
Optical Methods for Optimizing Fluorescence Imaging Field of View and Image Quality in Surgical Guidance Procedures
 ,
, 
Abstract
:
1. Introduction
2. Research Method
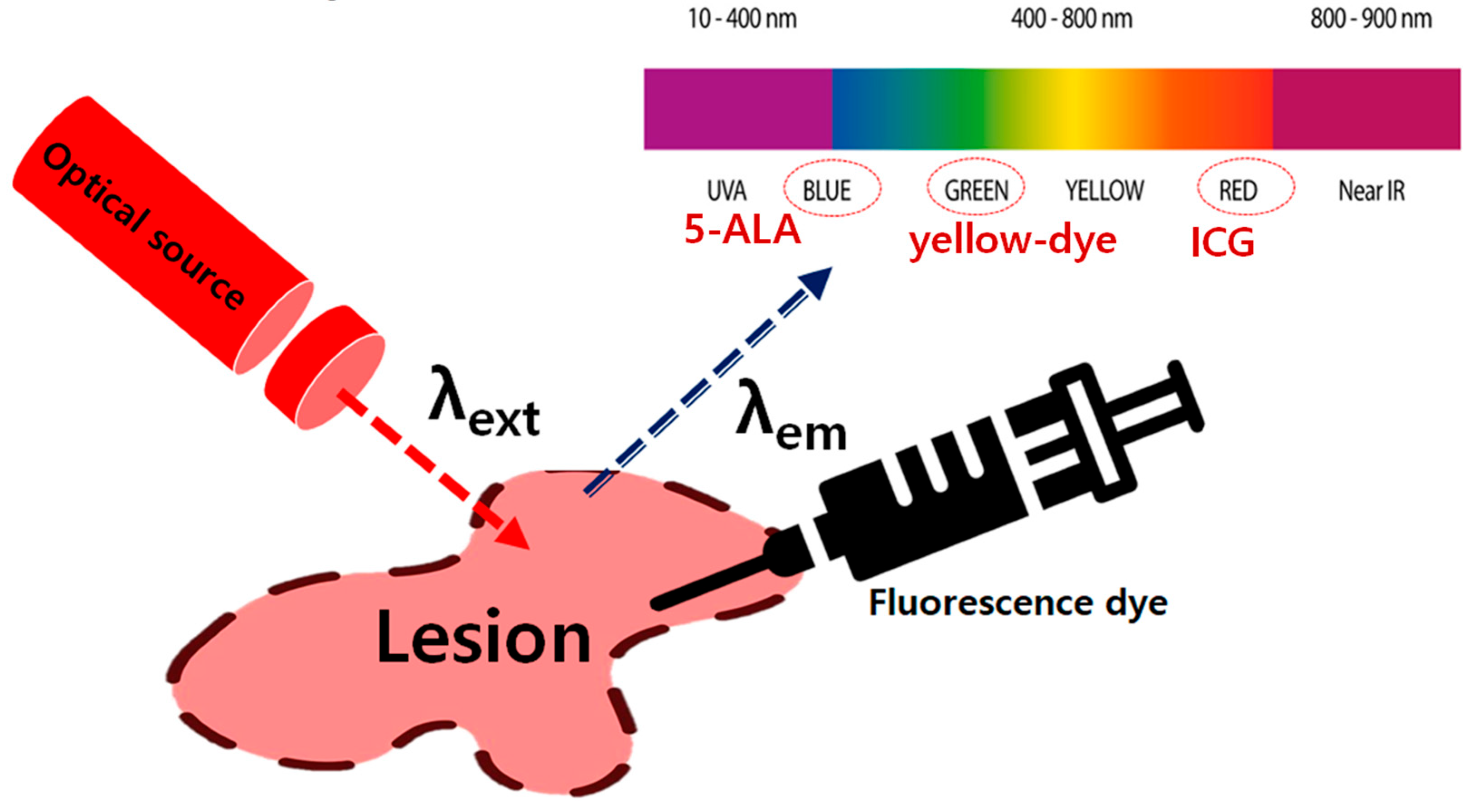
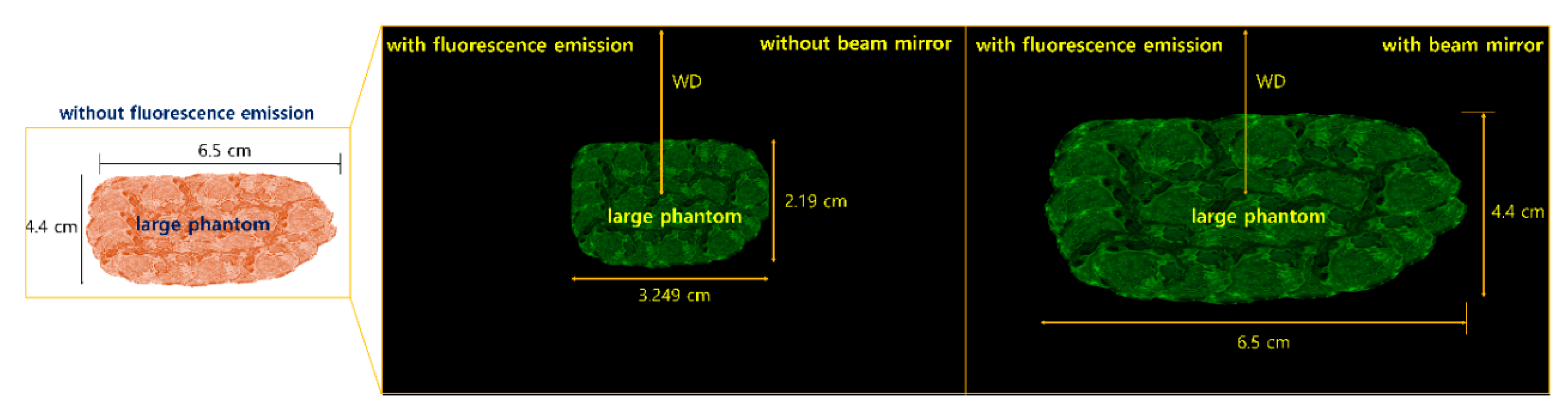
2.1. Analysis of Fluorescence Emission Phenomenon
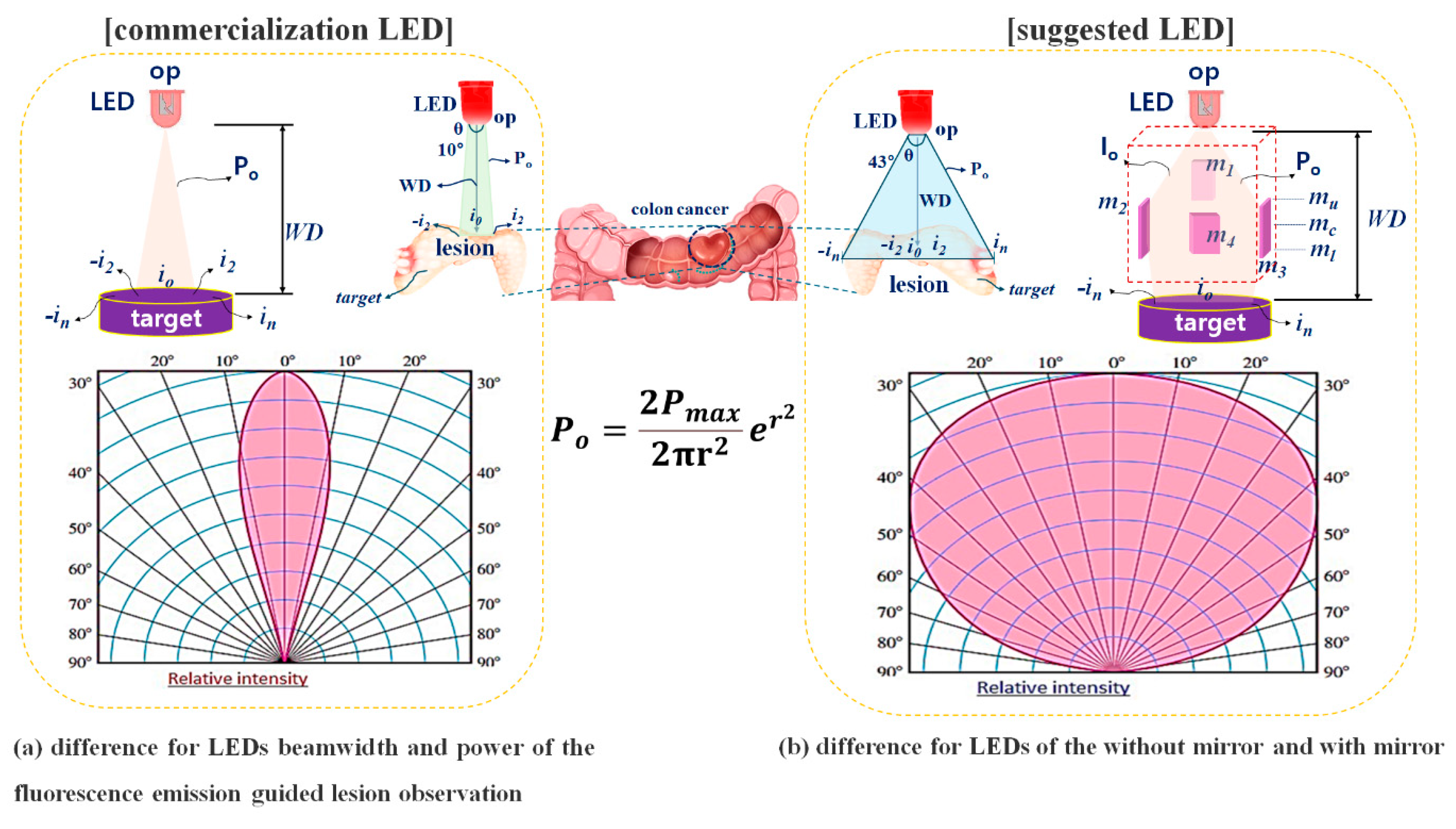
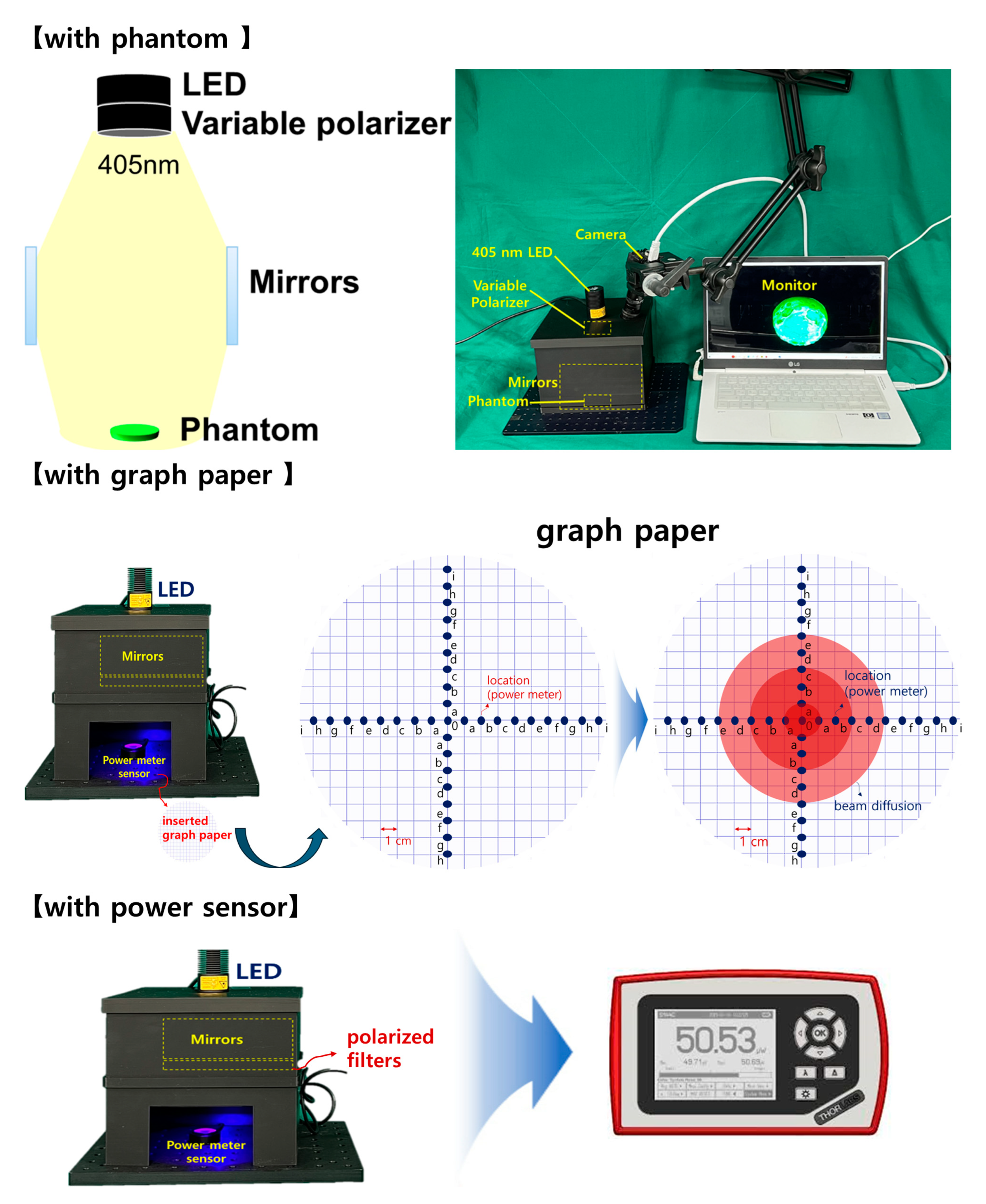
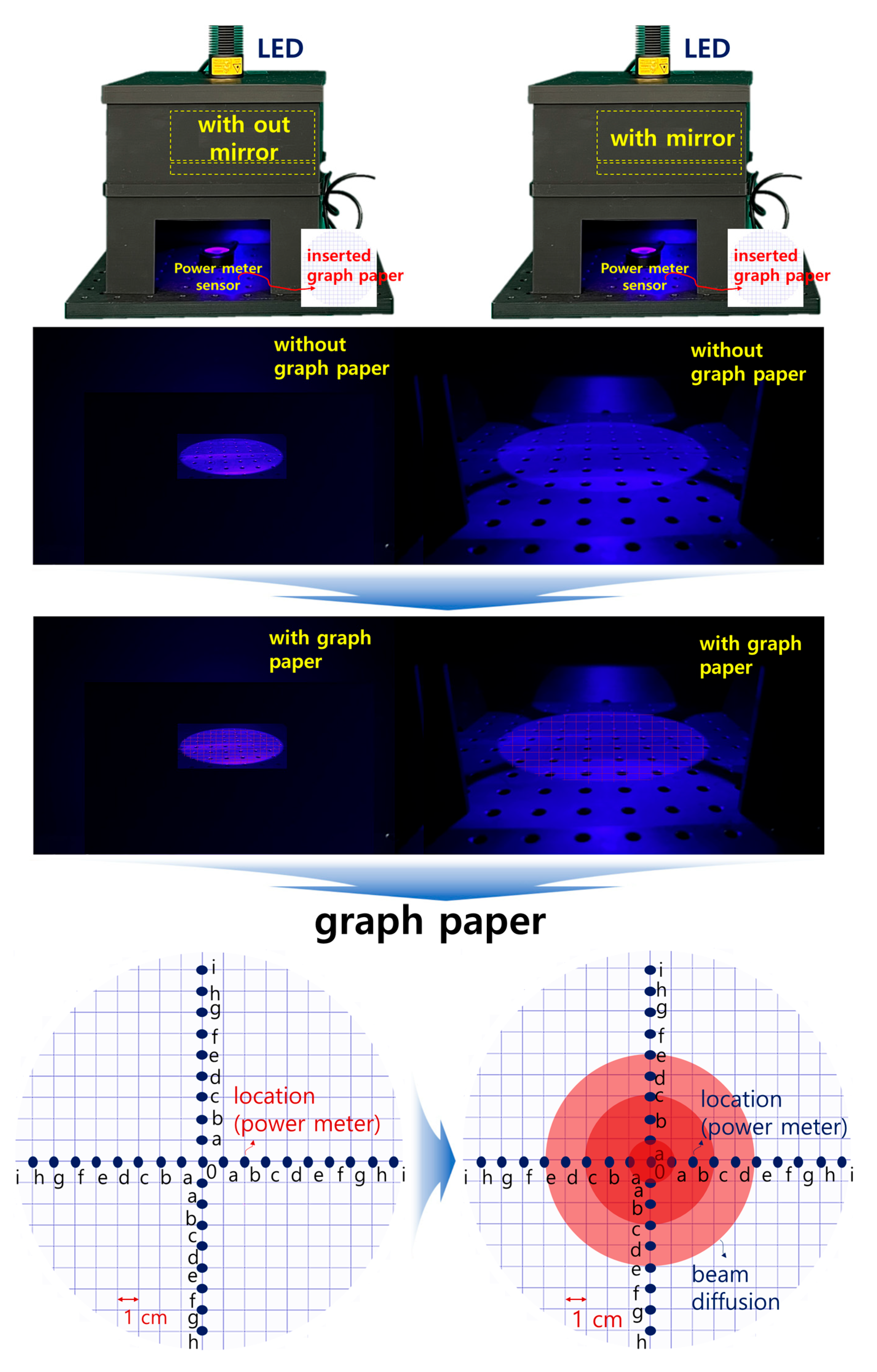
2.2. Analysis of Methods for Increasing Beam Width and Beam Intensity
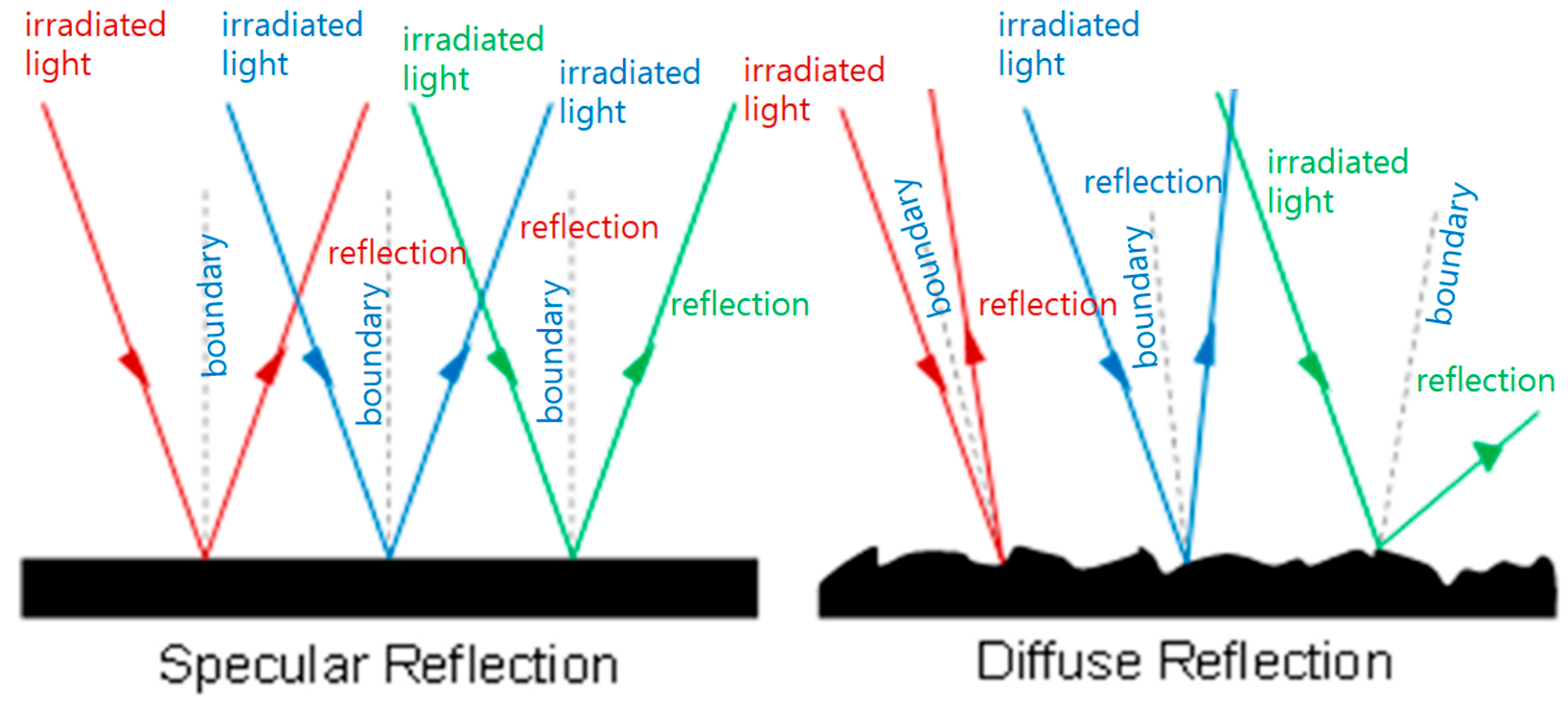
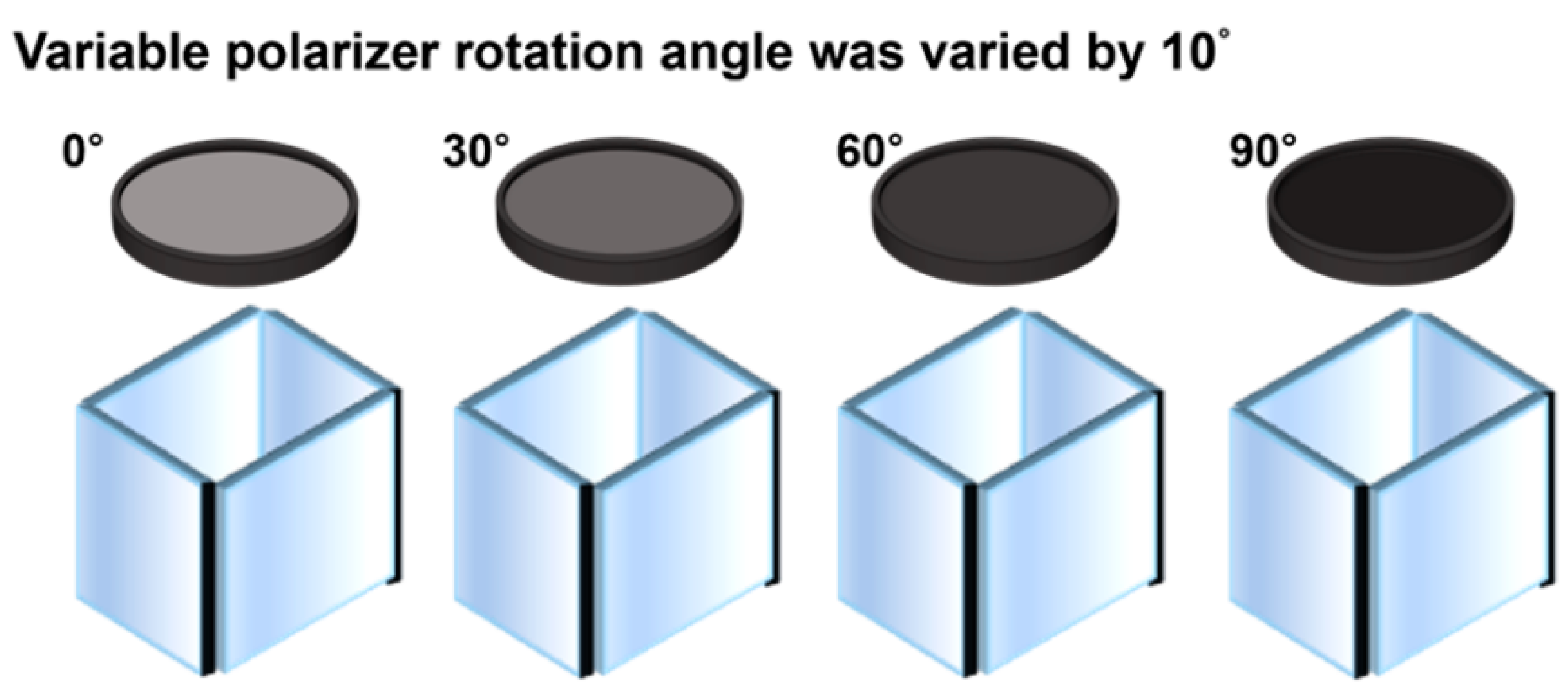
2.3. Analysis of Light Reflection Reduction Methods
3. Experimental Results
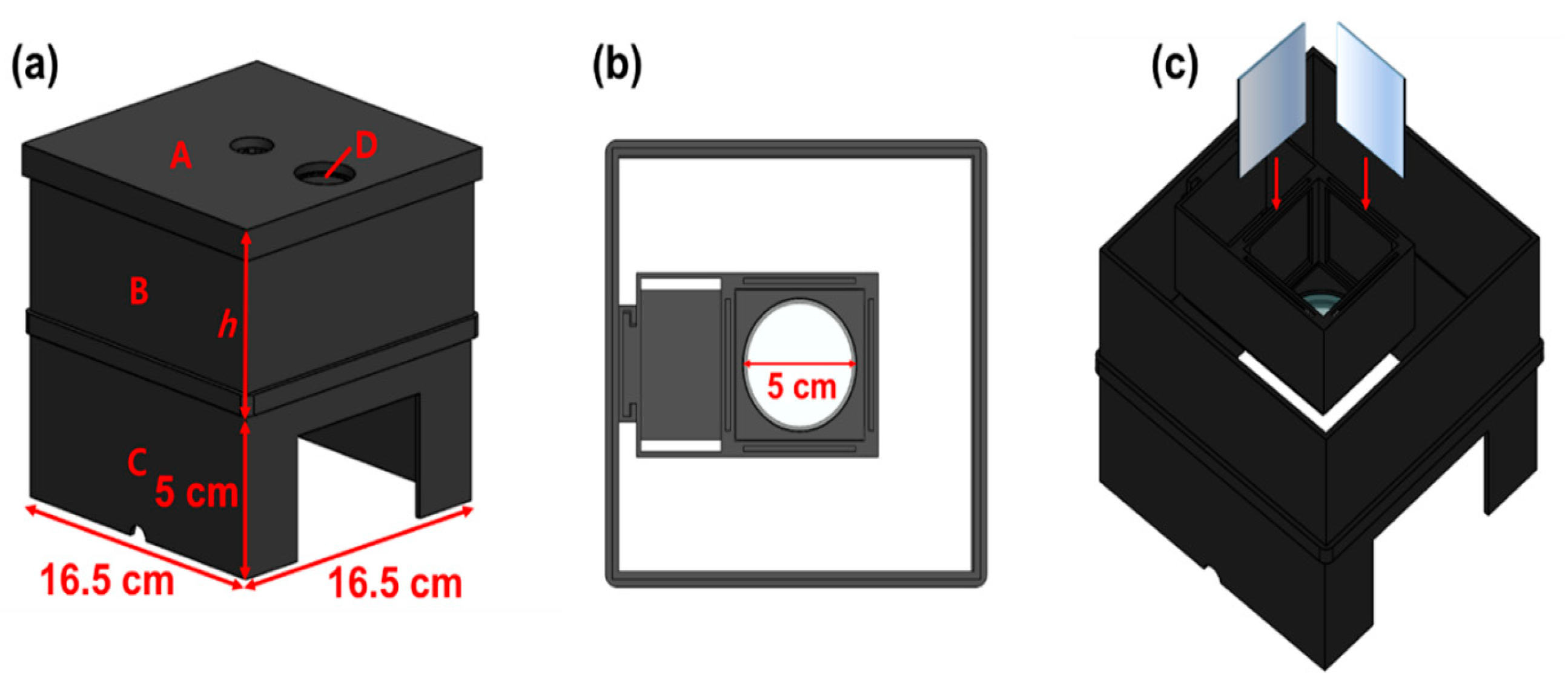
3.1. Experimental Environment Configuration
3.2. Experiment Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Visaggi, P.; Barberio, B.; Ghisa, M.; Ribolsi, M.; Savarino, V.; Fassan, M.; Valmasoni, M.; Marchi, S.; Bortoli, N.; Savarino, E.M. Diagnosis of early esophageal cancer: From blood biomarkers to advanced endoscopy and artificial intelligence. Cancers 2021, 13, 3162. [Google Scholar] [CrossRef]
- Suzuki, T.; Kitagawa, Y.; Nankinzan, R.; Yamaguchi, T. Early gastric cancer diagnostic ability of ultrathin endoscope loaded with laser light source. World J. Gastroenterol. 2019, 25, 1378–1386. [Google Scholar] [CrossRef]
