
COVID-19-Related Cholangiopathy: Histological Findings

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
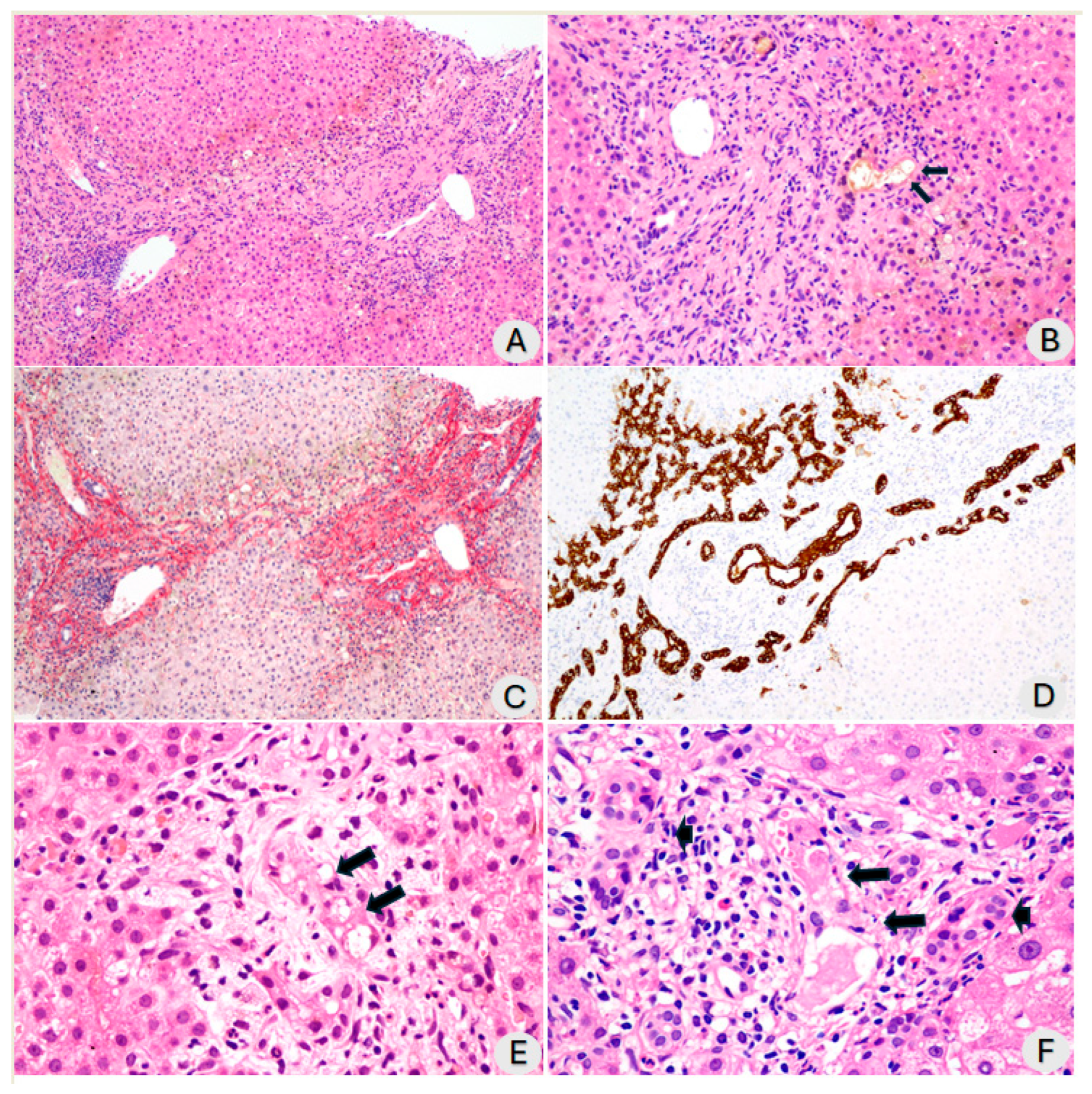
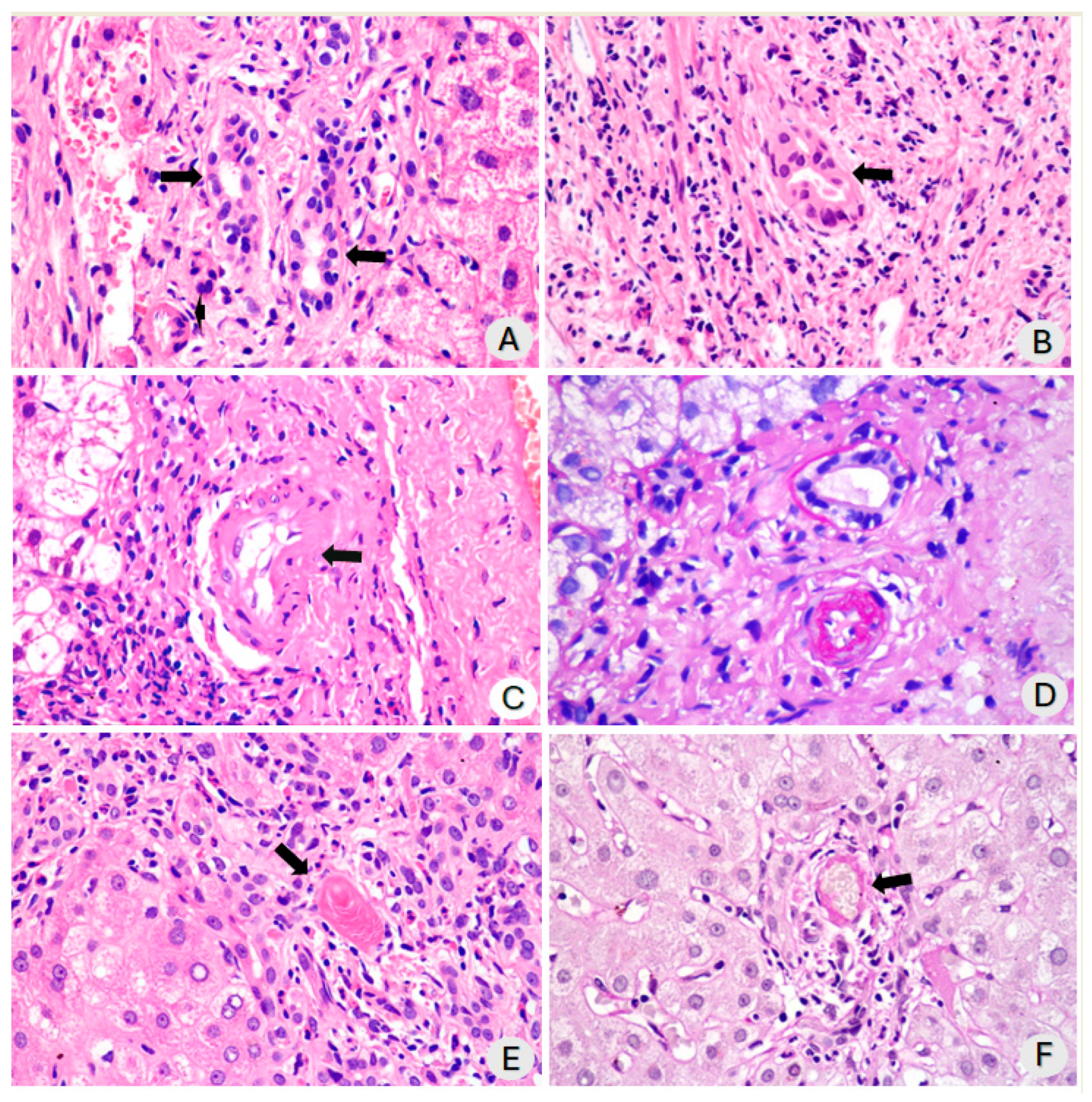
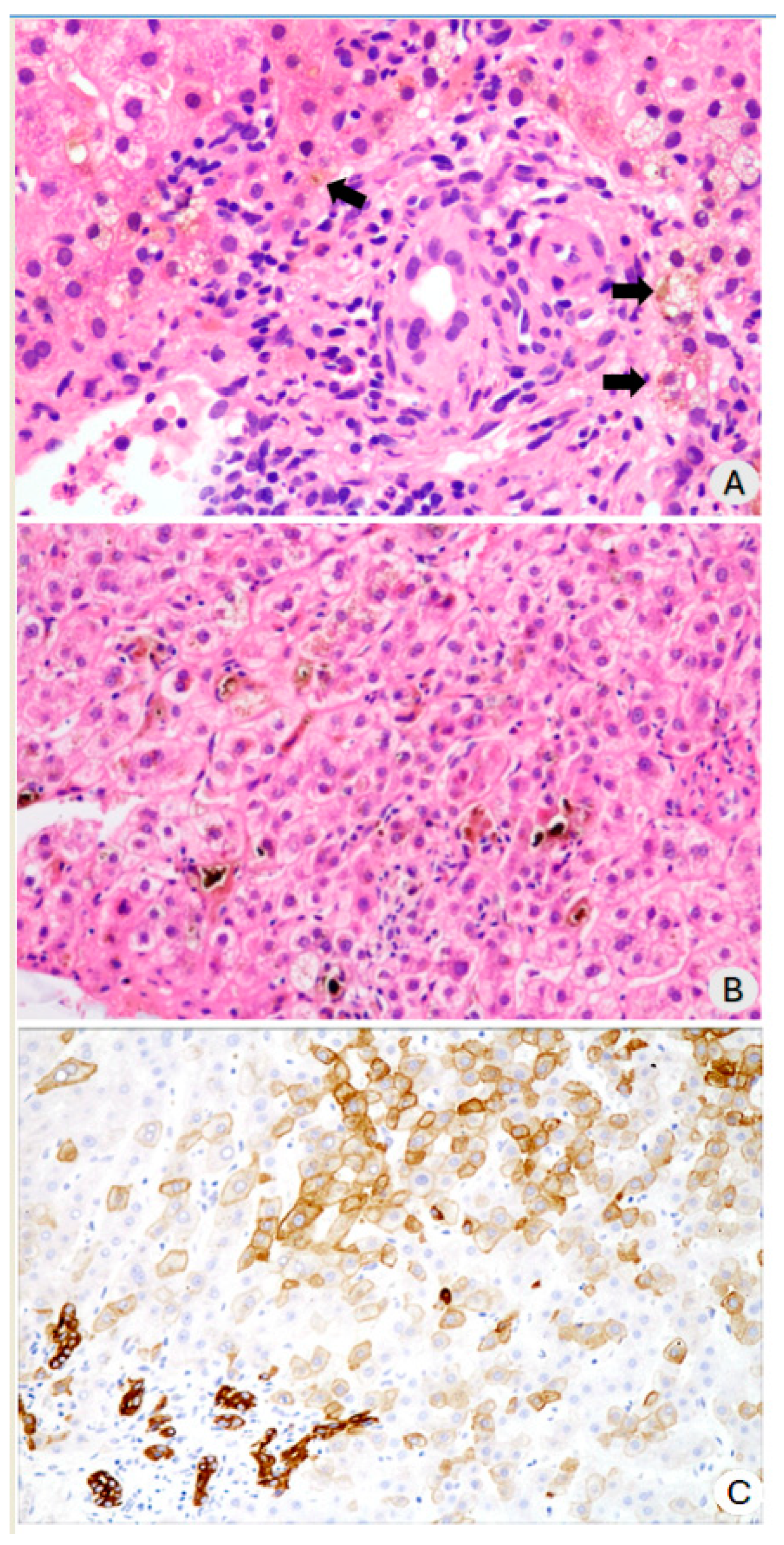
3.1. Histopathological Findings
3.2. Follow-Up
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Faruqui, S.; Okoli, F.C.; Olsen, S.K.; Feldman, D.M.; Kalia, H.S.; Park, J.S.; Stanca, C.M.; Diaz, V.F.; Yuan, S.; Dagher, N.N.; et al. Cholangiopathy after Severe COVID-19: Clinical Features and Prognostic Implications. Am. J. Gastroenterol. 2021, 116, 1414–1425. [Google Scholar] [CrossRef]
- Leonhardt, S.; Jürgensen, C.; Frohme, J.; Grajecki, D.; Adler, A.; Sigal, M.; Leonhardt, J.; Voll, J.M.; Kruse, J.M.; Körner, R.; et al. Hepatobiliary long-term consequences of COVID-19: Dramatically increased rate of secondary sclerosing cholangitis in critically ill COVID-19 patients. Hepatol. Int. 2023, 17, 1610–1625. [Google Scholar] [CrossRef]
- Werner, C.R.; Fusco, S.; Kienzle, K.; Döbele, S.; Artzner, K.; Malek, N.P.; Wichmann, D.; Göpel, S. Incidence of Secondary Sclerosing Cholangitis in Hospitalized Long COVID-19 Patients: A Retrospective Single Center Study. Diagnostics 2024, 14, 745. [Google Scholar] [CrossRef] [PubMed]
- Scheppach, W.; Druge, G.; Wittenberg, G.; Mueller, J.G.; Gassel, A.M.; Gassel, H.-J.; Richter, F. Sclerosing cholangitis and liver cirrhosis after extrabiliary infections: Report on three cases. Crit. Care Med. 2001, 29, 438–441. [Google Scholar] [CrossRef] [PubMed]
- Gelbmann, C.M.; Rümmele, P.; Wimmer, M.; Hofstädter, F.; Göhlmann, B.; Endlicher, E.; Kullmann, F.; Langgartner, J.; Schölmerich, J. Ischemic-Like Cholangiopathy with Secondary Sclerosing Cholangitis in Critically Ill Patients. Am. J. Gastroenterol. 2007, 102, 1221–1229. [Google Scholar] [CrossRef] [PubMed]
