
A Systematic Review of the Key Predictors of Progression and Mortality of Rheumatoid Arthritis-Associated Interstitial Lung Disease


Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility
2.2. Search Strategy
2.3. Data Extraction
3. Results
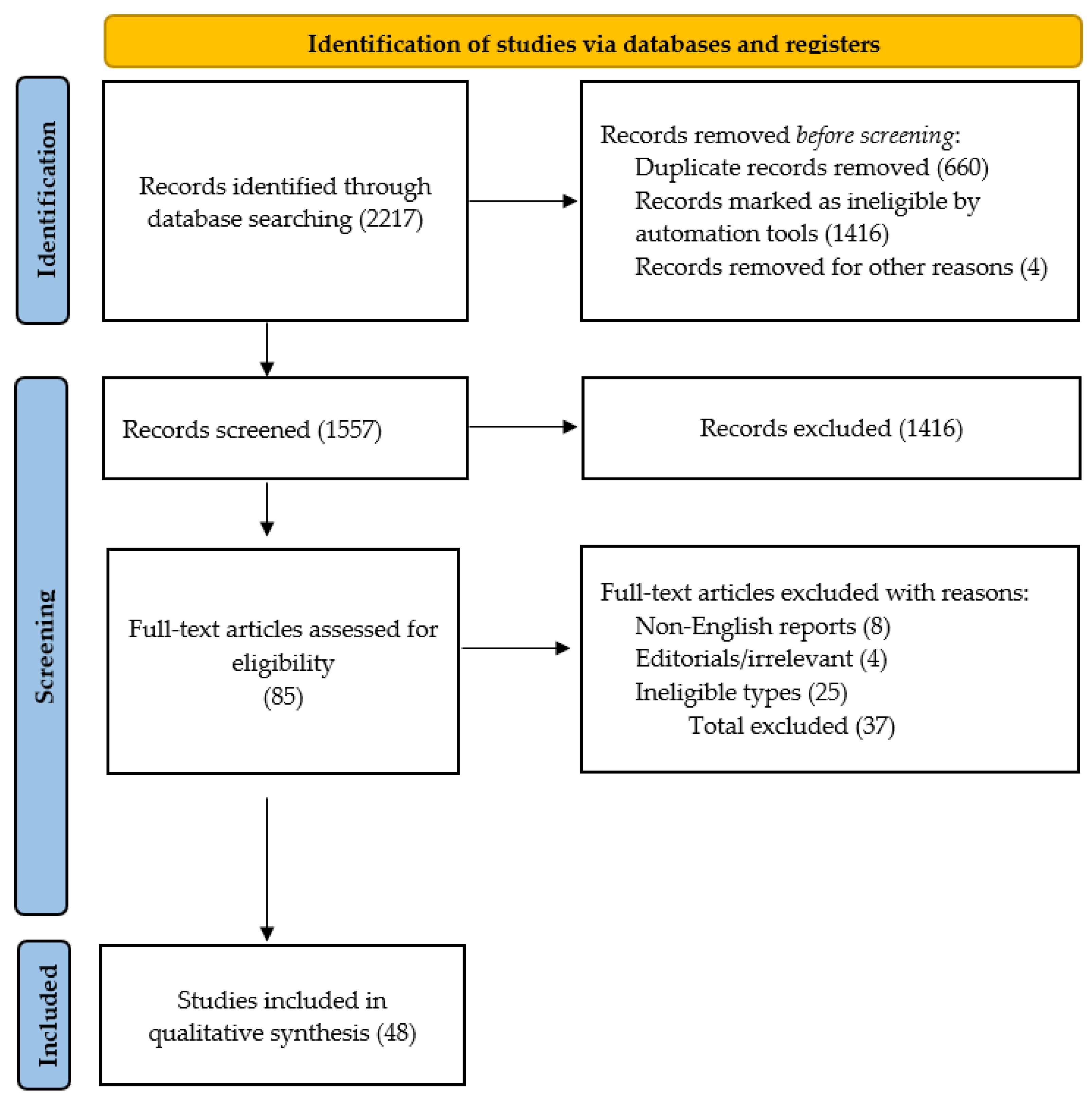
3.1. Selection of Studies
3.2. Demographic Features of Eligible Studies
3.3. Risk Factors of Lung Function Decline
3.4. Prognostic Factors for All-Cause Mortality of RA-ILD
3.5. Additional Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Study | Design | Subjects (n) | Smoking (n, %) | UIP Pattern (n, %) | Frequency of Lung Function Decline (n, %) | All-Cause Mortality (n, %) |
|---|---|---|---|---|---|---|
| Akiyama et al., 2016 [72] | Case/control retrospective (2008–2014) | 395 | 69 (20.3) | 78 (19.7) | 6 (1.5) | |
| Franzen et al., 2016 [83] | Observational retrospective (2013–2015) | 33 | 17 (51) | 6 (22) | ||
| Md Yusof et al., 2017 [84] | Observational retrospective (2004–2015) | 56 | 32 (57) | 20 (36) | 14 (25) | 9 (16) |
| Mochizuki et al., 2018 [40] | Observational retrospective, 47.8 months | 131 | ||||
| Kim et al., 2010 [60] | Observational retrospective (2001–2008) | 82 | 59 (72) | 20 (24) | 8 (9.7) | |
| Zamora-Legoff et al., 2016 [51] | Observational retrospective (1998–2014) | 167 | 105 (63) | 89 (53) | 33 (19) | |
| Dawson et al., 2015 [55] | Observational prospective, 2 years | 29 | 10 (34) | 10 (35) | 4 (14) | |
| Solomon et al., 2015 [44] | Observational retrospective (1995–2013) | 137 | 87 (64) | 108 (79) | 54 (39) | |
| Dixon et al., 2010 [37] | Observational registry-based cohort study, 3.8 years | 14.113 | 10799 (76) | 160 (1.13) | ||
| Wolfe et al., 2007 [70] | Case/control prospective, 3.6 years | 17498 | 100 (27) | |||
| Kurata et al., 2019 [85] | Observational retrospective (2008–2017) | 49 | 14 (35) | 6 (12) | ||
| Chen et al., 2020 [43] | Observational retrospective (2008–2017) | 241 | 88 (36) | 66 (27) | 39 (16) | |
| Hyldgaard et al., 2017 [86] | Case/control prospective (2004–2015) | 679 | 26 (3.8) | |||
| Koduri et al., 2010 [38] | Prospective cohort study (1986–1998) | 52 | 19 (36) | 39 (75) | ||
| Tsuchiya et al., 2011 [63] | Observational retrospective (1996–2006) | 144 | 54 (37.5) | 7 (5) | 71 (49) | |
| Song et al., 2012 [87] | Observational prospective (2002–2011) | 51 | 21 (41) | |||
| Izuka et al., 2021 [58] | Observational retrospective (2007–2019) | 165 | 73 (44) | 70 (42) | 30 (18) | 13 (8) |
| Nurmi et al., 2017 [49] | Observational retrospective (2000–2014) | 59 | 30 (51) | 31 (52) | 24 (41) | 27 (46) |
| Oh et al., 2022 [50] | Observational retrospective (1999–2015) | 144 | 63 (44) | 53 (37) | 44 (30) | |
| Hozumi et al., 2022 [56] | Observational retrospective (2007–2019) | 58 | 39 (67) | 34 (59) | 43 (74) | |
| Cano-Jiménez et al., 2021 [54] | Observational retrospective (2013–2018) | 106 | 63 (60) | 55(61) | 53 (50) | 18 (17) |
| Jacob et al., 2018 [57] | Observational retrospective (1995–2015) | 90 | 65 (72) | |||
| Kelly et al., 2014 [88] | Observational retrospective (1987–2012) | 230 | 135 (59) | 103 (65) | 90 (57) | |
| Ng et al., 2022 [69] | Observational retrospective (1997–2013) | 214 | 48 (22) | |||
| Li et al., 2019 [52] | Observational retrospective (2008–2017) | 278 | 106 (38) | 91 (33) | 83 (29) | 53 (69) |
| Juge et al., 2023 [89] | Observational retrospective (2013–2018) | 4330 | ||||
| Brooks et al., 2022 [46] | Prospective cohort study, 2 years | 227 | 192 (85) | 147 (65) | 108 (47) | |
| Rojas-Serrano et al., 2022 [90] | Observational prospective | 37 | ||||
| Kim et al., 2020 [47] | Observational retrospective (1995–2018) | 84 | 37 (44) | 34 (40) | 33 (39) | |
| Lee et al., 2016 [74] | Retrospective cohort study | 62 | 62 (100) | |||
| Avouac et al.2020 [42] | Observational prospective study | 147 | 52 (35) | 21 (14) | 7 (4.7) | |
| Ito et al., 2017 [53] | Observational retrospective (2007–2016) | 65 | 16 (24) | |||
| Font et al., 2017 [64] | Longitudinal prospective (2007–2017) | 37 | 26(72) | 24(66) | 7 (19) | |
| Nieto et al., 2021 [65] | Longitudinal prospective (2005–2018) | 47 | 25 (54) | 26 (55) | 10 (21) | 16 (34) |
| Yang et al., 2019 [10] | Longitudinal prospective (1991–2011) | 77 | 4 (5) | 32 (48) | 27 (36) | |
| Mena-Vázquez et al., 2024 [36] | Observational prospective (2015–2023) | 148 | 13 (18) | 46 (66) | 21 (30) | 1 (1.4) |