- World Health Organization. Guide to Early Cancer Diagnosis; World Health Organization: Lyon, France, 2017. [Google Scholar]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics. CA Cancer J. Clin. 2018, 68, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Bidram, E.; Esmaeili, Y.; Ranji–Burachaloo, H.; Al–Zaubai, N.; Zarrabi, A.; Stewart, A.; Dunstan Dave, E. A concise review on cancer treatment methods and delivery systems. J. Drug Deliv. Sci. Technol. 2019, 54, 101350. [Google Scholar] [CrossRef]
- Kim, H.R.; Lee, H.M.; Yoo, H.; Lee, S.H.; Kim, K.G. Review of Neurosurgical Fluorescence Imaging Systems for Clinical Application. J. Opt. Soc. Korea 2016, 20, 305–313. [Google Scholar] [CrossRef]
- Silva, E.B., Jr.; Ramina, R.; Coelho Neto, M.; Machado, G.A.S.; Cavalcanti, M.S.; Silva, J.F.C. Extending the Indications of 5-Aminolevulinic Acid for Fluorescence-Guided Surgery for Different Central Nervous System Tumors: A Series of 255 Cases in Latin America. Arq. Bras. Neurocir. 2022, 41, 35–42. [Google Scholar] [CrossRef]
- Hadjipanayis, C.G.; Stummer, W. 5–ALA and FDA approval for glioma surgery. J. Neuro–Oncol. 2019, 141, 479–486. [Google Scholar] [CrossRef] [PubMed]
- Ju, M.; Yoon, K.; Lee, S.; Kim, K.G. Single quasi–symmetrical LED with high intensity and wide beam width using diamond–shaped mirror refraction method for surgical fluorescence microscope applications. Diagnostics 2023, 13, 2763. [Google Scholar] [CrossRef]
