
Audiovestibular Dysfunction in Systemic Lupus Erythematosus Patients: A Systematic Review
 ,
, {kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods and Materials
2.1. Literature Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Article Screening Process
2.4. Data Extraction
2.5. Article Quality Grading
3. Results and Discussion
3.1. Vestibular System Involvement
3.1.1. Characteristics
3.1.2. Physiopathology
3.1.3. Examination
3.2. Auditory System Involvement
3.2.1. Characteristics
3.2.2. Physiopathology
3.2.3. Examination
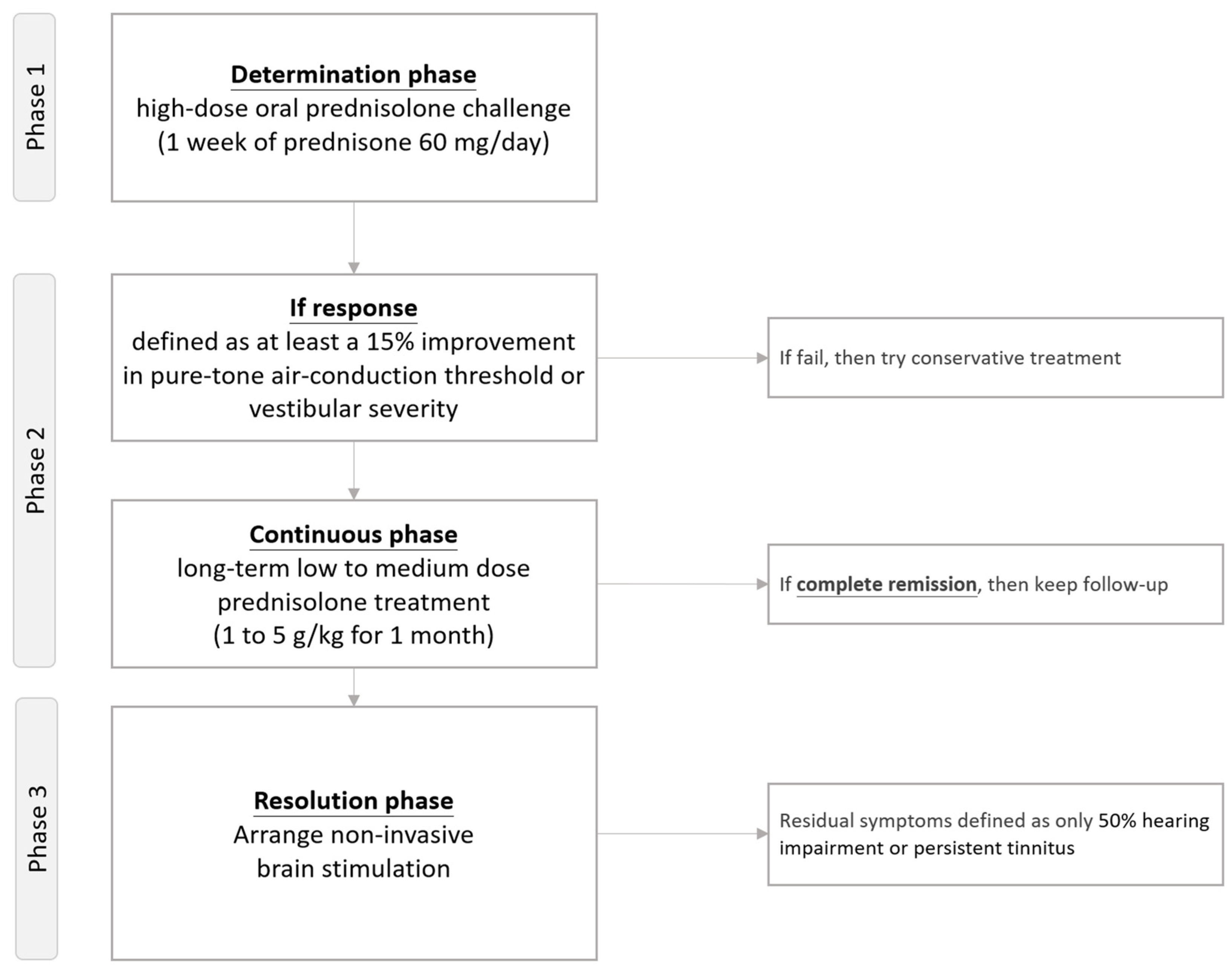
3.3. Treatment of Systemic Lupus Erythematosus-Related Vestibular and Auditory Dysfunction
Temporary Protocol of Steroid Treatment to Manage SLE-Related Audiovestibular Dysfunction
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Magro, R.; Borg, A.A. Characterisation of Patients with Systemic Lupus Erythematosus in Malta: A Population Based Cohort Cross-Sectional Study. Biomed. Res. Int. 2018, 2018, 2385386. [Google Scholar] [CrossRef] [PubMed]
- Anstey, N.M.; Bastian, I.; Dunckley, H.; Currie, B.J. Systemic lupus erythematosus in Australian aborigines: High prevalence, morbidity and mortality. Aust. N. Z. J. Med. 1993, 23, 646–651. [Google Scholar] [CrossRef] [PubMed]
- Lehman, T.; Nuruzzaman, F.; Taber, S. Chapter 8—Systemic Lupus Erythematosus: Etiology, Pathogenesis, Clinical Manifestations, and Management. In Handbook of Systemic Autoimmune Diseases; Cimaz, R., Lehman, T., Eds.; Elsevier: Amsterdam, The Netherlands, 2016; Volume 11, pp. 173–189. [Google Scholar]
- Albrecht, K.; Redeker, I.; Aringer, M.; Marschall, U.; Strangfeld, A.; Callhoff, J. Comorbidity and healthcare utilisation in persons with incident systemic lupus erythematosus followed for 3 years after diagnosis: Analysis of a claims data cohort. Lupus Sci. Med. 2021, 8, e000526. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, N.; Mihara, S.; Sakane, T. Development of pathogenic anti-DNA antibodies in patients with systemic lupus erythematosus. FASEB J. Off. Publ. Fed. Am. Soc. Exp. Biol. 1997, 11, 1033–1038. [Google Scholar] [CrossRef] [PubMed]