| Kim et al., 2024 [73] | Observational retrospective (1995–2018) | 313 | 139 (45) | 202 (65) | 125 (40) | |
| Chen et al., 2022 [43] | Observational prospective, 5 years | 60 | 3 (16) | 19 (49) | 4 (7) | |
| Kelly et al., 2021 [88] | Observational retrospective (1990–2015) | 290 | 174 (60) | 200 (69) | 75 (28) | |
| Venerito et al., 2022 [62] | Observational retrospective (2021–2022) | 30 | 18 (60) | 13 (43) | ||
| Yamakawa et al., 2019 [91] | Observational retrospective (2012–2017) | 96 | 45 (47) | 21 (20) | 11 (11) | 25 (26) |
| Ekici et al., 2021 [66] | Observational retrospective (2010–2018) | 156 | 67 (42) | 74 (47) | 40 (26) | |
| Kakutani et al., 2020 [67] | Observational retrospective (2009–2014) | 261/2702 | 120 (46) | 120 (46) | 19 (7) | |
| Wang et al., 2019 [39] | Observational retrospective (2016–2019) | 96 | 9 (20) | 18 (40) | 25 (56) | 4 (9) |
| Tanaka et al., 2021 [71] | Observational retrospective (2010–2019) | 125 | 59 (50) | 32 (25) | 37 (29) | |
| Kwon et al., 2022 [75] | Observational retrospective (2016–2022) | 310 | 87 (28) | 89 (29) | ||
| Kang et al., 2020 [68] | Retrospective cohort (2006–2015) | 1999 | 759 (38) | 415 (21) | ||
| Farquhar et al., 2024 [59] | Observational retrospective (2006–2008, 2011–2013) | 100 | 64 (64) | 38 (43) | 68 (73) | 26 (26) |
| Marcoux et al., 2023 [79] | Observational prospective (2015–2018) | 181 | 112 (70) | 66 (73) | 39 (24) | |
| Tyker et al., 2021 [45] | Observational retrospective (2006–2019) | 70 | 45 (64) | 47 (67) | 29 (70) |
| Category | Potential Risk Factors | References | Effect Estimate |
|---|---|---|---|
| Demographic features | Age * | [6,43,58] | OR 0.55–2.91, AUC 0.74 |
| CDAI score * | [72] | OR 4.7 | |
| Laboratory findings | ACPA ** | [6] | HR 3.94 |
| KL-6 * | [40,41,42,71] | OR 1.00–72.7 | |
| MMP13 ** | [43] | AUC 0.71 | |
| CXCL11/I-TAC ** | [43] | AUC 0.67 | |
| MUC5B mutation ** | [6] | HR 2.30 | |
| Pulmonary function | FVC% pred ** | [51] | HR 3.42 |
| DLCO% pred ** | [51] | HR 1.72 | |
| Underlying radiological features | UIP pattern on HRCT * | [6,58] | OR 2.29–4.11 |
| Pre-treatment | Corticosteroid * | [51] | HR 15.0 |
| Nonbiologic DMARDs * | [40,58] | OR 1.75–.75 | |
| Biologic DMARDs ** | [16,68] | HR 0.44–2.33 |
| Category | Potential Risk Factors | References | Effect Estimate |
|---|---|---|---|
| Demographic features | Age ** | [9,37,38,44,48,49,50,57,58,60,65,69] | HR 1.04–4.8 |
| Male gender ** | [17,65,86] | HR 2.83–14.5 | |
| Female gender ** | [17] | HR 3.6 | |
| Smoking history ** | [44,60] | HR 2.58–3.17 | |
| Low socioeconomic status * | [38] | HR 2.07 | |
| The onset of ILD before RA onset | [17] | HR 8.4 | |
| Disease activity | DAS28 score ** | [37] | HR 1.21–1.43 |
| CDAI score * | [90] | HR 1.07 | |
| MDHAQ score ** | [46] | HR 1.85 | |
| Pain VAS * | [38] | HR 1.01 | |
| Patient global assessment ** | [46] | HR 1.16 | |
| Laboratory findings | RF * | [9,44,45] | HR 1.00–2.08 |
| ESR ** | [38,46,50] | HR 1.01–1.15 | |
| CRP ** | [46] | HR 1.12 (1.06–1.18) | |
| LDH * | [9] | HR 1.05 | |
| KL-6 ** | [47,74] | HR 1.00–3.23 | |
| IL-6 ** | [74] | HR 1.04 | |
| SP-D * | [48] | HR 1.0 | |
| Pulmonary function | DLCO % pred ** | [44,46,49,50] | HR 0.97–1.77 |
| FVC % pred ** | [44,46,47,50,53,56] | HR 0.97–4.43 | |
| TLCO % pred ** | [50] | HR 0.97 | |
| PaO2/FiO2 * | [56] | HR 0.94 | |
| Underlying radiological features | ILD extent ** | [9,16,57,59] | HR 1.03–4.47 |
| UIP ** | [10,44,47,50,58,73,79] | HR 2.44–5.84 | |
| Honeycombing * | [48] | HR 2.49 | |
| Radiomics * | [62] | HR 9.35 | |
| DAD * | [63] | HR 2.88 | |
| Emphysema * | [50,57] | HR 3.43–6.84 | |
| Comorbidities | COPD ** | [69] | HR 2.12 |
| Diabetes mellitus ** | [69] | HR 1.09 | |
| Pre-treatment | Corticosteroid ** | [69] | HR 1.09 |
| Nonbiologic DMARDs * | [9,58] | HR 0.16–5.53 | |
| Biologic DMARDs ** | [49] | HR 0.44–2.33 | |
| Acute exacerbations of ILD ** | [48] | HR 1.12–3.19 |
References
- Aletaha, D.; Smolen, J.S. Diagnosis and Management of Rheumatoid Arthritis: A Review. JAMA 2018, 320, 1360–1372. [Google Scholar] [CrossRef]
- Almutairi, K.; Nossent, J.; Preen, D.; Keen, H.; Inderjeeth, C. The global prevalence of rheumatoid arthritis: A meta-analysis based on a systematic review. Rheumatol. Int. 2021, 41, 863–877. [Google Scholar] [CrossRef]
