
The Pivotal Role of Presepsin in Assessing Sepsis-Induced Cholestasis

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethical Issues
2.2. Study Population
2.3. Variables Assessment/Definition
2.4. Statistical Analysis
3. Results
3.1. Univariate Analysis
3.1.1. Comparisons between Patients with Increased and Normal Conjugated Bilirubin
3.1.2. Associations between Categorical and Numerical Parameters
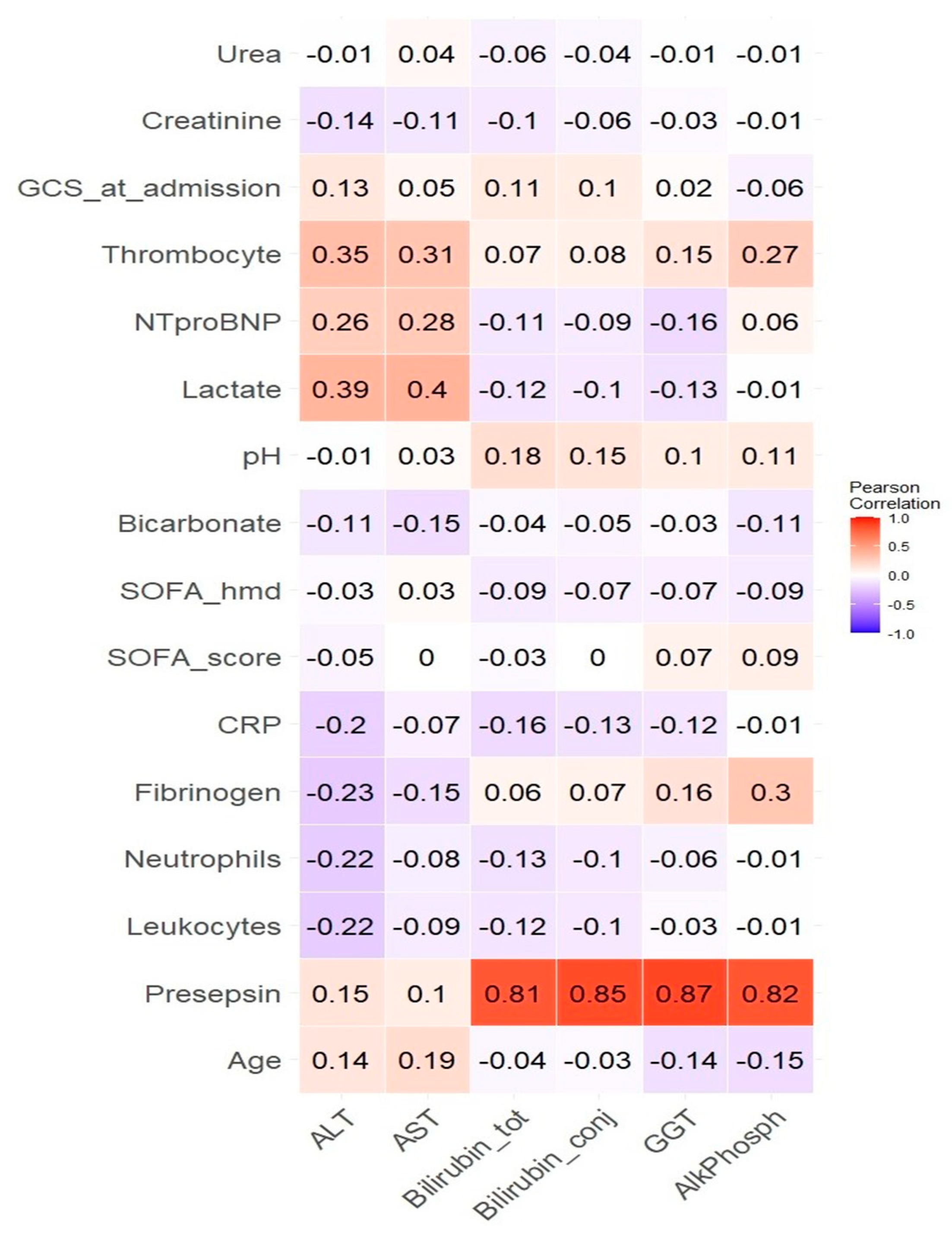
3.1.3. Correlations between Numerical Parameters
3.2. Multivariate Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Srzić, I.; Adam, V.N.; Pejak, D.T. Sepsis definition: What’s new in the treatment guidelines. Acta Clin. Croat. 2022, 61 (Suppl. S1), 67. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Deutschman, C.S.; Seymour, C.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Moustafa, R.; Albouni, T.; Aziz, G. The role of procalcitonin and presepsin in the septic febrile neutropenia in acute leukemia patients. PLoS ONE 2021, 16, e0253842. [Google Scholar] [CrossRef] [PubMed]
- Sharygin, D.; Koniaris, L.G.; Wells, C.; Zimmers, T.A.; Hamidi, T. Role of CD14 in human disease. Immunology 2023, 169, 260. [Google Scholar] [CrossRef]
- Naeim, F.; Rao, P.N.; Song, S.X.; Phan, R.T. Principles of Immunophenotyping. In Atlas of Hematopathology: Morphology, Immunophenotype, Cytogenetics, and Molecular Approaches, 2nd ed.; Academic Press: Cambridge, MA, USA, 2018; pp. 29–56. [Google Scholar]
- Roy, S.; Kothari, N.; Sharma, A.; Goyal, S.; Sankanagoudar, S.; Bhatia, P.K.; Sharma, P. Comparison of Diagnostic Accuracy of Presepsin and Procalcitonin for Sepsis in Critically Ill Patients: A Prospective Observational Study. Indian J. Crit. Care Med. 2023, 27, 289. [Google Scholar] [CrossRef]
- Zou, Q.; Wen, W.; Zhang, X.C. Presepsin as a novel sepsis biomarker. World J. Emerg. Med. 2014, 5, 16. [Google Scholar] [CrossRef]
- Liang, J.; Cai, Y.; Shao, Y. Comparison of presepsin and Mid-regional pro-adrenomedullin in the diagnosis of sepsis or septic shock: A systematic review and meta-analysis. BMC Infect. Dis. 2023, 23, 288. [Google Scholar] [CrossRef] [PubMed]
- Kyriazopoulou, E.; Leventogiannis, K.; Tavoulareas, G.; Mainas, E.; Toutouzas, K.; Mathas, C.; Prekates, A.; Sakka, V.; Panagopoulos, P.; Syrigos, K.; et al. Presepsin as a diagnostic and prognostic biomarker of severe bacterial infections and COVID-19. Sci. Rep. 2023, 13, 3814. [Google Scholar] [CrossRef]
- Paraskevas, T.; Chourpiliadi, C.; Demiri, S.; Micahilides, C.; Karanikolas, E.; Lagadinou, M.; Velissaris, D. Presepsin in the diagnosis of sepsis. Clin. Chim. Acta 2023, 550, 117588. [Google Scholar] [CrossRef]
- Wu, J.; Zhan, X.; Wang, S.; Liao, X.; Li, L.; Luo, J. The value of plasma presepsin as a diagnostic and prognostic biomarker for sepsis in Southern China. Inflamm. Res. 2023, 72, 1829–1837. [Google Scholar] [CrossRef]
