
Radial Artery Spasm—A Review on Incidence, Prevention and Treatment

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Incidence and Risk Factors

{kind=link}
{kind=link}
{kind=link}
| Authors | Enrollment | Criteria for RAS Diagnosis | RAS Incidence (%) |
|---|---|---|---|
| Aminian et al. [40] | 1307 | Clinical | 4 |
| Aminian et al. [41] | 114 | Clinical | 4.4 |
| Aminian et al. [42] | 1926 | Clinical | 5 |
| Astarcioglu et al. [43] | 150 | Angiographic | 26.6 |
| Beyer et al. [44] | 86 | Clinical | 25 |
| Bochenek et al. [33] | 293 | Clinical | 18.8 |
| Bouchahda et al. [45] | 1523 | Clinical | 20 |
| Byrne et al. [46] | 86 | Clinical | 12.9 |
| Candemir et al. [47] | 63 | Clinical | 16 |
| Caussin et al. [36] | 351 | Clinical | 11.1 |
| Chen et al. [48] | 406 | Angiographic | 7.3 |
| Collet et al. [49] | 220 | Angiographic | 9 |
| Coppola et al. [50] | 379 | Clinical | 11.6 |
| Coroleu et al. [51] | 736 | Clinical | 14.8 |
| Costa-Mateu et al. [52] | 1953 | Clinical | 9 |
| Curtis et al. [29] | 169 | Angiographic | 14.2 |
| Dahm et al. [53] | 171 | Clinical | 2.9 |
| Deftereos et al. [54] | 172 | Clinical | 7.6 |
| Deftereos et al. [27] | 2013 | Angiographic | 5.4 |
| Dharma et al. [55] | 150 | Clinical | 6 |
| Ercan et al. [28] | 81 | Clinical | 19.1 |
| Ezhumalai et al. [56] | 200 | Clinical | 4.5 |
| Filho et al. [57] | 50 | Clinical | 2.1 |
| Giannopoulos et al. [31] | 1582 | Clinical | 9.3 |
| Gorgulus et al. [19] | 1722 | Angiographic | 10.3 |
| Goldsmit et al. [32] | 1868 | Clinical | 2.7 |
| Gopalakrishnan et al. [10] | 100 | Clinical | 23 |
| Gul et al. [58] | 200 | Clinical | 6.5 |
| Hatem et al. [38] | 394 | Angiographic | 18.5 |
| van der Heijden et al. [59] | 165 | Clinical | 16 |
| Hildick-Smith et al. [60] | 500 | Clinical | 12 |
| Hizoh et al. [61] | 591 | Clinical | 1.4 |
| Horie et al. [62] | 600 | Clinical | 1.5 |
| Jia et al. [20] | 1427 | Clinical | 7.8 |
| Khan et al. [63] | 136 | Clinical | 13.2 |
| Kiani et al. [64] | 144 | Clinical | 2.7 |
| Kiemeneij et al. [23] | 100 | Automated Pullback Device | 15 |
| Kiemeneij et al. [24] | 50 | Automated Pullback Device | 8 |
| Kim et al. [65] | 150 | Angiographic | 51.3 |
| Kocayiğit et al. [39] | 155 | Clinical | 10.1 |
| Koga et al. [66] | 234 | Clinical | 7 |
| Livesay et al. [67] | 203 | Clinical | 1.4 |
| Mikaeili Mirak et al. [68] | 60 | Clinical | 0 * |
| Numasawa et al. [22] | 744 | Angiographic | 11.2 |
| Ouadhour et al. [69] | 84 | Clinical | 5.9 |
| Rathore et al. [70] | 790 | Clinical | 29.4 |
| Rosencher et al. [25] | 731 | Clinical | 20.1 |
| Ruiz-Salmeron et al. [71] | 500 | Clinical | 18.2 |
| Ruiz-Salmeron et al. [18] | 637 | Clinical | 20.2 |
| Saito et al. [72] | 73 | Clinical | 6.8 |
| da Silva et al. [8] | 2040 | Clinical | 12.1 |
| Tatlı et al. [73] | 104 | Clinical | 18.2 |
| Tebaldi et al. [74] | 418 | Angiographic | 30 |
| Toprak et al. [35] | 1713 | Clinical | 9.6 |
| Turan et al. [75] | 101 | Clinical | 22 |
| Varenne et al. [76] | 1219 | Clinical | 10.7 |
| Yazdi et al. [77] | 120 | Clinical | 15 |
| Youn et al. [21] | 76 | Clinical and angiographic | 18.4 |
| Zencirci et al. [34] | 115 | Clinical | 16.5 |
| Zencirci et al. [78] | 222 | Clinical | 10.8 |
| Category | Risk Factor |
|---|---|
| Patient General Characteristics | Female sex |
| Younger age | |
| Older age Small body size Anxiety Rapid baseline heart rate Hypertension Diabetes mellitus Dyslipidemia Smoking Peripheral artery disease | |
| Patient Local Characteristics | Small radial artery size |
| Low radial pulse intensity Anatomical variations of radial artery Dominant hand (higher RAS and RAO) | |
| Procedural Characteristics | Emergency procedure |
| Multiple access attempts | |
| Multiple catheters used | |
| Large sheaths and catheters Long procedures | |
| Novel Predictors | Low heart rate variability (HRV) |
| Low asymmetric dimethylarginine ADMA levels |
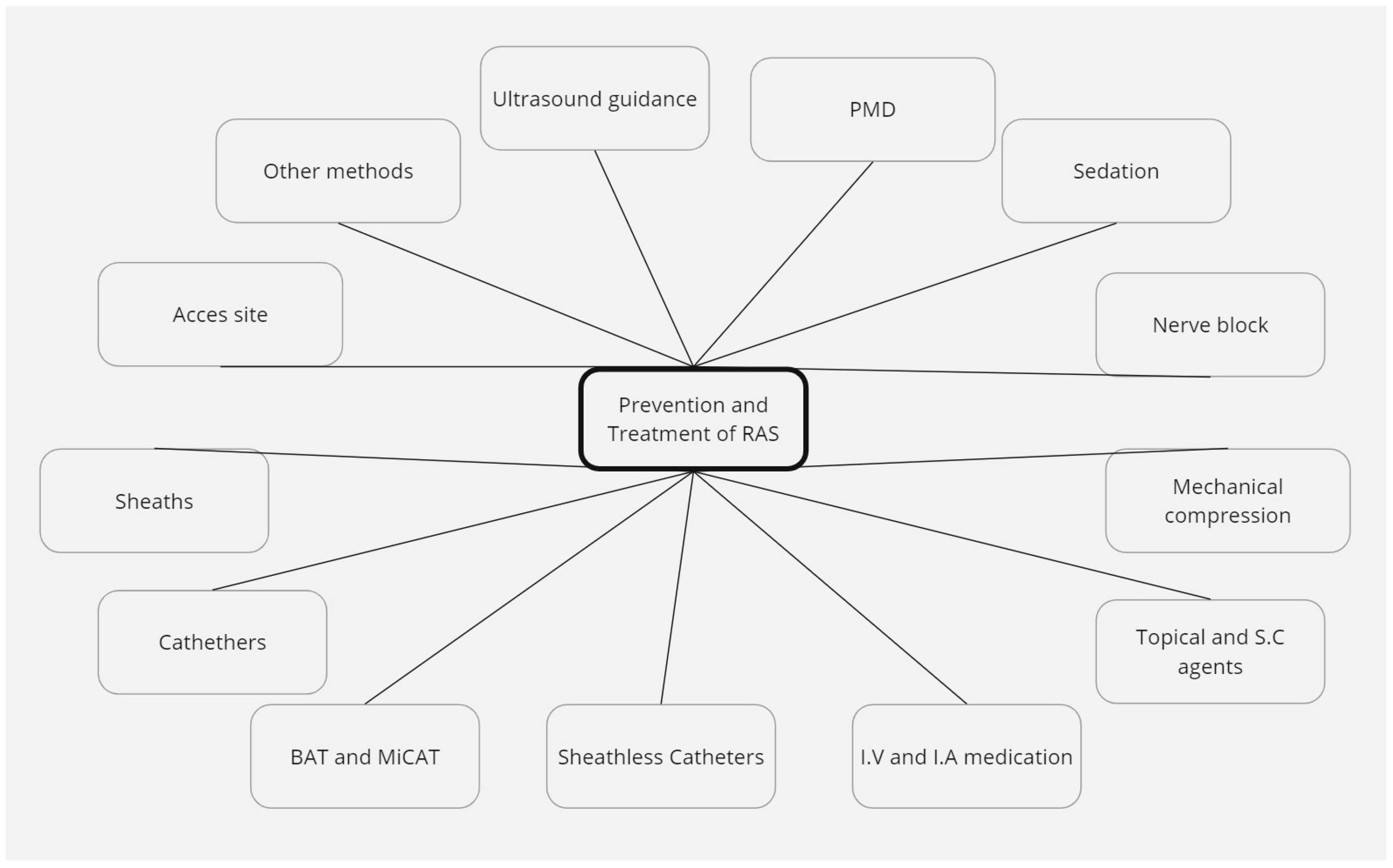
3.2. Prevention and Treatment Methods
3.2.1. Access Site
3.2.2. Sheaths
3.2.3. Catheters
3.2.4. Balloon-Assisted Tracking (BAT) and Microcatheter-Assisted Tracking (MiCAT)
3.2.5. Sheathless Catheters
3.2.6. Intravenous and Intraarterial Medication
3.2.7. Topical and Subcutaneous Agents
3.2.8. Mechanical Compression
3.2.9. Nerve Block
3.2.10. Pressure-Mediated Dilation (PMD)
3.2.11. Sedation
3.2.12. Ultrasound Guidance
3.2.13. Other Methods
3.3. Other Reviews and Guidelines Recommendations
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Conflicts of Interest
References
- Sandoval, Y.; Bell, M.R.; Gulati, R. Transradial Artery Access Complications. Circ. Cardiovasc. Interv. 2019, 12, e007386. [Google Scholar] [CrossRef] [PubMed]
- Roy, S.; Kabach, M.; Patel, D.B.; Guzman, L.A.; Jovin, I.S. Radial Artery Access Complications: Prevention, Diagnosis and Management. Cardiovasc. Revasc. Med. 2022, 40, 163–171. [Google Scholar] [CrossRef]