- Kadura, S.; Raghu, G. Rheumatoid arthritis-interstitial lung disease: Manifestations and current concepts in pathogenesis and management. Eur. Respir. Rev. 2021, 30, 210011. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.; Kronzer, V.L.; Dellaripa, P.F.; Deane, K.D.; Bolster, M.B.; Nagaraja, V.; Khanna, D.; Doyle, T.J.; Sparks, J.A. Rheumatoid Arthritis–Associated Interstitial Lung Disease: Current Update on Prevalence, Risk Factors, and Pharmacologic Treatment. Curr. Treat. Options Rheumatol. 2020, 6, 337–353. [Google Scholar] [CrossRef]
- Fazeli, M.S.; Khaychuk, V.; Wittstock, K.; Han, X.; Crocket, G.; Lin, M.; Ferri, L. Rheumatoid Arthritis-Associated Interstitial Lung Disease: Epidemiology, Risk/Prognostic Factors, and Treatment Landscape. Clin. Exp. Rheumatol. 2021, 39, 1108–1118. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.F.; Wang, Y.Y.; Li, Z.Y.; He, P.J.; Liu, S.; Li, Q.S. The prevalence and risk factors of rheumatoid arthritis-associated interstitial lung disease: A systematic review and meta-analysis. Ann. Med. 2024, 56, 2332406. [Google Scholar] [CrossRef]
- Albrecht, K.; Strangfeld, A.; Marschall, U.; Callhoff, J. Interstitial lung disease in rheumatoid arthritis: Incidence, prevalence and related drug prescriptions between 2007 and 2020. RMD Open 2023, 9, e002777. [Google Scholar] [CrossRef]
- Laria, A.; Lurati, A.M.; Zizzo, G.; Zaccara, E.; Mazzocchi, D.; Re, K.A.; Marrazza, M.; Faggioli, P.; Mazzone, A. Interstitial Lung Disease in Rheumatoid Arthritis: A Practical Review. Front. Med. 2022, 9, 837133. [Google Scholar] [CrossRef]
- Lee, H.; Lee, S.I.; Kim, H.O. Recent Advances in Basic and Clinical Aspects of Rheumatoid Arthritis-associated Interstitial Lung Diseases. J. Rheum. Dis. 2022, 29, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Zhang, Z.; Zhang, X.; Zhang, X.; Zhi, K.; Zhao, X.; Zhao, J.; Cao, W. Rheumatoid arthritis-associated interstitial lung disease hotspots and future directions: A Web-of-Science based scientometric and visualization study. Immun. Inflamm. Dis. 2023, 11, e944. [Google Scholar] [CrossRef]
- Fischer, A.; Du Bois, R. Interstitial lung disease in connective tissue disorders. Lancet 2012, 380, 689–698. [Google Scholar] [CrossRef] [PubMed]
- Kolb, M.; Vašáková, M. The natural history of progressive fibrosing interstitial lung diseases. Respir. Res. 2019, 20, 57. [Google Scholar] [CrossRef] [PubMed]
- Duarte, C.; Ferreira, R.J.O.; Santos, E.J.F.; Da Silva, J.A.P. Treating-to-target in rheumatology: Theory and practice. Best. Pract. Res. Clin. Rheumatol. 2022, 36, 101735. [Google Scholar] [CrossRef]
- Challa, D.N.V.; Crowson, C.S.; Davis, J.M. The Patient Global Assessment of Disease Activity in Rheumatoid Arthritis: Identification of Underlying Latent Factors. Rheumatol. Ther. 2017, 4, 201–208. [Google Scholar] [CrossRef]
- du Bois, R.M.; Weycker, D.; Albera, C.; Bradford, W.Z.; Costabel, U.; Kartashov, A.; King, T.E., Jr. Ascertainment of Individual Risk of Mortality for Patients with Idiopathic Pulmonary Fibrosis. Am. J. Respir. Crit. Care Med. 2011, 184, 459–466. [Google Scholar] [CrossRef]
- Kelly, C.A.; Saravanan, V.; Nisar, M.; Arthanari, S.; Woodhead, F.A.; Price-Forbes, A.N.; Dawson, J.; Sathi, N.; Ahmad, Y.; Koduri, G.; et al. Rheumatoid arthritis-related interstitial lung disease: Associations, prognostic factors and physiological and radiological characteristics—A large multicentre UK study. Rheumatology 2014, 53, 1676–1682. [Google Scholar] [CrossRef] [PubMed]
- Juge, P.A.; Crestani, B.; Dieudé, P. Recent advances in rheumatoid arthritis-associated interstitial lung disease. Curr. Opin. Pulm. Med. 2020, 26, 477–486. [Google Scholar] [CrossRef]
- Akiyama, M.; Kaneko, Y. Pathogenesis, clinical features, and treatment strategy for rheumatoid arthritis-associated interstitial lung disease. Autoimmun. Rev. 2022, 21, 103056. [Google Scholar] [CrossRef]
- Dai, Y.; Wang, W.; Yu, Y.; Hu, S. Rheumatoid arthritis–associated interstitial lung disease: An overview of epidemiology, pathogenesis and management. Clin. Rheumatol. 2021, 40, 1211–1220. [Google Scholar] [CrossRef]
- Al-Baldawi, S.; Zúñiga Salazar, G.; Zúñiga, D.; Balasubramanian, S.; Mehmood, K.T. Interstitial Lung Disease in Rheumatoid Arthritis: A Review. 5 February 2024. Available online: https://www.cureus.com/articles/220746-interstitial-lung-disease-in-rheumatoid-arthritis-a-review (accessed on 8 August 2024).
