

CBCT Evaluation of Alveolar Bone Change and Root Resorption after Orthodontic Treatment: A Retrospective Study

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design, Patient Selection, and Measurements
- Healthy adults (with completed development phase);
- No history of trauma;
- No previous orthodontic treatment;
- No periodontal disease;
- No significant illness related to bone metabolism;
- No movement or metal artifact on the CBCT images;
- Good quality and contrast imaging;
- Presence of at least a central incisor (CI), a first premolar (1PM), and a first molar (1M) in each dental arch;
- Patient underwent fixed orthodontic treatment with or without upper first or second premolar extraction cases using Roth prescription brackets (American Orthodontics, Sheboygan, WI, USA).
- Incomplete or sectional CBCT imaging;
- Previous orthodontic treatment;
- Systemic disease or medications that would influence the outcome of treatment;
- Patients that could not keep up with regular appointments during treatment;
- Failure to follow oral hygiene protocols during treatment (OHI).
2.1.1. Cone Beam Computed Tomography (CBCT)
2.1.2. Assessment of Alveolar Bone Level (ABL)
- Buccal and lingual ABL (B/L-ABL) measurements were performed in the sagittal plane for anterior teeth and in the coronal plane for posterior teeth.
- Mesial and distal ABL (M/D-ABL) measurements were performed in the coronal plane for anterior teeth and in the sagittal plane for posterior teeth.
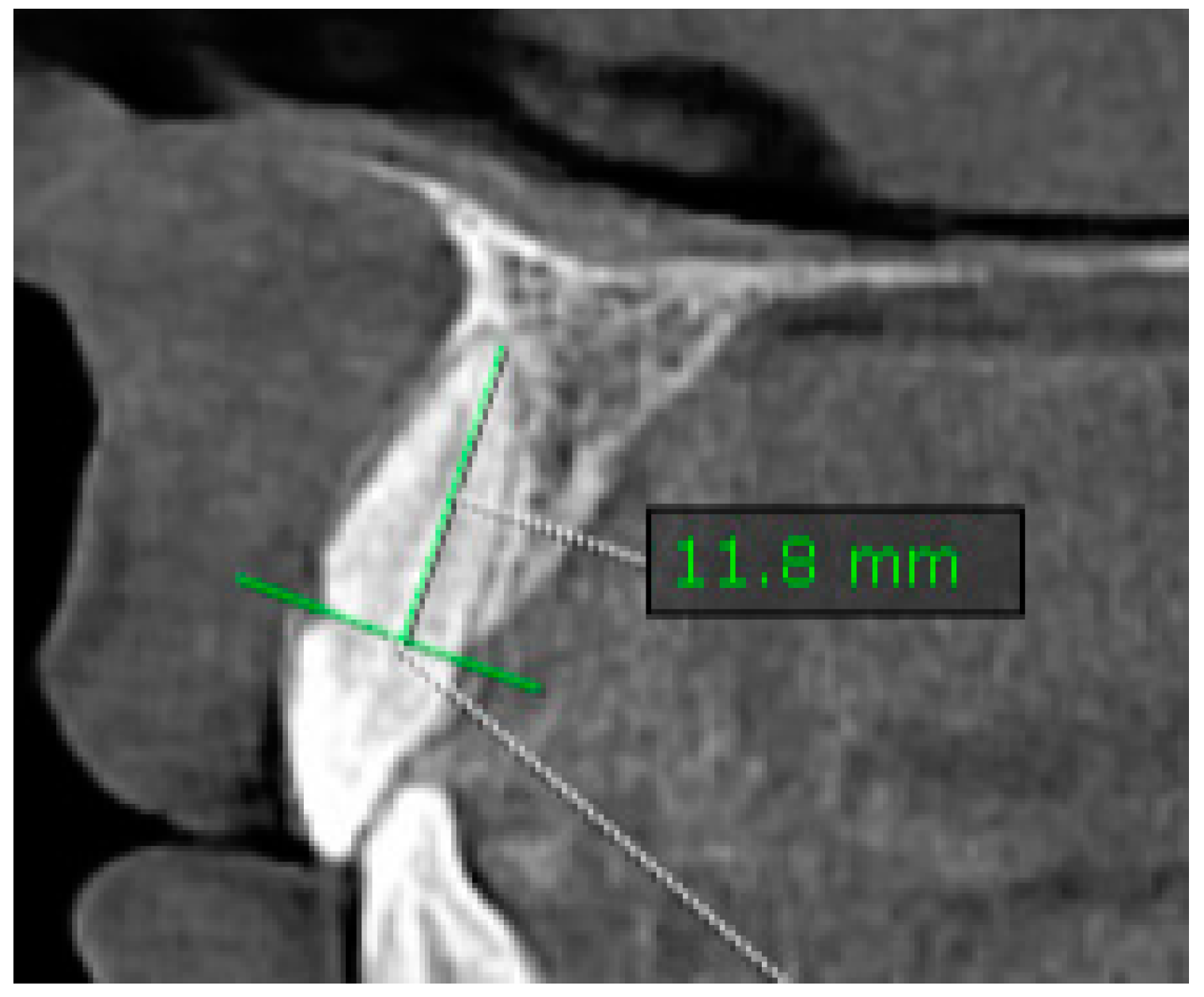
2.1.3. Assessment of Root Length (RL)
- Measurements were taken in the sagittal plane at the CIs of maxillary and mandibular teeth (Figure 2).