- Lee, S.M.; Yoon, K.C.; Lee, S.; Ryu, S.Y.; Kim, K.G. Multi–asymmetric irradiation method using a ring array to obtain an emission−capable LED beam power effect to observe cancer removal status in a surgical microscope. Diagnostics 2023, 13, 3482. [Google Scholar] [CrossRef]
- Jiao, J.; Fan, W.; Sun, J.; Satoshi, N. Highlight removal for camera captured documents based on image stitching. In Proceedings of the International Conference on Signal Processing, Washington, DC, USA, 6–10 November 2016. [Google Scholar]
- Wan, R.; Shi, B.; Duan, L.Y.; Tan, A.H.; Kot, A.C. Benchmarking single image reflection removal algorithm. In Proceedings of the International Conference on Computer Vision, Venice, Italy, 29 October 2017. [Google Scholar]
- Li, C.; Yang, Y.; He, K.; Lin, S.; Hopcroft, J.E. Single image reflection removal through cascaded refinement. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, Seattle, WA, USA, 14–19 June 2020; pp. 3565–3574. [Google Scholar]
- Tchoulack, S.; Pierre Langlois, J.M.; Cheriet, F. A video stream processor for real–time detection and correction of specular reflections in endoscopic images. In Proceedings of the Circuits and Systems and TAISA Conference, Montreal, QC, Canada, 22–25 June 2008; pp. 49–52. [Google Scholar]