- Xie, M.; Zhu, C.; Ye, Y. Incidence, risk factors, and prognosis of acute exacerbation of rheumatoid arthritis-associated interstitial lung disease: A systematic review and meta-analysis. BMC Pulm. Med. 2023, 23, 255. [Google Scholar] [CrossRef]
- Ley, B.; Ryerson, C.J.; Vittinghoff, E.; Ryu, J.H.; Tomassetti, S.; Lee, J.S.; Poletti, V.; Buccioli, M.; Elicker, B.M.; Jones, K.D.; et al. A Multidimensional Index and Staging System for Idiopathic Pulmonary Fibrosis. Ann. Intern. Med. 2012, 156, 684–691. [Google Scholar] [CrossRef]
- King, T.E., Jr.; Tooze, J.A.; Schwarz, M.I.; Brown, K.R.; Cherniack, R.M. Predicting Survival in Idiopathic Pulmonary Fibrosis: Scoring System and Survival Model. Am. J. Respir. Crit. Care Med. 2001, 164, 1171–1181. [Google Scholar] [CrossRef]
- Bendstrup, E.; Møller, J.; Kronborg-White, S.; Prior, T.S.; Hyldgaard, C. Interstitial Lung Disease in Rheumatoid Arthritis Remains a Challenge for Clinicians. J. Clin. Med. 2019, 8, 2038. [Google Scholar] [CrossRef] [PubMed]
- Otaola, M.; Paulin, F.; Rosemffet, M.; Balcazar, J.; Perandones, M.; Orausclio, P.; Cazenave, T.; Rossi, S.; Marciano, S.; Schneeberger, E.; et al. Lung ultrasound is a promising screening tool to rule out interstitial lung disease in patients with rheumatoid arthritis. Respirology 2024, 29, 588–595. [Google Scholar] [CrossRef] [PubMed]
- Bandinelli, F.; Benucci, M.; Mallia, I.; Mauro, I.; Pecani, N.; Li Gobbi, F.; Giannasi, G. Do Ultrasound Lung Abnormalities Correlate to Biomarkers and Male Gender in Rheumatoid Arthritis Patients? A Monocentric Cross-Sectional Study. J. Clin. Med. 2024, 13, 3534. [Google Scholar] [CrossRef] [PubMed]
- Matteson, E.L.; Kelly, C.; Distler, J.H.W.; Hoffmann-Vold, A.M.; Seibold, J.R.; Mittoo, S.; Dellaripa, P.F.; Aringer, M.; Pope, J.; Distler, O.; et al. Nintedanib in Patients with Autoimmune Disease–Related Progressive Fibrosing Interstitial Lung Diseases: Subgroup Analysis of the INBUILD Trial. Arthritis Rheumatol. 2022, 74, 1039–1047. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Arnett, F.C.; Edworthy, S.M.; Bloch, D.A.; Mcshane, D.J.; Fries, J.F.; Cooper, N.S.; Healey, L.A.; Kaplan, S.R.; Liang, M.H.; Luthra, H.S.; et al. The american rheumatism association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum. 1988, 31, 315–324. [Google Scholar] [CrossRef]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O., 3rd; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. 2010 Rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010, 62, 2569–2581. [Google Scholar] [CrossRef]
- American Thoracic Society; European Respiratory Society. American Thoracic Society/European Respiratory Society International Multidisciplinary Consensus Classification of the Idiopathic Interstitial Pneumonias. This Joint Statement of the American Thoracic Society (ATS), and the European Respiratory Society (ERS) Was Adopted by the ATS Board of Directors, June 2001 and by the ERS Executive Committee, June 2001. Am. J. Respir. Crit. Care Med. 2002, 165, 277–304. [Google Scholar]
- Travis, W.D.; Costabel, U.; Hansell, D.M.; King, T.E., Jr.; Lynch, D.A.; Nicholson, A.G.; Ryerson, C.J.; Ryu, J.H.; Selman, M.; Wells, A.U.; et al. An Official American Thoracic Society/European Respiratory Society Statement: Update of the International Multidisciplinary Classification of the Idiopathic Interstitial Pneumonias. Am. J. Respir. Crit. Care Med. 2013, 188, 733–748. [Google Scholar] [CrossRef] [PubMed]
- Flaherty, K.R.; Wells, A.U.; Cottin, V.; Devaraj, A.; Walsh, S.L.; Inoue, Y.; Brown, K.K. Nintedanib in Progressive Fibrosing Interstitial Lung Diseases. N. Engl. J. Med. 2019, 381, 1718–1727. [Google Scholar] [CrossRef] [PubMed]
- Clark, H.D.; Wells, G.A.; Huët, C.; McAlister, F.A.; Salmi, L.; Fergusson, D.; Laupacis, A. Assessing the Quality of Randomized Trials. Control Clin. Trials 1999, 20, 448–452. [Google Scholar] [CrossRef] [PubMed]
- Explanation of the 2011 OCEBM Levels of Evidence—Centre for Evidence-Based Medicine (CEBM), University of Oxford. Available online: https://www.cebm.ox.ac.uk/resources/levels-of-evidence/explanation-of-the-2011-ocebm-levels-of-evidence (accessed on 10 August 2024).
