


Best Practices for the Use of High-Frequency Ultrasound to Guide Aesthetic Filler Injections—Part 1: Upper Third of the Face



Abstract
1. Introduction
2. Materials and Methods
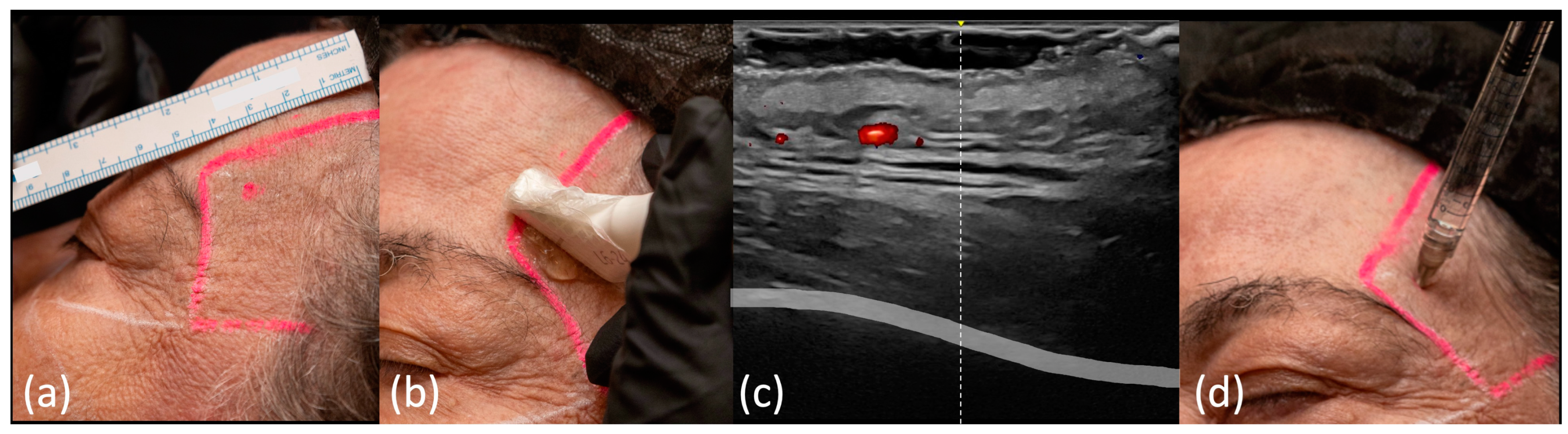
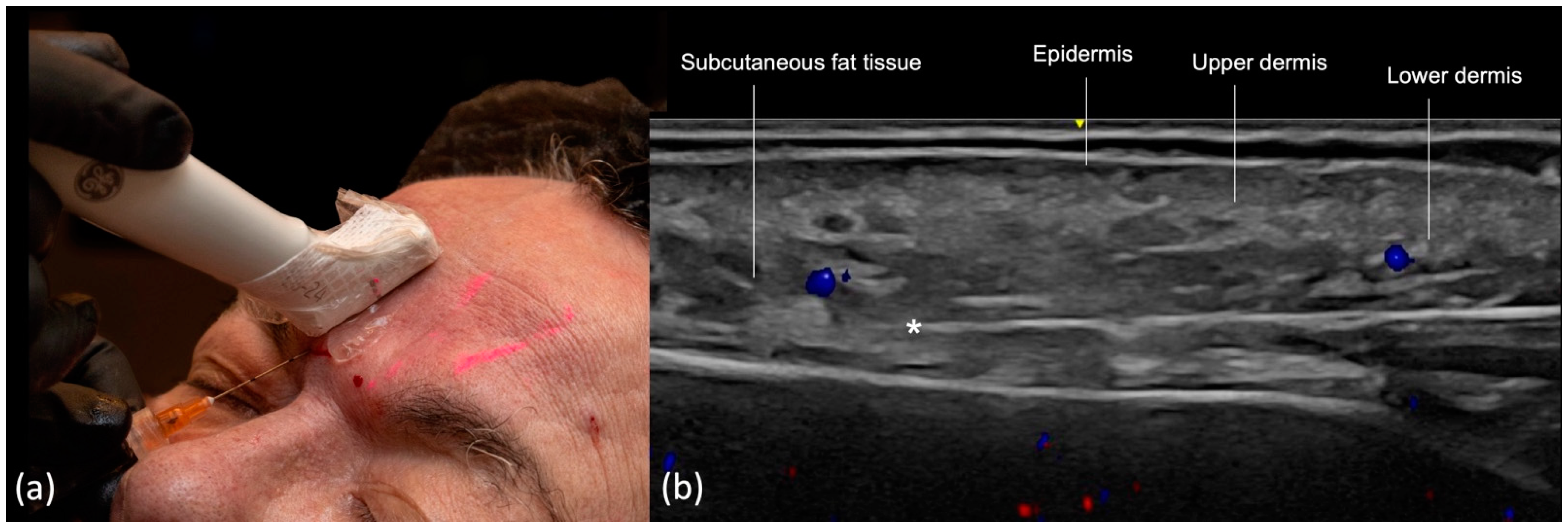
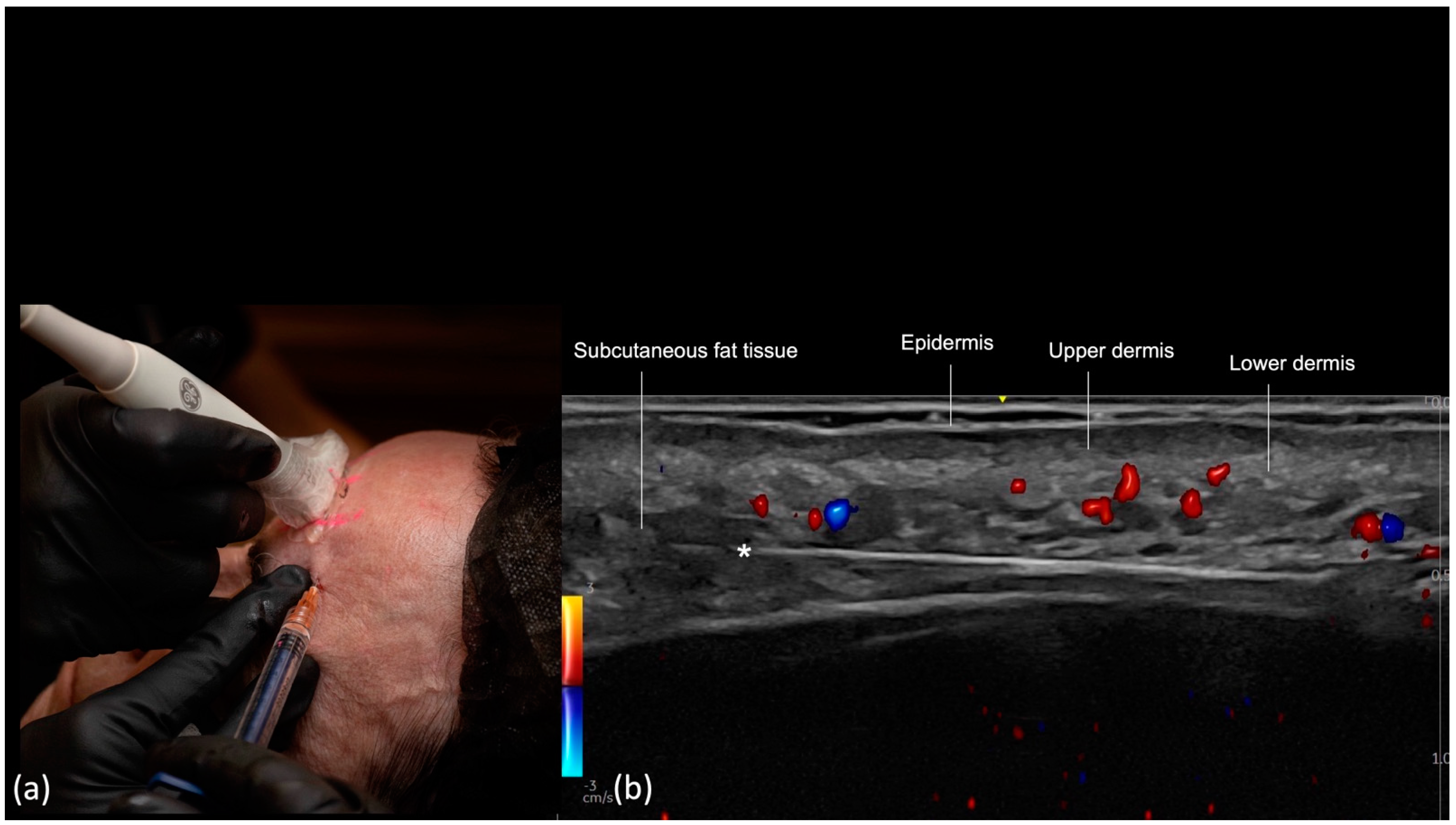
- Scan before injecting: The treatment area is scanned immediately before injection to assess the presence of vessels. The trajectory of the main arteries might be marked on the patient’s skin.
- Scan while injecting: In this case, the cannula is visualized in real time and positioned in the desired anatomical region, avoiding vascular structures.