- Yamazaki, M.; Chen, Y.; Xu, G. Separating reflections from images using kernel independent component analysis. In Proceedings of the 18th International Conference on Pattern Recognition, Hong Kong, China, 20–24 August 2006; Volume 3, pp. 194–197. [Google Scholar]
- Hodgson, A.; Kelly, N.; Peel, D. Unmanned aerial vehicles (UAVs) for surveying marine fauna: A dugong case study. PLoS ONE 2013, 8, e79556. [Google Scholar] [CrossRef]
- Ahn, J.; Nishida, K.; Ishii, Y.; Ura, T. A sea creatures classification method using convolutional neural networks. In Proceedings of the IEEE 18th International Conference on Control, Automation and Systems (ICCAS), PyeongChang, Republic of Korea, 17–20 October 2018. [Google Scholar]
- So, H.R.; Oh, S.J.; Jin, G.G. Modified geometric step–based box–counting method to estimate the complexity of Korean peninsula coastlines. J. Inst. Control. 2019, 25, 30–36. [Google Scholar]
- Goncalves, J.; Henriques, R. UAV photogrammetry for topographic monitoring of coastal areas. ISPRS J. Photogramm. Remote Sens. 2015, 104, 101–111. [Google Scholar] [CrossRef]
- Lee, S.; Yoon, K.C.; Kim, J.; Kim, K.G. Specular reflection suppression through the adjustment of linear polarization for tumor diagnosis using fluorescein sodium. Sensors 2022, 22, 6651. [Google Scholar] [CrossRef]