- Martins, P.; Machado, M.V. Secondary Sclerosing Cholangitis in Critically Ill Patients: An Underdiagnosed Entity. GE Port. J. Gastroenterol. 2019, 27, 103–114. [Google Scholar] [CrossRef]
- Roth, N.C.; Kim, A.; Vitkovski, T.; Xia, J.; Ramirez, G.; Bernstein, D.; Crawford, J.M. Post-COVID-19 Cholangiopathy: A Novel Entity. Am. J. Gastroenterol. 2021, 116, 1077–1082. [Google Scholar] [CrossRef]
- Faruqui, S.; Okoli, F.; Olsen, S.; Feldman, D.M.; Kalia, H.S.; Kim, S. Bile duct injury and severe cholestasis in patients recovering from severe COVID-19: A novel entity of COVID-associated cholangiopathy. AASLD Digit. Exp. 2020, 42. Available online: https://www.natap.org/2020/AASLD/AASLD_136.htm (accessed on 16 August 2024).
- Cotter, S.; Wong, J.; Gada, N.; Gill, R.; Jones, S.C.; Chai, G.; Foster, D.; Avigan, M.; Mundkur, M. Repeated or Continuous Medically Supervised Ketamine Administration Associated with Hepatobiliary Adverse Events: A Retrospective Case Series. Drug Saf. 2021, 44, 1365–1374. [Google Scholar] [CrossRef]
- de Tymowski, C.; Dépret, F.; Dudoignon, E.; Legrand, M.; Mallet, V. Ketamine-induced cholangiopathy in ARDS patients. Intensiv. Care Med. 2021, 47, 1173–1174. [Google Scholar] [CrossRef] [PubMed]
- Henrie, J.; Gerard, L.; Declerfayt, C.; Lejeune, A.; Baldin, P.; Robert, A.; Laterre, P.-F.; Hantson, P. Profile of liver cholestatic biomarkers following prolonged ketamine administration in patients with COVID-19. BMC Anesthesiol. 2023, 23, 44. [Google Scholar] [CrossRef]
- Leonhardt, S.; Baumann, S.; Jürgensen, C.; Hüter, L.; Leonhardt, J.; Höfert, L.; Bauer, M.; Tacke, F.; on behalf of the Ketamine Cast Research Group. Role of intravenous ketamine in the pathogenesis of secondary sclerosing cholangitis in critically ill patients: Perpetrator or innocent bystander? Answers provided by forensic toxicology. Intensiv. Care Med. 2023, 49, 1549–1551. [Google Scholar] [CrossRef]
