Abstract
Meningiomas are tumors originating from arachnoid meningothelial cells. Occasionally, meningiomas are identified outside the central nervous system, and are referred to as extracranial meningiomas (EMs). The vast majority of EMs are an extension from an intracranial or intraspinal tumor. However, primary EMs may arise from extracranial sites with the most common sites being the skin and scalp subcutis, which are further categorized as cutaneous meningiomas (CMs). CMs are rare cutaneous tumors with similar ultrastructural and cytologic findings compared to those of intracranial meningiomas, but with a wide range of histologic differences. Therefore, an assessment using a panel of investigative tools, including imaging, histopathology, and immunohistochemistry, is required to determine the diagnosis of CMs. Here, we report the case of a 64-year-old gentleman presenting with a posttraumatic well-circumscribed superficial mass overlying the right nasal bridge. We are unable to identify other cases arising in the nasal bridge.
Meningiomas are the most frequently reported primary central nervous system (CNS) neoplasms in adults, accounting for over one-third of all CNS tumors [1]. They are classified as intracranial extra-axial neoplasms by the World Health Organization (WHO) due to their origin from arachnoid meningothelial cells. While most intracranial meningiomas are typically diagnosed via medical imaging and subsequent histopathologic examination, extracranial meningiomas are easily misdiagnosed due to their rarity and a broad spectrum of differential diagnoses with benign nerve sheath tumors and skin tumors. The diagnosis is typically made only after histopathologic examination in most cases [2,3]. Complete surgical excision is the first-line treatment for the majority of symptomatic and enlarging extracranial meningiomas, and patients exhibit favorable prognosis and a low recurrence rate [4].
Extracranial meningiomas can be divided into primary and secondary extracranial meningiomas (PEMs and SEMs) based on the tumor origin, where SEMs present at a secondary location away from an existing primary intracranial tumor, whereas PEMs refer to the meningiomas that arise from extracranial sites without a known primary intracranial tumor [5]. The common sites for PEMs are the head and neck region, including the skin and the scalp subcutis; sinonasal PEMs are less common [6]. Although extracranial meningiomas are rare, extension and metastasis from intracranial or intraspinal tumors comprise the vast majority of extracranial meningiomas. Therefore, the exclusion of a primary intracranial meningioma is required for the diagnosis of a PEM.
Primary cutaneous meningiomas are usually present at birth, with a high occurrence on the scalp, forehead, and paravertebral regions [7]; these are designated as type I lesions thought to derive from ectopic arachnoid cells [8]. Type II lesions usually present in adulthood and are derived from meningothelial cells located in the cutis. Type II lesions have been speculated to arise from ectopic meningothelial cells, potentially displaced from the arachnid during head trauma. Type III lesions are defined by direct extension from intracranial or intraspinal tumors [8]. Herein, we report an unusual case of a Type II cutaneous meningioma involving the nasal bridge that may be associated with remote head trauma (Figure 1 and Figure 2).
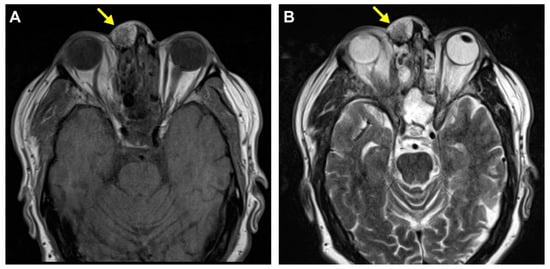
Figure 1.
Radiologic finding of the mass on MRI imaging. A 64-year-old man presented with a slightly tender mass overlying the right nasal bridge following back surgery three years ago. An axial T1 non-contrast CT scan revealed a well-circumscribed soft tissue mass external to the right nasal bone with no intracranial or sinus communication (A). An MRI scan showed a recently enlarging 2.0 × 1.4 × 1.1 cm circumscribed superficial mass with heterogeneous enhancement and mixed fat and soft tissue signal intensity components overlying the right nasal bridge (B).