- Mena-Vázquez, N.; Redondo-Rodriguez, R.; Rojas-Gimenez, M.; Romero-Barco, C.M.; Fuego-Varela, C.; Perez-Gómez, N.; Añón-Oñate, I.; Castro Pérez, P.; García-Studer, A.; Hidalgo-Conde, A.; et al. Rate of severe and fatal infections in a cohort of patients with interstitial lung disease associated with rheumatoid arthritis: A multicenter prospective study. Front. Immunol. 2024, 15, 1341321. [Google Scholar] [CrossRef] [PubMed]
- Dixon, W.G.; Hyrich, K.L.; Watson, K.D.; Lunt, M.; BSRBR Control Centre Consortium; Symmons DPM. Influence of anti-TNF therapy on mortality in patients with rheumatoid arthritis-associated interstitial lung disease: Results from the British Society for Rheumatology Biologics Register. Ann. Rheum. Dis. 2010, 69, 1086–1091. [Google Scholar] [CrossRef]
- Koduri, G.; Norton, S.; Young, A.; Cox, N.; Davies, P.; Devlin, J.; Dixey, J.; Gough, A.; Prouse, P.; Winfield, J.; et al. Interstitial lung disease has a poor prognosis in rheumatoid arthritis: Results from an inception cohort. Rheumatology 2010, 49, 1483–1489. [Google Scholar] [CrossRef]
- Wang, Y.; Chen, S.; Zheng, S.; Lin, J.; Hu, S.; Zhuang, J.; Lin, Q.; Xie, X.; Zheng, K.; Zhang, W.; et al. The role of lung ultrasound B-lines and serum KL-6 in the screening and follow-up of rheumatoid arthritis patients for an identification of interstitial lung disease: Review of the literature, proposal for a preliminary algorithm, and clinical application to cases. Arthritis Res. Ther. 2021, 23, 212. [Google Scholar]
- Mochizuki, T.; Ikari, K.; Yano, K.; Sato, M.; Okazaki, K. Long-term deterioration of interstitial lung disease in patients with rheumatoid arthritis treated with abatacept. Mod. Rheumatol. 2019, 29, 413–417. [Google Scholar] [CrossRef]
- Fotoh, D.S.; Helal, A.; Rizk, M.S.; Esaily, H.A. Serum Krebs von den Lungen-6 and lung ultrasound B lines as potential diagnostic and prognostic factors for rheumatoid arthritis–associated interstitial lung disease. Clin. Rheumatol. 2021, 40, 2689–2697. [Google Scholar] [CrossRef]
- Avouac, J.; Cauvet, A.; Steelandt, A.; Shirai, Y.; Elhai, M.; Kuwana, M.; Distler, O.; Allanore, Y. Improving risk-stratification of rheumatoid arthritis patients for interstitial lung disease. PLoS ONE 2020, 15, e0232978. [Google Scholar] [CrossRef]
- Chen, J.; Chen, Y.; Liu, D.; Lin, Y.; Zhu, L.; Song, S.; Hu, Y.; Liang, T.; Liu, Y.; Liu, W.; et al. Predictors of long-term prognosis in rheumatoid arthritis-related interstitial lung disease. Sci. Rep. 2022, 12, 9469. [Google Scholar] [CrossRef] [PubMed]
- Solomon, J.J.; Chung, J.H.; Cosgrove, G.P.; Demoruelle, M.K.; Fernandez-Perez, E.R.; Fischer, A.; Frankel, S.K.; Hobbs, S.B.; Huie, T.J.; Ketzer, J.; et al. Predictors of mortality in rheumatoid arthritis-associated interstitial lung disease. Eur. Respir. J. 2016, 47, 588–596. [Google Scholar] [CrossRef] [PubMed]
- Tyker, A.; Ventura, I.B.; Lee, C.T.; Strykowski, R.; Garcia, N.; Guzy, R.; Jablonski, R.; Vij, R.; Strek, M.E.; Chung, J.H.; et al. High-titer rheumatoid factor seropositivity predicts mediastinal lymphadenopathy and mortality in rheumatoid arthritis-related interstitial lung disease. Sci. Rep. 2021, 11, 22821. [Google Scholar] [CrossRef] [PubMed]
- Brooks, R.; Baker, J.F.; Yang, Y.; Roul, P.; Kerr, G.S.; Reimold, A.M.; Kunkel, G.; Wysham, K.D.; Singh, N.; Lazaro, D.; et al. The impact of disease severity measures on survival in U.S. veterans with rheumatoid arthritis-associated interstitial lung disease. Rheumatology 2022, 61, 4667–4677. [Google Scholar] [CrossRef]
- Kim, H.C.; Choi, K.H.; Jacob, J.; Song, J.W. Prognostic role of blood KL-6 in rheumatoid arthritis–associated interstitial lung disease. PLoS ONE 2020, 15, e0229997. [Google Scholar] [CrossRef]
- Yamakawa, H.; Sato, S.; Tsumiyama, E.; Nishizawa, T.; Kawabe, R.; Oba, T.; Kamikawa, T.; Horikoshi, M.; Akasaka, K.; Amano, M.; et al. Predictive factors of mortality in rheumatoid arthritis-associated interstitial lung disease analysed by modified HRCT classification of idiopathic pulmonary fibrosis according to the 2018 ATS/ERS/JRS/ALAT criteria. J. Thorac. Dis. 2019, 11, 5247–5257. [Google Scholar] [CrossRef]
- Nurmi, H.M.; Purokivi, M.K.; Kärkkäinen, M.S.; Kettunen, H.P.; Selander, T.A.; Kaarteenaho, R.L. Are risk predicting models useful for estimating survival of patients with rheumatoid arthritis-associated interstitial lung disease? BMC Pulm. Med. 2017, 17, 16. [Google Scholar] [CrossRef]
- Oh, J.H.; Kim, G.H.J.; Cross, G.; Barnett, J.; Jacob, J.; Hong, S.; Song, J.W. Automated quantification system predicts survival in rheumatoid arthritis-associated interstitial lung disease. Rheumatology 2022, 61, 4702–4710. [Google Scholar] [CrossRef]
- Zamora-Legoff, J.A.; Krause, M.L.; Crowson, C.S.; Ryu, J.H.; Matteson, E.L. Progressive Decline of Lung Function in Rheumatoid Arthritis–Associated Interstitial Lung Disease. Arthritis Rheumatol. 2017, 69, 542–549. [Google Scholar] [CrossRef]
- Li, L.; Liu, R.; Zhang, Y.; Zhou, J.; Li, Y.; Xu, Y.; Gao, S.; Zheng, Y. A retrospective study on the predictive implications of clinical characteristics and therapeutic management in patients with rheumatoid arthritis-associated interstitial lung disease. Clin. Rheumatol. 2020, 39, 1457–1470. [Google Scholar] [CrossRef]
- Ito, Y.; Arita, M.; Kumagai, S.; Takei, R.; Noyama, M.; Tokioka, F.; Nishimura, K.; Koyama, T.; Ishida, T. Male Gender and Fibrosis Score on High-Resolution Computed Tomography are Independent Poor Prognostic Factors of Survival in Patients with Rheumatoid Arthritis-Related Interstitial Lung Disease. In Diffuse Parenchymal Lung Disease; European Respiratory Society: Lausanne, Switzerland, 2017; p. PA887. Available online: http://erj.ersjournals.com/lookup/doi/10.1183/1393003.congress-2017.PA887 (accessed on 13 July 2024).