- Mallet, V.; Bock, K.; Mandengue, P.D.; Dufour, N.; Voigtlaender, T.; Ricard, J.-D.; Isnard, P.; Frochot, V.; Letavernier, E.; Moga, L.; et al. Intravenous ketamine and progressive cholangiopathy in COVID-19 patients. J. Hepatol. 2021, 74, 1243–1244. [Google Scholar] [CrossRef]
- Kumar, V.; Abbas, A.K.; Aster, J.C.; Deyrup, A.T. Robbins & Kumar Basic Pathology, 11th ed.; International Edition; Elsevier: Philadelphia, PA, USA, 2023. [Google Scholar]
- Kerr, J.F.R. History of the events leading to the formulation of the apoptosis concept. Toxicology 2002, 181–182, 471–474. [Google Scholar] [CrossRef]
- Guicciardi, M.E.; Malhi, H.; Mott, J.L.; Gores, G.J. Apoptosis and necrosis in the liver. Compr. Physiol. 2013, 32, 977–1010. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef]
- Shih, A.R.; Hatipoglu, D.; Wilechansky, R.; Goiffon, R.; Deshpande, V.; Misdraji, J.; Chung, R.T. Persistent Cholestatic Injury and Secondary Sclerosing Cholangitis in COVID-19 Patients. Arch. Pathol. Lab. Med. 2022, 146, 1184–1193. [Google Scholar] [CrossRef]
- Durazo, F.A.; Nicholas, A.A.; Mahaffey, J.J.; Sova, S.; Evans, J.J.; Trivella, J.P.; Loy, V.; Kim, J.; Zimmerman, M.A.; Hong, J.C. Post-COVID-19 Cholangiopathy—A New Indication for Liver Transplantation: A Case Report. Transplant. Proc. 2021, 53, 1132–1137. [Google Scholar] [CrossRef]
- Ferreira, F.B.; Mourato, M.; Bragança, S.; Paulo, J.B.; Sismeiro, R.; Pereira, A.; Mónica, A.N.; Lourenço, L.C.; Cardoso, M. COVID-19-associated secondary sclerosing cholangitis—A case series of 4 patients. Clin. Res. Hepatol. Gastroenterol. 2022, 46, 102048. [Google Scholar] [CrossRef]
- Esposito, I.; Kubisova, A.; Stiehl, A.; Kulaksiz, H.; Schirmacher, P. Secondary sclerosing cholangitis after intensive care unit treatment: Clues to the histopathological differential diagnosis. Virchows Arch. 2008, 453, 339–345. [Google Scholar] [CrossRef]