- Zong, X.; Liu, Y.; Gu, L.; Chen, X.; Yang, C. Early diagnostic value of Presepsin in sepsis: A prospective study on a population with suspected sepsis in fever clinics. Chin. Crit. Care Med. 2024, 36, 340–344. [Google Scholar]
- Ha, E.Y.; Park, I.R.; Chung, S.M.; Roh, Y.N.; Park, C.H.; Kim, T.G.; Kim, W.; Moon, J.S. The Potential Role of Presepsin in Predicting Severe Infection in Patients with Diabetic Foot Ulcers. J. Clin. Med. 2024, 13, 2311. [Google Scholar] [CrossRef]
- Ren, E.; Xiao, H.; Wang, G.; Zhao, Y.; Yu, H.; Li, C. Value of procalcitonin and presepsin in the diagnosis and severity stratification of sepsis and septic shock. World J. Emerg. Med. 2024, 15, 135–138. [Google Scholar]
- Juneja, D.; Jain, N.; Singh, O.; Goel, A.; Arora, S. Comparison between presepsin, procalcitonin, and CRP as biomarkers to diagnose sepsis in critically ill patients. J. Anaesthesiol. Clin. Pharmacol. 2023, 39, 458–462. [Google Scholar] [PubMed]
- Xiao, H.; Zhang, H.; Wang, G.; Wang, Y.; Tan, Z.; Sun, X.; Zhou, J.; Duan, M.; Zhi, D.; Hang, C.; et al. Comparison among presepsin, procalcitonin, and c-reactive protein in predicting blood culture positivity and pathogen in sepsis patients. Shock 2024, 61, 387–394. [Google Scholar] [CrossRef] [PubMed]
- Ndomba, N.; Soldera, J. Management of sepsis in a cirrhotic patient admitted to the intensive care unit: A systematic literature review. World J. Hepatol. 2023, 15, 850–866. [Google Scholar] [PubMed]
- Piccioni, A.; Santoro, M.C.; de Cunzo, T.; Tullo, G.; Cicchinelli, S.; Saviano, A.; Valletta, F.; Pascale, M.M.; Candelli, M.; Covino, M.; et al. Presepsin as Early Marker of Sepsis in Emergency Department: A Narrative Review. Medicina 2021, 57, 770. [Google Scholar] [CrossRef] [PubMed]
- van Helmond, N.; Johnson, B.D.; Curry, T.B.; Cap, A.P.; Convertino, V.A.; Joyner, M.J. White blood cell concentrations during lower body negative pressure and blood loss in humans. Exp. Physiol. 2016, 101, 1265–1275. [Google Scholar] [CrossRef] [PubMed]
- Ruangsomboon, O.; Panjaikaew, P.; Monsomboon, A.; Chakorn, T.; Permpikul, C.; Limsuwat, C. Diagnostic and prognostic utility of presepsin for sepsis in very elderly patients in the emergency department. Clin. Chim. Acta 2020, 510, 723–732. [Google Scholar] [CrossRef]
- Yao, S.; Kaido, T.; Uozumi, R.; Hirata, M.; Iwamura, S.; Miyachi, Y.; Macshut, M.; Sharshar, M.; Yagi, S.; Uemoto, S. Diagnostic potential of presepsin in bacterial infection following hepato-biliary-pancreatic surgery: A prospective observational study. J. Hepato-Biliary-Pancreat. Sci. 2020, 27, 756–766. [Google Scholar] [CrossRef]