- Valgimigli, M.; Frigoli, E.; Leonardi, S.; Vranckx, P.; Rothenbühler, M.; Tebaldi, M.; Varbella, F.; Calabrò, P.; Garducci, S.; Rubartelli, P.; et al. Radial versus femoral access and bivalirudin versus unfractionated heparin in invasively managed patients with acute coronary syndrome (MATRIX): Final 1-year results of a multicentre, randomised controlled trial. Lancet 2018, 392, 835–848. [Google Scholar] [CrossRef] [PubMed]
- Jolly, S.S.; Yusuf, S.; Cairns, J.; Niemelä, K.; Xavier, D.; Widimsky, P.; Budaj, A.; Niemelä, M.; Valentin, V.; Lewis, B.S.; et al. Radial versus femoral access for coronary angiography and intervention in patients with acute coronary syndromes (RIVAL): A randomised, parallel group, multicentre trial. Lancet 2011, 377, 1409–1420, Erratum in Lancet 2011, 377, 1408; Erratum in Lancet 2011, 378, 30. [Google Scholar] [CrossRef] [PubMed]
- Kwok, C.S.; Khan, M.A.; Rao, S.V.; Kinnaird, T.; Sperrin, M.; Buchan, I.; de Belder, M.A.; Ludman, P.F.; Nolan, J.; Loke, Y.K.; et al. Access and Non–Access Site Bleeding After Percutaneous Coronary Intervention and Risk of Subsequent Mortality and Major Adverse Cardiovascular Events. Circ. Cardiovasc. Interv. 2015, 8, e001645. [Google Scholar] [CrossRef] [PubMed]
- Crişan, S.; Petriş, A.O.; Petrescu, L.; Luca, C.T. Current Perspectives in Facilitated Angioplasty. Am. J. Ther. 2019, 26, e208–e212. [Google Scholar] [CrossRef]
- Lee, P.; Liew, D.; Brennan, A.; Stub, D.; Lefkovits, J.; Reid, C.M.; Zomer, E. Cost-effectiveness of Radial Access Percutaneous Coronary Intervention in Acute Coronary Syndrome. Am. J. Cardiol. 2021, 156, 44–51. [Google Scholar] [CrossRef] [PubMed]
- da Silva, R.L.; de Andrade, P.B.; Dangas, G.; Joaquim, R.M.; da Silva, T.R.; Vieira, R.G.; Pereira, V.C.; Sousa, A.G.; Feres, F.; Costa, J.R. Randomized Clinical Trial on Prevention of Radial Occlusion after Transradial Access Using Nitroglycerin. JACC Cardiovasc. Interv. 2022, 15, 1009–1018. [Google Scholar] [CrossRef] [PubMed]
- Tsigkas, G.; Papanikolaou, A.; Apostolos, A.; Kramvis, A.; Timpilis, F.; Latta, A.; Papafaklis, M.I.; Aminian, A.; Davlouros, P. Preventing and Managing Radial Artery Occlusion following Transradial Procedures: Strategies and Considerations. J. Cardiovasc. Dev. Dis. 2023, 10, 283. [Google Scholar] [CrossRef]
- Gopalakrishnan, P.P.; David, M.; Manoharan, P.; Ponniah, S.R.; Duffy, B. Abstract 16146: Topical Nitroglycerine Reduces Radial Access Site Failure and Femoral Crossover—Topical Nitroglycerine to Prevent Radial Artery Spasm (TNTRASP) Study. Circulation 2020, 142 (Suppl. S3), 16146. [Google Scholar] [CrossRef]
- Dang, D.; Dowling, C.; Zaman, S.; Cameron, J.; Kuhn, L. Predictors of radial to femoral artery crossover during primary percutaneous coronary intervention in ST-elevation myocardial infarction: A systematic review and meta-analysis. Aust. Crit. Care 2023, 36, 915–923. [Google Scholar] [CrossRef]
- Zencirci, E.; Değirmencioğlu, A. Catheter entrapment due to severe radial artery spasm during transradial approach. Cardiol. J. 2016, 23, 324–332. [Google Scholar] [CrossRef] [PubMed]
- Alkhouli, M.; Cohen, H.A.; Bashir, R. Radial artery avulsion—A rare complication of transradial catheterization. Catheter. Cardiovasc. Interv. 2015, 85, E32–E34. [Google Scholar] [CrossRef] [PubMed]
- Ho, H.H.; Jafary, F.H.; Ong, P.J. Radial artery spasm during transradial cardiac catheterization and percutaneous coronary intervention: Incidence, predisposing factors, prevention, and management. Cardiovasc. Revasc. Med. 2012, 13, 193–195. [Google Scholar] [CrossRef] [PubMed]
- He, G.-W.; Yang, C.-Q. Comparison among arterial grafts and coronary artery: An attempt at functional classification. J. Thorac. Cardiovasc. Surg. 1995, 109, 707–715. [Google Scholar] [CrossRef] [PubMed]
- Stojnic, N.; Bukarica, L.G.; Peric, M.; Lesic, A.; Lipkovski, J.M.; Heinle, H. Analysis of Vasoreactivity of Isolated Human Radial Artery. J. Pharmacol. Sci. 2006, 100, 34–40. [Google Scholar] [CrossRef]
- He, G.-W.; Yang, C.-Q. Characteristics of adrenoceptors in the human radial artery: Clinical implications. J. Thorac. Cardiovasc. Surg. 1998, 115, 1136–1141. [Google Scholar] [CrossRef]
- Ruiz-Salmerón, R.J.; Mora, R.; Vélez-Gimón, M.; Ortiz, J.; Fernández, C.; Vidal, B.; Masotti, M.; Betriu, A. Radial artery spasm in transradial cardiac catheterization. Assessment of factors related to its occurrence, and of its consequences during follow-up. Rev. Esp. Cardiol. 2005, 58, 504–511. [Google Scholar] [CrossRef]
- Gorgulu, S.; Norgaz, T.; Karaahmet, T.; Dagdelen, S. Incidence and Predictors of Radial Artery Spasm at the Beginning of a Transradial Coronary Procedure. J. Interv. Cardiol. 2013, 26, 208–213. [Google Scholar] [CrossRef]
- Jia, D.-A.; Zhou, Y.-J.; Shi, D.-M.; Liu, Y.-Y.; Wang, J.-L.; Liu, X.-L.; Wang, Z.-J.; Yang, S.-W.; Ge, H.-L.; Hu, B.; et al. Incidence and predictors of radial artery spasm during transradial coronary angiography and intervention. Chin. Med. J. 2010, 123, 843–847. [Google Scholar]
- Youn, Y.J.; Kim, W.-T.; Lee, J.-W.; Ahn, S.-G.; Ahn, M.-S.; Kim, J.-Y.; Yoo, B.-S.; Lee, S.-H.; Yoon, J.; Choe, K.-H. Eutectic Mixture of Local Anesthesia Cream Can Reduce Both the Radial Pain and Sympathetic Response during Transradial Coronary Angiography. Korean Circ. J. 2011, 41, 726–732. [Google Scholar] [CrossRef]