3. Results
3.1. Temporal Region
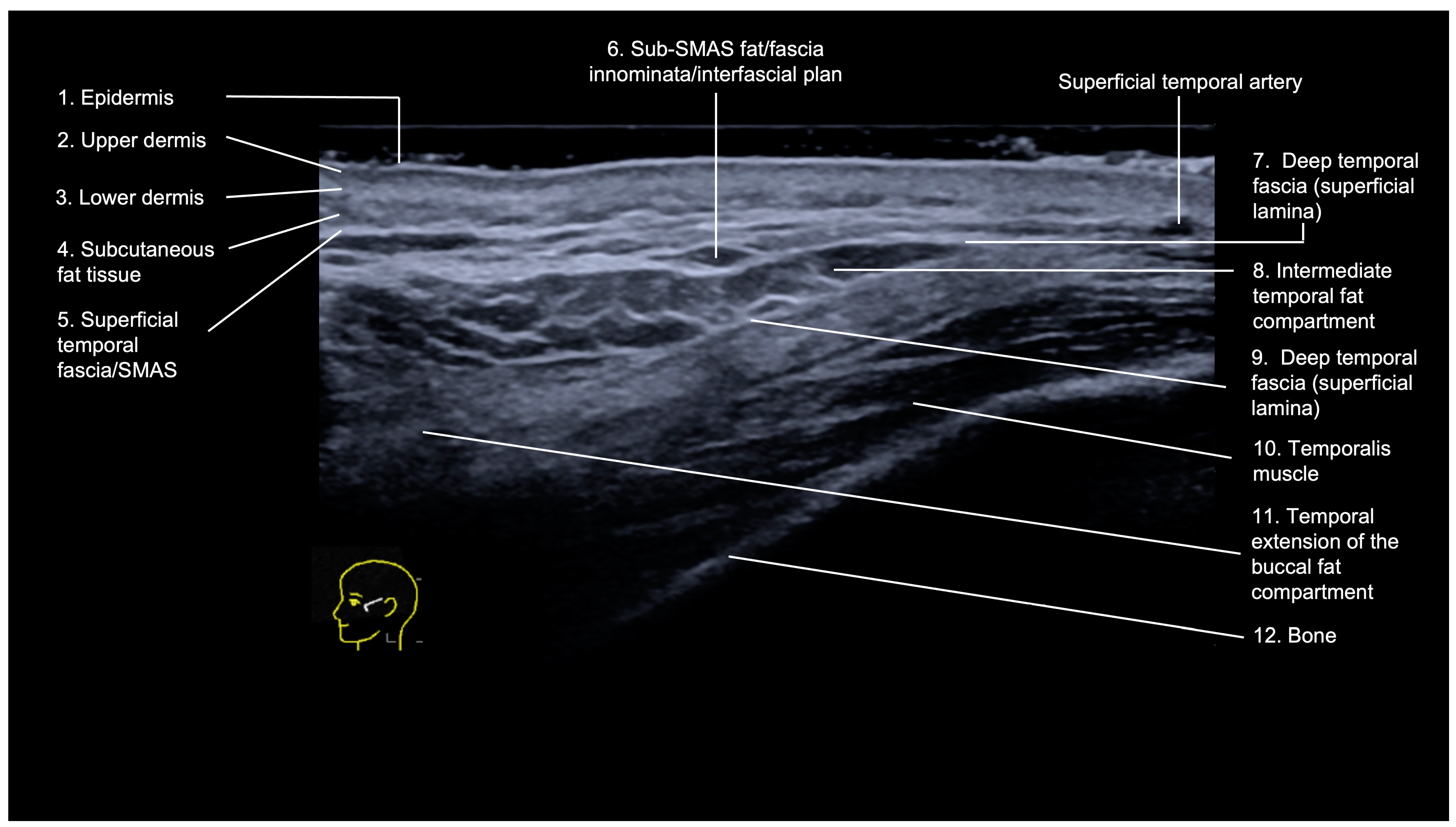
3.1.1. Sonographic Anatomy
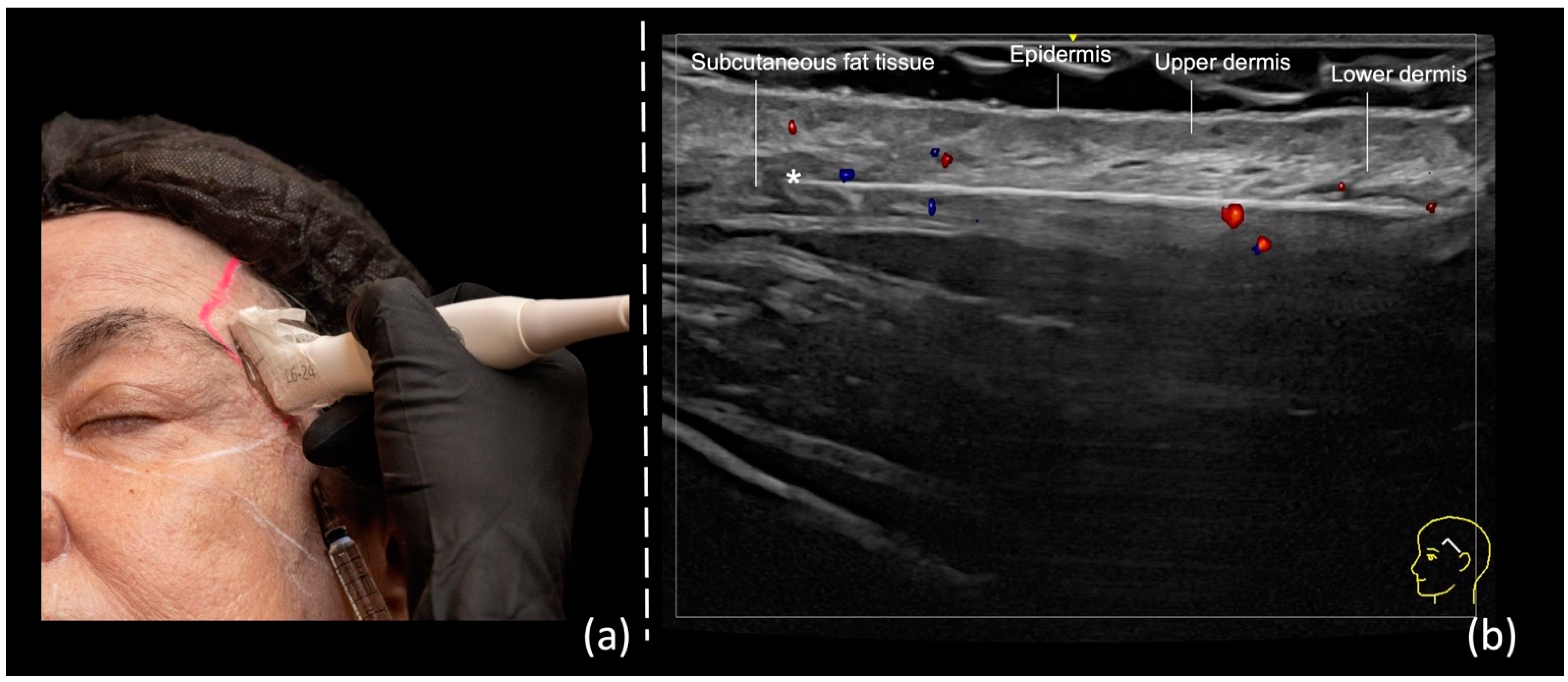
- Epidermis: hyperechoic line.
- Upper dermis: hypoechoic homogeneous layer.
- Lower dermis: usually more echogenic layer than the upper dermis.
