
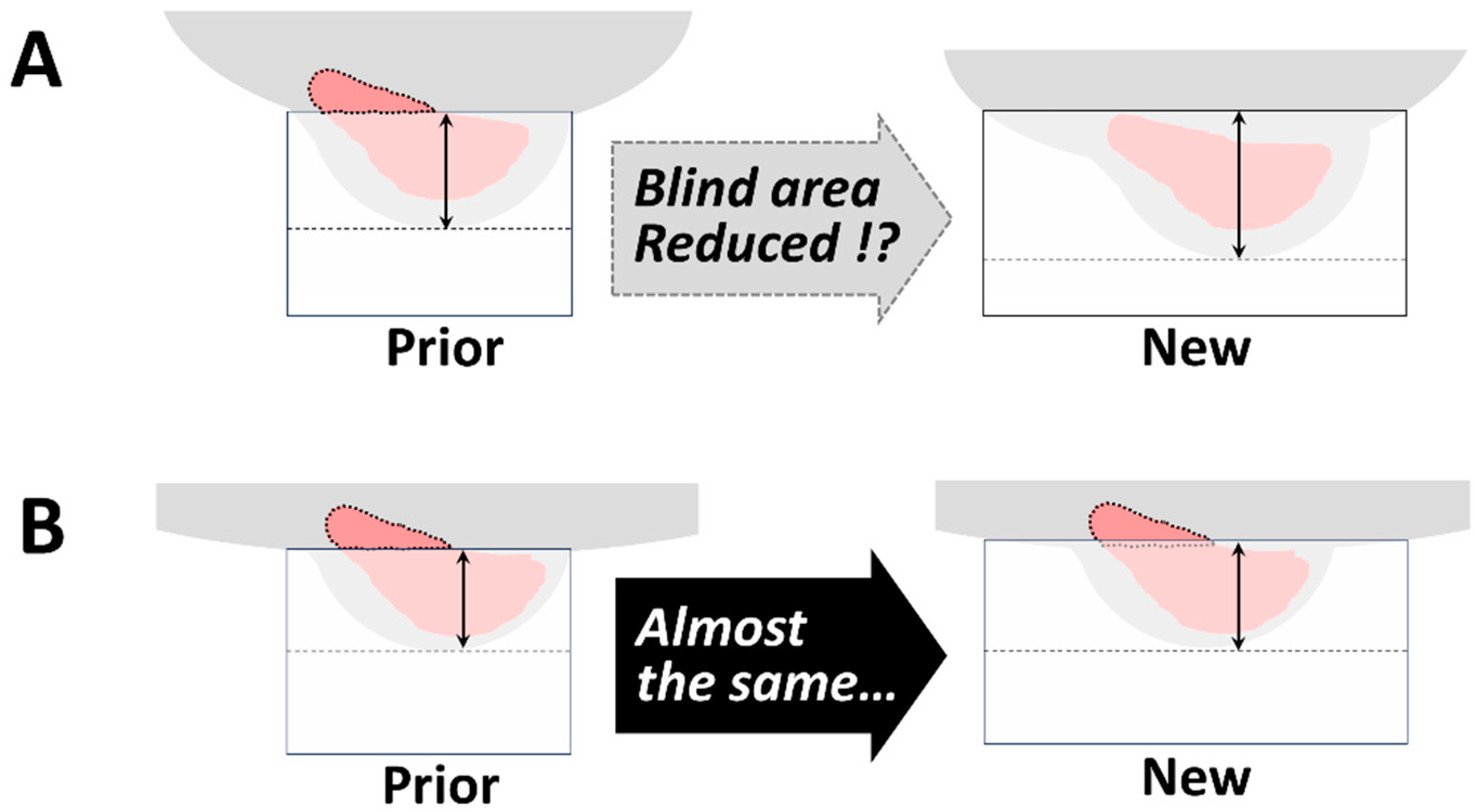
Can the Newer Model of Breast-Specific Positron Emission Tomography Reduce the “Blind Area”?

