

The Role of the Basophil Activation Test in the Diagnosis of Drug-Induced Anaphylaxis

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
- Group 1 with indications for allergy diagnosis before administering the COVID-19 vaccine selected from among DIA patients due to COVID-19 pandemic context (history of anaphylactic reaction to the vaccine, history of hypersensitivity to polyethylene glycol (PEG), and hypersensitivity to many drugs from various chemical groups),
- Group 2 with indications for the diagnosis of allergies to other drugs,
- Group 3 with no indications for the diagnosis of drug allergies. This was a group of patients referred with a suspected vaccine allergy—due to adverse reactions after vaccination or an incriminating allergy history.
Statistical Analysis
3. Results
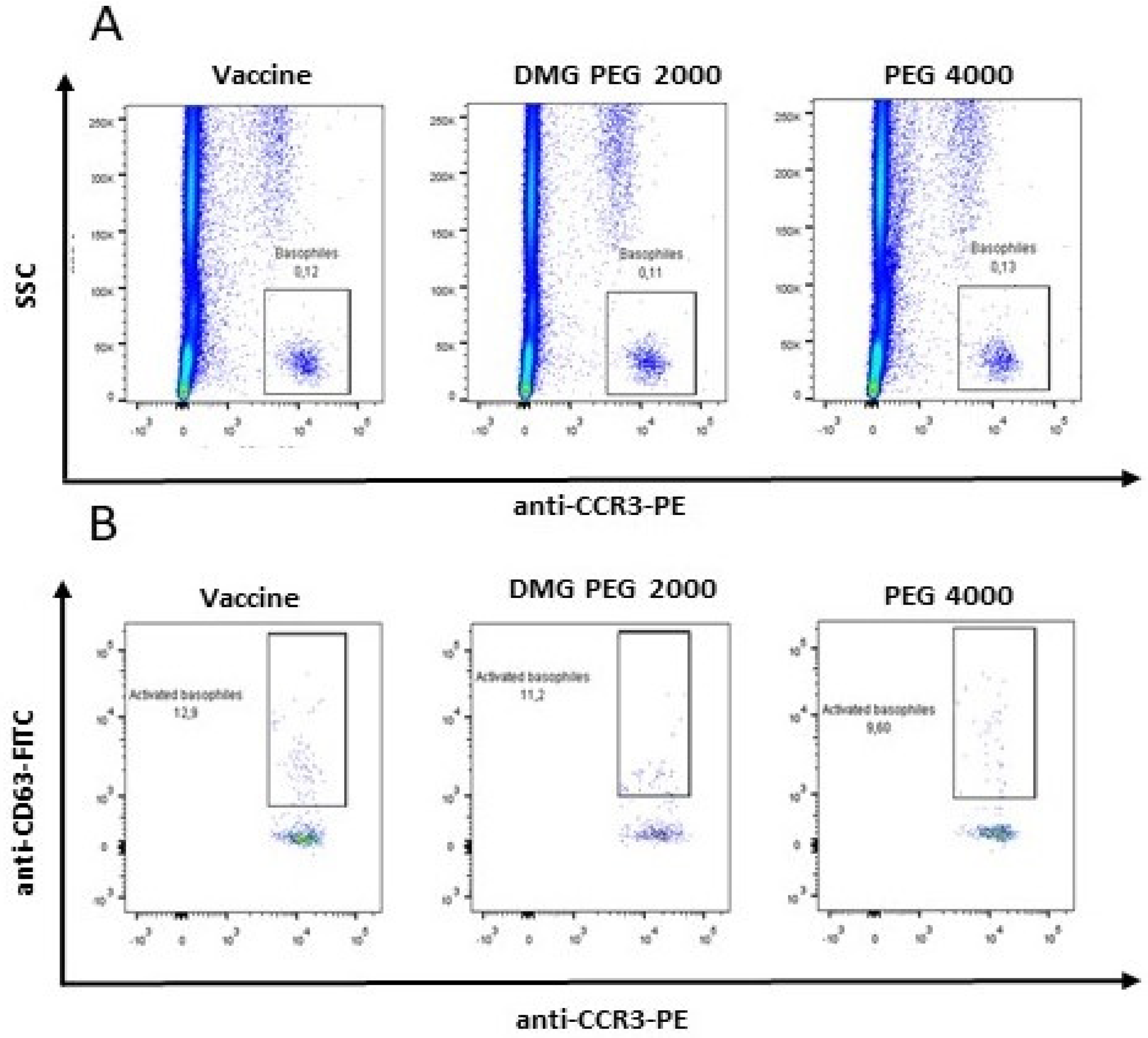
3.1. Patient 1
3.2. Patient 2
- with the percentage of activated basophils for DMG-PEG 2000, there is a statistically significant positive correlation, r = 0.488801; p = 0.0395,
- with SI for DMG-PEG 2000, there is a statistically significant positive correlation, r = 0.519732; p = 0.0271,
- with the percentage of activated basophils for PEG 4000, there is a statistically significant positive correlation, r = 0.636658; p = 0.0478,
- with SI for PEG 4000, there is a statistically significant positive correlation, r = 0.729909; p = 0.0166,
- with the percentage of activated basophils for the vaccine, there is a statistically significant positive correlation, r = 0.766223; p = 0.0160,
- with SI for the vaccine, there is a significant positive correlation r = 0.632157; p = 0.0678.