- Subcutaneous fat tissue: a hypoechoic layer composed of fat lobules and hyperechoic septae.
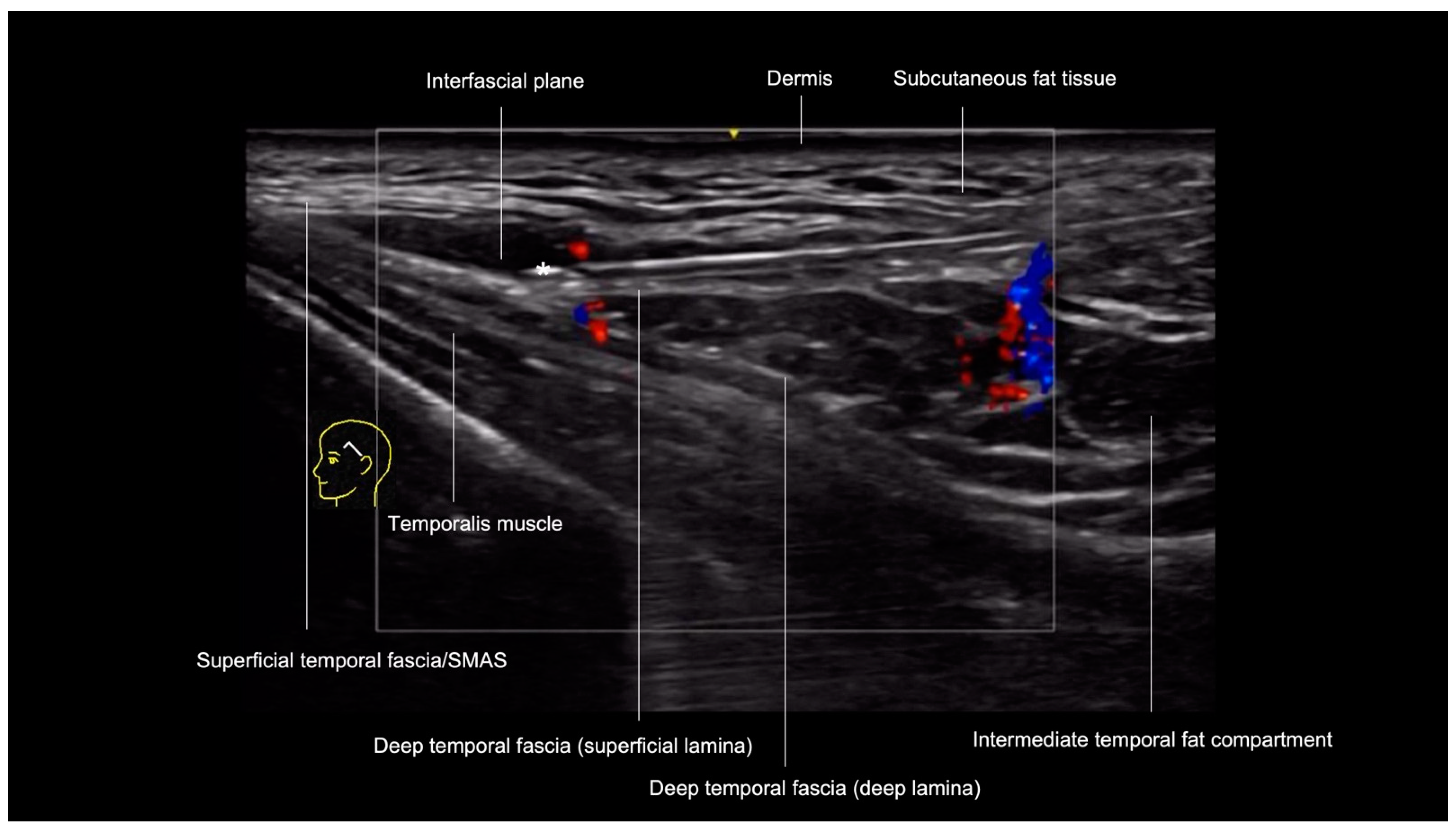
- Superficial temporal fascia/Superficial musculoaponeurotic system (SMAS): linear hyperechoic layers enveloping the superficial temporal artery and vein.