- Wei, S.; Shen, Z.; Yin, Y.; Cong, Z.; Zeng, Z.; Zhu, X. Advances of presepsin in sepsis-associated ARDS. Postgrad. Med. J. 2024, 100, 209–218. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Song, J.; Park, D.W.; Seok, H.; Ahn, S.; Kim, J.; Park, J.; Cho, H.-J.; Moon, S. Diagnostic and prognostic value of presepsin and procalcitonin in non-infectious organ failure, sepsis, and septic shock: A prospective observational study according to the Sepsis-3 definitions. BMC Infect. Dis. 2022, 22, 8. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Feng, Y.; Liang, X.; Gui, S.; Ren, D.; Liu, Y.; She, J.; Zhang, X.; Song, F.; Yu, L.; et al. Elevations in presepsin, P.C.T.; hs-CRP; IL-6 levels predict mortality among septic patients in, ICU. J. Leukoc. Biol. 2024, qiae121. [Google Scholar] [CrossRef] [PubMed]
- Lee, G.B.; Lee, J.W.; Yoon, S.H.; Hwang, W.M.; Yun, S.R.; Koh, D.H.; Park, Y. Plasma presepsin for mortality prediction in patients with sepsis-associated acute kidney injury requiring continuous kidney replacement therapy. Kidney Res. Clin. Pract. 2024, 43, 457. [Google Scholar] [CrossRef] [PubMed]
- Aliu-Bejta, A.; Kurshumliu, M.; Namani, S.; Dreshaj, S.; Baršić, B. Ability of presepsin concentrations to predict mortality in adult patients with sepsis. J. Clin. Transl. Sci. 2023, 7, e121. [Google Scholar] [CrossRef]
- Narendra, S.; Wyawahare, M.; Adole, P.S. Presepsin vs Procalcitonin as Predictors of Sepsis Outcome. J. Assoc. Physicians India 2022, 70, 38–40. [Google Scholar] [CrossRef]
- Pollock, G.; Minuk, G.Y. Diagnostic considerations for cholestatic liver disease. J. Gastroenterol. Hepatol. 2017, 32, 1303–1309. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, S.; De Tymowski, C.; Stern, J.; Bouzid, D.; Zappella, N.; Snauwaert, A.; Robert, T.; Lortat-Jacob, B.; Tran-Dinh, A.; Augustin, P.; et al. Relationship between liver dysfunction, lipoprotein concentration and mortality during sepsis. PLoS ONE 2022, 17, e0272352. [Google Scholar] [CrossRef] [PubMed]
- Fan HBin Yang, D.L.; Chen, A.S.; Li, Z.; Xu, L.T.; Ma, X.J.; Zhou, H.; Tian, Z.-F.; Wu, J.-J.; Yan, F.-M.; Yang, D.-L.; et al. Sepsis-associated cholestasis in adult patients: A prospective study. Am. J. Med. Sci. 2013, 346, 462–466. [Google Scholar]
- Gramignoli, R.; Ranade, A.R.; Venkataramanan, R.; Strom, S.C. Effects of Pro-Inflammatory Cytokines on Hepatic Metabolism in Primary Human Hepatocytes. Int. J. Mol. Sci. 2022, 23, 14880. [Google Scholar] [CrossRef]
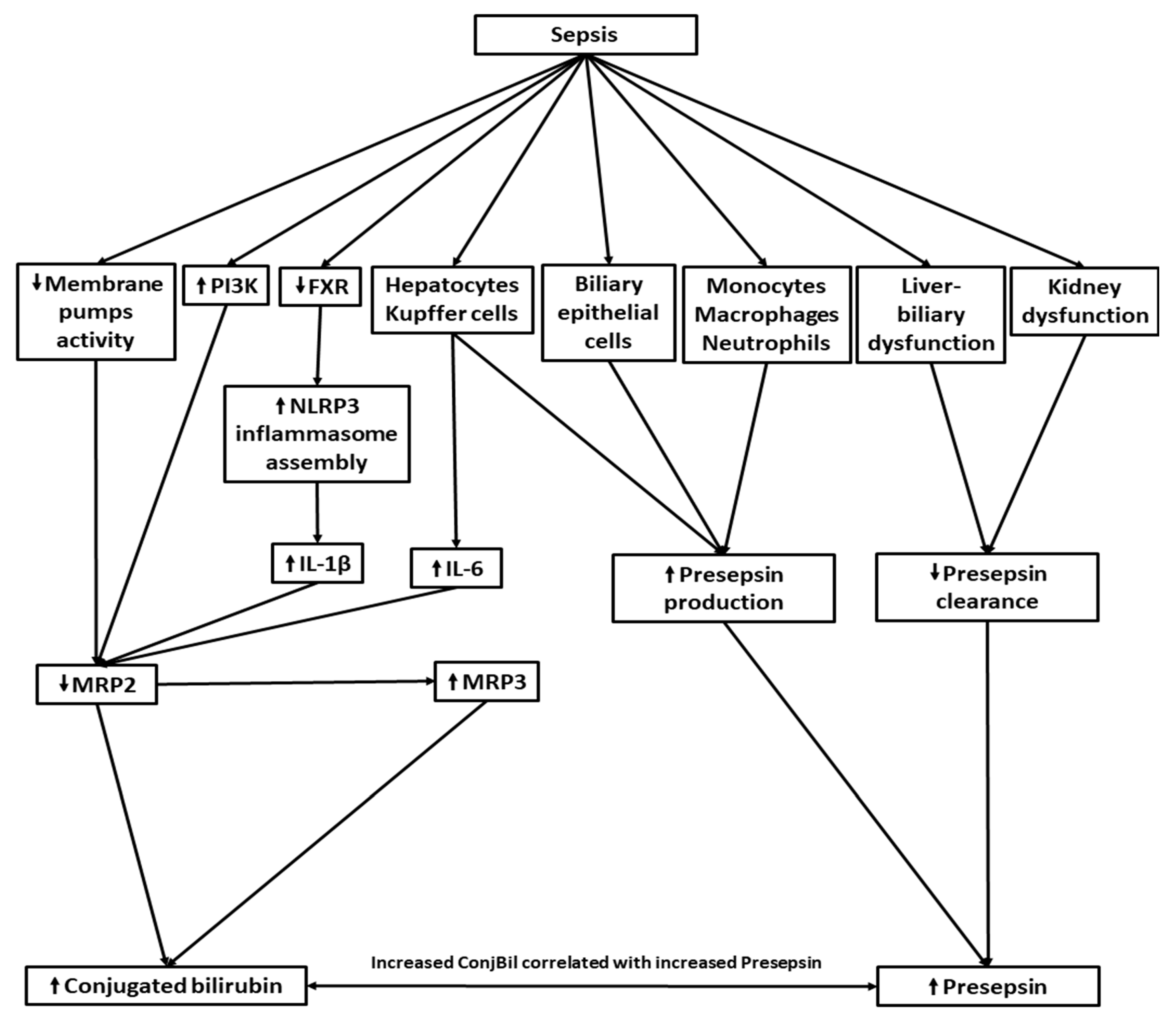
- Ghenu, M.I.; Dragoş, D.; Manea, M.M.; Ionescu, D.; Negreanu, L. Pathophysiology of sepsis-induced cholestasis: A review. JGH Open 2022, 6, 378–387. [Google Scholar] [CrossRef] [PubMed]
- Wauters, J.; Mesotten, D.; Van Zwam, K.; Van Pelt, J.; Thiessen, S.; Dieudonné, A.S.; Borght, S.V.; Berghe, G.V.D.; Wilmer, A. The impact of resuscitated fecal peritonitis on the expression of the hepatic bile salt transporters in a porcine model. Shock 2010, 34, 508–516. [Google Scholar] [CrossRef] [PubMed]