- Arnold, W.; Pfaltz, R.; Altermatt, H.J. Evidence of serum antibodies against inner ear tissues in the blood of patients with certain sensorineural hearing disorders. Acta Otolaryngol. 1985, 99, 437–444. [Google Scholar] [CrossRef] [PubMed]
- Ruckenstein, M.J. Autoimmune inner ear disease. Curr. Opin. Otolaryngol. Head. Neck Surg. 2004, 12, 426–430. [Google Scholar] [CrossRef] [PubMed]
- Mathews, J.; Rao, S.; Kumar, B.N. Autoimmune sensorineural hearing loss: Is it still a clinical diagnosis? J. Laryngol. Otol. 2003, 117, 212–214. [Google Scholar] [CrossRef] [PubMed]
- Ralli, M.; Di Stadio, A.; De Virgilio, A.; Croce, A.; de Vincentiis, M. Autoimmunity and Otolaryngology Diseases. J. Immunol. Res. 2018, 2018, 2747904. [Google Scholar] [CrossRef]
- Stone, J.H.; Francis, H.W. Immune-mediated inner ear disease. Curr. Opin. Rheumatol. 2000, 12, 32–40. [Google Scholar] [CrossRef]
- Colletti, V.; Fiorino, F.G.; Bruni, L.; Biasi, D. Middle ear mechanics in subjects with rheumatoid arthritis. Audiology 1997, 36, 136–146. [Google Scholar] [CrossRef]
- Frade, C.; Martin, C. Diagnostic value of the multifrequency tympanometry in active rheumatoid arthritis. Auris Nasus Larynx 1998, 25, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.M.; Zhuang, S.M.; Xiao, Z.W.; Luo, J.Q.; Long, Z.; Lan, L.C.; Zhang, H.Q.; Zhang, G.P. Autoimmune thyroiditis in patients with sudden sensorineural hearing loss. Laryngoscope Investig. Otolaryngol. 2022, 7, 571–577. [Google Scholar] [CrossRef] [PubMed]
- Di Stadio, A.; Ralli, M. Systemic Lupus Erythematosus and hearing disorders: Literature review and meta-analysis of clinical and temporal bone findings. J. Int. Med. Res. 2017, 45, 1470–1480. [Google Scholar] [CrossRef] [PubMed]
- Harris, J.P.; Sharp, P.A. Inner ear autoantibodies in patients with rapidly progressive sensorineural hearing loss. Laryngoscope 1990, 100, 516–524. [Google Scholar] [CrossRef] [PubMed]
- Veldman, J.E.; Roord, J.J.; O’Connor, A.F.; Shea, J.J. Autoimmunity and inner ear disorders: An immune-complex mediated sensorineural hearing loss. Laryngoscope 1984, 94, 501–507. [Google Scholar] [CrossRef]