- Sub-SMAS fat: also called innominate fascia, it is a hypoechoic layer composed of loose connective tissue and fat lobules. This is the interfascial plane.
- Superficial lamina of the deep temporal fascia: a hyperechoic line, which is juxtaposed to the intermediate temporal fat compartment.
- Intermediate fat compartment (loose areolar tissue): a hypoechoic triangular layer composed of fat lobules and hyperechoic septae. The middle temporal vein can be encountered in this layer.
- Deep lamina of the deep temporal fascia: a hyperechoic line, which is deep to the intermediate temporal fat compartment.
- Temporal muscle: a large hypoechoic structure above the bone, where the anterior and posterior deep temporal arteries are located.
- Temporal extension of the buccal fat compartment: a hypoechoic fat compartment adjacent to the lateral orbital rim, connected to the buccal fat pat. Easily recognized when patient is asked to open and close the mouth, this fat pad can be found under the deep lamina of the deep temporal fascia.
- Bone: a thin hyperechoic line with acoustic shadowing.
3.1.2. Ultrasound-Guided Filling Techniques of the Temporal Region
- Technique 1: Subdermal filler placement
- Technique 2: Interfascial filler placement
- Technique 3: Supraperiosteal filler placement
3.2. Frontal Region (Glabella, Forehead, and Supraorbital Region)
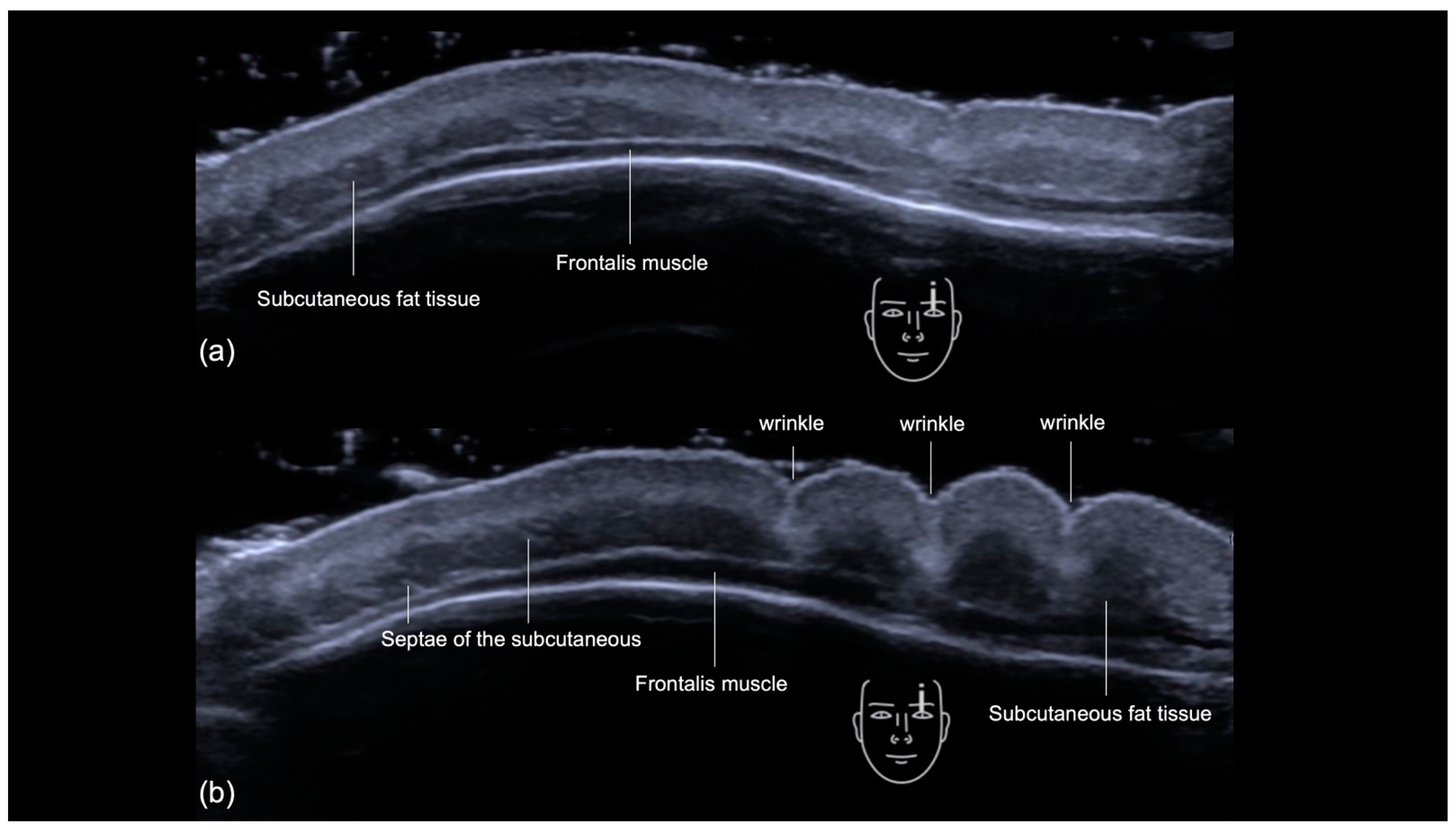
3.2.1. Sonographic Anatomy
- Epidermis: a hyperechoic line.