 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Old and New dbPET Scanners
2.2. Patients
2.3. Imaging Protocol
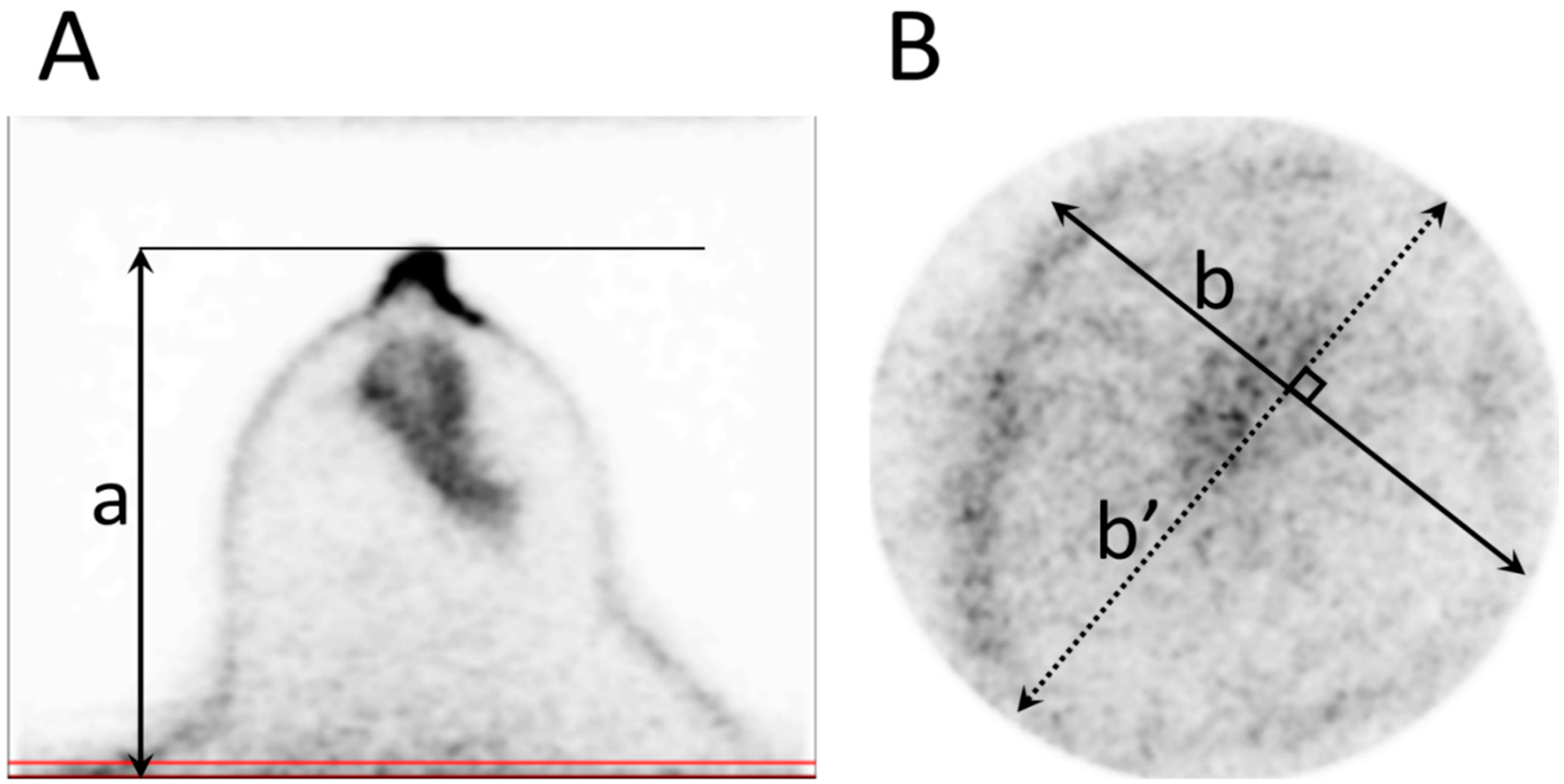
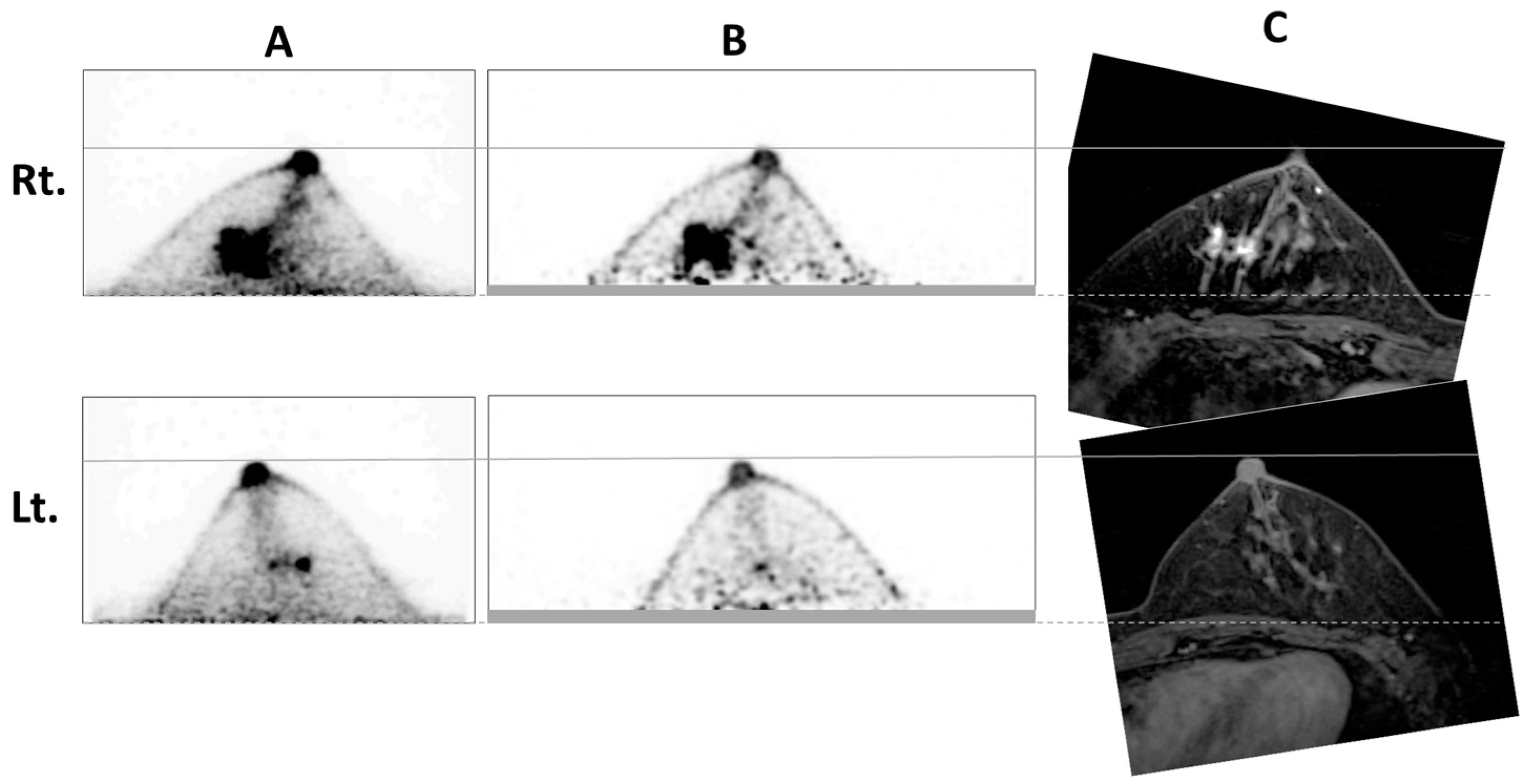
2.4. Image Analysis
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Miyake, K.K.; Matsumoto, K.; Inoue, M.; Nakamoto, Y.; Kanao, S.; Oishi, T.; Kawase, S.; Kitamura, K.; Yamakawa, Y.; Akazawa, A.; et al. Performance evaluation of a new dedicated breast PET scanner using NEMA NU4-2008 standards. J. Nucl. Med. 2014, 55, 1198–1203. [Google Scholar] [CrossRef] [PubMed]
- Satoh, Y.; Motosugi, U.; Imai, M.; Onishi, H. Comparison of dedicated breast positron emission tomography and whole-body positron emission tomography/computed tomography images: A common phantom study. Ann. Nucl. Med. 2020, 34, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, R.; Akashi-Tanaka, S.; Watanabe, C.; Masuda, H.; Taruno, K.; Takamaru, T.; Ide, Y.; Kuwayama, T.; Kobayashi, Y.; Takimoto, M.; et al. Diagnostic performance of dedicated breast positron emission tomography. Breast Cancer 2022, 29, 1013–1021. [Google Scholar] [CrossRef] [PubMed]
- Berg, W.; Madsen, K.S.; Schilling, K.; Tartar, M.; Pisano, E.D.; Larsen, L.H.; Narayanan, D.; Ozonoff, A.; Miller, J.P.; Kalinyak, J.E. Breast cancer: Comparative effectiveness of positron emission mammography and MR imaging in presurgical planning for the ipsilateral breast. Radiology 2011, 258, 59–72. [Google Scholar] [CrossRef] [PubMed]
- Satoh, Y.; Motosugi, U.; Omiya, Y.; Onishi, H. Unexpected abnormal uptake in the breasts at dedicated breast PET: Incidentally detected small cancers or nonmalignant features? AJR Am. J. Roentgenol. 