- Lin, C.; Lin, S.W.; Weng, S.F.; Lin, Y.S. Risk of sudden sensorineural hearing loss in patients with systemic lupus erythematosus: A population-based cohort study. Audiol. Neurootol. 2013, 18, 95–100. [Google Scholar] [CrossRef]
- Garcia-Berrocal, J.R.; De Diego, B.; Roldan-Fidalgo, A.; Yebra-Bango, M.; Millan, I.; Trinidad, A.; Ramirez-Camacho, R. Young systemic lupus erythematosus patients with no hearing involvement: 10-year follow up. J. Laryngol. Otol. 2013, 127, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Abbasi, M.; Yazdi, Z.; Kazemifar, A.M.; Bakhsh, Z.Z. Hearing loss in patients with systemic lupus erythematosus. Glob. J. Health Sci. 2013, 5, 102–106. [Google Scholar] [CrossRef] [PubMed]
- Karatas, E.; Onat, A.M.; Durucu, C.; Baglam, T.; Kanlikama, M.; Altunoren, O.; Buyukhatipoglu, H. Audiovestibular disturbance in patients with systemic lupus erythematosus. Otolaryngol. Head. Neck Surg. 2007, 136, 82–86. [Google Scholar] [CrossRef]
- Rahne, T.; Clauss, F.; Plontke, S.K.; Keysser, G. Prevalence of hearing impairment in patients with rheumatoid arthritis, granulomatosis with polyangiitis (GPA, Wegener’s granulomatosis), or systemic lupus erythematosus. Clin. Rheumatol. 2017, 36, 1501–1510. [Google Scholar] [CrossRef]
- Maciaszczyk, K.; Durko, T.; Waszczykowska, E.; Erkiert-Polguj, A.; Pajor, A. Auditory function in patients with systemic lupus erythematosus. Auris Nasus Larynx 2011, 38, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Green, L.; Miller, E.B. Sudden sensorineural hearing loss as a first manifestation of systemic lupus erythematosus: Association with anticardiolipin antibodies. Clin. Rheumatol. 2001, 20, 220–222. [Google Scholar] [CrossRef] [PubMed]
- Andonopoulos, A.P.; Naxakis, S.; Goumas, P.; Lygatsikas, C. Sensorineural hearing disorders in systemic lupus erythematosus. A controlled study. Clin. Exp. Rheumatol. 1995, 13, 137–141. [Google Scholar] [PubMed]
- Hamblin, T.J.; Mufti, G.J.; Bracewell, A. Severe deafness in systemic lupus erythematosus: Its immediate relief by plasma exchange. Br. Med. J. Clin. Res. Ed. 1982, 284, 1374. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Bmj 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 12 June 2024).