- Upper dermis: a hypoechoic homogeneous layer.
- Lower dermis: a hyperechoic layer.
- Subcutaneous fat tissue: a hypoechoic layer composed of fat lobules and hyperechoic septae.
- Suprafrontalis fascia: a thin hyperechoic upper layer of galea aponeurotica.
- Frontalis muscle: a hypoechoic band-like structure.
- Retro-Orbicularis Oculi Fat compartment (ROOF): a hyperechoic fibrous fat layer that separates the frontalis muscle from the bone. It can be appreciated in the inferolateral part of the forehead.
- Periosteum and subfrontalis fascia: a hyperechoic line showing combined imaging of these structures, with acoustic shadowing below. Due to the convexity and reflective nature of the frontal bone, there is usually a mirror imaging artefact.
3.2.2. Ultrasound-Guided Filler Injection Techniques for the Frontal Region
- Scan before injecting
- Scan while injecting
Glabella
Forehead
Supraorbital Region
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Park, H.J.; Lee, J.H.; Lee, K.L.; Choi, Y.J.; Hu, K.S.; Kim, H.J. Ultrasonography Analysis of Vessels Around the Forehead Midline. Aesthetic Surg. J. 2021, 41, 1189–1194. [Google Scholar] [CrossRef]
- Thanasarnaksorn, W.; Cotofana, S.; Rudolph, C.; Kraisak, P.; Chanasumon, N.; Suwanchinda, A. Severe vision loss caused by cosmetic filler augmentation: Case series with review of cause and therapy. J. Cosmet. Dermatol. 2018, 17, 712–718. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.C.; Yu, N.; Wang, X.; Dong, R.; Long, X.; Feng, X.; Li, J.; Wu, W.T.L. Cerebral Embolism as a Result of Facial Filler Injections: A Literature Review. Aesthetic Surg. J. 2022, 42, NP162–NP175. [Google Scholar] [CrossRef] [PubMed]
- Schelke, L.; Farber, N.; Swift, A. Ultrasound as an Educational Tool in Facial Aesthetic Injections. Plast. Reconstr. Surg. Glob. Open 2022, 10, e4639. [Google Scholar] [CrossRef]
- Vasconcelos-Berg, R.; Izidoro, J.F.; Wenz, F.; Müller, A.; Navarini, A.A.; Sigrist, R.M.S. Doppler Ultrasound-Guided Filler Injections: Useful Tips to Integrate Ultrasound in Daily Practice. Aesthetic Surg. J. 2023, 43, 773–783. [Google Scholar] [CrossRef] [PubMed]
- Desyatnikova, S. Ultrasound-Guided Temple Filler Injection. Facial Plast. Surg. Aesthetic Med. 2022, 24, 501–503. [Google Scholar] [CrossRef]
- Kadouch, J.; Schelke, L.W.; Swift, A. Ultrasound to Improve the Safety and Efficacy of Lipofilling of the Temples. Aesthetic Surg. J. 2021, 41, 603–612. [Google Scholar] [CrossRef]
- Lee, W.; Park, J.W.; Yang, E.J. Temple augmentation by injecting a hyaluronic acid filler between the superficial and deep temporal fasciae. J. Cosmet. Dermatol. 2022, 21, 4313–4318. [Google Scholar] [CrossRef]
- Kim, S.B.; Hu, H.; Bae, H.; Yi, K.H. Anatomy of the temporal region to guide filler injections. Surg. Radiol. Anat. 2024, 46, 615–624. [Google Scholar] [CrossRef]
- Surek, C.C. A New Target for Temple Volumization? An Anatomical and Ultrasound-Guided Study of the Intermediate Temporal Fat Pad. Aesthetic Surg. J. 2021, 41, 1339–1343. [Google Scholar] [CrossRef]
- Desyatnikova, S. Understanding the Anatomic Layers of the Forehead Seen on Ultrasound: A Guide for Injectable Fillers and Chemodenervation. Facial Plast. Surg. Aesthetic Med. 2023, 25, 179–181. [Google Scholar] [CrossRef]
- Cotofana, S.; Velthuis, P.J.; Alfertshofer, M.; Frank, K.; Bertucci, V.; Beleznay, K.; Swift, A.; Gavril, D.L.; Lachman, N.; Schelke, L. The Change of Plane of the Supratrochlear and Supraorbital Arteries in the Forehead—An Ultrasound-Based Investigation. Aesthetic Surg. J. 2021, 41, NP1589–NP1598. [Google Scholar] [CrossRef]