3.3. BAT in the Diagnosis of DIA with Other Drugs
4. Discussion
4.1. Clinical Characteristics of the Study Population
4.2. Symptom Profile of DIA
4.3. The Role of the BAT in the Qualification for Vaccination against COVID-19
4.4. The Usefulness of BAT in the Diagnosis of DIA after Other Drugs
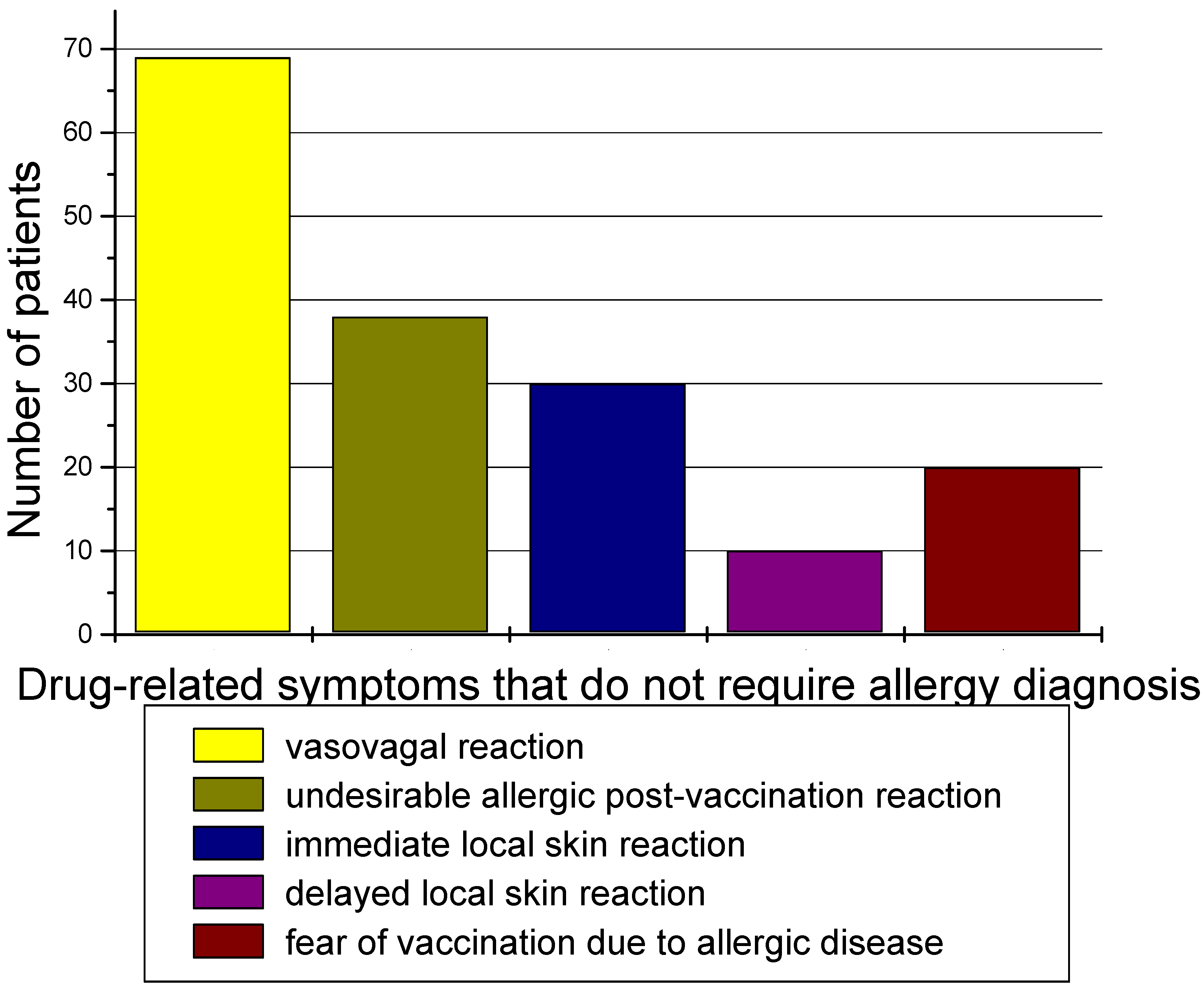
4.5. Patients with No Indications for a Drug Allergy Diagnosis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cardona, V.; Ansotegui, I.J.; Ebisawa, M.; El-Gamal, Y.; Fernandez Rivas, M.; Fineman, S.; Geller, M.; Gonzalez-Estrada, A.; Greenberger, P.A.; Sanchez Borges, M.; et al. World allergy organization anaphylaxis guidance 2020. World Allergy Organ. J. 2020, 13, 100472. [Google Scholar] [CrossRef] [PubMed]
- Muraro, A.; Worm, M.; Alviani, C.; Cardona, V.; DunnGalvin, A.; Garvey, L.H.; Riggioni, C.; de Silva, D.; Angier, E.; Arasi, S.; et al. EAACI guidelines: Anaphylaxis (2021 update). Allergy 2022, 77, 357. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Pérez, R.; de las Vecillas, L.; Cabañas, R.; Bellón, T. Tools for Etiologic Diagnosis of Drug-Induced Allergic Conditions. Int. J. Mol. Sci. 2023, 24, 12577. [Google Scholar] [CrossRef] [PubMed]
- Blazowski, L.; Majak, P.; Kurzawa, R.; Kuna, P.; Jerzynska, J. A severity grading system of food-induced acute allergic reactions to avoid the delay of epinephrine administration. Ann. Allergy Asthma Immunol. 2021, 127, 462. [Google Scholar] [CrossRef]