2.2. Data Collection
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hathaway-Schrader, J.D.; Novince, C.M. Maintaining homeostatic control of periodontal bone tissue. Periodontol. 2000 2021, 86, 157–187. [Google Scholar] [CrossRef] [PubMed]
- Alasqah, M.; Alshammery, D.A.; Baseer, M.A.; Aladwane, H.; Alsakr, A. Evaluation of alveolar bone level after orthodontic clear aligners treatment: A retrospective study. Saudi J. Oral Sci. 2024, 11, 26–36. [Google Scholar] [CrossRef]
- Antoun, J.S.; Mei, L.; Gibbs, K.; Farella, M. Effect of orthodontic treatment on the periodontal tissues. Periodontol. 2000 2017, 74, 140–157. [Google Scholar] [CrossRef] [PubMed]
- Tondelli, P.M. Orthodontic treatment as an adjunct to periodontal therapy. Dent. Press J. Orthod. 2019, 24, 80–92. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Harris, E.F.; Baker, W.C. Loss of root length and crestal bone height before and during treatment in adolescent and adult orthodontic patients. Am. J. Orthod. Dentofac. Orthop. 1990, 98, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Handelman, C.S. The anterior alveolus: Its importance in limiting orthodontic treatment and its influence on the occurrence of iatrogenic sequelae. Angle Orthod. 1996, 66, 95–109. [Google Scholar] [PubMed]
- Yousif, A.A.A.; Elmarhoumy, S. Alveolar Bone Changes after Orthodontic Tooth Movements: A CBCT Study. Egypt. Dent. J. 2020, 66, 747–757. [Google Scholar] [CrossRef]
- Nauli, J.; Thahar, B.; Salim, J.; Mardiati, E. The influence of orthodontic treatment period using the standard edgewise fixed device on the resorption of the top of alveolar bone in canines region, mandible second premolar, and first molar. Padjadjaran J. Dent. 2014, 26. [Google Scholar] [CrossRef]
- Natto, Z.S.; Olwi, A.; Abduljawad, F. A comparison of the horizontal and vertical bitewing images in detecting approximal caries and interdental bone loss in posterior teeth: A diagnostic accuracy randomized cross over clinical trial. J. Dent. Sci. 2023, 18, 645–651. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Christiaens, V.; Pauwels, R.; Mowafey, B.; Jacobs, R. Accuracy of Intra-Oral Radiography and Cone Beam Computed Tomography in the Diagnosis of Buccal Bone Loss. J. Imaging 2023, 9, 164. [Google Scholar] [CrossRef]
- Jäger, F.; Mah, J.K.; Bumann, A. Peridental bone changes after orthodontic tooth movement with fixed appliances: A cone-beam computed tomographic study. Angle Orthod. 2017, 87, 672–680. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zasčiurinskienė, E.; Lund, H.; Lindsten, R.; Jansson, H.; Bjerklin, K. Outcome of periodontal-orthodontic treatment in subjects with periodontal disease. Part II: A CBCT study of alveolar bone level changes. Eur. J. Orthod. 2019, 41, 565–574. [Google Scholar] [CrossRef] [PubMed]