- Numasawa, Y.; Kawamura, A.; Kohsaka, S.; Takahashi, M.; Endo, A.; Arai, T.; Ohno, Y.; Yuasa, S.; Maekawa, Y.; Fukuda, K. Anatomical variations affect radial artery spasm and procedural achievement of transradial cardiac catheterization. Heart Vessel. 2014, 29, 49–57. [Google Scholar] [CrossRef]
- Kiemeneij, F.; Vajifdar, B.U.; Eccleshall, S.C.; Laarman, G.; Slagboom, T.; van der Wieken, R. Evaluation of a spasmolytic cocktail to prevent radial artery spasm during coronary procedures. Catheter. Cardiovasc. Interv. 2003, 58, 281–284. [Google Scholar] [CrossRef]
- Kiemeneij, F.; Vajifdar, B.U.; Eccleshall, S.C.; Laarman, G.; Slagboom, T.; van der Wieken, R. Measurement of radial artery spasm using an automatic pullback device. Catheter. Cardiovasc. Interv. 2001, 54, 437–441. [Google Scholar] [CrossRef]
- Rosencher, J.; Chaïb, A.; Barbou, F.; Arnould, M.; Huber, A.; Salengro, E.; Jégou, A.; Allouch, P.; Zuily, S.; Mihoub, F.; et al. How to limit radial artery spasm during percutaneous coronary interventions: The spasmolytic agents to avoid spasm during transradial percutaneous coronary interventions (SPASM3) study. Catheter. Cardiovasc. Interv. 2014, 84, 766–771. [Google Scholar] [CrossRef]
- Dahm, J.B.; Wolpers, H.; Becker, J.; Hansen, C.; Felix, S. Transradial access in percutaneous coronary interventions. Herz 2010, 35, 482–487. [Google Scholar] [CrossRef]
- Deftereos, S.; Giannopoulos, G.; Raisakis, K.; Hahalis, G.; Kaoukis, A.; Kossyvakis, C.; Avramides, D.; Pappas, L.; Panagopoulou, V.; Pyrgakis, V.; et al. Moderate Procedural Sedation and Opioid Analgesia during Transradial Coronary Interventions to Prevent Spasm. JACC Cardiovasc. Interv. 2013, 6, 267–273. [Google Scholar] [CrossRef]
- Ercan, S.; Unal, A.; Altunbas, G.; Kaya, H.; Davutoglu, V.; Yuce, M.; Ozer, O. Anxiety Score as a Risk Factor for Radial Artery Vasospasm during Radial Interventions: A Pilot Study. Angiology 2014, 65, 67–70. [Google Scholar] [CrossRef]
- Curtis, E.; Fernandez, R.; Khoo, J.; Weaver, J.; Lee, A.; Halcomb, E.; Halcomb, L. Clinical predictors and management for radial artery spasm: An Australian cross-sectional study. BMC Cardiovasc. Disord. 2023, 23, 67–70. [Google Scholar] [CrossRef]
- Dehghani, P.; Mohammad, A.; Bajaj, R.; Hong, T.; Suen, C.M.; Sharieff, W.; Chisholm, R.J.; Kutryk, M.J.; Fam, N.P.; Cheema, A.N. Mechanism and Predictors of Failed Transradial Approach for Percutaneous Coronary Interventions. JACC Cardiovasc. Interv. 2009, 2, 1057–1064. [Google Scholar] [CrossRef]
- Giannopoulos, G.; Raisakis, K.; Synetos, A.; Davlouros, P.; Hahalis, G.; Alexopoulos, D.; Tousoulis, D.; Lekakis, J.; Stefanadis, C.; Cleman, M.W.; et al. A predictive score of radial artery spasm in patients undergoing transradial percutaneous coronary intervention. Int. J. Cardiol. 2015, 188, 76–80. [Google Scholar] [CrossRef]
- Goldsmit, A.; Kiemeneij, F.; Gilchrist, I.C.; Kantor, P.; Kedev, S.; Kwan, T.; Dharma, S.; Valdivieso, L.; Wenstemberg, B.; Patel, T. Radial artery spasm associated with transradial cardiovascular procedures: Results from the RAS registry. Catheter. Cardiovasc. Interv. 2014, 83, E32–E36. [Google Scholar] [CrossRef] [PubMed]
- Bochenek, T.; Lelek, M.; Kowal-Kałamajka, M.; Kusz, B.; Szczogiel, J.; Jaklik, A.; Roleder, T.; Mizia-Stec, K. Coronary interventions via radial artery without pre procedural routine use of spasmolytic agents. Adv. Interv. Cardiol. 2020, 16, 138–144. [Google Scholar] [CrossRef]
- Zencirci, E.; Değirmencioğlu, A. Can radial artery pulse grading predict radial artery spasm during transradial approach? Kardiol. Polska 2017, 75, 360–367. [Google Scholar] [CrossRef]
- Toprak, K.; Inanır, M.; Memioğlu, T.; Palice, A.; Kaplangoray, M.; Yesilay, A.B.; Tascanov, M.B.; Altıparmak, H.; Demirbağ, R. Effect of Hand Dominance on Radial Artery Spasm and Occlusion: A Prospective Observational Study. Angiology 2024, 75, 340–348. [Google Scholar] [CrossRef]
- Caussin, C.; Gharbi, M.; Durier, C.; Ghostine, S.; Pesenti-Rossi, D.; Rahal, S.; Brenot, P.; Barri, M.; Durup, F.; Lancelin, B. Reduction in spasm with a long hydrophylic transradial sheath. Catheter. Cardiovasc. Interv. 2010, 76, 668–672. [Google Scholar] [CrossRef]
- Meng, S.; Guo, Q.; Tong, G.; Shen, Y.; Tong, X.; Gu, J.; Li, X. Development and Validation of a Nomogram for Predicting Radial Artery Spasm during Coronary Angiography. Angiology 2023, 74, 242–251. [Google Scholar] [CrossRef]
- Hatem, E.; Aslan, O.; Yildirim, S. Relationship between heart rate variability and radial artery spasm in patients undergoing percutaneous coronary angiography via radial access. Eur. Rev. Med. Pharmacol. Sci. 2023, 27, 2927–2935. [Google Scholar] [CrossRef]
- Kocayigit, I. Relation between Serum Asymmetric Dimethylarginine Levels and Radial Artery Spasm. Anatol. J. Cardiol. 2020, 23, 228–232. [Google Scholar] [CrossRef] [PubMed]
- Aminian, A.; Sgueglia, G.A.; Wiemer, M.; Kefer, J.; Gasparini, G.L.; Ruzsa, Z.; van Leeuwen, M.A.; Ungureanu, C.; Leibundgut, G.; Vandeloo, B.; et al. Distal Versus Conventional Radial Access for Coronary Angiography and Intervention. JACC Cardiovasc. Interv. 2022, 15, 1191–1201. [Google Scholar] [CrossRef]