- Kim, J.G.; Lee, S.U.; Lee, C.N.; Yu, S.W.; Park, K.W.; Kim, J.S. Bilateral vestibulopathy as an early manifestation of systemic lupus erythematosus. J. Neurol. 2020, 267, 1855–1858. [Google Scholar] [CrossRef] [PubMed]
- Sperling, N.M.; Tehrani, K.; Liebling, A.; Ginzler, E. Aural symptoms and hearing loss in patients with lupus. Otolaryngol. Head. Neck Surg. 1998, 118, 762–765. [Google Scholar] [CrossRef]
- Batuecas-Caletrio, A.; del Pino-Montes, J.; Cordero-Civantos, C.; Calle-Cabanillas, M.I.; Lopez-Escamez, J.A. Hearing and vestibular disorders in patients with systemic lupus erythematosus. Lupus 2013, 22, 437–442. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.H.; Yang, Y.H.; Chiang, B.L. Systemic lupus erythematosus with presentation as vertigo and vertical nystagmus: Report of one case. Acta Paediatr. Taiwan. 2003, 44, 158–160. [Google Scholar]
- Hughes, G.B.; Moscicki, R.; Barna, B.P.; San Martin, J.E. Laboratory diagnosis of immune inner ear disease. Am. J. Otol. 1994, 15, 198–202. [Google Scholar]
- Brey, R.L.; Holliday, S.L.; Saklad, A.R.; Navarrete, M.G.; Hermosillo-Romo, D.; Stallworth, C.L.; Valdez, C.R.; Escalante, A.; del Rincon, I.; Gronseth, G.; et al. Neuropsychiatric syndromes in lupus: Prevalence using standardized definitions. Neurology 2002, 58, 1214–1220. [Google Scholar] [CrossRef] [PubMed]
- Sibbitt, W.L., Jr.; Sibbitt, R.R.; Brooks, W.M. Neuroimaging in neuropsychiatric systemic lupus erythematosus. Arthritis Rheum. 1999, 42, 2026–2038. [Google Scholar] [CrossRef]
- Ellis, S.G.; Verity, M.A. Central nervous system involvement in systemic lupus erythematosus: A review of neuropathologic findings in 57 cases, 1955–1977. Semin. Arthritis Rheum. 1979, 8, 212–221. [Google Scholar] [CrossRef] [PubMed]
- Kurki, P.; Helve, T.; Dahl, D.; Virtanen, I. Neurofilament antibodies in systemic lupus erythematosus. J. Rheumatol. 1986, 13, 69–73. [Google Scholar] [PubMed]
- Fukushima, N.; Fukushima, H.; Cureoglu, S.; Schachern, P.A.; Paparella, M.M. Hearing loss associated with systemic lupus erythematosus: Temporal bone histopathology. Otol. Neurotol. 2006, 27, 127–128. [Google Scholar] [CrossRef]
- Kariya, S.; Hizli, O.; Kaya, S.; Hizli, P.; Nishizaki, K.; Paparella, M.M.; Cureoglu, S. Histopathologic Findings in Peripheral Vestibular System from Patients with Systemic Lupus Erythematosus: A Human Temporal Bone Study. Otol. Neurotol. 2015, 36, 1702–1707. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, J.M. The immunobiology of autoimmune disease of the inner ear. In Immunology of the Ear; Bernstein, J., Ogra, P., Eds.; Raven Press: New York, NY, USA, 1987; pp. 419–426. [Google Scholar]
- Mouadeb, D.A.; Ruckenstein, M.J. Antiphospholipid inner ear syndrome. Laryngoscope 2005, 115, 879–883. [Google Scholar] [CrossRef] [PubMed]
- Polanski, J.F.; Tanaka, E.A.; Barros, H.; Chuchene, A.G.; Miguel, P.T.G.; Skare, T.L. Chloroquine, Hydroxychloroquine and Hearing Loss: A Study in Systemic Lupus Erythematosus Patients. Laryngoscope 2021, 131, E957–E960. [Google Scholar] [CrossRef] [PubMed]
- Yuen, E.; Fried, J.; Nguyen, S.A.; Rizk, H.G.; Ward, C.; Meyer, T.A. Hearing loss in patients with systemic lupus erythematosus: A systematic review and meta-analysis. Lupus 2021, 30, 937–945. [Google Scholar] [CrossRef]