- Castro, L.O.; Castro, I.O.; de Alencar, A.H.; Valladares-Neto, J.; Estrela, C. Cone beam computed tomography evaluation of distance from cementoenamel junction to alveolar crest before and after nonextraction orthodontic treatment. Angle Orthod. 2016, 86, 543–549. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nahm, K.Y.; Kang, J.H.; Moon, S.C.; Choi, Y.S.; Kook, Y.A.; Kim, S.H.; Huang, J. Alveolar bone loss around incisors in Class I bidentoalveolar protrusion patients: A retrospective three-dimensional cone beam CT study. Dentomaxillofac. Radiol. 2012, 41, 481–488. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ma, Z.G.; Yang, C.; Fang, B.; Xia, Y.H.; Mao, L.X.; Feng, Y.M. Three-D imaging of dental alveolar bone change after fixed orthodontic treatment in patients with periodontitis. Int. J. Clin. Exp. Med. 2015, 8, 2385–2391. [Google Scholar] [PubMed] [PubMed Central]
- Thilander, B. Infrabony pockets and reduced alveolar bone height in relation to orthodontic therapy. Semin. Orthod. 1996, 2, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Hong, H.; Zhou, J.; Fan, Q.; Jiao, R.; Kuang, Q.; Zhou, H.; Long, H. Characteristics of spatial changes in molars and alveolar bone resorption among patients with loss of mandibular first molars: A CBCT-based morphometric study. J. Clin. Med. 2023, 12, 1932. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Ji, L.; Zhao, Z.; Liao, W. Detailed Correlation between Central Incisor Movement and Alveolar Bone Resorption in Adults with Orthodontic Premolar Extraction Treatment: A Retrospective Cohort CBCT Study. J. Clin. Med. 2022, 11, 6872. [Google Scholar] [CrossRef] [PubMed]
- Scarfe, W.C.; Farman, A.G.; Sukovic, P. Clinical applications of cone-beam computed tomography in dental practice. J. Can. Dent. Assoc. 2006, 72, 75–80. [Google Scholar]
- Yassir, Y.A.; McIntyre, G.T.; Bearn, D.R. Orthodontic treatment and root resorption: An overview of systematic reviews. Eur. J. Orthod. 2021, 43, 442–456. [Google Scholar] [CrossRef]
- Samandara, A.; Papageorgiou, S.N.; Ioannidou-Marathiotou, I.; Kavvadia-Tsatala, S.; Papadopoulos, M.A. Evaluation of orthodontically induced external root resorption following orthodontic treatment using cone beam computed tomography (CBCT): A systematic review and meta-analysis. Eur. J. Orthod. 2019, 41, 67–79. [Google Scholar] [CrossRef] [PubMed]
- Deng, Y.; Sun, Y.; Xu, T. Evaluation of root resorption after comprehensive orthodontic treatment using cone beam computed tomography (CBCT): A meta-analysis. BMC Oral Health 2018, 18, 116. [Google Scholar] [CrossRef] [PubMed]
- Weltman, B.; Vig, K.W.; Fields, H.W.; Shanker, S.; Kaizar, E.E. Root resorption associated with orthodontic tooth movement: A systematic review. Am. J. Orthod. Dentofac. Orthop. 2010, 137, 462–476. discussion 12A. [Google Scholar] [CrossRef]
- Currell, S.D.; Liaw, A.; Blackmore Grant, P.D.; Esterman, A.; Nimmo, A. Orthodontic mechanotherapies and their influence on external root resorption: A systematic review. Am. J. Orthod. Dentofac. Orthop. 2019, 155, 313–329. [Google Scholar] [CrossRef] [PubMed]
- Nowzari, H.; Molayem, S.; Chiu, C.H.K.; Rich, S.K. Cone beam computed tomographic measurement of maxillary central incisors to determine prevalence of facial alveolar bone width $2 mm. Clin. Implant Dent. Relat. Res. 2012, 14, 595–602. [Google Scholar] [CrossRef]