- Nie, C.; Xu, C.; Li, Z.; Chu, L.; Hu, Y. Specular Reflections Detection and Removal for Endoscopic Images Based on Brightness Classification. Sensors 2023, 23, 974. [Google Scholar] [CrossRef]
- Yoon, K.C.; Kim, K.G.; Lee, S.A. Surgical pen–type probe design for real–time optical diagnosis of tumor status using 5–aminolevulinic acid. Diagnostics 2021, 11, 1014. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Li, X.; Zhang, B.; Xie, G.; Zhou, Z.; Yang, X.; Ying, L.; Mei, Y.; Fan, W.; Lon, Z.; et al. Optical gain at 637 nm wavelength in polymer waveguide amplifier under commercial LED Pumping for planar photonic Integration. Adv. Opt. Mater. 2022, 10, 2200205. [Google Scholar] [CrossRef]
- Yoon, K.C.; Kim, K.G. NIR irradiation based on low–power LED drive module design for fat reduction. BioMed Res. Int. 2021, 12, 9992095. [Google Scholar] [CrossRef]
- Sun, Y.; Wang, H.; Zhang, X.; Yu, W.; Zhang, L.; Han, X. Specular Highlight Removal Based on Dichromatic Reflection Model and Priority-Based Adaptive Direction with Light Field Camera. Opt. Express 2021, 29, 43678–43695. [Google Scholar]
- Lee, S.; Yoon, K.C.; Kim, J.; Kim, K.G. Reduction of specular reflection based on linear polarization control for fluorescence–induced diagnostic evaluation. Diagnostics 2022, 12, 1990. [Google Scholar] [CrossRef]