- Ring, J.; Messmer, K. Incidence and severity of anaphylactoid reactions to colloid volume substitutes. Lancet 1977, 1, 466. [Google Scholar] [CrossRef]
- Pallardy, M.; Bechara, R.; Whritenour, J.; Mitchell-Ryan, S.; Herzyk, D.; Lebrec, H.; Merk, H.; Gourley, I.; Komocsar, W.J.; Piccotti, J.R.; et al. Drug hypersensitivity reactions: Review of the state of the science for prediction and diagnosis. Toxicol. Sci. 2024, 200, 11–30. [Google Scholar] [CrossRef]
- Castells, M. Diagnosis and management of anaphylaxis in precision medicine. J. Allergy Clin. Immunol. 2017, 140, 321. [Google Scholar] [CrossRef]
- Santos, A.F.; Alpan, O.; Hoffmann, H.J. Basophil activation test: Mechanisms and considerations for use in clinical trials and clinical practice. Allergy 2021, 76, 2420. [Google Scholar] [CrossRef]
- Bahri, R.; Custovic, A.; Korosec, P.; Tsoumani, M.; Barron, M.; Wu, J.; Sayers, R.; Weimann, A.; Ruiz-Garcia, M.; Patel, N.; et al. Mast cell activation test in the diagnosis of allergic disease and anaphylaxis. J. Allergy Clin. Immunol. 2018, 142, 485–496.e16. [Google Scholar] [CrossRef]
- CDC. Interim Clinical Considerations for Use of COVID-19 Vaccines Currently Approved or Authorized in the United States 2021. Available online: https://www.cdc.gov/vaccines/covid-19/clinical-considerations/covid-19-vaccines-us.html (accessed on 1 April 2024).