- Azad, A.K.; Raihan, T.; Ahmed, J.; Hakim, A.; Emon, T.H.; Chowdhury, P.A. Human Aquaporins: Functional Diversity and Potential Roles in Infectious and Non-infectious Diseases. Front. Genet. 2021, 12, 654865. [Google Scholar] [CrossRef] [PubMed]
- Hao, H.; Cao, L.; Jiang, C.; Che, Y.; Zhang, S.; Takahashi, S.; Wang, G.; Gonzalez, F.J. Farnesoid X Receptor Regulation of the NLRP3 Inflammasome Underlies Cholestasis-Associated Sepsis. Cell Metab. 2017, 25, 856. [Google Scholar] [CrossRef] [PubMed]
- Ye, X.; Zhang, T.; Han, H. PPARα: A potential therapeutic target of cholestasis. Front. Pharmacol. 2022, 13, 916866. [Google Scholar] [CrossRef] [PubMed]
- Beer, A.J.; Hertz, D.; Seemann, E.; Beretta, M.; Westermann, M.; Bauer, R.; Bauer, M.; Kessels, M.M.; Qualmann, B. Reduced Mrp2 surface availability as PI3Kγ-mediated hepatocytic dysfunction reflecting a hallmark of cholestasis in sepsis. Sci. Rep. 2020, 10, 13110. [Google Scholar] [CrossRef] [PubMed]
- Recknagel, P.; Gonnert, F.A.; Westermann, M.; Lambeck, S.; Lupp, A.; Rudiger, A.; Dyson, A.; Carré, J.E.; Kortgen, A.; Krafft, C.; et al. Liver dysfunction and phosphatidylinositol-3-kinase signalling in early sepsis: Experimental studies in rodent models of peritonitis. PLoS Med. 2012, 9, e1001338. [Google Scholar] [CrossRef] [PubMed]
- Thon, P.; Rump, K.; Knorr, A.; Dyck, B.; Ziehe, D.; Unterberg, M.; Nowak, H.; Bergmann, L.; Wolf, A.; Bazzi, M.; et al. The Distinctive Activation of Toll-Like Receptor 4 in Human Samples with Sepsis. Cells 2022, 11, 3020. [Google Scholar] [CrossRef]
- Franca, A.; Carlos Melo Lima Filho, A.; Guerra, M.T.; Weerachayaphorn, J.; Loiola dos Santos, M.; Njei, B.; Nathanson, M.H. Effects of endotoxin on type 3 inositol 1,4,5-trisphosphate receptor in human cholangiocytes. Hepatology 2019, 69, 817. [Google Scholar] [CrossRef]
- Tsuchida, T.; Ie, K.; Okuse, C.; Hirose, M.; Nishisako, H.; Torikai, K.; Tanaka, T.; Kunishima, H.; Matsuda, T. Determining the factors affecting serum presepsin level and its diagnostic utility: A cross-sectional study. J. Infect. Chemother. 2021, 27, 585–591. [Google Scholar] [CrossRef]
- Yamaguchi, T.; Ohira, M.; Kawagoe, N.; Nakamura, S.; Tanaka, S.; Oka, R.; Watanabe, Y.; Sato, Y.; Nagayama, D.; Saiki, A.; et al. High presepsin concentrations in bile and its marked elevation in biliary tract diseases: A retrospective analysis. Clin. Chim. Acta 2021, 521, 278–284. [Google Scholar] [CrossRef]
- CDC; Ncezid’s Division of Healthcare Quality Promotion. Pneumonia (Ventilator-Associated [VAP] and Non-Ventilator-Associated Pneumonia [PNEU]) Event. 2024. Available online: https://www.cdc.gov/nhsn/pdfs/pscmanual/6pscvapcurrent.pdf (accessed on 5 March 2024).
- Morais, V.; Texeira, E.; Suárez, N. Respiratory Tract Infections: Bacteria. Encycl. Infect. Immun. 2022, 3, 1–12. [Google Scholar]
- Bono, M.J.; Leslie, S.W.; Reygaert, W.C. Urinary Tract Infection; StatPearls Publishing: Treasure Island, FL, USA, 2022; pp. 10–13. Available online: https://www.ncbi.nlm.nih.gov/books/NBK470195/ (accessed on 25 April 2023).