- Castro, I.O.; Alencar, A.H.G.; Valladares, J.; Estrela, C. Apical root resorption due to orthodontic treatment detected by cone beam computed tomography. Angle Orthod. 2013, 83, 196–203. [Google Scholar] [CrossRef]
- Lund, H.; Gröndahl, K.; Gröndahl, H.G. Cone beam computed tomography evaluations of marginal alveolar bone before and after orthodontic treatment combined with premolar extractions. Eur. J. Oral Sci. 2012, 120, 201–211. [Google Scholar] [CrossRef]
- Ikeda, Y.; Chigasaki, O.; Mizutani, K.; Sasaki, Y.; Aoyama, N.; Mikami, R.; Gokyu, M.; Umeda, M.; Izumi, Y.; Aoki, A.; et al. The Potential of a Saliva Test for Screening of Alveolar Bone Resorption. Healthcare 2023, 11, 1822. [Google Scholar] [CrossRef] [PubMed]
- Maspero, C.; Gaffuri, F.; Castro, I.O.; Lanteri, V.; Ugolini, A.; Farronato, M. Correlation between Dental vestibular–palatal inclination and alveolar bone remodeling after Orthodontic Treatment: A CBCT Analysis. Materials 2019, 12, 4225. [Google Scholar] [CrossRef]
- Pan, F.; Yang, Z.; Wang, J.; Cai, R.; Liu, J.; Zhang, C.; Liao, W. Influence of orthodontic treatment with premolar extraction on the spatial position of maxillary third molars in adult patients: A retrospective cohort cone-bean computed tomography study. BMC Oral Health 2020, 20, 321. [Google Scholar] [CrossRef]
- Ahn, H.-W.; Moon, S.C.; Baek, S.-H. Morphometric evaluation of changes in the alveolar bone and roots of the maxillary anterior teeth before and after en masse retraction using cone-beam computed tomography. Angle Orthod. 2013, 83, 212–221. [Google Scholar] [CrossRef]
- Ising, N.; Kim, K.B.; Araujo, E.; Buschang, P. Evaluation of dehiscences using cone beam computed tomography. Angle Orthod. 2012, 82, 122–130. [Google Scholar] [CrossRef] [PubMed]
- Garlock, D.T.; Buschang, P.H.; Araujo, E.A.; Behrents, R.G.; Kim, K.B. Evaluation of marginal alveolar bone in the anterior mandible with pretreatment and posttreatment computed tomography in nonextraction patients. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 192–201. [Google Scholar] [CrossRef] [PubMed]
- Yu, Q.; Pan, X.; Ji, G.; Shen, G. The Association between Lower Incisal Inclination and Morphology of the Supporting Alveolar Bone—A Cone-Beam CT Study. Int. J. Oral Sci. 2009, 1, 217–223. [Google Scholar] [CrossRef]
- Son, E.J.; Kim, S.J.; Hong, C.; Chan, V.; Sim, H.Y.; Ji, S.; Hong, S.Y.; Baik, U.-B.; Shin, J.W.; Kim, Y.H.; et al. A study on the morphologic change of palatal alveolar bone shape after intrusion and retraction of maxillary incisors. Sci. Rep. 2020, 10, 14454. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y. Study on the perception of orthodontic treatment according to age: A questionnaire survey. Korean J. Orthod. 2017, 47, 215–221. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kapila, S.D.; Nervina, J.M. CBCT in orthodontics: Assessment of treatment outcomes and indications for its use. Dentomaxillofac. Radiol. 2015, 44, 20140282. [Google Scholar] [CrossRef] [PubMed]