- Cano-Jiménez, E.; Rodríguez, T.V.; Martín-Robles, I.; Villegas, D.C.; García, J.J.; de Miguel, E.B.; Robles-Pérez, A.; Galván, M.F.; Roibas, C.M.; Lara, S.H.; et al. Diagnostic delay of associated interstitial lung disease increases mortality in rheumatoid arthritis. Sci. Rep. 2021, 11, 9184. [Google Scholar] [CrossRef]
- Dawson, J.K. Predictors of progression of HRCT diagnosed fibrosing alveolitis in patients with rheumatoid arthritis. Ann. Rheum. Dis. 2002, 61, 517–521. [Google Scholar] [CrossRef] [PubMed]
- Hozumi, H.; Kono, M.; Hasegawa, H.; Kato, S.; Inoue, Y.; Suzuki, Y.; Karayama, M.; Furuhashi, K.; Enomoto, N.; Fujisawa, T.; et al. Acute Exacerbation of Rheumatoid Arthritis-Associated Interstitial Lung Disease: Mortality and Its Prediction Model. Respir. Res. 2022, 23, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Jacob, J.; Hirani, N.; van Moorsel, C.H.M.; Rajagopalan, S.; Murchison, J.T.; van Es, H.W.; Bartholmai, B.J.; van Beek, F.T.; Struik, M.H.L.; Stewart, G.A.; et al. Predicting outcomes in rheumatoid arthritis related interstitial lung disease. Eur. Respir. J. 2019, 53, 1800869. [Google Scholar] [CrossRef] [PubMed]
- Izuka, S.; Yamashita, H.; Iba, A.; Takahashi, Y.; Kaneko, H. Acute exacerbation of rheumatoid arthritis–associated interstitial lung disease: Clinical features and prognosis. Rheumatology 2021, 60, 2348–2354. [Google Scholar] [CrossRef] [PubMed]
- Farquhar, H.J.; Beckert, N.; Beckert, L.; Edwards, A.L.; Matteson, E.L.; Frampton, C.; Stamp, L.K. Survival of adults with rheumatoid arthritis associated interstitial lung disease—A systematic review and meta-analysis. Semin. Arthritis Rheum. 2023, 60, 152187. [Google Scholar] [CrossRef]
- Kim, E.J.; Elicker, B.M.; Maldonado, F.; Webb, W.R.; Ryu, J.H.; Van Uden, J.H.; Lee, J.S.; King, T.E., Jr.; Collard, H.R. Usual interstitial pneumonia in rheumatoid arthritis-associated interstitial lung disease. Eur. Respir. J. 2010, 35, 1322–1328. [Google Scholar] [CrossRef]
- Cassone, G.; Manfredi, A.; Vacchi, C.; Luppi, F.; Coppi, F.; Salvarani, C.; Sebastiani, M. Treatment of Rheumatoid Arthritis-Associated Interstitial Lung Disease: Lights and Shadows. J. Clin. Med. 2020, 9, 1082. [Google Scholar] [CrossRef]
- Venerito, V.; Manfredi, A.; Carletto, A.; Gentileschi, S.; Atzeni, F.; Guiducci, S.; Lavista, M.; La Corte, L.; Pedrollo, E.; Scardapane, A.; et al. Evolution of Rheumatoid-Arthritis-Associated Interstitial Lung Disease in Patients Treated with JAK Inhibitors: A Retrospective Exploratory Study. J. Clin. Med. 2023, 12, 957. [Google Scholar] [CrossRef]
- Tsuchiya, Y.; Takayanagi, N.; Sugiura, H.; Miyahara, Y.; Tokunaga, D.; Kawabata, Y.; Sugita, Y. Lung diseases directly associated with rheumatoid arthritis and their relationship to outcome. Eur. Respir. J. 2011, 37, 1411–1417. [Google Scholar] [CrossRef]
- Mortality and Clinical Features in Rheumatoid Arthritis and Interstitial Lung Disease-ACR Meeting Abstracts. Available online: https://acrabstracts.org/abstract/mortality-and-clinical-features-in-rheumatoid-arthritis-and-interstitial-lung-disease/ (accessed on 15 July 2024).