- CDC; Ncezid’s Division of Healthcare Quality Promotion. CDC/NHSN Surveillance Definitions for Specific Types of Infections. 2023. Available online: https://stacks.cdc.gov/view/cdc/127235 (accessed on 5 May 2023).
- Garlicki, A.M.; Jawień, M.; Pancewicz, S.; Moniuszko-Malinowska, A.; Kalinowska-Nowak, A.; Bociąga-Jasik, M. Management of bacterial skin and soft tissue infections. Epidemiol. Rev. 2020, 74, 89–107. [Google Scholar] [CrossRef] [PubMed]
- Rüddel, H.; Thomas-Rüddel, D.O.; Reinhart, K.; Bach, F.; Gerlach, H.; Lindner, M.; Marshall, J.C.; Simon, P.; Weiss, M.; Bloos, F.; et al. Adverse effects of delayed antimicrobial treatment and surgical source control in adults with sepsis: Results of a planned secondary analysis of a cluster-randomized controlled trial. Crit. Care 2022, 26, 51. [Google Scholar] [CrossRef]
- Nardulli, P.; Hall, G.G.; Quarta, A.; Fruscio, G.; Laforgia, M.; Garrisi, V.M.; Ruggiero, R.; Scacco, S.; De Vito, D. Antibiotic Abuse and Antimicrobial Resistance in Hospital Environment: A Retrospective Observational Comparative Study. Medicina 2022, 58, 1257. [Google Scholar] [CrossRef]
- Hasjim, B.J.; Grigorian, A.; Stopenski, S.; Swentek, L.; Sun, B.; Livingston, J.K.; Williams, B.; Nastanski, F.; Nahmias, J. Moderate to severe leukocytosis with vasopressor use is associated with increased mortality in trauma patients. J. Intensive Care Soc. 2022, 23, 117. [Google Scholar] [CrossRef] [PubMed]
- Szasz, J.; Noitz, M.; Dünser, M. Diagnosing acute organ ischemia: A practical guide for the emergency and intensive care physician. Med. Klin. Intensivmed. Notfmed. 2020, 115, 159–172. [Google Scholar] [CrossRef] [PubMed]
- Soleimanpour, H.; Safari, S.; Rahmani, F.; Nejabatian, A.; Alavian, S.M. Hepatic Shock Differential Diagnosis and Risk Factors: A Review Article. Hepat. Mon. 2015, 15, 6. [Google Scholar] [CrossRef] [PubMed]
- Tang, L.; Cai, N.; Zhou, Y.; Liu, Y.; Hu, J.; Li, Y.; Yi, S.; Song, W.; Kang, L.; He, H. Acute stress induces an inflammation dominated by innate immunity represented by neutrophils in mice. Front. Immunol. 2022, 13, 1014296. [Google Scholar] [CrossRef]
- Rando, E.; Matteini, E.; Guerriero, S.; Fantoni, M. Gram-negative infections in frail patients. Infez. Med. 2022, 31, 31. [Google Scholar]
- De Ávila, D.X.; de Andrade, T.G.; Mocarzel, L.O.C.; Gismondi, R.A.O.C.; Cabrita, C.M.; Mesquita, E.T.; Villacorta, H. Liver stiffness as measured by transient elastography is a predictor of outcomes in patients with chronic heart failure with reduced, mid-range, and recovered left-ventricular ejection fraction. Am. Heart Hournal Plus Cardiol. Res. Pract. 2021, 11, 100048. [Google Scholar] [CrossRef] [PubMed]
- Alvarez, A.M.; Mukherjee, D. Liver Abnormalities in Cardiac Diseases and Heart Failure. Int. J. Angiol. 2011, 20, 135. [Google Scholar] [CrossRef] [PubMed]