- Mao, H.; Yang, A.; Pan, Y.; Li, H.; Lei, L. Displacement in root apex and changes in incisor inclination affect alveolar bone remodeling in adult bimaxillary protrusion patients: A retrospective study. Head Face Med. 2020, 16, 29. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Huang, J.; Jiang, J.-H. Morphological analysis of the alveolar bone of the anterior teeth in severe high-angle skeletal Class II and Class III malocclusions assessed with cone-beam computed tomography. PLoS ONE 2019, 14, e0210461. [Google Scholar] [CrossRef]
- Heinz, J.; Stewart, K.; Ghoneima, A. Evaluation of two-dimensional lateral cephalogram and three-dimensional cone beam computed tomography superimpositions: A comparative study. Int. J. Oral Maxillofac. Surg. 2019, 48, 519–525. [Google Scholar] [CrossRef]
- Choi, J.-Y.; Oh, S.H.; Kim, S.-H.; Ahn, H.-W.; Kang, Y.-G.; Choi, Y.-S.; Kook, Y.-A.; Nelson, G. Effectiveness of 2D radiographs in detecting CBCT-based incidental findings in orthodontic patients. Sci. Rep. 2021, 11, 9280. [Google Scholar] [CrossRef] [PubMed]
- Yodthong, N.; Charoemratrote, C.; Leethanakul, C. Factors related to alveolar bone thickness during upper incisor retraction. Angle Orthod. 2013, 83, 394–401. [Google Scholar] [CrossRef] [PubMed]
- Fuhrmann, R. Three-dimensional interpretation of periodontal lesions and remodeling during orthodontic treatment. Part III. J. Orofac. Orthop. 1996, 57, 224–237. [Google Scholar] [CrossRef] [PubMed]
- Bollen, A.M.; Cunha-Cruz, J.; Bakko, D.W.; Huang, G.J.; Hujoel, P.P. The effects of orthodontic therapy on periodontal health: A systematic review of controlled evidence. J. Am. Dent. Assoc. 2008, 139, 413–422. [Google Scholar] [CrossRef]
- Liu, H.; Xi, X.; Liu, D. Three-dimensional (3D) quantitative evaluation of the morphological changes of the upper anterior alveolar bone after retraction of a maxillary incisor. BMC Oral Health 2023, 23, 295. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Treatment Phase | Minimum | Maximum | Mean | Std. Deviation | Std. Error of Mean | Lower 95% CI of Mean | Upper 95% CI of Mean | |
|---|---|---|---|---|---|---|---|---|
| Pre-treatment | RU_CI | 1.3 | 5.7 | 2.853 | 1.039 | 0.2383 | 2.352 | 3.353 |
| LU_CI | 1.3 | 4.5 | 2.758 | 0.8167 | 0.1874 | 2.364 | 3.152 | |
| LL_CI | 1.3 | 6.1 | 3.463 | 1.311 | 0.3008 | 2.831 | 4.095 | |
| RL_CI | 1.8 | 5.8 | 3.529 | 1.438 | 0.3389 | 2.814 | 4.244 | |
| RU_PM1 | 1.8 | 6.5 | 3.735 | 1.234 | 0.2994 | 3.101 | 4.37 | |
| LU_PM1 | 1.2 | 5.5 | 3.569 | 1.138 | 0.2846 | 2.962 | 4.175 | |
| LL_PM1 | 1.8 | 5 | 3.358 | 0.9131 | 0.2095 | 2.918 | 3.798 | |
| RL_PM1 | 1.5 | 6 | 2.974 | 1.171 | 0.2686 | 2.409 | 3.538 | |
| RU_M1 | 2.6 | 5.4 | 3.275 | 0.7921 | 0.2287 | 2.772 | 3.778 | |
| LU_M1 | 1.5 | 5 | 3.723 | 0.8918 | 0.2473 | 3.184 | 4.262 | |
| LU_M1 | 2.2 | 3.1 | 2.68 | 0.3421 | 0.153 | 2.255 | 3.105 | |
| RL_M1 | 1.8 | 5.3 | 3.01 | 0.9643 | 0.3049 | 2.32 | 3.7 | |
| Post-treatment | RU_CI | 0.5 | 6.1 | 2.759 | 1.386 | 0.3361 | 2.046 | 3.471 |
| LU_CI | 1.3 | 5 | 2.682 | 0.8719 | 0.2115 | 2.234 | 3.131 | |
