawat, R.; Durgapal, P.; Sharma, R.; Kandasamy, D.; Bal, C.; Kumar, R. Somatostatin Receptor Based PET/CT Imaging with 68Ga-DOTA-Nal3-octreotide for Localization of Clinically and Biochemically Suspected Insulinoma. Q. J. Nucl. Med. Mol. Imaging 2016, 60, 69–76. [Google Scholar]
- Sharma, P.; Arora, S.; Dhull, V.S.; Naswa, N.; Kumar, R.; Ammini, A.C.; Bal, C. Evaluation of (68)Ga-DOTANOC PET/CT Imaging in a Large Exclusive Population of Pancreatic Neuroendocrine Tumors. Abdom. Imaging 2015, 40, 299–309. [Google Scholar] [CrossRef]
- Christ, E.; Wild, D.; Forrer, F.; Brändle, M.; Sahli, R.; Clerici, T.; Gloor, B.; Martius, F.; Maecke, H.; Reubi, J.C. Glucagon-like peptide-1 receptor imaging for localization of insulinomas. J. Clin. Endocrinol. Metab. 2009, 94, 4398–4405. [Google Scholar] [CrossRef] [PubMed]
- van Dijk, J.G.; Thijs, R.D.; Benditt, D.G.; Wieling, W. A Guide to Disorders Causing Transient Loss of Consciousness: Focus on Syncope. Nat. Rev. Neurol. 2009, 5, 438–448. [Google Scholar] [CrossRef]
- Thijs, R.D.; Benditt, D.G.; Mathias, C.J.; Schondorf, R.; Sutton, R.; Wieling, W.; van Dijk, J.G. Unconscious Confusion–a Literature Search for Definitions of Syncope and Related Disorders. Clin. Auton. Res. 2005, 15, 35–39. [Google Scholar] [CrossRef]
- Easton, J.D.; Saver, J.L.; Albers, G.W.; Alberts, M.J.; Chaturvedi, S.; Feldmann, E.; Hatsukami, T.S.; Higashida, R.T.; Johnston, S.C.; Kidwell, C.S.; et al. Definition and Evaluation of Transient Ischemic Attack: A Scientific Statement for Healthcare Professionals from the American Heart Association/American Stroke Association Stroke Council; Council on Cardiovascular Surgery and Anesthesia; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Nursing; and the Interdisciplinary Council on Peripheral Vascular Disease. The American Academy of Neurology Affirms the Value of This Statement as an Educational Tool for Neurologists. Stroke 2009, 40, 2276–2293. [Google Scholar] [CrossRef]
- Dizon, A.M.; Kowalyk, S.; Hoogwerf, B.J. Neuroglycopenic and other symptoms in patients with insulinomas. Am. J. Med. 1999, 106, 307–310. [Google Scholar] [CrossRef] [PubMed]
- Harrington, M.G.; McGeorge, A.P.; Ballantyne, J.P.; Beastall, G. A prospective survey for insulinomas in a neurology department. Lancet 1983, 1, 1094–1095. [Google Scholar] [CrossRef] [PubMed]
- Service, F. Hypoglycemic Disorders. N. Engl. J. Med. 1995, 332, 1144–1152. [Google Scholar] [CrossRef]
- Service, F.J.; Natt, N.; Thompson, G.B.; Grant, C.S.; van Heerden, J.A.; Andrews, J.C.; Lorenz, E.; Terzic, A.; Lloyd, R.V. Noninsulinoma pancreatogenous hypoglycemia: A novel syndrome of hyperinsulinemic hypoglycemia in adults independent of mutations in Kir6.2 and SUR1 genes. J. Clin. Endocrinol. Metab. 1999, 84, 1582–1589. [Google Scholar] [CrossRef] [PubMed]
- Jg, W.; Hs, T.; Ah, Y.; Kt, T.; Ts, J.; Ch, L.; Hd, L.; N, B.; G, P.; A, V. Clinical Features and Morphological Characterization of 10 Patients with Noninsulinoma Pancreatogenous Hypoglycaemia Syndrome (NIPHS). Clin. Endocrinol. 2006, 65, 566–578. [Google Scholar] [CrossRef]
- Nathan, D.M.; Axelrod, L.; Proppe, K.H.; Wald, R.; Hirsch, H.J.; Martin, D.B. Nesidioblastosis Associated with Insulin-Mediated Hypoglycemia in an Adult. Diabetes Care 1981, 4, 383–388. [Google Scholar] [CrossRef]
- Rostambeigi, N.; Thompson, G.B. What should be done in an operating room when an insulinoma cannot be found? Clin. Endocrinol. 2009, 70, 512–515. [Google Scholar] [CrossRef] [PubMed]
- Low, G.; Panu, A.; Millo, N.; Leen, E. Multimodality Imaging of Neoplastic and Nonneoplastic Solid Lesions of the Pancreas. Radiographics 2011, 31, 993–1015. [Google Scholar] [CrossRef]