- Deltenre, P.; Valla, D.-C. Ischemic cholangiopathy. J. Hepatol. 2006, 44, 806–817. [Google Scholar] [CrossRef]
- Onuiri, J.; I Fiel, M. COVID Cholangiopathy Can Occur Despite Mild COVID. Am. J. Clin. Pathol. 2022, 158, S128–S129. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines on sclerosing cholangitis. J. Hepatol. 2022, 77, 761–806. [Google Scholar] [CrossRef] [PubMed]
- Bütikofer, S.; Lenggenhager, D.; Garcia, P.D.W.; Maggio, E.M.; Haberecker, M.; Reiner, C.S.; Brüllmann, G.; Buehler, P.K.; Gubler, C.; Müllhaupt, B.; et al. Secondary sclerosing cholangitis as cause of persistent jaundice in patients with severe COVID-19. Liver Int. 2021, 41, 2404–2417. [Google Scholar] [CrossRef]
- Gudnason, H.O.; Björnsson, E.S. Secondary sclerosing cholangitis in critically ill patients: Current perspectives. Clin. Exp. Gastroenterol. 2017, 10, 105–111. [Google Scholar] [CrossRef]
- Umesh, A.; Pranay, K.; Pandey, R.C.; Gupta, M.K. Evidence mapping and review of long-COVID and its underlying pathophysiological mechanism. Infection 2022, 50, 1053–1066. [Google Scholar] [CrossRef]
- Carvalho, L.V.; Souza, C.d.S.; Fontes, J.L.; Cardoso, L.; Salomar, M.; Duarte-Neto, A.N.; Figueira, C.; Brito, R.; Mesquita, B.; de Freitas, L.A.; et al. COVID-19 beyond DAD: Persisting microcirculation thrombosis, hidden infections, and early pulmonary fibrosis as remaining challenges of the disease. Hum. Pathol. Rep. 2022, 27, 300607. [Google Scholar] [CrossRef]
- Teymouri, A.; Nasoori, H.; Fakheri, M.; Nasiri, A. Features of biliary tract diseases in ketamine abusers: A systematic review of case reports. J. Med. Case Rep. 2024, 18, 84. [Google Scholar] [CrossRef]