- Li, X.; Cao, Z.; Chen, F.; Yang, D.; Zhao, F. Sensorineural Hearing Loss in Autoimmune Diseases: A Systematic Review and Meta-analysis. J. Int. Adv. Otol. 2023, 19, 277–282. [Google Scholar] [CrossRef]
- Paraschou, V.; Chaitidis, N.; Papadopoulou, Z.; Theocharis, P.; Siolos, P.; Festas, C. Association of systemic lupus erythematosus with hearing loss: A systemic review and meta-analysis. Rheumatol. Int. 2021, 41, 681–689. [Google Scholar] [CrossRef] [PubMed]
- Roverano, S.; Cassano, G.; Paira, S.; Chiavarini, J.; Graf, C.; Rico, L.; Heredia, C. Asymptomatic sensorineural hearing loss in patients with systemic lupus erythematosus. J. Clin. Rheumatol. 2006, 12, 217–220. [Google Scholar] [CrossRef] [PubMed]
- Gomides, A.P.; do Rosario, E.J.; Borges, H.M.; Gomides, H.H.; de Padua, P.M.; Sampaio-Barros, P.D. Sensorineural dysacusis in patients with systemic lupus erythematosus. Lupus 2007, 16, 987–990. [Google Scholar] [CrossRef] [PubMed]
- Jimenez-Alonso, J.; Gutierrez-Cabello, F.; Castillo, J.L.; Sabio, J.M.; Hidalgo-Tenorio, C.; Leon, L.; Grupo Lupus Virgen de las Nieves. Ear involvement in systemic lupus erythematosus patients: A comparative study. J. Laryngol. Otol. 2002, 116, 746. [Google Scholar] [CrossRef] [PubMed]
- Riera, J.L.; Del, R.M.M.; Musuruana, J.L.; Cavallasca, J.A. Sudden Sensorineural Hearing Loss in Systemic Lupus Erythematosus and Antiphospholipid Syndrome: A Clinical Review. Curr. Rheumatol. Rev. 2020, 16, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Kastanioudakis, I.; Ziavra, N.; Voulgari, P.V.; Exarchakos, G.; Skevas, A.; Drosos, A.A. Ear involvement in systemic lupus erythematosus patients: A comparative study. J. Laryngol. Otol. 2002, 116, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Toubi, E.; Ben-David, J.; Kessel, A.; Podoshin, L.; Golan, T.D. Autoimmune aberration in sudden sensorineural hearing loss: Association with anti-cardiolipin antibodies. Lupus 1997, 6, 540–542. [Google Scholar] [CrossRef]
- Bruner, A.P.; Sato, E.I.; Pereira, L.D. Central auditory processing in patients with systemic lupus erythematosus. Acta Reumatol. Port. 2009, 34, 600–607. [Google Scholar]
- Jung, T.T.; Rhee, C.K.; Lee, C.S.; Park, Y.S.; Choi, D.C. Ototoxicity of salicylate, nonsteroidal antiinflammatory drugs, and quinine. Otolaryngol. Clin. N. Am. 1993, 26, 791–810. [Google Scholar] [CrossRef]
- Fernandes, M.R.N.; Soares, D.B.R.; Thien, C.I.; Carneiro, S. Hydroxychloroquine ototoxicity in a patient with systemic lupus erythematosus. An. Bras. Dermatol. 2018, 93, 469–470. [Google Scholar] [CrossRef]
- Ruckenstein, M.J.; Keithley, E.M.; Bennett, T.; Powell, H.C.; Baird, S.; Harris, J.P. Ultrastructural pathology in the stria vascularis of the MRL-Fasl(lpr) mouse. Hear. Res. 1999, 131, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Rahne, T.; Plontke, S.; Keysser, G. Vasculitis and the ear: A literature review. Curr. Opin. Rheumatol. 2020, 32, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Ralli, M.; D’Aguanno, V.; Di Stadio, A.; De Virgilio, A.; Croce, A.; Longo, L.; Greco, A.; de Vincentiis, M. Audiovestibular Symptoms in Systemic Autoimmune Diseases. J. Immunol. Res. 2018, 2018, 5798103. [Google Scholar] [CrossRef] [PubMed]