2019, 212, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Noritake, M.; Narui, K.; Kaneta, T.; Sugae, S.; Sakamaki, K.; Inoue, T.; Ishikawa, T. Evaluation of the response to breast Cancer neoadjuvant chemotherapy using 18F-FDG positron emission mammography compared with whole-body 18F-FDG PET: A prospective observational study. Clin. Nucl. Med. 2017, 42, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Diwanji, D.; Onishi, N.; Hathi, D.K.; Lawhn-Heath, C.; Kornak, J.; Li, W.; Guo, R.; Molina-Vega, J.; Seo, Y.; Flavell, R.R.; et al. 18F-FDG dedicated breast PET complementary to breast MRI for evaluating early response to neoadjuvant chemotherapy. Radiol. Imaging Cancer 2024, 6, e230082. [Google Scholar] [CrossRef] [PubMed]
- Koyasu, H.; Goshima, S.; Noda, Y.; Nishibori, H.; Takeuchi, M.; Matsunaga, K.; Yamada, T.; Matsuo, M. The feasibility of dedicated breast PET for the assessment of residual tumor after neoadjuvant chemotherapy. Jpn. J. Radiol. 2019, 37, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Tokuda, Y.; Yanagawa, M.; Fujita, Y.; Honma, K.; Tanei, T.; Shimoda, M.; Miyake, T.; Naoi, Y.; Kim, S.J.; Shimazu, K.; et al. Prediction of pathological complete response after neoadjuvant chemotherapy in breast cancer: Comparison of diagnostic performances of dedicated breast PET, whole-body PET, and dynamic contrast-enhanced MRI. Breast Cancer Res. Treat. 2021, 188, 107–115. [Google Scholar] [CrossRef]
- Satoh, Y.; Imai, M.; Ikegawa, C.; Hirata, K.; Abo, N.; Kusuzaki, M.; Oyama-Manabe, N.; Onishi, H. Effect of radioactivity outside the field of view on image quality of dedicated breast positron emission tomography: Preliminary phantom and clinical studies. Ann. Nucl. Med. 2022, 36, 1010–1018. [Google Scholar]
- Satoh, Y.; Motosugi, U.; Imai, M.; Omiya, Y.; Onishi, H. Evaluation of image quality at the detector’s edge of dedicated breast positron emission tomography. EJNMMI Phys. 2021, 8, 5. [Google Scholar] [CrossRef]