- Nieto, M.A.; Sanchez-Pernaute, O.; Romero-Bueno, F.; Leon, L.; Vadillo, C.; Freites-Nuñez, D.D.; Jover, J.A.; Álvarez-Sala, J.L.; Abasolo, L. Mortality rate in rheumatoid arthritis-related interstitial lung disease: The role of radiographic patterns. BMC Pulm. Med. 2021, 21, 205. [Google Scholar] [CrossRef] [PubMed]
- Ekici, M.; Baytar, Y.; Kardas, R.C.; Sari, A.; Akdogan, A.; Durhan, G.; Ariyurek, M.; Kalyoncu, U. Predictors of mortality in rheumatoid arthritis-associated lung disease: A retrospective study on ten years. Jt. Bone Spine 2021, 88, 105133. [Google Scholar] [CrossRef]
- Kakutani, T.; Hashimoto, A.; Tominaga, A.; Kodama, K.; Nogi, S.; Tsuno, H.; Ogihara, H.; Nunokawa, T.; Komiya, A.; Furukawa, H.; et al. Related factors, increased mortality and causes of death in patients with rheumatoid arthritis-associated interstitial lung disease. Mod. Rheumatol. 2020, 30, 458–464. [Google Scholar] [CrossRef]
- Kang, E.H.; Jin, Y.; Desai, R.J.; Liu, J.; Sparks, J.A.; Kim, S.C. Risk of exacerbation of pulmonary comorbidities in patients with rheumatoid arthritis after initiation of abatacept versus TNF inhibitors: A cohort study. Semin. Arthritis Rheum. 2020, 50, 401–408. [Google Scholar] [CrossRef]
- Ng, K.H.; Chen, D.Y.; Lin, C.H.; Chao, W.C.; Chen, H.H. Analysis of risk factors of mortality in rheumatoid arthritis patients with interstitial lung disease: A nationwide, population-based cohort study in Taiwan. RMD Open 2022, 8, e002343. [Google Scholar] [CrossRef]
- Wolfe, F.; Caplan, L.; Michaud, K. Rheumatoid arthritis treatment and the risk of severe interstitial lung disease. Scand. J. Rheumatol. 2007, 36, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, N.; Nishimura, K.; Waki, D.; Kadoba, K.; Murabe, H.; Yokota, T. Annual variation rate of KL-6 for predicting acute exacerbation in patients with rheumatoid arthritis-associated interstitial lung disease. Mod. Rheumatol. 2021, 31, 1100–1106. [Google Scholar] [CrossRef] [PubMed]
- Akiyama, M.; Kaneko, Y.; Yamaoka, K.; Kondo, H.; Takeuchi, T. Association of disease activity with acute exacerbation of interstitial lung disease during tocilizumab treatment in patients with rheumatoid arthritis: A retrospective, case–control study. Rheumatol. Int. 2016, 36, 881–889. [Google Scholar] [CrossRef]
- Kim, S.H.; Kim, S.Y.; Yoon, H.Y.; Song, J.W. PM10 increases mortality risk in rheumatoid arthritis-associated interstitial lung disease. RMD Open 2024, 10, e003680. [Google Scholar] [CrossRef]
- Lee, J.S.; Lee, E.Y.; Ha, Y.J.; Kang, E.H.; Lee, Y.J.; Song, Y.W. Serum KL-6 levels reflect the severity of interstitial lung disease associated with connective tissue disease. Arthritis Res. Ther. 2019, 21, 58. [Google Scholar] [CrossRef]
- Kwon, B.S.; Lee, H.Y.; Choe, J.; Chae, E.J.; Hong, S.; Song, J.W. Acute Respiratory Deterioration in Rheumatoid Arthritis-Associated Interstitial Lung Disease. Chest 2022, 162, 136–144. [Google Scholar] [CrossRef] [PubMed]
- Habib, H.M.; Eisa, A.A.; Arafat, W.R.; Marie, M.A. Pulmonary involvement in early rheumatoid arthritis patients. Clin. Rheumatol. 2011, 30, 217–221. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.H.; Lee, J.S.; Ha, Y.-J.; Kim, M.U.; Park, C.H.; Lee, J.S.; Kim, J.-W.; Chung, S.W.; Pyo, J.Y.; Lee, S.W.; et al. Lung function trajectory of rheumatoid arthritis–associated interstitial lung disease. Rheumatology 2023, 62, 3014–3024. [Google Scholar] [CrossRef] [PubMed]
- Courvoisier, D.S.; Chatzidionysiou, K.; Mongin, D.; Lauper, K.; Mariette, X.; Morel, J.; Gottenberg, J.-E.; Bergstra, S.A.; Suarez, M.P.; Codreanu, C.; et al. The impact of seropositivity on the effectiveness of biologic anti-rheumatic agents: Results from a collaboration of 16 registries. Rheumatology 2021, 60, 820–828. [Google Scholar] [CrossRef]
- Marcoux, V.; Lok, S.; Mondal, P.; Assayag, D.; Fisher, J.H.; Shapera, S.; Morisset, J.; Manganas, H.; Fell, C.D.; Hambly, N.; et al. Treatment of Rheumatoid Arthritis-Associated Interstitial Lung Disease in A Multi-Center Registry Cohort. J. Thorac. Dis. 2023, 15, 2517. [Google Scholar] [CrossRef]
- Matson, S.M.; Baqir, M.; Moua, T.; Marll, M.; Kent, J.; Iannazzo, N.S.; Boente, R.D.; Donatelli, J.M.; Dai, J.; Diaz, F.J.; et al. Treatment Outcomes for Rheumatoid Arthritis-Associated Interstitial Lung Disease. Chest 2023, 163, 861–869. [Google Scholar] [CrossRef]
- Pugashetti, J.V.; Adegunsoye, A.; Wu, Z.; Lee, C.T.; Srikrishnan, A.; Ghodrati, S.; Vo, V.; Renzoni, E.A.; Wells, A.U.; Garcia, C.K.; et al. Validation of Proposed Criteria for Progressive Pulmonary Fibrosis. Am. J. Respir. Crit. Care Med. 2023, 207, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Singh, N.; Varghese, J.; England, B.R.; Solomon, J.J.; Michaud, K.; Mikuls, T.R.; Healy, H.S.; Kimpston, E.M.; Schweizer, M.L. Impact of the pattern of interstitial lung disease on mortality in rheumatoid arthritis: A systematic literature review and meta-analysis. Semin. Arthritis Rheum. 2019, 49, 358–365. [Google Scholar] [CrossRef]
- Franzen, D.; Ciurea, A.; Bratton, D.J.; Clarenbach, C.F.; Latshang, T.D.; Russi, E.W.; Kyburz, D.; Kohler, M. Effect of rituximab on pulmonary function in patients with rheumatoid arthritis. Pulm. Pharmacol. Ther. 2016, 37, 24–29. [Google Scholar] [CrossRef]