- Bujang, M.A. An elaboration on sample size determination for correlations based on effect sizes and confidence interval width: A guide for researchers. Restor. Dent. Endod. 2024, 49, e21. [Google Scholar] [CrossRef]
- Hanschmann, T.; Francuzik, W.; Dölle-Bierke, S.; Hofmeier, K.S.; Grabenhenrich, L.; Ruëff, F.; Renaudin, J.M.; Pföhler, C.; Treudler, R.; Bilò, M.B.; et al. Different phenotypes of drug-induced anaphylaxis-Data from the European Anaphylaxis Registry. Allergy 2023, 78, 1615. [Google Scholar] [CrossRef] [PubMed]
- Koumaki, D.; Gregoriou, S.; Evangelou, G.; Katoulis, A.; Papadakis, M.; Krueger-Krasagakis, S.E.; Doxastaki, A.; Mylonakis, D.; Krasagakis, K. Real-Life Utility of Basophil Activation Test in the Diagnosis of Immediate Hypersensitivity Drug Reactions. Dermatol. Ther. 2023, 13, 3229. [Google Scholar] [CrossRef] [PubMed]
- Furman, K.; Kasprzyk-Wieczorkowska, E.; Glück, J.; Gawlik, R. Bezpieczeństwo szczepienia przeciw COVID-19 wśród pacjentów po przebytych reakcjach alergicznych. Alergol. Pol. Pol. J. Allergol. 2023, 10, 41. [Google Scholar] [CrossRef]
- Barbaud, A.; Garvey, L.H.; Arcolaci, A.; Brockow, K.; Mori, F.; Mayorga, C.; Bonadonna, P.; Atanaskovic-Markovic, M.; Moral, L.; Zanoni, G.; et al. Allergies and COVID-19 vaccines: An ENDA/EAACI Position paper. Allergy 2022, 77, 2292. [Google Scholar] [CrossRef] [PubMed]
- Kruszewski, J.; Cichocka-Jarosz, E.; Czarnobilska, E.; Jutel, M.; Kulus, M.; Kuna, P.; Kupczyk, M.; Niedoszytko, M.; Nittner-Marszalska, M.; Pałczyński, C.; et al. Rekomendacje Polskiego Towarzystwa Alergologicznego dotyczące kwalifikacji osób z alergią i anafilaksją do szczepienia przeciw COVID-19. Alergol. Pol. Pol. J. Allergol. 2021, 8, 1. [Google Scholar] [CrossRef]
- Blumenthal, K.G.; Robinson, L.B.; Camargo, C.A.; Shenoy, E.S.; Banerji, A.; Landman, A.B.; Wickner, P. Acute allergic reactions to mRNA COVID-19 vaccines. JAMA 2021, 325, 1562. [Google Scholar] [CrossRef]
- Czarnobilska, M.; Bulanda, M.; Kurnik-Łucka, M.; Gil, K. Hypersensitivity to polyethylene glycol (PEG). Folia Med. Cracov. 2021, 61, 55. [Google Scholar] [CrossRef]
- Sellaturay, P.; Nasser, S.; Ewan, P. Polyethylene Glycol-Induced Systemic Allergic Reactions (Anaphylaxis). Allergy Clin. Immunol. Pract. 2021, 9, 670. [Google Scholar] [CrossRef]
- Warren, C.M.; Snow, T.T.; Lee, A.S.; Shah, M.M.; Heider, A.; Blomkalns, A.; Betts, B.; Buzzanco, A.S.; Gonzalez, J.; Chinthrajah, R.S.; et al. Assessment of allergic and anaphylactic reactions to mRNA COVID-19 vaccines with confirmatory testing in a US regional health system. JAMA Netw. Open 2021, 4, e2125524. [Google Scholar] [CrossRef] [PubMed]
- Eberlein, B.; Mathes, S.; Fischer, J.; Darsow, U.; Biedermann, T.; Brockow, K. Do basophil activation tests help elucidate allergic reactions to the ingredients in COVID-19 vaccines? Allergy 2022, 77, 2924. [Google Scholar] [CrossRef]
- Brockow, K.; Mathes, S.; Fischer, J.; Volc, S.; Darsow, U.; Eberlein, B.; Biedermann, T. Experience with polyethylene glycol allergy-guided risk management for COVID-19 vaccine anaphylaxis. Allergy 2022, 77, 2200. [Google Scholar] [CrossRef]
- Labella, M.; Céspedes, J.A.; Doña, I.; Shamji, M.H.; Agache, I.; Mayorga, C.; Torres, M.J. The value of the basophil activation test in the evaluation of patients reporting allergic reactions to the BNT162b2 mRNA COVID-19 vaccine. Allergy 2022, 77, 2067. [Google Scholar] [CrossRef]