- Rha, S.E.; Jung, S.E.; Lee, K.H.; Ku, Y.M.; Byun, J.Y.; Lee, J.M. CT and MR Imaging Findings of Endocrine Tumor of the Pancreas According to WHO Classification. Eur. J. Radiol. 2007, 62, 371–377. [Google Scholar] [CrossRef]
- Anaye, A.; Mathieu, A.; Closset, J.; Bali, M.A.; Metens, T.; Matos, C. Successful Preoperative Localization of a Small Pancreatic Insulinoma by Diffusion-Weighted MRI. JOP J. Pancreas 2009, 10, 528–531. [Google Scholar]
- Sundin, A.; Arnold, R.; Baudin, E.; Cwikla, J.B.; Eriksson, B.; Fanti, S.; Fazio, N.; Giammarile, F.; Hicks, R.J.; Kjaer, A.; et al. ENETS Consensus Guidelines for the Standards of Care in Neuroendocrine Tumors: Radiological, Nuclear Medicine & Hybrid Imaging. Neuroendocrinology 2017, 105, 212–244. [Google Scholar] [CrossRef]
- Moreno-Moreno, P.; Alhambra-Expósito, M.R.; Herrera-Martínez, A.D.; Palomares-Ortega, R.; Zurera-Tendero, L.; Espejo Herrero, J.J.; Gálvez-Moreno, M.A. Arterial Calcium Stimulation with Hepatic Venous Sampling in the Localization Diagnosis of Endogenous Hyperinsulinism. Int. J. Endocrinol. 2016, 2016, 4581094. [Google Scholar] [CrossRef]
- Christ, E.; Antwi, K.; Fani, M.; Wild, D. Innovative imaging of insulinoma: The end of sampling? A review. Endocr.-Relat. Cancer 2020, 27, R79–R92. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Refardt, J.; Hofland, J.; Wild, D.; Christ, E. Molecular Imaging of Neuroendocrine Neoplasms. J. Clin. Endocrinol. Metab. 2022, 107, e2662–e2670. [Google Scholar] [CrossRef] [PubMed]
- Reubi, J.C.; Waser, B. Concomitant expression of several peptide receptors in neuroendocrine tumours: Molecular basis for in vivo multireceptor tumour targeting. Eur. J. Nucl. Med. Mol. Imaging 2003, 30, 781–793. [Google Scholar] [CrossRef] [PubMed]
- Zimmer, T.; Stölzel, U.; Bäder, M.; Koppenhagen, K.; Hamm, B.; Buhr, H.; Riecken, E.O.; Wiedenmann, B. Endoscopic Ultrasonography and Somatostatin Receptor Scintigraphy in the Preoperative Localisation of Insulinomas and Gastrinomas. Gut 1996, 39, 562–568. [Google Scholar] [CrossRef]
- Alsohaibani, F.; Bigam, D.; Kneteman, N.; Shapiro, A.M.J.; Sandha, G.S. The Impact of Preoperative Endoscopic Ultrasound on the Surgical Management of Pancreatic Neuroendocrine Tumours. Can. J. Gastroenterol. = J. Can. Gastroenterol. 2008, 22, 817–820. [Google Scholar] [CrossRef]
- Morganstein, D.L.; Lewis, D.H.; Jackson, J.; Isla, A.; Lynn, J.; Devendra, D.; Meeran, K.; Todd, J.F. The Role of Arterial Stimulation and Simultaneous Venous Sampling in Addition to Cross-Sectional Imaging for Localisation of Biochemically Proven Insulinoma. Eur. Radiol. 2009, 19, 2467–2473. [Google Scholar] [CrossRef]
- Antwi, K.; Fani, M.; Heye, T.; Nicolas, G.; Rottenburger, C.; Kaul, F.; Merkle, E.; Zech, C.J.; Boll, D.; Vogt, D.R.; et al. Comparison of Glucagon-like Peptide-1 Receptor (GLP-1R) PET/CT, SPECT/CT and 3T MRI for the Localisation of Occult Insulinomas: Evaluation of Diagnostic Accuracy in a Prospective Crossover Imaging Study. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 2318–2327. [Google Scholar] [CrossRef]
- Boss, M.; Mikkola, K.; Buitinga, M.; Brom, M.; Wild, D.; Prasad, V.; Brouwers, A.; Pattou, F.; Nuutila, P.; Gotthardt, M. 68Ga-NODAGA-exendin-4 PET/CT for the Localization of Insulinomas. Nuklearmedizin-NuclearMedicine 2019, 58, V31. [Google Scholar] [CrossRef]
- Luo, Y.; Pan, Q.; Yao, S.; Yu, M.; Wu, W.; Xue, H.; Kiesewetter, D.O.; Zhu, Z.; Li, F.; Zhao, Y.; et al. Glucagon-Like Peptide-1 Receptor PET/CT with 68Ga-NOTA-Exendin-4 for Detecting Localized Insulinoma: A Prospective Cohort Study. J. Nucl. Med. 2016, 57, 715–720. [Google Scholar] [CrossRef]