- Aminian, A.; Dolatabadi, D.; Lefebvre, P.; Zimmerman, R.; Brunner, P.; Michalakis, G.; Lalmand, J. Initial experience with the glidesheath slender for transradial coronary angiography and intervention: A feasibility study with prospective radial ultrasound follow-up. Catheter. Cardiovasc. Interv. 2014, 84, 436–442. [Google Scholar] [CrossRef]
- Aminian, A.; Saito, S.; Takahashi, A.; Bernat, I.; Jobe, R.; Kajiya, T.; Gilchrist, I.; Louvard, Y.; Kiemeneij, F.; Van Royen, N.; et al. Comparison of a new slender 6 Fr sheath with a standard 5 Fr sheath for transradial coronary angiography and intervention: RAP and BEAT (Radial Artery Patency and Bleeding, Efficacy, Adverse even T), a randomised multicentre trial. EuroIntervention 2017, 13, e549–e556. [Google Scholar] [CrossRef]
- Astarcioglu, M.A.; Sen, T.; Kilit, C.; Durmus, H.I.; Gozubuyuk, G.; Agus, H.Z.; Kalcik, M.; Karakoyun, S.; Yesin, M.; Dogan, A.; et al. Procedural sedation during transradial coronary angiography to prevent spasm. Herz 2016, 41, 435–438. [Google Scholar] [CrossRef]
- Beyer, A.T.; Ng, R.; Singh, A.; Zimmet, J.; Shunk, K.; Yeghiazarians, Y.; Ports, T.A.; Boyle, A.J. Topical nitroglycerin and lidocaine to dilate the radial artery prior to transradial cardiac catheterization: A randomized, placebo-controlled, double-blind clinical trial. Int. J. Cardiol. 2013, 168, 2575–2578. [Google Scholar] [CrossRef] [PubMed]
- Bouchahda, N.; Ben Abdessalem, M.A.; Ben Hlima, N.; Ben Messaoud, M.; Denguir, H.; Boussaada, M.M.; Saoudi, W.; Jamel, A.; Hassine, M.; Bouraoui, H.; et al. Combination Therapy with Nicardipine and Isosorbide Dinitrate to Prevent Spasm in Transradial Percutaneous Coronary Intervention (from the NISTRA Multicenter Double-Blind Randomized Controlled Trial). Am. J. Cardiol. 2023, 188, 89–94. [Google Scholar] [CrossRef]
- Byrne, J.; Spence, M.; Haegeli, L.; Fretz, E.; Della Siega, A.; Williams, M.; Kinloch, D.; Mildenberger, R.; Klinke, P.; Hilton, D. Magnesium sulphate during transradial cardiac catheterization: A new use for an old drug? J. Invasive Cardiol. 2008, 20, 539–542. [Google Scholar]
- Candemir, B.; Kumbasar, D.; Turhan, S.; Kilickap, M.; Ozdol, C.; Akyurek, O.; Atmaca, Y.; Altin, T. Facilitation of Radial Artery Cannulation by Periradial Subcutaneous Administration of Nitroglycerin. J. Vasc. Interv. Radiol. 2009, 20, 1151–1156. [Google Scholar] [CrossRef]
- Chen, C.-W.; Lin, C.-L.; Lin, T.-K.; Lin, C.-D. A Simple and Effective Regimen for Prevention of Radial Artery Spasm during Coronary Catheterization. Cardiology 2006, 105, 43–47. [Google Scholar] [CrossRef]
- Collet, C.; Corral, J.; Cavalcante, R.; Tateishi, H.; Belzarez, O.; Costa, J.R.; Costa, R.; Chamié, D.; Onuma, Y.; de Winter, R.; et al. Pressure-mediated versus pharmacologic treatment of radial artery spasm during cardiac catheterisation: A randomised pilot study. EuroIntervention 2017, 12, e2212–e2218. [Google Scholar] [CrossRef]
- Coppola, J.; Patel, T.; Kwan, T.; Sanghvi, K.; Srivastava, S.; Shah, S.; Staniloae, C. Nitroglycerin, nitroprusside, or both, in preventing radial artery spasm during transradial artery catheterization. J. Invasive Cardiol. 2006, 18, 155–158. [Google Scholar] [PubMed]
- Coroleu, S.; Allín, J.; Migliaro, G.; Leiva, G.; Baglioni, P.; Nogués, I.; Rodríguez, C.; Donato, B.; Álvarez, J. Use of subcutaneous nitroglycerin to facilitate transradial access in coronary procedures (NiSAR Study). REC Interv. Cardiol. (Engl. Ed.) 2022, 3, 26–32. [Google Scholar] [CrossRef]
- Costa-Mateu, J.; Fernández-Rodríguez, D.; Rivera, K.; Casanova, J.; Irigaray, P.; Zielonka, M.; Pereyra-Acha, E.; Aldomá, A.; Worner, F. Impact of One-Catheter Strategy with TIG I Catheter on Coronary Catheterization Performance and Economic Costs. Arq. Bras. Cardiol. 2019, 113, 960–968. [Google Scholar] [CrossRef]
- Dahm, J.B.; Vogelgesang, D.; Hummel, A.; Staudt, A.; Völzke, H.; Felix, S.B. A randomized trial of 5 vs. 6 French transradial percutaneous coronary interventions. Catheter. Cardiovasc. Interv. 2002, 57, 172–176. [Google Scholar] [CrossRef]
- Deftereos, S.; Giannopoulos, G.; Kossyvakis, C.; Driva, M.; Kaoukis, A.; Raisakis, K.; Theodorakis, A.; Panagopoulou, V.; Lappos, S.; Tampaki, E.; et al. Radial artery flow-mediated dilation predicts arterial spasm during transradial coronary interventions. Catheter. Cardiovasc. Interv. 2011, 77, 649–654. [Google Scholar] [CrossRef]
- Dharma, S.; Shah, S.; Radadiya, R.; Vyas, C.; Pancholy, S.; Patel, T. Nitroglycerin plus diltiazem versus nitroglycerin alone for spasm prophylaxis with transradial approach. J. Invasive Cardiol. 2012, 24, 122–125. [Google Scholar] [PubMed]
- Ezhumalai, B.; Satheesh, S.; Jayaraman, B. Effects of subcutaneously infiltrated nitroglycerin on diameter, palpability, ease-of-puncture and pre-cannulation spasm of radial artery during transradial coronary angiography. Indian Heart J. 2014, 66, 593–597. [Google Scholar] [CrossRef]