- Santana, M.F.; Guerra, M.T.; Hundt, M.A.; Ciarleglio, M.M.; Pinto, R.A.d.A.; Dutra, B.G.; Xavier, M.S.; Lacerda, M.V.G.; Ferreira, A.J.; Wanderley, D.C.; et al. Correlation Between Clinical and Pathological Findings of Liver Injury in 27 Patients with Lethal COVID-19 Infections in Brazil. Hepatol. Commun. 2021, 6, 270–280. [Google Scholar] [CrossRef]
- Massoth, L.R.; Desai, N.; Szabolcs, A.; Harris, C.K.; Neyaz, A.; Crotty, R.M.; Chebib, I.; Rivera, M.N.; Sholl, L.M.; Stone, J.R.; et al. Comparison of RNA In Situ Hybridization and Immunohistochemistry Techniques for the Detection and Localization of SARS-CoV-2 in Human Tissues. Am. J. Surg. Pathol. 2020, 45, 14–24. [Google Scholar] [CrossRef]
- Wang, X.-X.; Shao, C.; Huang, X.-J.; Sun, L.; Meng, L.-J.; Liu, H.; Zhang, S.-J.; Li, H.-J.; Lv, F.-D. Histopathological features of multiorgan percutaneous tissue core biopsy in patients with COVID-19. J. Clin. Pathol. 2020, 74, 522–527. [Google Scholar] [CrossRef]
- Rasheed, M.A.; Ballotin, V.R.; Bigarella, L.G.; Soldera, J. Post-COVID-19 cholangiopathy: Systematic review. World J. Methodol. 2023, 13, 296–322. [Google Scholar] [CrossRef]
- Yanny, B.; Alkhero, M.; Alani, M.; Stenberg, D.; Saharan, A.; Saab, S. Post-COVID-19 Cholangiopathy: A Systematic Review. J. Clin. Exp. Hepatol. 2022, 13, 489–499. [Google Scholar] [CrossRef]
- Rodriguez-Espada, A.; la Mora, M.S.-D.; Rodriguez-Paniagua, B.M.; la Rosa, N.L.-D.; Martinez-Gutierrez, M.I.; Pastrana-Brandes, S.; Navarro-Alvarez, N. Histopathological impact of SARS-CoV-2 on the liver: Cellular damage and long-term complications. World J. Gastroenterol. 2024, 30, 2866–2880. [Google Scholar] [CrossRef]
- Hofstetter, P.; Zuber-Jerger, I.; Mehrl, A.; Graf, B.; Lunz, D.; Lubnow, M.; Müller, T.; Schmid, S.; Müller, M.; Kandulski, A. Endoscopic Characterization and Outcome of COVID-19 Patients with Secondary Sclerosing Cholangitis: A Case Series of a Tertiary Center. J. Gastrointest. Liver Dis. 2024, 33, 218–225. [Google Scholar] [CrossRef]