- Vespa, S.; Del Biondo, P.; Simeone, P.; Cavallucci, E.; Catitti, G.; Auciello, R.; De Bellis, D.; Altomare, I.; Pierdomenico, L.; Canonico, B.; et al. Basophil Activation Test with Different Polyethylene Glycols in Patients with Suspected PEG Hypersensitivity Reactions. Int. J. Mol. Sci. 2022, 23, 14592. [Google Scholar] [CrossRef]
- Restivo, V.; Candore, G.; Barrale, M.; Caravello, E.; Graziano, G.; Onida, R.; Raineri, M.; Tiralongo, S.; Brusca, I. Allergy to polyethylene glycol of anti-SARS CoV2 vaccine recipient: A case report of young adult recipient and the management of future exposure to SARS-CoV2. Vaccines 2021, 9, 412. [Google Scholar] [CrossRef]
- Kwok, M.; Lack, G.; Santos, A.F. Improved standardisation of the whole blood basophil activation test to peanut. Clin. Transl. Allergy 2017, 8 (Suppl. S2), 15–16. [Google Scholar]
- Sturm, G.J.; Kranzelbinder, B.; Sturm, E.M.; Heinemann, A.; Groselj-Strele, A.; Aberer, W. The basophil activation test in the diagnosis of allergy: Technical issues and critical factors. Allergy 2009, 64, 1319–1326. [Google Scholar] [CrossRef]
- Adkinson, N.F. A guide to skin testing for penicillin allergy. Med. Times 1976, 104, 164. [Google Scholar]
- Jeimy, S.; Ben-Shoshan, M.; Abrams, E.M.; Ellis, A.K.; Connors, L.; Wong, T. Practical guide for evaluation and management of beta-lactam allergy: Position statement from the Canadian Society of Allergy and Clinical Immunology. Allergy Asthma Clin. Immunol. 2020, 16, 95. [Google Scholar] [CrossRef]
- Chiriac, A.M.; Vasconcelos, M.J.; Izquierdo, L.; Ferrando, L.; Nahas, O.; Demoly, P. To challenge or not to challenge: Literature data on the positive predictive value of skin tests to beta-lactams. J. Allergy Clin. Immunol. Pract. 2019, 7, 2404. [Google Scholar] [CrossRef]
- Torres, M.J.; Padial, A.; Mayorga, C.; Fernandez, T.; Sanchez-Sabate, E.; Cornejo-Garcia, J.A.; Antunez, C.; Blanca, M. The diagnostic interpretation of basophil activation test in immediate allergic reactions to beta-lactams. Clin. Exp. Allergy 2004, 34, 1768. [Google Scholar] [CrossRef]
- Thinnes, A.; Merk, H.F.; Wurpts, G.; Röseler, S.; Lehmann, S.; Tenbrock, K.; Baron, J.M.; Balakirski, G. Individual risk assessment in the diagnosis of immediate type drug hypersensitivity reactions to betalactam and non-betalactam antibiotics using basophil activation test: A single center experience. Cutan. Ocul. Toxicol. 2018, 37, 309. [Google Scholar] [CrossRef] [PubMed]
- De Weck, A.L.; Sanz, M.L.; Gamboa, P.M.; Aberer, W.; Sturm, G.; Bilo, M.B.; Montroni, M.; Blanca, M.; Torres, M.J.; Mayorga, L.; et al. Diagnosis of immediate-type beta-lactam allergy in vitro by flowcytometric basophil activation test (BAT alias FLOW-CAST) and sulfidoleukotriene production (CAST-ELISA): A multicentric study. J. Investig. Allergol. Clin. Immunol. 2009, 19, 91. [Google Scholar]
- Uyttebroek, A.; Sabato, V.; Cop, N.; Decuyper, I.; Faber, M.; Bridts, C.; Mertens, C.; Hagendorens, M.; De Clerck, L.; Ebo, D. Diagnosing cefazolin hypersensitivity: Lessons from dual-labeling flow cytometry. J. Allergy Clin. Immunol. Pract. 2016, 4, 1243. [Google Scholar] [CrossRef] [PubMed]
- Céspedes, J.A.; Fernández-Santamaría, R.; Ariza, A.; Bogas, G.; Doña, I.; Rondón, C.; Salas, M.; Labella, M.; Frecha, C.; Mayorga, C.; et al. Diagnosis of immediate reactions to amoxicillin: Comparison of basophil activation markers CD63 and CD203c in a prospective study. Allergy 2023, 78, 2745. [Google Scholar] [CrossRef]