- Triplett, J.D.; Buzzard, K.A.; Lubomski, M.; Riminton, D.S.; Barnett, M.H.; Welgampola, M.S.; Halmagyi, G.M.; Nguyen, M.; Landau, K.; Lee, A.G.; et al. Immune-mediated conditions affecting the brain, eye and ear (BEE syndromes). J. Neurol. Neurosurg. Psychiatry 2019, 90, 882–894. [Google Scholar] [CrossRef] [PubMed]
- Caldarelli, D.D.; Rejowski, J.E.; Corey, J.P. Sensorineural hearing loss in lupus erythematosus. Am. J. Otol. 1986, 7, 210–213. [Google Scholar] [PubMed]
- Johnsson, L.G. Vascular pathology in the human inner ear. Adv. Otorhinolaryngol. 1973, 20, 197–220. [Google Scholar] [CrossRef] [PubMed]
- Bouman, H.; Klis, S.F.; de Groot, J.C.; Huizing, E.H.; Smoorenburg, G.F.; Veldman, J.E. Induction of endolymphatic hydrops in the guinea pig by perisaccular deposition of sepharose beads carrying and not carrying immune complexes. Hear. Res. 1998, 117, 119–130. [Google Scholar] [CrossRef]
- Sone, M.; Schachern, P.A.; Paparella, M.M.; Morizono, N. Study of systemic lupus erythematosus in temporal bones. Ann. Otol. Rhinol. Laryngol. 1999, 108, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Yoon, T.H.; Paparella, M.M.; Schachern, P.A. Systemic vasculitis: A temporal bone histopathologic study. Laryngoscope 1989, 99, 600–609. [Google Scholar] [CrossRef]
- Kariya, S.; Kaya, S.; Hizli, O.; Hizli, P.; Nishizaki, K.; Paparella, M.M.; Cureoglu, S. Cochlear Histopathologic Findings in Patients With Systemic Lupus Erythematosus: A Human Temporal Bone Study. Otol. Neurotol. 2016, 37, 593–597. [Google Scholar] [CrossRef]
- Barna, B.P.; Hughes, G.B. Autoimmunity and otologic disease: Clinical and experimental aspects. Clin. Lab. Med. 1988, 8, 385–398. [Google Scholar] [CrossRef] [PubMed]
- Bernard, P. Alterations of auditory evoked potentials during the course of chloroquine treatment. Acta Otolaryngol. 1985, 99, 387–392. [Google Scholar] [CrossRef] [PubMed]
- Lasso de la Vega, M.; Villarreal, I.M.; Lopez Moya, J.; Garcia-Berrocal, J.R. Extended high frequency audiometry can diagnose sub-clinic involvement in a seemingly normal hearing systemic lupus erythematosus population. Acta Otolaryngol. 2017, 137, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Wang, F.; Yang, Y.; Hua, B.; Wang, H.; Chen, J.; Feng, X. Characteristics of Hearing Loss in Patients with Systemic Lupus Erythematosus. J. Clin. Med. 2022, 11, 7527. [Google Scholar] [CrossRef] [PubMed]
- Cordeschi, S.; Salvinelli, F.; D’Ascanio, L. Sensorineural hearing impairment in systemic lupus erythematosus: Sudden or progressive? Clin. Exp. Rheumatol. 2004, 22, 653. [Google Scholar] [PubMed]
- Karabulut, H.; Dagli, M.; Ates, A.; Karaaslan, Y. Results for audiology and distortion product and transient evoked otoacoustic emissions in patients with systemic lupus erythematosus. J. Laryngol. Otol. 2010, 124, 137–140. [Google Scholar] [CrossRef] [PubMed]
- Fradis, M.; Podoshin, L.; Ben-David, J.; Statter, P.; Pratt, H.; Nahir, M. Brainstem auditory evoked potentials with increased stimulus rate in patients suffering from systemic lupus erythematosus. Laryngoscope 1989, 99, 325–329. [Google Scholar] [CrossRef]