- Ghafoor, S.; Germann, M.; Jüngst, C.; Müllhaupt, B.; Reiner, C.S.; Stocker, D. Imaging features of COVID-19-associated secondary sclerosing cholangitis on magnetic resonance cholangiopancreatography: A retrospective analysis. Insights Imaging 2022, 13, 128. [Google Scholar] [CrossRef]
- Leonhardt, S.; Grajecki, D.; Geisel, D.; Fehrenbach, U.; Adler, A.; Leonhardt, J.; Horst, D.; Kurth, F.; Thibeault, C.; Janssen, H.-J.; et al. Endoscopic Features of Post-COVID-19 Cholangiopathy and Its Management Using ERCP. Am. J. Gastroenterol. 2023, 119, 748–759. [Google Scholar] [CrossRef]
- Barnhill, M.S.; Jayasekera, C. Secondary Sclerosing Cholangiopathies. Curr. Hepatol. Rep. 2024, 23, 145–152. [Google Scholar] [CrossRef]
- Machado, M.C.C.; Filho, R.K.; el Bacha, I.A.H.; de Oliveira, I.S.; Ribeiro, C.M.d.F.; de Souza, H.P.; Parise, E.R. Post-COVID-19 Secondary Sclerosing Cholangitis: A Rare but Severe Condition with no Treatment Besides Liver Transplantation. Am. J. Case Rep. 2022, 23, e936250-1–e936250-5. [Google Scholar] [CrossRef]
- Ludwig, D.R.; Anderson, M.A.; Itani, M.; Sharbidre, K.G.; Lalwani, N.; Paspulati, R.M. Secondary sclerosing cholangitis: Mimics of primary sclerosing cholangitis. Abdom. Imaging 2022, 48, 151–165. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Gender, male, n (%) | 5 | (50%) |
| Molecular diagnosis of COVID-19, n (%) | 10 | (100%) |
| ICU admission, n (%) | 10 | (100%) |
| Mechanical ventilation, n (%) | 10 | (100%) |
| Age, years | ||
| Median [IQR] | 56 | [51.2–60] |
| Mean ± SD | 54.4 | ±12.2 |
| Hospital stays, days | ||
| Median [IQR] | 55 | [38–60.5] |
| Mean ± SD | 62.1 | ±34.1 |
| Alkaline phosphatase, U/L | ||
| Median [IQR] | 645.5 | [389.5–1256] |
| Mean ± SD | 804.8 | ±593.8 |
| Gamma-glutamyl transferase, U/L | ||
| Median [IQR] | 925.2 | [663.7–2169] |
| Mean ± SD | 1389 | ±1094.8 |