- Yoon, K.C.; Seol, J.; Kim, K.G. Removal of specular reflection using angle adjustment of linear polarized filter in medical imaging diagnosis. Diagnostics 2022, 12, 863. [Google Scholar] [CrossRef]
- Ewelt, C.; Nemes, A.; Senner, V.; Wölfer, J.; Brokinkel, B.; Stummer, W.; Holling, M. Fluorescence in neurosurgery: Its diagnostic and therapeutic use. Review of the literature. J. Photochem. Photobiol. B 2015, 148, 302–309. [Google Scholar] [CrossRef]
- Khalafi, S.; Botero Fonnegra, C.; Reyes, A.; Hui, V.W. Developments in the Use of Indocyanine Green (ICG) Fluorescence in Colorectal Surgery. J. Clin. Med. 2024, 13, 4003. [Google Scholar] [CrossRef] [PubMed]
- Acerbi, F.; Broggi, M.; Eoli, M.; Anghileri, E.; Cavallo, C.; Boffano, C.; Cordera, S.; Schiariti, M.; Prada, F.; Ferroli, P. Fluorescein application in cranial and spinal tumors enhancing at preoperative MRI and operated with a dedicated filter on the surgical microscope: Preliminary results in 279 patients enrolled in the FLUOCERTUM prospective study. Cancers 2021, 13, 1912. [Google Scholar]
- Maclean, M.; MacGregor, S.J.; Anderson, J.G.; Woolsey, G.A. 405 nm Light Technology for the Inactivation of Pathogens and Its Potential Role for Environmental Disinfection and Infection Control. Int. J. Environ. Res. Public Health 2010, 7, 2835–2857. [Google Scholar] [CrossRef] [PubMed]