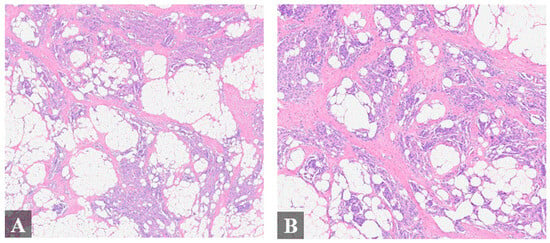
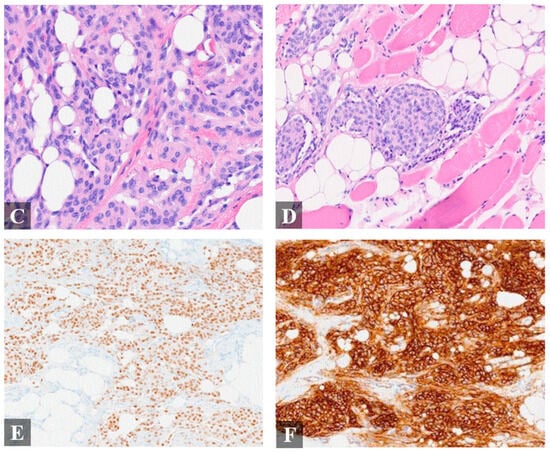
Figure 2.
Histologic finding of the resected mass. Histologic examination of the specimen showed a meningothelial vascular-rich epithelial proliferation arranged in nodular nests heterogeneously distributed within fibroadipose tissue and skeletal muscle (A–D), resembling a glomus tumor or “meningiolipoma”. (A), 4× magnification; (B), 4× magnification; (C), 20× magnification; (D), 20× magnification. Immunohistochemistry (IHC) exhibited immunoreactivity for epithelial membrane antigen (EMA), progesterone receptor ((E), 20× magnification), somatostatin receptor 2 ((F), 20× magnification), and androgen receptor. Cytokeratin AE1/AE3, p63, S100, smooth muscle actin, desmin, and HMB-45 were negative.
Author Contributions
Conceptualization, W.H.Y.; data curation, D.R. and J.L.; writing—original draft preparation, D.R. and W.H.Y.; visualization, E.K. and W.H.Y.; supervision, M.P.-R. and W.H.Y. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Written informed consent was obtained from the patient to publish this paper.
Data Availability Statement
The authors declare that all the data described in this article are available upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Ostrom, Q.T.; Gittleman, H.; Farah, P.; Ondracek, A.; Chen, Y.; Wolinsky, Y.; Stroup, N.E.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS statistical report: Primary brain and central nervous system tumors diagnosed in the United States in 2006–2010. Neuro-oncology 2013, 15 (Suppl. S2), ii1–ii56. [Google Scholar] [CrossRef] [PubMed]
- Agaimy, A.; Buslei, R.; Coras, R.; Rubin, B.P.; Mentzel, T. Comparative study of soft tissue perineurioma and meningioma using a five-marker immunohistochemical panel. Histopathology 2014, 65, 60–70. [Google Scholar] [CrossRef] [PubMed]
- Koutlas, I.G.; Scheithauer, B.W.; Folpe, A.L. Intraoral perineurioma, soft tissue type: Report of five cases, including 3 intraosseous examples, and review of the literature. Head Neck Pathol. 2010, 4, 113–120. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Liu, H.; Qian, H.; Li, X.; Zuo, F.; Meng, X.; Liu, S.; Wan, J. Clinial Features, Individualized Treatment and Long-Term Surgical Outcomes of Skull Base Meningiomas with Extracranial Extensions. Front. Oncol. 2020, 10, 1054. [Google Scholar] [CrossRef] [PubMed]
- Simpson, M.T.; Sneddon, K.J. Extracranial meningioma of the oral cavity. Br. J. Oral Maxillofac. Surg. 1987, 25, 520–525. [Google Scholar] [CrossRef] [PubMed]
- Miedema, J.R.; Zedek, D. Cutaneous meningioma. Arch. Pathol. Lab. Med. 2012, 136, 208–211. [Google Scholar] [CrossRef] [PubMed]
- Zeikus, P.; Robinson-Bostom, L.; Stopa, E. Primary cutaneous meningioma in association with a sinus pericranii. J. Am. Acad. Dermatol. 2006, 54 (Suppl. S2), S49–S50. [Google Scholar] [CrossRef] [PubMed]
- Arnold, M.; Cleaver, D.; Cleaver, N. Type II Cutaneous Meningioma. Dermatol. Surg. 2020, 46, 1449–1451. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).