- Filho, J.R.M.; Assad, J.A.R.; Zago, A.D.C.; da Costa, R.L.V.; Pierre, A.G.M.; Saleh, M.H.; Barretto, R.; Braga, S.L.N.; Feres, F.; Sousa, A.G.M.R.; et al. Comparative study of the use of diltiazem as an antispasmodic drug in coronary angiography via the transradial approach. Arq. Bras. Cardiol. 2003, 81, 59–63. [Google Scholar] [CrossRef]
- Gul, B.; Stolar, M.; Stair, B.; Hermany, P.; Willis, S.; Mena-Hurtado, C.; Attaran, R. Comparison of procedural success between two radial sheaths: Comparison of the 6-Fr Glidesheath Slender to 6-Fr standard sheath. Herz 2020, 45, 79–85. [Google Scholar] [CrossRef]
- van der Heijden, D.; van Leeuwen, M.; Janssens, G.; Hermie, J.; Lenzen, M.; Ritt, M.; van de Ven, P.; Kiemeneij, F.; van Royen, N. Endothelial dysfunction and the occurrence of radial artery spasm during transradial coronary procedures: The ACRA-Spasm study. EuroIntervention 2016, 12, 1263–1270. [Google Scholar] [CrossRef]
- Hildick-Smith, D.J.; Walsh, J.T.; Lowe, M.D.; Shapiro, L.M.; Petch, M.C. Transradial coronary angiography in patients with contraindications to the femoral approach: An analysis of 500 cases. Catheter. Cardiovasc. Interv. 2004, 61, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Hizoh, I.; Majoros, Z.; Major, L.; Gulyas, Z.; Szabo, G.; Kerecsen, G.; Korda, A.; Molnar, F.; Kiss, R.G. Need for Prophylactic Application of Verapamil in Transradial Coronary Procedures: A Randomized Trial: The VITRIOL (Is Verapamil In TransRadial Interventions OmittabLe?). Trial. J. Am. Heart Assoc. 2014, 3, e000588. [Google Scholar] [CrossRef] [PubMed]
- Horie, K.; Tada, N.; Isawa, T.; Matsumoto, T.; Taguri, M.; Kato, S.; Honda, T.; Ootomo, T.; Inoue, N. A randomised comparison of incidence of radial artery occlusion and symptomatic radial artery spasm associated with elective transradial coronary intervention using 6.5 Fr SheathLess Eaucath Guiding Catheter vs. 6.0 Fr Glidesheath Slender. EuroIntervention 2018, 13, 2018–2025. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.; Daud, M.Y.; Awan, M.S.; Khan, M.I.; Khan, H.; Yousuf, M.A. Frequency and Predictors of Radial Artery Spasm during Coronary Angiography/Percutaneous Coronary Intervention. J. Ayub. Med. Coll. Abbottabad JAMC 2020, 32, 356–358. [Google Scholar]
- Kiani, R.; Alemzadeh-Ansari, M.J.; Sanati, H.R.; Hashemi, R.; Firouzi, A.; Shakerian, F.; Zahedmehr, A.; Peighambari, M.M.; Abdolrahimi, S.A. Periarterial Injections of Nitroglycerin Facilitate Radial Artery Cannulation. Iran. Heart J. 2017, 18, 6–11. [Google Scholar]
- Kim, S.H.; Kim, E.J.; Cheon, W.S.; Kim, M.-K.; Park, W.J.; Cho, G.-Y.; Choi, Y.J.; Rhim, C.Y. Comparative study of nicorandil and a spasmolytic cocktail in preventing radial artery spasm during transradial coronary angiography. Int. J. Cardiol. 2007, 120, 325–330. [Google Scholar] [CrossRef]
- Koga, S.; Ikeda, S.; Futagawa, K.; Sonoda, K.; Yoshitake, T.; Miyahara, Y.; Kohno, S. The use of a hydrophilic-coated catheter during transradial cardiac catheterization is associated with a low incidence of radial artery spasm. Int. J. Cardiol. 2004, 96, 255–258. [Google Scholar] [CrossRef]
- Livesay, J.; Baljepally, R.; Tahir, H.; Heidel, R. Heme Effects in Lowering Patient Discomfort in Radial Artery Verapamil Injection. Cardiol. Res. 2021, 12, 286–292. [Google Scholar] [CrossRef]
- Mikailimirak, S.; Talasaz, A.H.; Jenab, Y.; Vatanara, A.; Amini, M.; Jalali, A.; Gheymati, A. Novel combined topical gel of lidocaine–verapamil–nitroglycerin can dilate the radial artery and reduce radial pain during trans-radial angioplasty. IJC Heart Vasc. 2021, 32, 100689. [Google Scholar] [CrossRef]
- Ouadhour, A.; Sideris, G.; Smida, W.; Logeart, D.; Stratiev, V.; Henry, P. Usefulness of subcutaneous nitrate for radial access. Catheter. Cardiovasc. Interv. 2008, 72, 343–346. [Google Scholar] [CrossRef] [PubMed]
- Rathore, S.; Stables, R.H.; Pauriah, M.; Hakeem, A.; Mills, J.D.; Palmer, N.D.; Perry, R.A.; Morris, J.L. Impact of Length and Hydrophilic Coating of the Introducer Sheath on Radial Artery Spasm during Transradial Coronary Intervention. JACC Cardiovasc. Interv. 2010, 3, 475–483. [Google Scholar] [CrossRef]
- Ruiz-Salmerón, R.J.; Mora, R.; Masotti, M.; Betriu, A. Assessment of the efficacy of phentolamine to prevent radial artery spasm during cardiac catheterization procedures: A randomized study comparing phentolamine vs. verapamil. Catheter. Cardiovasc. Interv. 2005, 66, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Saito, S.; Tanaka, S.; Hiroe, Y.; Miyashita, Y.; Takahashi, S.; Satake, S.; Tanaka, K.; Yamamoto, M. Usefulness of hydrophilic coating on arterial sheath introducer in transradial coronary intervention. Catheter. Cardiovasc. Interv. 2002, 56, 328–332. [Google Scholar] [CrossRef] [PubMed]
- Tatlı, E.; Yılmaztepe, M.A.; Vural, M.G.; Tokatlı, A.; Aksoy, M.; Ağaç, M.T.; Çakar, M.A.; Gündüz, H.; Akdemir, R. Cutaneous analgesia before transradial access for coronary intervention to prevent radial artery spasm. Perfusion 2018, 33, 110–114. [Google Scholar] [CrossRef]