- Schebesch, K.M.; Proescholdt, M.; Höhne, J.; Hohenberger, C.; Hansen, E.; Riemenschneider, M.J.; Ullrich, W.; Doenitz, C.; Schlaier, J.; Lange, M.; et al. Sodium fluorescein–guided resection under the YELLOW 560 nm surgical microscope filter in malignant brain tumor surgery—A feasibility study. Acta Neurochir. 2013, 155, 693–699. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.R.; Davis, G.L.; Oden, Z.M.; Razavi, M.R.; Fateh, A.; Ghazanfari, M.; Abdolrahimi, F.; Poorazar, S.; Sakhaie, F.; Olsen, R.J.; et al. Portable, battery–operated, low–cost, bright field and fluorescence microscope. PLoS ONE 2010, 5, e11890. [Google Scholar] [CrossRef]
- Wang, X. LED ring array light source design and uniform illumination properties analysis. Optik 2017, 140, 273–281. [Google Scholar] [CrossRef]
- Ma, L.; Fei, B. Comprehensive review of surgical microscopes: Technology development and medical applications. J. Biomed. Opt. 2021, 26, 010901. [Google Scholar] [CrossRef]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| F2 Rotation Angle of Filter (θ) | Light Reflection Intensity [mW/cm2] | F2 Filter Rotation Angle (θ) | Light Reflection Intensity [mW/cm2] |
|---|---|---|---|
| 0° | 50.0 | 210° | 37.5 |
| 30° | 37.5 | 240° | 12.5 |
| 60° | 50.0 | 270° | 0.00 |
| 90° | 0.00 | 300° | 12.5 |
| 120° | 12.5 | 330° | 37.5 |