- Ishii, K.; Hanaoka, K.; Watanabe, S.; Morimoto-Ishikawa, D.; Yamada, T.; Kaida, H.; Yamakawa, Y.; Minagawa, S.; Takenouchi, S.; Ohtani, A.; et al. High-resolution silicon photomultiplier time-of-flight dedicated head PET system for clinical brain studies. J. Nucl. Med. 2023, 64, 153–158. [Google Scholar] [CrossRef] [PubMed]
- Satoh, Y.; Hanaoka, K.; Ikegawa, C.; Imai, M.; Watanabe, S.; Morimoto-Ishikawa, D.; Onishi, H.; Ito, T.; Komoike, Y.; Ishii, K. Organ-specific positron emission tomography scanners for breast imaging: Comparison between the performances of prior and novel models. Diagnostics 2023, 13, 1079. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, E.; Kudo, H. Subset-dependent relaxation in block-iterative algorithms for image reconstruction in emission tomography. Phys. Med. Biol. 2003, 48, 1405–1422. [Google Scholar] [CrossRef] [PubMed]
- Shimoi, T.; Nagai, S.E.; Yoshinami, T.; Takahashi, M.; Arioka, H.; Ishihara, M.; Kikawa, Y.; Koizumi, K.; Kondo, N.; Sagara, Y.; et al. The Japanese Breast Cancer Society Clinical Practice Guidelines for Breast Cancer 2018. Breast Cancer 2020, 27, 322–331. (In Japanese) [Google Scholar] [CrossRef] [PubMed]
- Miyake, K.K.; Kataoka, M.; Ishimori, T.; Matsumoto, Y.; Torii, M.; Takada, M.; Satoh, Y.; Kubota, K.; Satake, H.; Yakami, M.; et al. A proposed dedicated breast PET lexicon: Standardization of description and reporting of radiotracer uptake in the breast. Diagnostics 2021, 11, 1267. [Google Scholar] [CrossRef] [PubMed]
- Satoh, Y.; Kawamoto, M.; Kubota, K.; Murakami, K.; Hosono, M.; Senda, M.; Sasaki, M.; Momose, T.; Ito, K.; Okamura, T.; et al. Clinical practice guidelines for high-resolution breast PET, 2019 edition. Ann. Nucl. Med. 2021, 35, 406–414. [Google Scholar] [CrossRef] [PubMed]