- Tansatit, T.; Phumyoo, T.; Jitaree, B.; Sawatwong, W.; Rungsawang, C.; Jiirasutat, N.; Sahraoui, Y.M.E.; Lee, J.H. Ultrasound evaluation of arterial anastomosis of the forehead. J. Cosmet. Dermatol. 2018, 17, 1031–1036. [Google Scholar] [CrossRef]
- Bravo, B.S.F.; de Melo Carvalho, R.; Penedo, L.; de Bastos, J.T.; Calomeni Elias, M.; Cotofana, S.; Frank, K.; Moellhoff, N.; Freitag, L.; Alfertshofer, M. Applied anatomy of the layers and soft tissues of the forehead during minimally-invasive aesthetic procedures. J. Cosmet. Dermatol. 2022, 21, 5864–5871. [Google Scholar] [CrossRef]
- Choi, Y.J.; Lee, K.W.; Gil, Y.C.; Hu, K.S.; Kim, H.J. Ultrasonographic Analyses of the Forehead Region for Injectable Treatments. Ultrasound Med. Biol. 2019, 45, 2641–2648. [Google Scholar] [CrossRef]
- Phumyoo, T.; Jiirasutat, N.; Jitaree, B.; Rungsawang, C.; Uruwan, S.; Tansatit, T. Anatomical and Ultrasonography-Based Investigation to Localize the Arteries on the Central Forehead Region During the Glabellar Augmentation Procedure. Clin. Anat. 2020, 33, 370–382. [Google Scholar] [CrossRef]
- Kapoor, K.M.; Bertossi, D.; Li, C.Q.; Saputra, D.I.; Heydenrych, I.; Yavuzer, R. A Systematic Literature Review of the Middle Temporal Vein Anatomy: ‘Venous Danger Zone’ in Temporal Fossa for Filler Injections. Aesthetic Plast. Surg. 2020, 44, 1803–1810. [Google Scholar] [CrossRef]
- Cotofana, S.; Gaete, A.; Hernandez, C.A.; Casabona, G.; Bay, S.; Pavicic, T.; Coimbra, D.; Suwanchinda, A.; Swift, A.; Green, J.B.; et al. The six different injection techniques for the temple relevant for soft tissue filler augmentation procedures–Clinical anatomy and danger zones. J. Cosmet. Dermatol. 2020, 19, 1570–1579. [Google Scholar] [CrossRef]
- Cong, L.Y.; Phothong, W.; Lee, S.H.; Wanitphakdeedecha, R.; Koh, I.; Tansatit, T.; Kim, H.J. Topographic Analysis of the Supratrochlear Artery and the Supraorbital Artery: Implication for Improving the Safety of Forehead Augmentation. Plast. Reconstr. Surg. 2017, 139, 620e–627e. [Google Scholar] [CrossRef]
- Shen, W.W.; Du, J.N.; Ma, J.X.; Xia, Y.C.; Cui, L.G. Evaluation of Supratrochlear, Supraorbital and Angular Artery Course Variations and Depth by Doppler Ultrasound. Aesthetic Plast. Surg. 2023, 47, 791–798. [Google Scholar] [CrossRef]
- Cotofana, S.; Alfertshofer, M.; Frank, K.; Bertucci, V.; Beleznay, K.; Nikolis, A.; Sykes, J.; Swift, A.; Lachman, N.; Schenck, T.L. Relationship Between Vertical Glabellar Lines and the Supratrochlear and Supraorbital Arteries. Aesthetic Surg. J. 2020, 40, 1341–1348. [Google Scholar] [CrossRef]
- Walker, L.; Convery, C.; Davies, E.; Murray, G.; Croasdell, B. Consensus Opinion for The Management of Soft Tissue Filler Induced Vision Loss. J. Clin. Aesthetic Dermatol. 2021, 14, E84–E94. [Google Scholar]
- Kim, J. Novel Forehead Augmentation Strategy: Forehead Depression Categorization and Calcium-Hydroxyapatite Filler Delivery after Tumescent Injection. Plast. Reconstr. Surg. Glob. Open 2018, 6, e1858. [Google Scholar] [CrossRef]
- Sykes, J.M.; Cotofana, S.; Trevidic, P.; Solish, N.; Carruthers, J.; Carruthers, A.; Moradi, A.; Swift, A.; Massry, G.G.; Lambros, V.; et al. Upper Face: Clinical Anatomy and Regional Approaches with Injectable Fillers. Plast. Reconstr. Surg. 2015, 136 (Suppl. S5), 204S–218S. [Google Scholar] [CrossRef]
- Nikolis, A.; Enright, K.M.; Troupis, T.; Koutsilieris, M.; Stratigos, A.J.; Rigopoulos, D.; Cotofana, S. Topography of the deep temporal arteries and implications for performing safe aesthetic injections. J. Cosmet. Dermatol. 2022, 21, 608–614. [Google Scholar] [CrossRef]
- Wortsman, X. The Accuracy of Ultrasonography on Location of Lipomas in Forehead. Dermatol. Surg. 2017, 43, 158–159. [Google Scholar] [CrossRef]
- Wortsman, X. Atlas of Dermatologic Ultrasound; Springer International Publishing AG: Cham, Switzerland, 2018. [Google Scholar]