- Tebaldi, M.; Biscaglia, S.; Tumscitz, C.; Del Franco, A.; Gallo, F.; Spitaleri, G.; Fileti, L.; Serenelli, M.; Tonet, E.; Erriquez, A.; et al. Comparison of Verapamil versus Heparin as Adjunctive Treatment for Transradial Coronary Procedures: The VERMUT Study. Cardiology 2018, 140, 74–82. [Google Scholar] [CrossRef]
- Turan, B.; Daşlı, T.; Erkol, A.; Erden, I. Effectiveness of sublingual nitroglycerin before puncture compared with conventional intra-arterial nitroglycerin in transradial procedures: A randomized trial. Cardiovasc. Revasc. Med. 2015, 16, 391–396. [Google Scholar] [CrossRef]
- Varenne, O.; Jégou, A.; Cohen, R.; Empana, J.P.; Salengro, E.; Ohanessian, A.; Gaultier, C.; Allouch, P.; Walspurger, S.; Margot, O.; et al. Prevention of arterial spasm during percutaneous coronary interventions through radial artery: The SPASM study. Catheter. Cardiovasc. Interv. 2006, 68, 231–235. [Google Scholar] [CrossRef]
- Yazdi, A.; Mehr, A.Z.; Khalilipur, E. Effects of Adding Papaverine for the Local Anesthesia of the Access Site in the Transradial Approach for Cardiac Catheterization. Iran. Heart J. 2019, 20, 6–12. [Google Scholar]
- Zencirci, E.; Zencirci, A.E.; Degirmencioglu, A. A randomized trial of flow-mediated dilation to prevent radial artery spasm during transradial approach. Minerva Cardioangiol. 2022, 70, 563–571. [Google Scholar] [CrossRef]
- Gragnano, F.; Jolly, S.S.; Mehta, S.R.; Branca, M.; van Klaveren, D.; Frigoli, E.; Gargiulo, G.; Leonardi, S.; Vranckx, P.; Di Maio, D.; et al. Prediction of radial crossover in acute coronary syndromes: Derivation and validation of the MATRIX score. EuroIntervention 2021, 17, e971–e980. [Google Scholar] [CrossRef]
- Lee, J.-W.; Kim, Y.; Lee, B.-K.; Yoo, S.-Y.; Lee, S.-Y.; Kim, C.-J.; Jin, H.-Y.; Park, J.S.; Heo, J.-H.; Kim, D.-H.; et al. Distal Radial Access for Coronary Procedures in a Large Prospective Multicenter Registry. JACC Cardiovasc. Interv. 2024, 17, 329–340. [Google Scholar] [CrossRef]
- Wang, Y.; Liu, Z.; Wu, Y.; Li, Z.; Wang, Y.; Wang, S.; Xu, R.; Zhang, L.; Wang, Y.; Guo, J. Early prevention of radial artery occlusion via distal transradial access for primary percutaneous coronary intervention. Front. Cardiovasc. Med. 2022, 9, 1071575. [Google Scholar] [CrossRef]
- Nairoukh, Z.; Jahangir, S.; Adjepong, D.; Malik, B.H. Distal Radial Artery Access: The Future of Cardiovascular Intervention. Cureus 2020, 12, e7201. [Google Scholar] [CrossRef]
- Prasad, R.M.; Pandrangi, P.; Pandrangi, G.; Yoo, H.; Salazar, A.M.; Ukponmwan, E.; Kehdi, M.; Abela, G. Meta-Analysis Comparing Distal Radial Artery Approach versus Traditional for Coronary Procedures. Am. J. Cardiol. 2022, 164, 52–56. [Google Scholar] [CrossRef]
- Daralammouri, Y.; Nazzal, Z.; Mosleh, Y.S.; Abdulhaq, H.K.; Khayyat, Z.Y.; El Hamshary, Y.; Azamtta, M.; Ghanim, A.; Awwad, F.; Majadla, S.; et al. Distal Radial Artery Access in comparison to Forearm Radial Artery Access for Cardiac Catheterization: A Randomized Controlled Trial (DARFORA Trial). J. Interv. Cardiol. 2022, 2022, 7698583. [Google Scholar] [CrossRef] [PubMed]
- Kindel, M.; Rüppel, R. Hydrophilic-coated sheaths increase the success rate of transradial coronary procedures and reduce patient discomfort but do not reduce the occlusion rate: Randomized single-blind comparison of coated vs. non-coated sheaths. Clin. Res. Cardiol. 2008, 97, 609–614. [Google Scholar] [CrossRef] [PubMed]
- Goel, P.K.; Menon, A.; Mullasari, A.S.; Valaparambil, A.K.; Pinto, B.; Pahlajani, D.; Gunasekaran, S.; Trehan, V.K.; Abhaichand, R.K.; Chugh, S.K.; et al. Transradial access for coronary diagnostic and interventional procedures: Consensus statement and recommendations for India Advancing Complex CoronariES Sciences through TransRADIAL intervention in India—ACCESS RADIAL™: Clinical consensus recommendations in collaboration with Cardiological Society of India. Indian Heart J. 2018, 70, 922–933. [Google Scholar] [CrossRef]
- Coghill, E.M.; Johnson, T.; Morris, R.E.; Megson, I.L.; Leslie, S.J. Radial artery access site complications during cardiac procedures, clinical implications and potential solutions: The role of nitric oxide. World J. Cardiol. 2019, 12, 26–34. [Google Scholar] [CrossRef]
- Alushi, B.; Lauten, A.; Ndrepepa, G.; Leistner, D.M.; Kufner, S.; Xhepa, E.; Landmesser, U.; Kastrati, A.; Cassese, S. Procedural and clinical performance of dual- versus single-catheter strategy for transradial coronary angiography: A meta-analysis of randomized trials. Catheter. Cardiovasc. Interv. 2020, 96, 276–282. [Google Scholar] [CrossRef]
- Obaid, D.; Hailan, A.; Chase, A.; Dorman, S.; Jenkins, G.; Raybould, A.; Ramsey, M.; Thomas, P.; Smith, D.; Ionescu, A. Balloon-Assisted Tracking Use Reduces Radial Artery Access Failure in an Experienced Radial Center and is Feasible during Primary PCI for STEMI. J. Invasive Cardiol. 2017, 29, 219–224. [Google Scholar] [PubMed]
- Liang, M.; Devlin, G.; Harding, S.A. Radial Artery Spasm and Perforation: Simple Solutions for Challenging Cases. Heart Lung Circ. 2015, 24, e71–e74. [Google Scholar] [CrossRef]