| Total bilirubin, mg/dL | 3 | 1–6 |
| Median [IQR] | 3.6 | [0.9–9.4] |
| Mean ± SD | 6.2 | ±6.6 |
| Aspartate aminotransferase, U/L | ||
| Median [IQR] | 86.8 | [67.6–105.7] |
| Mean ± SD | 86.8 | ±28.1 |
| Alanine aminotransferase, U/L | ||
| Median [IQR] | 100.3 | [86.2–113.2] |
| Mean ± SD | 107.6 | ±42.4 |
| Median or n | Range or % | |
|---|---|---|
| Number of portal tracts | 25 | 15–32 |
| Portal and periportal fibrosis | 10/10 | 100% |
| Septal fibrosis | 7/10 | 70% |
| Periductal fibrosis (mild) | 2/10 | 2% |
| Inflammatory infiltrate (mild to moderate) | 10/10 | 100% |
| Bile duct dystrophy | 10/10 | 100% |
| Bile plugs in bile ductules | 6/10 | 60% |
| Swelling of endothelial cells of arterioles | 5/10 | 50% |
| Microthrombi in small vessels | 1/10 | 10% |
| Ductopenia | 0/10 | 0% |
| Parenchymal cholestasis (Mild to severe) | 9/10 | 90% |
| Biliary infarcts (Multiple small) | 1/10 | 10% |
| Hepatocyte biliary metaplasia (Cytokeratin 7+ cells) | 7/7 | 100% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borges, V.F.A.; Cotrim, H.P.; Andrade, A.R.C.F.; Mendes, L.S.C.; Penna, F.G.C.; Silva, M.C.; Salomão, F.C.; Freitas, L.A.R. COVID-19-Related Cholangiopathy: Histological Findings. Diagnostics 2024, 14, 1804. https://doi.org/10.3390/diagnostics14161804
Borges VFA, Cotrim HP, Andrade ARCF, Mendes LSC, Penna FGC, Silva MC, Salomão FC, Freitas LAR. COVID-19-Related Cholangiopathy: Histological Findings. Diagnostics. 2024; 14(16):1804. https://doi.org/10.3390/diagnostics14161804
Chicago/Turabian StyleBorges, Valéria F. A., Helma P. Cotrim, Antônio Ricardo C. F. Andrade, Liliana S. C. Mendes, Francisco G. C. Penna, Marcelo C. Silva, Frederico C. Salomão, and Luiz A. R. Freitas. 2024. "COVID-19-Related Cholangiopathy: Histological Findings" Diagnostics 14, no. 16: 1804. https://doi.org/10.3390/diagnostics14161804