- Yusof, Y.M.; Kabia, A.; Darby, M.; Lettieri, G.; Beirne, P.; Vital, E.M.; Dass, S.; Emery, P. Effect of rituximab on the progression of rheumatoid arthritis–related interstitial lung disease: 10 years’ experience at a single centre. Rheumatology 2017, 56, 1348–1357. [Google Scholar] [CrossRef]
- Kurata, I.; Tsuboi, H.; Terasaki, M.; Shimizu, M.; Toko, H.; Honda, F.; Ohyama, A.; Yagishita, M.; Osada, A.; Ebe, H.; et al. Effect of Biological Disease-modifying Anti-rheumatic Drugs on Airway and Interstitial Lung Disease in Patients with Rheumatoid Arthritis. Intern. Med. 2019, 58, 1703–1712. [Google Scholar] [CrossRef]
- Hyldgaard, C.; Hilberg, O.; Pedersen, A.B.; Ulrichsen, S.P.; Løkke, A.; Bendstrup, E.; Ellingsen, T. A population-based cohort study of rheumatoid arthritis-associated interstitial lung disease: Comorbidity and mortality. Ann. Rheum. Dis. 2017, 76, 1700–1706. [Google Scholar] [CrossRef] [PubMed]
- Song, J.W.; Lee, H.K.; Lee, C.K.; Chae, E.J.; Jang, S.J.; Colby, T.V.; Kim, D.S. Clinical Course and Outcome of Rheumatoid Arthritis-Related Usual Interstitial Pneumonia. Sarcoidosis Vasc. Diffuse. Lung Dis. 2013, 30, 103–112. [Google Scholar]
- Kelly, C.A.; Nisar, M.; Arthanari, S.; Carty, S.; Woodhead, F.A.; Price-Forbes, A.; Middleton, D.; Dempsey, O.; Miller, D.; Basu, N.; et al. Rheumatoid arthritis related interstitial lung disease—Improving outcomes over 25 years: A large multicentre UK study. Rheumatology 2021, 60, 1882–1890. [Google Scholar] [CrossRef] [PubMed]
- Juge, P.A.; Hayashi, K.; McDermott, G.C.; Vanni, K.M.M.; Kowalski, E.; Qian, G.; Bade, K.; Saavedra, A.; Dieudé, P.; Dellaripa, P.F.; et al. Effectiveness and tolerability of antifibrotics in rheumatoid arthritis-associated interstitial lung disease. Semin. Arthritis Rheum. 2024, 64, 152312. [Google Scholar] [CrossRef] [PubMed]
- Rojas-Serrano, J.; Herrera-Bringas, D.; Pérez-Román, D.I.; Pérez-Dorame, R.; Mateos-Toledo, H.; Mejía, M. Rheumatoid arthritis-related interstitial lung disease (RA-ILD): Methotrexate and the severity of lung disease are associated to prognosis. Clin. Rheumatol. 2017, 36, 1493–1500. [Google Scholar] [CrossRef] [PubMed]
- Yamakawa, H.; Ogura, T.; Kameda, H.; Kishaba, T.; Iwasawa, T.; Takemura, T.; Kuwano, K. Decision-Making Strategy for the Treatment of Rheumatoid Arthritis-Associated Interstitial Lung Disease (RA-ILD). J. Clin. Med. 2021, 10, 3806. [Google Scholar] [CrossRef]
| Potential Risk Factors | Study | Effect Estimate |
|---|---|---|
| Age at ILD diagnosis ** | 44, 70 | HR 2.18; OR 1.7 |
| Male gender ** | 70 | OR 2.2 |
| Smoking history *** | 37, 70 | OR 1.7–6.13 |
| DAS28 *** | 37 | OR 1.71 |
| Arthritis onset ** | 44 | HR 1.87 |
| KL-6 ** | 74 | HR 3.37 |
| DLCO ** | 53 | OR 3.02 |
| UIP pattern ** | 53 | OR 3.47 |
| Combined pulmonary fibrosis and emphysema ** | 59 | OR 6.12 |
| Preexisting rheumatic airway disease ** | 95 | OR 7.40 |
| Prognostic Factor | References | Effect Estimate |
|---|---|---|
| Age ** | [10,38,43,44,48,50,52,54,65,67] | HR 1.04–5.02 |
| Male gender ** | [70] | OR 2.5–18.13 |
| Female gender ** | [53] | HR 6.8 |
| Smoking history * | [67] | HR 1.06–3.89 |
| Disease duration of RA ** | [50] | HR 1.3 |
| ESR ** | [44] | HR 5.35 |
| HAQ disability ** | [70] | OR 2.3 |
| Steinbrocker class 3 or 4 ** | [67] | HR 2.1 |
| FVC% pred * | [44] | HR 2.52 |
| DLCO *** | [49,54] | HR 0.85–0.97 |
| TLCO ** | [55] | HR 0.98 |
| Final oxygen saturation in the 6MWT ** | [54] | HR 0.62 |
| UIP pattern ** | [43,60,65,66,67] | HR 2.3–10.3 |
| Non-UIP pattern ** | [67] | HR 4.9 |
| ILD extent *** | [52,53] | HR 2.40–9.01 |
| Radiological honeycombing ** | [48] | HR 3.69 |
| Combined pulmonary fibrosis and emphysema ** | [57] | HR 2.16 |
| Pleural effusion ** | [66] | HR 14.4 |
| Corticosteroid * | [70] | HR 2.5 |
| Immunosuppressive agents ** | [70] | HR 3.0 |
| Withdrawal of MTX or LFN after ILD diagnosis ** | [54] | HR 2.18 |
| Diagnostic delay of ILD ** | [54] | HR 1.11 |
| PM10 * | [73] | HR 1.67 |
| History of acute ILD exacerbations *** | [48,75] | HR 2.42–6.48 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Groseanu, L.; Niță, C. A Systematic Review of the Key Predictors of Progression and Mortality of Rheumatoid Arthritis-Associated Interstitial Lung Disease. Diagnostics 2024, 14, 1890. https://doi.org/10.3390/diagnostics14171890
Groseanu L, Niță C. A Systematic Review of the Key Predictors of Progression and Mortality of Rheumatoid Arthritis-Associated Interstitial Lung Disease. Diagnostics. 2024; 14(17):1890. https://doi.org/10.3390/diagnostics14171890
Chicago/Turabian StyleGroseanu, Laura, and Cristina Niță. 2024. "A Systematic Review of the Key Predictors of Progression and Mortality of Rheumatoid Arthritis-Associated Interstitial Lung Disease" Diagnostics 14, no. 17: 1890. https://doi.org/10.3390/diagnostics14171890
APA StyleGroseanu, L., & Niță, C. (2024). A Systematic Review of the Key Predictors of Progression and Mortality of Rheumatoid Arthritis-Associated Interstitial Lung Disease. Diagnostics, 14(17), 1890. https://doi.org/10.3390/diagnostics14171890