| LL_CI | 1.6 | 6.6 | 3.447 | 1.285 | 0.3117 | 2.786 | 4.108 | |
| RL_CI | 1.6 | 7.1 | 3.335 | 1.516 | 0.3677 | 2.556 | 4.115 | |
| RU_PM1 | 1.6 | 5.6 | 3.333 | 1.056 | 0.2727 | 2.749 | 3.918 | |
| LU_PM1 | 1.5 | 5.9 | 3.362 | 1.226 | 0.34 | 2.621 | 4.102 | |
| LL_PM1 | 1.7 | 6.2 | 3.167 | 1.213 | 0.2859 | 2.563 | 3.77 | |
| RL_PM1 | 2 | 4.4 | 3.106 | 0.8111 | 0.2028 | 2.674 | 3.538 | |
| RU_M1 | 2 | 4.9 | 3.067 | 0.9206 | 0.3069 | 2.359 | 3.774 | |
| LU_M1 | 0.8 | 5.4 | 3.533 | 1.162 | 0.3354 | 2.795 | 4.271 | |
| LL_M1 | 2 | 3.6 | 2.933 | 0.8327 | 0.4807 | 0.8649 | 5.002 | |
| RL_M1 | 1.6 | 5 | 3.075 | 1.229 | 0.4346 | 2.047 | 4.103 |
| Mean | Mean | p-Value | ||||
|---|---|---|---|---|---|---|
| Pre-treatment | RU_CI | 2.853 | Post-treatment | RU_CI | 2.759 | 0.5398 |
| LU_CI | 2.758 | LU_CI | 2.682 | 0.8499 | ||
| LL_CI | 3.463 | LL_CI | 3.447 | 0.9438 | ||
| RL_CI | 3.529 | RL_CI | 3.335 | 0.7259 | ||
| RU_PM1 | 3.735 | RU_PM1 | 3.333 | 0.1177 | ||
| LU_PM1 | 3.569 | LU_PM1 | 3.362 | 0.6719 | ||
| LL_PM1 | 3.358 | LL_PM1 | 3.167 | 0.2729 | ||
| RL_PM1 | 2974 | RL_PM1 | 3.106 | 0.2458 | ||
| RU_M1 | 3.275 | RU_M1 | 3.067 | 0.6328 | ||
| LU_M1 | 3.723 | LU_M1 | 3.533 | 0.3477 | ||
| LL_M1 | 2.68 | LL_M1 | 2.933 | 0.5179 | ||
| RL-M1 | 3.01 | RL_M1 | 3.075 | 0.9493 |
| Mean | Mean | p-Value | ||||
|---|---|---|---|---|---|---|
| Pre-treatment | RU_CI | 2.947 | Post-treatment | RU_CI | 2.665 | 0.4466 |
| LU_CI | 3.821 | LU_CI | 2.412 | 0.1674 | ||
| LL_CI | 2.405 | LL_CI | 2.683 | 0.5356 | ||
| RL_CI | 2.383 | RL_CI | 2.676 | 0.2781 | ||
| RU_PM1 | 2.529 | RU_PM1 | 2.627 | 0.9890 | ||
| LU_PM1 | 2.9 | LU_PM1 | 2.815 | 0.9268 | ||
| LL_PM1 | 2.963 | LL_PM1 | 2.574 | 0.1349 | ||
| RL-PM1 | 2.8 | RL-PM1 | 2.794 | 0.4711 | ||
| RU_M1 | 3.092 | RU_M1 | 3.018 | >0.9999 | ||
| LU_M1 | 2.885 | LU_M1 | 2.842 | 0.8411 | ||
| LL_M1 | 2.04 | LL_M1 | 2.467 | 0.3929 | ||
| RL-M1 | 2.28 | RL-M1 | 2.213 | 0.6250 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pop, S.I.; Cerghizan, D.; Mițariu, L.; Jánosi, K.M.; D’Andrea, A. CBCT Evaluation of Alveolar Bone Change and Root Resorption after Orthodontic Treatment: A Retrospective Study. Diagnostics 2024, 14, 1757. https://doi.org/10.3390/diagnostics14161757
Pop SI, Cerghizan D, Mițariu L, Jánosi KM, D’Andrea A. CBCT Evaluation of Alveolar Bone Change and Root Resorption after Orthodontic Treatment: A Retrospective Study. Diagnostics. 2024; 14(16):1757. https://doi.org/10.3390/diagnostics14161757
Chicago/Turabian StylePop, Silvia Izabella, Diana Cerghizan, Loredana Mițariu, Kinga Mária Jánosi, and Antonella D’Andrea. 2024. "CBCT Evaluation of Alveolar Bone Change and Root Resorption after Orthodontic Treatment: A Retrospective Study" Diagnostics 14, no. 16: 1757. https://doi.org/10.3390/diagnostics14161757
APA StylePop, S. I., Cerghizan, D., Mițariu, L., Jánosi, K. M., & D’Andrea, A. (2024). CBCT Evaluation of Alveolar Bone Change and Root Resorption after Orthodontic Treatment: A Retrospective Study. Diagnostics, 14(16), 1757. https://doi.org/10.3390/diagnostics14161757