- Reina-Couto, M.; Pereira-Terra, P.; Quelhas-Santos, J.; Silva-Pereira, C.; Albino-Teixeira, A.; Sousa, T. Inflammation in Human Heart Failure: Major Mediators and Therapeutic Targets. Front. Physiol. 2021, 12, 746494. [Google Scholar] [CrossRef] [PubMed]
- Niehues, T. C-reactive protein and other biomarkers—The sense and non-sense of using inflammation biomarkers for the diagnosis of severe bacterial infection. LymphoSign J. 2018, 5, 35–47. [Google Scholar] [CrossRef]
- Mozes, B.; Milatiner, D.; Block, C.; Blumstein, Z.; Halkin, H. Inconsistency of a model aimed at predicting bacteremia in hospitalized patients. J. Clin. Epidemiol. 1993, 46, 1035–1040. [Google Scholar] [CrossRef] [PubMed]
- Gille-Johnson, P.; Hansson, K.E.; Gårdlund, B. Clinical and laboratory variables identifying bacterial infection and bacteraemia in the emergency department. Scand. J. Infect. Dis. 2012, 44, 745–752. [Google Scholar] [CrossRef] [PubMed]
- Kanai, S.; Honda, T.; Uehara, T.; Matsumoto, T. Liver function tests in patients with bacteremia. J. Clin. Lab. Anal. 2008, 22, 66–69. [Google Scholar] [CrossRef] [PubMed]
- Cheung, B.M.Y.; Ong, K.L.; Cheung, R.V.; Wong, L.Y.F.; Wat, N.M.S.; Tam, S.; Leung, G.M.; Cheng, C.H.; Woo, J.; Janus, E.D.; et al. Association between plasma alkaline phosphatase and C-reactive protein in Hong Kong Chinese. Clin. Chem. Lab. Med. 2008, 46, 523–527. [Google Scholar] [CrossRef] [PubMed]
- Hozumi, H.; Tada, R.; Murakami, T.; Adachi, Y.; Ohno, N. Comparative Analysis of Hepatic CD14 Expression between Two Different Endotoxin Shock Model Mice: Relation between Hepatic Injury and CD14 Expression. PLoS ONE 2013, 8, e53692. [Google Scholar] [CrossRef]
- Chou, M.H.; Chuang, J.H.; Eng, H.L.; Tsai, P.C.; Hsieh, C.S.; Liu, H.C.; Wang, C.-H.; Lin, C.-Y.; Lin, T.-M. Effects of Hepatocyte CD14 Upregulation during Cholestasis on Endotoxin Sensitivity. PLoS ONE 2012, 7, e34903. [Google Scholar] [CrossRef]
- Chou, M.H.; Chuang, J.H.; Eng, H.L.; Chen, C.M.; Wang, C.H.; Chen, C.L.; Lin, T.-M. Endotoxin and CD14 in the progression of biliary atresia. J. Transl. Med. 2010, 8, 138. [Google Scholar] [CrossRef] [PubMed]
- Bas, S.; Gauthier, B.R.; Spenato, U.; Stingelin, S.; Gabay, C. CD14 Is an Acute-Phase Protein. J. Immunol. 2004, 172, 4470–4479. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Numerical Parameter | Median (IQR) for Patients with Increased ConjBil | Median (IQR) for Patients with Normal ConjBil | W Statistics | p-Value |
|---|---|---|---|---|
| Age (years) | 73 (65–82.5) | 73 (64–82) | 17,555 | 0.6 |
| Presepsin (pg/mL) | 1340 (618.5–3220.5) | 789 (318–1700) | 12,633.5 | 6 × 10−7 |
| Leukocytes (μL) | 16,120 (9995–21,740) | 14,660 (10,620–21,200) | 17,389.5 | 0.5 |
| Neutrophils (μL) | 12,665 (7695–18,654.5) | 12,009.5 (8057.5–18,132.25) | 17,299.5 | 0.5 |