- Yuan, L.; Zhuang, J.; Chai, H.; Wu, Y.; Su, X.; Jiang, L.; Jia, Y.; Hu, J.; Wang, Y. An Exploration of the Anatomy of the Forehead of Asians and Its Relationship with Forehead Lines Based on Ultrasound Imaging. Aesthetic Surg. J. 2023, 43, NP956–NP961. [Google Scholar] [CrossRef]
- Zhuang, J.; Yuan, L.; Shai, H.; Hu, J.; Wang, Y. Response to: Demystifying the Forehead Using Ultrasonography. Aesthetic Surg. J. 2024, 44, NP525–NP526. [Google Scholar] [CrossRef]
- Meneses, C.C.B.; Freitas, S.; Knoedler, L.; Knoedler, S.; Davidovic, K.; Bravo, C.; Pappas, A.; Biesman, B.S.; Alfertshofer, M.; Cotofana, S. Increasing precision during neuromodulator injections for frontal rhytids—Using ultrasound imaging to identify the line of convergence. J. Cosmet. Dermatol. 2024, 23, 2373–2379. [Google Scholar] [CrossRef]
- Abdulsalam, A.J.; Ricci, V.; Cocco, G.; Aksakal, M.F.; Kara, M.; Özçakar, L. Demystifying the Forehead Using Ultrasonography. Aesthetic Surg. J. 2024, 44, NP523–NP524. [Google Scholar] [CrossRef]
- Ingallina, F.; Alfertshofer, M.G.; Schelke, L.; Velthuis, P.J.; Frank, K.; Mardini, S.; Millesi, E.; Ehrl, D.; Green, J.B.; Cotofana, S. The Fascias of the Forehead and Temple Aligned—An Anatomic Narrative Review. Facial Plast. Surg. Clin. N. Am. 2022, 30, 215–224. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Region | Scan before Injecting | Scan While Injecting | Desired Planes to Inject | What to Avoid in This Region |
|---|---|---|---|---|
| Temporal Region Technique 1: Subdermal filler placement | No | Yes | Subcutaneous fat tissue | Superficial temporal artery and vein |
| Temporal Region Technique 2: Interfascial filler placement | No | Yes | Interfascial plane between the superficial temporal fascia and deep temporal fascia (superficial lamina) | Superficial temporal artery and vein, middle temporal vein, sentinel vein |
| Temporal Region Technique 3: Low supraperiosteal filler placement (“one up, one over” technique) | Yes | No | Supraperiosteal plane | Anterior deep temporal artery |
| Frontal Region: Glabella | Yes | Yes | Usually superficial, may vary according to the depth of the arteries on DUS | Supratrochlear, central and paracentral arteries |
| Frontal Region: Forehead | Yes | Yes | Usually deep, may vary according to the depth of the arteries on DUS | Supraorbital, supratrochlear, central and paracentral arteries |
| Frontal Region: Supraorbital region | Yes | Yes | ROOF | Supraorbital artery |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sigrist, R.; Desyatnikova, S.; Chammas, M.C.; Vasconcelos-Berg, R. Best Practices for the Use of High-Frequency Ultrasound to Guide Aesthetic Filler Injections—Part 1: Upper Third of the Face. Diagnostics 2024, 14, 1718. https://doi.org/10.3390/diagnostics14161718
Sigrist R, Desyatnikova S, Chammas MC, Vasconcelos-Berg R. Best Practices for the Use of High-Frequency Ultrasound to Guide Aesthetic Filler Injections—Part 1: Upper Third of the Face. Diagnostics. 2024; 14(16):1718. https://doi.org/10.3390/diagnostics14161718
Chicago/Turabian StyleSigrist, Rosa, Stella Desyatnikova, Maria Cristina Chammas, and Roberta Vasconcelos-Berg. 2024. "Best Practices for the Use of High-Frequency Ultrasound to Guide Aesthetic Filler Injections—Part 1: Upper Third of the Face" Diagnostics 14, no. 16: 1718. https://doi.org/10.3390/diagnostics14161718
APA StyleSigrist, R., Desyatnikova, S., Chammas, M. C., & Vasconcelos-Berg, R. (2024). Best Practices for the Use of High-Frequency Ultrasound to Guide Aesthetic Filler Injections—Part 1: Upper Third of the Face. Diagnostics, 14(16), 1718. https://doi.org/10.3390/diagnostics14161718