- Blumenthal, K.G.; Peter, J.G.; Trubiano, J.A.; Phillips, E.J. Antibiotic allergy. Lancet 2019, 393, 183. [Google Scholar] [CrossRef]
- Steiner, M.; Harrer, A.; Himly, M. Basophil Reactivity as Biomarker in Immediate Drug Hypersensitivity Reactions—Potential and Limitations. Front. Pharmacol. 2016, 7, 171. [Google Scholar] [CrossRef] [PubMed]
- Marraccini, P.; Pignatti, P.; D Apos Alcamo, A.; Salimbeni, R.; Consonni, D. Basophil Activation Test Application in Drug Hypersensitivity Diagnosis: An Empirical Approach. Int. Arch. Allergy Immunol. 2018, 177, 160. [Google Scholar] [CrossRef]
- Zuo, J.; Gong, R.; Liu, X.; Zhao, J. Risk of True Allergy to Local Anesthetics: 10-Year Experience from an Anesthesia Allergy Clinic in China. Ther. Clin. Risk Manag. 2020, 16, 1297–1303. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Age | Gender | Severity | BAT Vaccine | SPT Vaccine | IDT Vaccine | BAT PEG 2000 | BATPEG 4000 |
|---|---|---|---|---|---|---|---|---|
| 1 | 40 | F | III | + | - | + | + | + |
| 2 | 24 | F | III | - | - | - | + | + |
| Drug No. | Culprit Agent | Age | Gender | Severity R&M | BAT | SI | % of Activated Basophils | SPT | IDT |
|---|---|---|---|---|---|---|---|---|---|
| 1 | ciprofloxacin | 35 | M | I | + | 16 | 38.3 | nt | nt |
| 2 | penicillin | 42 | F | III | + | 70 | 28.1 | nt | nt |
| 3 | ampicillin | 31 | F | III | + | 65 | 26.1 | nt | nt |
| 4 | penicillin | 49 | M | III | + | 5.3 | 11.7 | nt | nt |
| 5 | cefuroxime | 68 | F | III | + | 13.1 | 26.2 | - | + |
| 6 | clarithromycin | 46 | F | II | + | 22.6 | 11.3 | nt | nt |
| 7 | amoxicillin | 36 | F | III | + | 140.4 | 70.2 | nt | nt |
| 8 | penicillin | 68 | F | III | + | 56.2 | 28.1 | nt | nt |
| 9 | ampicillin | 42 | F | III | + | 52.2 | 26.1 | nt | nt |
| 10 | amoxicillin + clavulanic acid | 46 | F | III | + | 17.65 | 70.6 | - | + |
| 11 | cefuroxime | 64 | F | II | + | 13.1 | 26.2 | - | + |
| 12 | amoxicillin + clavulanic acid | 31 | F | II | + | 2.2 | 6.5 | nt | nt |
| 13 | cefuroxime | 31 | F | III | + | 2.1 | 6.2 | nt | nt |
| 14 | penicillin | 19 | M | III | + | 2 | 6.9 | nt | nt |
| 15 | ibuprofen | 23 | M | II | + | 3.6 | 13.6 | nt | nt |
| 16 | acetylsalicylic acid | 62 | F | II | + | 5.4 | 7.1 | nt | nt |
| 17 | lidocaine | 19 | F | II | + | 5.4 | 13.5 | nt | nt |
| 18 | lidocaine | 21 | F | II | + | 2.3 | 7.3 | nt | nt |
| 19 | lidocaine | 20 | F | II | + | 2.8 | 10 | nt | nt |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Czarnobilska, M.; Bulanda, M.; Czarnobilska, E.; Dyga, W.; Mazur, M. The Role of the Basophil Activation Test in the Diagnosis of Drug-Induced Anaphylaxis. Diagnostics 2024, 14, 2036. https://doi.org/10.3390/diagnostics14182036
Czarnobilska M, Bulanda M, Czarnobilska E, Dyga W, Mazur M. The Role of the Basophil Activation Test in the Diagnosis of Drug-Induced Anaphylaxis. Diagnostics. 2024; 14(18):2036. https://doi.org/10.3390/diagnostics14182036
Chicago/Turabian StyleCzarnobilska, Maria, Małgorzata Bulanda, Ewa Czarnobilska, Wojciech Dyga, and Marcel Mazur. 2024. "The Role of the Basophil Activation Test in the Diagnosis of Drug-Induced Anaphylaxis" Diagnostics 14, no. 18: 2036. https://doi.org/10.3390/diagnostics14182036
APA StyleCzarnobilska, M., Bulanda, M., Czarnobilska, E., Dyga, W., & Mazur, M. (2024). The Role of the Basophil Activation Test in the Diagnosis of Drug-Induced Anaphylaxis. Diagnostics, 14(18), 2036. https://doi.org/10.3390/diagnostics14182036