| Fibrinogen (mg/dL) | 495.5 (383–757) | 482 (385–660) | 15,899.5 | 0.2 |
| C reactive protein (mg/dL) | 16.05 (8.25–27.75) | 9.4 (3.7–20.8) | 3612.5 | 0.006 |
| SOFA_score | 5 (2–8) | 4 (2–6) | 14,210 | 4 × 10−4 |
| SOFA_hmd | 0 (0–2) | 0 (0–0) | 15,112 | 4 × 10−4 |
| Bicarbonate (mEq/L) | 19 (15.9–21.4) | 20.5 (15.175–24.5) | 17,459.5 | 0.02 |
| pH | 7.42 (7.3–7.48) | 7.37 (7.28–7.45) | 12,653 | 0.008 |
| Lactate (mmol/L) | 2.18 (1.215–4.005) | 1.27 (0.8–2.23) | 6794.5 | 5 × 10−5 |
| NTproBNP (pg/mL) | 226 (223–325) | 4710 (1641.5–15,948) | 450.5 | 0.05 |
| Thrombocyte count (× 103/μL) | 225 (167–310) | 261 (195–351) | 21,040 | 0.007 |
| GCS_at_admission | 15 (10–15) | 15 (11–15) | 19,428 | 0.2 |
| Creatinine (mg/dL) | 2.1 (1.065–3.725) | 1.62 (0.94–4.18) | 17,063 | 0.3 |
| Urea (mg/dL) | 92 (54–155) | 69 (42–155) | 16,050 | 0.06 |
| ALT (U/L) | 41 (25–78.5) | 28 (17–45) | 12,695 | 8 × 10−7 |
| AST (U/L) | 49 (28–102) | 28 (20–43) | 11,134 | 2 × 10−10 |
| GGT (U/L) | 51 (32.5–126) | 41 (24.55–76.5) | 6143.5 | 0.02 |
| AlkPh (U/L) | 101.5 (76–147.25) | 83 (66–119) | 5397 | 0.004 |
| Categorical Parameter | a/b/c/d | Odds Ratio (95% CI) | p-Value |
|---|---|---|---|
| Pulmonary infection | 197/56/110/33 | 1.06 (0.62 to 1.77) | 0.9 |
| Urinary infection | 201/52/105/38 | 1.4 (0.84 to 2.32) | 0.17 |
| Cutaneous infection | 248/5/133/10 | 3.72 (1.13 to 14.16) | 0.024 |
| Digestive infection | 247/6/141/2 | 0.58 (0.06 to 3.33) | 0.72 |
| Gallbladder stones | 230/23/130/13 | 1 (0.45 to 2.14) | 1 |
| Male gender | 154/99/60/83 | 2.15 (1.39 to 3.34) | 0.00035 |
| Deceased | 163/90/82/61 | 1.35 (0.87 to 2.09) | 0.2 |
| Numerical Parameter | Categorical Parameter | #Pts | Median (IQR) | #Pts | Median (IQR) | W Statistics | p-Value |
|---|---|---|---|---|---|---|---|
| Deceased | Survivors | ||||||
| AlkPh | Survival | 151 | 106 (78–131) | 245 | 85 (66–120.25) | 4751 | 0.01 |
| AST | Survival | 151 | 37 (24–68.5) | 245 | 30 (20–52) | 15,880.5 | 0.02 |
| ConjBil | Survival | 151 | 0.26 (0.2–0.515) | 245 | 0.24 (0.16–0.39) | 15,377.5 | 0.005 |
| Male gender | Female gender | ||||||
| ConjBil | Gender | 182 | 0.28 (0.19–0.5) | 214 | 0.22 (0.16–0.36) | 15,948.5 | 0.002 |
| TotBil | Gender | 182 | 0.66 (0.49–1.1275) | 214 | 0.575 (0.44–0.96) | 17,239.5 | 0.05 |
| Cutaneous infection_yes | Cutaneous infection_no | ||||||
| ConjBil | Cutaneous infection | 15 | 0.59 (0.265–1.775) | 381 | 0.25 (0.17–0.41) | 1383 | 0.0007 |
| TotBil | Cutaneous infection | 15 | 0.91 (0.605–2.445) | 381 | 0.62 (0.45–1.02) | 1546 | 0.003 |
| Urinary infection_yes | Urinary infection_no | ||||||
| ConjBil | Urinary infection | 90 | 0.28 (0.2–0.465) | 306 | 0.24 (0.16–0.41) | 11,740 | 0.03 |
| TotBil | Urinary infection | 90 | 0.73 (0.523–1.078) | 306 | 0.605 (0.44–1.015) | 11,508.5 | 0.02 |
| ALT | AST | TotBil | ConjBil | GGT | AlkPh | |
|---|---|---|---|---|---|---|