- Borton, T.E.; Eby, T.L.; Ball, E.V.; Nolen, B.L.; Bradley, E.L. Stimulus repetition rate effect on the auditory brainstem response in systemic lupus erythematosus. Laryngoscope 1992, 102, 335–339. [Google Scholar] [CrossRef]
- Tan, C.L.; Yahaya, M.H.; Ahmad, N.S.; Lim, C.H. Macrophage activation syndrome as an initial presentation of systemic lupus erythematosus with sensorineural hearing loss in a young male patient. BMJ Case Rep. 2020, 13, e233330. [Google Scholar] [CrossRef]
- Ferrari, A.L.; Calonga, L.; Lapa, A.T.; Postal, M.; Sinicato, N.A.; Pelicari, K.O.; Peres, F.A.; Valente, J.P.; Soki, M.; Appenzeller, S.; et al. Low-Density Lipoprotein Cholesterol Is Associated With Asymptomatic Sensorineural Hearing Loss in Patients With Systemic Lupus Erythematosus. J. Clin. Rheumatol. 2016, 22, 312–315. [Google Scholar] [CrossRef]
- Bowman, C.A.; Linthicum, F.H., Jr.; Nelson, R.A.; Mikami, K.; Quismorio, F. Sensorineural hearing loss associated with systemic lupus erythematosus. Otolaryngol. Head. Neck Surg. 1986, 94, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, S.; Fujishiro, N.; Sugiyama, K. Systemic lupus erythematosus with sensorineural hearing loss and improvement after plasmapheresis using the double filtration method. Intern. Med. 1992, 31, 778–781. [Google Scholar] [CrossRef] [PubMed]
- Chawki, S.; Aouizerate, J.; Trad, S.; Prinseau, J.; Hanslik, T. Bilateral sudden sensorineural hearing loss as a presenting feature of systemic lupus erythematosus: Case report and brief review of other published cases. Medicine 2016, 95, e4345. [Google Scholar] [CrossRef] [PubMed]
- Khalidi, N.A.; Rebello, R.; Robertson, D.D. Sensorineural hearing loss in systemic lupus erythematosus: Case report and literature review. J. Laryngol. Otol. 2008, 122, 1371–1376. [Google Scholar] [CrossRef] [PubMed]
- Bullington, M.; Davies, G.; MacDonald, C.B. Reversible Sensorineural Hearing Loss Resulting from Hypertrophic Pachymeningitis in Systemic Lupus Erythematosus: A Case Report. OTO Open 2019, 3, 2473974X19865526. [Google Scholar] [CrossRef] [PubMed]
- Kataoka, H.; Takeda, T.; Nakatani, H.; Saito, H. Sensorineural hearing loss of suspected autoimmune etiology: A report of three cases. Auris Nasus Larynx 1995, 22, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Girasoli, L.; Cazzador, D.; Padoan, R.; Nardello, E.; Felicetti, M.; Zanoletti, E.; Schiavon, F.; Bovo, R. Update on Vertigo in Autoimmune Disorders, from Diagnosis to Treatment. J. Immunol. Res. 2018, 2018, 5072582. [Google Scholar] [CrossRef] [PubMed]
- Dasgupta, S.; Dasgupta, S. Therapeutic Interventions of Tissue Specific Autoimmune Onset in Systemic Lupus Erythematosus. Mini Rev. Med. Chem. 2017, 17, 1418–1424. [Google Scholar] [CrossRef] [PubMed]
- Compadretti, G.C.; Brandolini, C.; Tasca, I. Sudden sensorineural hearing loss in lupus erythematosus associated with antiphospholipid syndrome: Case report and review. Ann. Otol. Rhinol. Laryngol. 2005, 114, 214–218. [Google Scholar] [CrossRef]
- Chen, J.J.; Tseng, P.T. The efficacy of a modified steroid treatment protocol in SLE-related audiovestibular dysfunction. Prospect Clinic for Otorhinolaryngology & Neurology, Kaohsiung City, Taiwan. 2024; manuscript in preparation. [Google Scholar]