| 150° | 37.5 | 360° | 50.0 |
| 180° | 50.0 |
| Ref. [#] | λext [nm] | WD [cm] | Beam Width [cm2] | Pmax [mW] | Target Received Power [mW] | LED Quantity [ea] |
|---|---|---|---|---|---|---|
| This study | 405 | 18.0 | 6.50 | 200 | 10.9 | 1.00 (LED) |
| [32] | 550 | 56.75 | 5.72 | 7920 | 0.196 | 9.00 (LED) |
| [33] | 625 | 30.00 | 3.24 | 300,300 | 26.55 | 130 (LED) |
| [34] | 467 | 6.17 | 3.31 | 100 | 6.10 | 52 (LED) |
| [35] | 405 | 0.25 | 0.027 | 40.0 | 12.3 | 1.0 (laser) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seo, J.; Park, J.; Yoon, K.; Lee, S.; Kim, M.; Ryu, S.Y.; Kim, K.G. Optical Methods for Optimizing Fluorescence Imaging Field of View and Image Quality in Surgical Guidance Procedures. Diagnostics 2024, 14, 1996. https://doi.org/10.3390/diagnostics14171996
Seo J, Park J, Yoon K, Lee S, Kim M, Ryu SY, Kim KG. Optical Methods for Optimizing Fluorescence Imaging Field of View and Image Quality in Surgical Guidance Procedures. Diagnostics. 2024; 14(17):1996. https://doi.org/10.3390/diagnostics14171996
Chicago/Turabian StyleSeo, Jeongmin, Jina Park, Kicheol Yoon, Sangyun Lee, Minchan Kim, Seung Yeob Ryu, and Kwang Gi Kim. 2024. "Optical Methods for Optimizing Fluorescence Imaging Field of View and Image Quality in Surgical Guidance Procedures" Diagnostics 14, no. 17: 1996. https://doi.org/10.3390/diagnostics14171996