- Patel, T.; Shah, S.; Pancholy, S. Balloon-assisted tracking of a guide catheter through difficult radial anatomy: A technical report. Catheter. Cardiovasc. Interv. 2013, 81, E215–E218. [Google Scholar] [CrossRef]
- Pavlidis, A.N.; Karamasis, G.V.; Rees, P. Balloon-assisted tracking during primary percutaneous coronary intervention. Acute Card. Care 2015, 17, 26–28. [Google Scholar] [CrossRef]
- Felekos, I.; Hussain, R.; Patel, S.J.; Pavlidis, A.N. Balloon-assisted tracking: A practical solution to avoid radial access failure due to difficult anatomical challenges. Cardiovasc. Revasc. Med. 2018, 19, 564–569. [Google Scholar] [CrossRef] [PubMed]
- Scoccia, A.; Khokhar, A.; Oshoala, K.; Laricchia, A.; Chandra, K.; Cardelli, L.; Gasparini, G.; Giannini, F.; Colombo, A.; Mangieri, A. Mother-in-Child Assisted Tracking (MiCAT): A Mechanical Technique to Overcome Severe Radial Artery Spasm. J. Invasive Cardiol. 2022, 34, E588–E593. [Google Scholar] [CrossRef] [PubMed]
- Vuurmans, T.; Hilton, D. Brewing the right cocktail for radial intervention. Indian Heart J. 2011, 62, 221–225. [Google Scholar]
- Boyer, N.; Beyer, A.; Gupta, V.; Dehghani, H.; Hindnavis, V.; Shunk, K.; Zimmet, J.; Yeghiazarians, Y.; Ports, T.; Boyle, A. The effects of intra-arterial vasodilators on radial artery size and spasm: Implications for contemporary use of trans-radial access for coronary angiography and percutaneous coronary intervention. Cardiovasc. Revasc. Med. 2013, 14, 321–324. [Google Scholar] [CrossRef]
- Kwok, C.S.; Rashid, M.; Fraser, D.; Nolan, J.; Mamas, M. Intra-arterial vasodilators to prevent radial artery spasm: A systematic review and pooled analysis of clinical studies. Cardiovasc. Revasc. Med. 2015, 16, 484–490. [Google Scholar] [CrossRef] [PubMed]
- Asghar, H.; Shroff, A. Preventing spasm during transradial angiography: Sometimes less is more. J. Invasive Cardiol. 2012, 24, 126–127. [Google Scholar] [PubMed]
- Chong, A.-Y.; Lo, T.; George, S.; Ratib, K.; Mamas, M.; Nolan, J. The effect of pre-procedure sublingual nitroglycerin on radial artery diameter and Allen’s test outcome—Relevance to transradial catheterization. Cardiovasc. Revasc. Med. 2018, 19, 163–167. [Google Scholar] [CrossRef]
- Pancholy, S.B. Comparison of the Effect of Intra-Arterial versus Intravenous Heparin on Radial Artery Occlusion after Transradial Catheterization. Am. J. Cardiol. 2009, 104, 1083–1085. [Google Scholar] [CrossRef]
- Bertrand, O.F.; Rao, S.V.; Pancholy, S.; Jolly, S.S.; Rodés-Cabau, J.; Larose, É.; Costerousse, O.; Hamon, M.; Mann, T. Transradial Approach for Coronary Angiography and Interventions. JACC Cardiovasc. Interv. 2010, 3, 1022–1031. [Google Scholar] [CrossRef]
- Nisanoglu, V.; Battaloglu, B.; Ozgur, B.; Eroglu, T.; Erdil, N. Topical Vasodilators for Preventing Radial Artery Spasm during Harvesting for Coronary Revascularization: Comparison of 4 Agents. Heart Surg. Forum 2006, 9, E807–E812. [Google Scholar] [CrossRef] [PubMed]
- Majure, D.T.; Hallaux, M.; Yeghiazarians, Y.; Boyle, A.J. Topical nitroglycerin and lidocaine locally vasodilate the radial artery without affecting systemic blood pressure: A dose-finding phase I study. J. Crit. Care 2012, 27, 532.e9–532.e13. [Google Scholar] [CrossRef] [PubMed]
- Economou, F.I.; Doundoulakis, I.; Kalamakidou, I.; Koliastasis, L.; Soulaidopoulos, S.; Samara, M.; Dimitriadis, K.; Papazisis, G.; Tsiachris, D.; Tsioufis, K. Prevention of Radial Artery Spasm with Transdermal Glyceryl Trinitrate Patches. JACC Cardiovasc. Interv. 2023, 16, 365–367. [Google Scholar] [CrossRef]
- Pancholy, S.B.; Coppola, J.; Patel, T. Subcutaneous administration of nitroglycerin to facilitate radial artery cannulation. Catheter. Cardiovasc. Interv. 2006, 68, 389–391. [Google Scholar] [CrossRef] [PubMed]
- Koca, F.; Levent, F.; Demir, Ö.F.; Kat, N.; Tenekecioglu, E. Does the Use of Ethyl Chloride Spray Facilitate Radial Angiography? Angiology 2024, 75, 22–28. [Google Scholar] [CrossRef]
- Taniguchi, M.; Ozaki, Y.; Katayama, Y.; Satogami, K.; Ino, Y.; Tanaka, A. Impact of Upper Arm Prolonged Occlusion on Radial Artery Diameter before Coronary Angiography in Patients with Coronary Artery Disease. Cardiovasc. Revasc. Med. 2023, 51, 38–42. [Google Scholar] [CrossRef]
- Doubell, J.; Kyriakakis, C.; Weich, H.; Herbst, P.; Pecoraro, A.; Moses, J.; Griffiths, B.; Snyman, H.W.; Kabwe, L.; Du Toit, R.; et al. Radial artery dilatation to improve access and lower complications during coronary angiography: The RADIAL trial. EuroIntervention 2021, 16, 1349–1355. [Google Scholar] [CrossRef]
- Ying, L.; Xu, K.; Gong, X.; Liu, X.; Fan, Y.; Zhao, H.; Wang, F.; Khurwolah, M.R.; Li, C. Flow-mediated dilatation to relieve puncture-induced radial artery spasm: A pilot study. Cardiol. J. 2018, 25, 1–6. [Google Scholar] [CrossRef]
- Rao, S.V.; Wegermann, Z.K. Pumping up best practices in radial artery access: Prolonged occlusion flow-mediated dilation improves radial artery access success. EuroIntervention 2021, 16, 1299–1300. [Google Scholar] [CrossRef]