| Age | 0.00014 | 0.049 | ||||
| Bicarbonate | 0.00082 | 0.0031 | 0.0042 | |||
| Creatinine | 0.00035 | 0.048 | 0.0033 | |||
| CRP | 0.05 | 0.028 | 0.0015 | 0.027 | ||
| Fibrinogen | 0.04 | |||||
| GCS_at_admission | 0.00043 | |||||
| Lactate | 0.0085 | 4.3 × 10−7 | 0.00041 | 0.00017 | 0.0084 | |
| Leukocytes | 0.012 | |||||
| Neutrophils | 0.003 | |||||
| NTproBNP | 0.013 | |||||
| pH | 0.00018 | 0.0059 | ||||
| Presepsin | 7.7 × 10−6 | 3.9 × 10−12 | 0.00014 | 3 × 10−11 | 2.7 × 10−8 | 1.7 × 10−11 |
| SOFA_hmd | 0.0064 | 0.0055 | 9.3 × 10−6 | 0.0027 | ||
| SOFA_score | 0.0025 | 2.3 × 10−8 | 0.0022 | 2.2 × 10−5 | 0.0036 | |
| Thrombocyte count | 9.6 × 10−6 | 0.011 | ||||
| Urea | 0.042 | 3.5 × 10−5 | 0.00035 | 0.0025 |
| Dependent Variable | Independent Variable | Estimate | 95% Confidence Interval | t-Statistic | p-Value |
|---|---|---|---|---|---|
| AlkPh | Presepsin | 0.019 | (0.012, 0.024) | 5.649 | 7 × 10−8 |
| AlkPh | Creatinine | −7.58 | (−12.98, −2.18) | −2.752 | 0.007 |
| AlkPh | CRP | 1.34 | (0.2, 2.48) | 2.300 | 0.02 |
| ALT | Lactate | 8.97 | (4.65, 13.28) | 4.074 | 6 × 10−5 |
| ALT | Presepsin | 0.0095 | (0.0048, 0.014) | 3.957 | 1 × 10−4 |
| AST | Lactate | 13.6 | (6.26, 20.93) | 3.631 | 0.0003 |
| AST | Presepsin | 0.013 | (0.0055, 0.021) | 3.331 | 0.001 |
| AST | SOFA_hmd | 26.95 | (6.28, 47.61) | 2.555 | 0.01 |
| ConjBil | Presepsin | 0.00011 | (0.000080, 0.00013) | 8.185 | 4 × 10−15 |
| ConjBil | Creatinine | −0.077 | (−0.11, −0.044) | −4.665 | 4 × 10−6 |
| ConjBil | Urea | 0.0014 | (0.00040, 0.0024) | 2.767 | 0.006 |
| ConjBil | Thrombocyte count | 0.00043 | (−0.00082, −0.000032) | −2.117 | 0.035 |
| GGT | Presepsin | 0.019 | (0.013, 0.024) | 6.480 | 5 × 10−10 |
| GGT | Age | −1.76 | (−2.90, −0.61) | −3.004 | 0.003 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghenu, M.I.; Dragoș, D.; Manea, M.M.; Balcangiu-Stroescu, A.-E.; Ionescu, D.; Negreanu, L.; Vlad, A. The Pivotal Role of Presepsin in Assessing Sepsis-Induced Cholestasis. Diagnostics 2024, 14, 1706. https://doi.org/10.3390/diagnostics14161706
Ghenu MI, Dragoș D, Manea MM, Balcangiu-Stroescu A-E, Ionescu D, Negreanu L, Vlad A. The Pivotal Role of Presepsin in Assessing Sepsis-Induced Cholestasis. Diagnostics. 2024; 14(16):1706. https://doi.org/10.3390/diagnostics14161706
Chicago/Turabian StyleGhenu, Maria Iuliana, Dorin Dragoș, Maria Mirabela Manea, Andra-Elena Balcangiu-Stroescu, Dorin Ionescu, Lucian Negreanu, and Adelina Vlad. 2024. "The Pivotal Role of Presepsin in Assessing Sepsis-Induced Cholestasis" Diagnostics 14, no. 16: 1706. https://doi.org/10.3390/diagnostics14161706
APA StyleGhenu, M. I., Dragoș, D., Manea, M. M., Balcangiu-Stroescu, A. -E., Ionescu, D., Negreanu, L., & Vlad, A. (2024). The Pivotal Role of Presepsin in Assessing Sepsis-Induced Cholestasis. Diagnostics, 14(16), 1706. https://doi.org/10.3390/diagnostics14161706