- Thoeni, R.F.; Mueller-Lisse, U.G.; Chan, R.; Do, N.K.; Shyn, P.B. Detection of Small, Functional Islet Cell Tumors in the Pancreas: Selection of MR Imaging Sequences for Optimal Sensitivity. Radiology 2000, 214, 483–490. [Google Scholar] [CrossRef]
- Shah, R.; Garg, R.; Majmundar, M.; Purandare, N.; Malhotra, G.; Patil, V.; Ramteke-Jadhav, S.; Lila, A.; Shah, N.; Bandgar, T. Exendin-4-Based Imaging in Insulinoma Localization: Systematic Review and Meta-Analysis. Clin. Endocrinol. 2021, 95, 354–364. [Google Scholar] [CrossRef]
- Rösch, T.; Lightdale, C.J.; Botet, J.F.; Boyce, G.A.; Sivak, M.V.; Yasuda, K.; Heyder, N.; Palazzo, L.; Dancygier, H.; Schusdziarra, V. Localization of Pancreatic Endocrine Tumors by Endoscopic Ultrasonography. N. Engl. J. Med. 1992, 326, 1721–1726. [Google Scholar] [CrossRef]
- Mehrabi, A.; Fischer, L.; Hafezi, M.; Dirlewanger, A.; Grenacher, L.; Diener, M.K.; Fonouni, H.; Golriz, M.; Garoussi, C.; Fard, N.; et al. A Systematic Review of Localization, Surgical Treatment Options, and Outcome of Insulinoma. Pancreas 2014, 43, 675–686. [Google Scholar] [CrossRef]
- Naples, R.; Thomas, J.D.; Orabi, D.A.; Reynolds, J.P.; Robertson, S.; Siperstein, A.E.; Walsh, R.M.; Simon, R.; Shin, J.J.; Jin, J.; et al. A Critical Analysis of Laparoscopic and Open Approaches to Sporadic Pancreatic Insulinoma Resection in the Modern Era. Am. J. Surg. 2022, 223, 912–917. [Google Scholar] [CrossRef]
- Richards, M.L.; Thompson, G.B.; Farley, D.R.; Kendrick, M.L.; Service, J.F.; Vella, A.; Grant, C.S. Setting the Bar for Laparoscopic Resection of Sporadic Insulinoma. World J. Surg. 2011, 35, 785–789. [Google Scholar] [CrossRef]
- Rossi, G.; Petrone, M.C.; Healey, A.J.; Arcidiacono, P.G. Approaching Small Neuroendocrine Tumors with Radiofrequency Ablation. Diagnostics 2023, 13, 1561. [Google Scholar] [CrossRef]
- Peltola, E.; Hannula, P.; Huhtala, H.; Metso, S.; Sand, J.; Laukkarinen, J.; Tiikkainen, M.; Sirén, J.; Soinio, M.; Nuutila, P.; et al. Long-term morbidity and mortality in patients diagnosed with an insulinoma. Eur. J. Endocrinol. 2021, 185, 577–586. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]


{kind=link}
{kind=link}
{kind=link}
| Characteristics | Median True Positive Rate (Range) | References | |
|---|---|---|---|
| MDCT | Small (<2 cm), well-defined, hypervascular, rarely hypovascular | 63% (40–77%) | [25,28,29,30,31,32,33] |
| MRI | T2WI hyperintense, T1WI hypointense, ADC map | 66% (56–85%) | [25,29,30,31,33,34,34] |
| SRS | Low expression of SSTR (50–60%) | 44% (33–68%) | [7,25,30,31,32,33,35] |
| EUS | EUS guided FNA, superior in the proximal pancreas, rarely isoechoic | 85% (82–93%) | [28,30,33,36] |
| Exendin-4 PET/CT | 94% (85–98%) | [25,31,32,33,35] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grubor, N.M.; Grubor, N.N.; Micev, M. Diagnostic Challenges in Difficult-to-Localize Insulinomas: A Case Report and Review of Literature. Diagnostics 2024, 14, 1600. https://doi.org/10.3390/diagnostics14151600
Grubor NM, Grubor NN, Micev M. Diagnostic Challenges in Difficult-to-Localize Insulinomas: A Case Report and Review of Literature. Diagnostics. 2024; 14(15):1600. https://doi.org/10.3390/diagnostics14151600
Chicago/Turabian StyleGrubor, Nikica M., Nikola N. Grubor, and Marjan Micev. 2024. "Diagnostic Challenges in Difficult-to-Localize Insulinomas: A Case Report and Review of Literature" Diagnostics 14, no. 15: 1600. https://doi.org/10.3390/diagnostics14151600