- Sinha, C.; Kumar, A.; Kumari, P.; Kumar, A.; Bhar, D.; Singh, V. Does radial or median nerve blocks affect the area and blood flow of radial artery? Anaesth. Crit. Care Pain Med. 2021, 40, 100831. [Google Scholar] [CrossRef] [PubMed]
- Bhakta, P.; Zaheer, H. Ultrasound-guided radial nerve block to relieve cannulation-induced radial arterial spasm. Can. J. Anaesth. 2017, 64, 1269–1270. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, P.L.; Deutch, Z.; Castillo, D. Brachial Plexus Block for Removal of Retained Radial Artery Sheath. Cureus 2022, 14, e33068. [Google Scholar] [CrossRef]
- Cochet, A.A.; Bellin, D.A. Surgery Averted Using a Novel, Minimally Invasive Approach to Treat Very Severe Radial Artery Spasm. Case Rep. Cardiol. 2017, 2017, 8487056. [Google Scholar] [CrossRef] [PubMed]
- Price, B. Managing patients’ anxiety about planned medical interventions. Nurs. Stand. 2017, 31, 53–63. [Google Scholar] [CrossRef]
- Chugh, S.K.; Chugh, S.; Chugh, Y.; Rao, S.V. Feasibility and utility of pre-procedure ultrasound imaging of the arm to facilitate transradial coronary diagnostic and interventional procedures (PRIMAFACIE-TRI). Catheter. Cardiovasc. Interv. 2013, 82, 64–73. [Google Scholar] [CrossRef]
- Pacha, H.M.; Alahdab, F.; Al-Khadra, Y.; Idris, A.; Rabbat, F.; Darmoch, F.; Soud, M.; Zaitoun, A.; Kaki, A.; Rao, S.V.; et al. Ultrasound-guided versus palpation-guided radial artery catheterization in adult population: A systematic review and meta-analysis of randomized controlled trials. Am. Heart J. 2018, 204, 1–8. [Google Scholar] [CrossRef]
- Riangwiwat, T.; Mumtaz, T.; Blankenship, J.C. Barriers to use of radial access for percutaneous coronary intervention. Catheter. Cardiovasc. Interv. 2020, 96, 268–273. [Google Scholar] [CrossRef]
- Raut, M.; Mantri, R.; Sharma, M.; Maheshwari, A. Propofol to relieve radial artery spasm. Indian Heart J. 2016, 68, 364–365. [Google Scholar] [CrossRef]
- Repanas, T.; Christopoulos, G.; Brilakis, E.S. Administration of ViperSlide™ for treating severe radial artery spasm: Case report and systematic review of the literature. Cardiovasc. Revasc. Med. 2015, 16, 243–245. [Google Scholar] [CrossRef]
- Raje, V.; Christopher, S.; Hopkinson, D.A.; Kania, D.A.; Jovin, I.S. Administration of Rotaglide™ solution for treating refractory severe radial artery spasm: A case report. Cardiovasc. Revasc. Med. 2018, 19, 56–57. [Google Scholar] [CrossRef] [PubMed]
- Barcin, C.; Kursaklioglu, H.; Kose, S.; Amasyali, B.; Isik, E. Resistant radial artery spasm during coronary angiography via radial approach responded to local warm compress. Anadolu Kardiyol. Dergisi Anatol. J. Cardiol. 2010, 10, 90–91. [Google Scholar] [CrossRef]
- Abdelazeem, B.; Abuelazm, M.T.; Swed, S.; Gamal, M.; Atef, M.; Al-Zeftawy, M.A.; Noori, M.A.; Lutz, A.; Volgman, A.S. The efficacy of nitroglycerin to prevent radial artery spasm and occlusion during and after transradial catheterization: A systematic review and meta-analysis of randomized controlled trials. Clin. Cardiol. 2022, 45, 1171–1183. [Google Scholar] [CrossRef]
- Curtis, E.; Fernandez, R.; Lee, A. The effect of topical medications on radial artery spasm in patients undergoing transradial coronary procedures: A systematic review. JBI Database Syst. Rev. Implement Rep. 2018, 16, 738–751. [Google Scholar] [CrossRef]
- Mason, P.J.; Shah, B.; Tamis-Holland, J.E.; Bittl, J.A.; Cohen, M.G.; Safirstein, J.; Drachman, D.E.; Valle, J.A.; Rhodes, D.; Gilchrist, I.C.; et al. An Update on Radial Artery Access and Best Practices for Transradial Coronary Angiography and Intervention in Acute Coronary Syndrome: A Scientific Statement from the American Heart Association. Circ. Cardiovasc. Interv. 2018, 11, e000035. [Google Scholar] [CrossRef]
- Shroff, A.R.; Gulati, R.; Drachman, D.E.; Feldman, D.N.; Gilchrist, I.C.; Kaul, P.; Lata, K.; Pancholy, S.B.; Panetta, C.J.; Seto, A.H.; et al. SCAI expert consensus statement update on best practices for transradial angiography and intervention. Catheter. Cardiovasc. Interv. 2020, 95, 245–252. [Google Scholar] [CrossRef]
- Satti, S.R.; Vance, A.Z. Radial Access for Neurovascular Procedures. Semin. Interv. Radiol. 2020, 37, 182–191. [Google Scholar] [CrossRef]


| Clinical Factors Used to Define RAS |
|---|
|
|
|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zus, A.S.; Crișan, S.; Luca, S.; Nișulescu, D.; Valcovici, M.; Pătru, O.; Lazăr, M.-A.; Văcărescu, C.; Gaiță, D.; Luca, C.-T. Radial Artery Spasm—A Review on Incidence, Prevention and Treatment. Diagnostics 2024, 14, 1897. https://doi.org/10.3390/diagnostics14171897
Zus AS, Crișan S, Luca S, Nișulescu D, Valcovici M, Pătru O, Lazăr M-A, Văcărescu C, Gaiță D, Luca C-T. Radial Artery Spasm—A Review on Incidence, Prevention and Treatment. Diagnostics. 2024; 14(17):1897. https://doi.org/10.3390/diagnostics14171897
Chicago/Turabian StyleZus, Adrian Sebastian, Simina Crișan, Silvia Luca, Daniel Nișulescu, Mihaela Valcovici, Oana Pătru, Mihai-Andrei Lazăr, Cristina Văcărescu, Dan Gaiță, and Constantin-Tudor Luca. 2024. "Radial Artery Spasm—A Review on Incidence, Prevention and Treatment" Diagnostics 14, no. 17: 1897. https://doi.org/10.3390/diagnostics14171897