- Yanai, A.; Itoh, M.; Hirakawa, H.; Yanai, K.; Tashiro, M.; Harada, R.; Yoshikawa, A.; Yamamoto, S.; Ohuchi, N.; Ishida, T. Newly-developed positron emission mammography (PEM) device for the detection of small breast Cancer. Tohoku J. Exp. Med. 2018, 245, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Yano, F.; Itoh, M.; Hirakawa, H.; Yamamoto, S.; Yoshikawa, A.; Hatazawa, J. Diagnostic accuracy of positron emission mammography with 18F-fluorodeoxyglucose in breast cancer tumor of less than 20 mm in size. Asia Ocean. J. Nucl. Med. Biol. 2019, 7, 13–21. [Google Scholar] [PubMed]
- Nassar, L.; Kassas, M.; Abi-Ghanem, A.S.; El-Jebai, M.; Al-Zakleet, S.; Baassiri, A.S.; Naccoul, R.A.; Barakat, A.; Tfayli, A.; Assi, H.; et al. Prone versus supine FDG PET/CT in the staging of breast cancer. Diagnostics 2023, 13, 367. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Satoh, Y.; Ishida, J.; Inui, Y.; Takenaka, A.; Bando, S.; Ishida, S.; Toyama, H. Can the Newer Model of Breast-Specific Positron Emission Tomography Reduce the “Blind Area”? Diagnostics 2024, 14, 2068. https://doi.org/10.3390/diagnostics14182068
Satoh Y, Ishida J, Inui Y, Takenaka A, Bando S, Ishida S, Toyama H. Can the Newer Model of Breast-Specific Positron Emission Tomography Reduce the “Blind Area”? Diagnostics. 2024; 14(18):2068. https://doi.org/10.3390/diagnostics14182068
Chicago/Turabian StyleSatoh, Yoko, Jiro Ishida, Yoshitaka Inui, Akinori Takenaka, Shuji Bando, Sayuri Ishida, and Hiroshi Toyama. 2024. "Can the Newer Model of Breast-Specific Positron Emission Tomography Reduce the “Blind Area”?" Diagnostics 14, no. 18: 2068. https://doi.org/10.3390/diagnostics14182068