- Alexander, T.H.; Weisman, M.H.; Derebery, J.M.; Espeland, M.A.; Gantz, B.J.; Gulya, A.J.; Hammerschlag, P.E.; Hannley, M.; Hughes, G.B.; Moscicki, R.; et al. Safety of high-dose corticosteroids for the treatment of autoimmune inner ear disease. Otol. Neurotol. 2009, 30, 443–448. [Google Scholar] [CrossRef]
- Chen, J.J.; Zeng, B.S.; Wu, C.N.; Stubbs, B.; Carvalho, A.F.; Brunoni, A.R.; Su, K.P.; Tu, Y.K.; Wu, Y.C.; Chen, T.Y.; et al. Association of Central Noninvasive Brain Stimulation Interventions With Efficacy and Safety in Tinnitus Management: A Meta-analysis. JAMA Otolaryngol. Head. Neck Surg. 2020, 146, 801–809. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.J.; Zeng, B.Y.; Lui, C.C.; Chen, T.Y.; Chen, Y.W.; Tseng, P.T. Pfizer-BioNTech COVID-19 vaccine associated tinnitus and treatment with transcranial magnetic stimulation. QJM 2022, 115, 623–624. [Google Scholar] [CrossRef] [PubMed]
- Frejo, L.; Lopez-Escamez, J.A. Cytokines and Inflammation in Meniere Disease. Clin. Exp. Otorhinolaryngol. 2022, 15, 49–59. [Google Scholar] [CrossRef] [PubMed]
- Poshattiwar, R.S.; Acharya, S.; Shukla, S.; Kumar, S. Neurological Manifestations of Connective Tissue Disorders. Cureus 2023, 15, e47108. [Google Scholar] [CrossRef]
- Crincoli, V.; Piancino, M.G.; Iannone, F.; Errede, M.; Di Comite, M. Temporomandibular Disorders and Oral Features in Systemic Lupus Erythematosus Patients: An Observational Study of Symptoms and Signs. Int. J. Med. Sci. 2020, 17, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Xie, S.; Ning, H.; She, Y.; Jing, Q.; Jiang, Q.; Zhang, Y.; Mei, L.; Feng, Y.; Wu, X. Effect of systemic lupus erythematosus and rheumatoid arthritis on sudden sensorineural hearing loss. Laryngoscope 2020, 130, 2475–2480. [Google Scholar] [CrossRef] [PubMed]
- Motoyama, R.; Higuchi, T.; Hirahara, S.; Konda, N.; Yamada, R.; Watanabe, K.; Fujisaki, M.; Yamaguchi, R.; Katsumata, Y.; Kawaguchi, Y.; et al. A case of systemic lupus erythematosus having concurrent Evans syndrome and acquired thrombotic thrombocytopenic purpura. Mod. Rheumatol. Case Rep. 2023, 7, 383–387. [Google Scholar] [CrossRef]
- Gazquez, I.; Soto-Varela, A.; Aran, I.; Santos, S.; Batuecas, A.; Trinidad, G.; Perez-Garrigues, H.; Gonzalez-Oller, C.; Acosta, L.; Lopez-Escamez, J.A. High prevalence of systemic autoimmune diseases in patients with Meniere’s disease. PLoS ONE 2011, 6, e26759. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, J.-J.; Hsu, C.-W.; Chen, Y.-W.; Chen, T.-Y.; Zeng, B.-S.; Tseng, P.-T. Audiovestibular Dysfunction in Systemic Lupus Erythematosus Patients: A Systematic Review. Diagnostics 2024, 14, 1670. https://doi.org/10.3390/diagnostics14151670
Chen J-J, Hsu C-W, Chen Y-W, Chen T-Y, Zeng B-S, Tseng P-T. Audiovestibular Dysfunction in Systemic Lupus Erythematosus Patients: A Systematic Review. Diagnostics. 2024; 14(15):1670. https://doi.org/10.3390/diagnostics14151670
Chicago/Turabian StyleChen, Jiann-Jy, Chih-Wei Hsu, Yen-Wen Chen, Tien-Yu Chen, Bing-Syuan Zeng, and Ping-Tao Tseng. 2024. "Audiovestibular Dysfunction in Systemic Lupus Erythematosus Patients: A Systematic Review" Diagnostics 14, no. 15: 1670. https://doi.org/10.3390/diagnostics14151670