

Diagnosing and Treating IgAN: Steroids, Budesonide, or Maybe Both?

 , ,
, ,
Abstract
:1. Introduction
2. Pathogenesis of IgA Nephropathy
3. Treatment Options in IgAN
3.1. Non-Immunological Treatment
3.2. Immunological Treatment
3.2.1. Systemic Steroids
3.2.2. Other Immunosuppressive Therapies
4. Mechanism of Action of Immune Treatment Modalities
4.1. Systemic Steroids: Mechanism of Action in IgAN
4.2. Budesonide: Mechanism of Action in IgAN
4.3. Similarities and Differences between Targeted-Release Budesonide and Systemic Corticosteroids
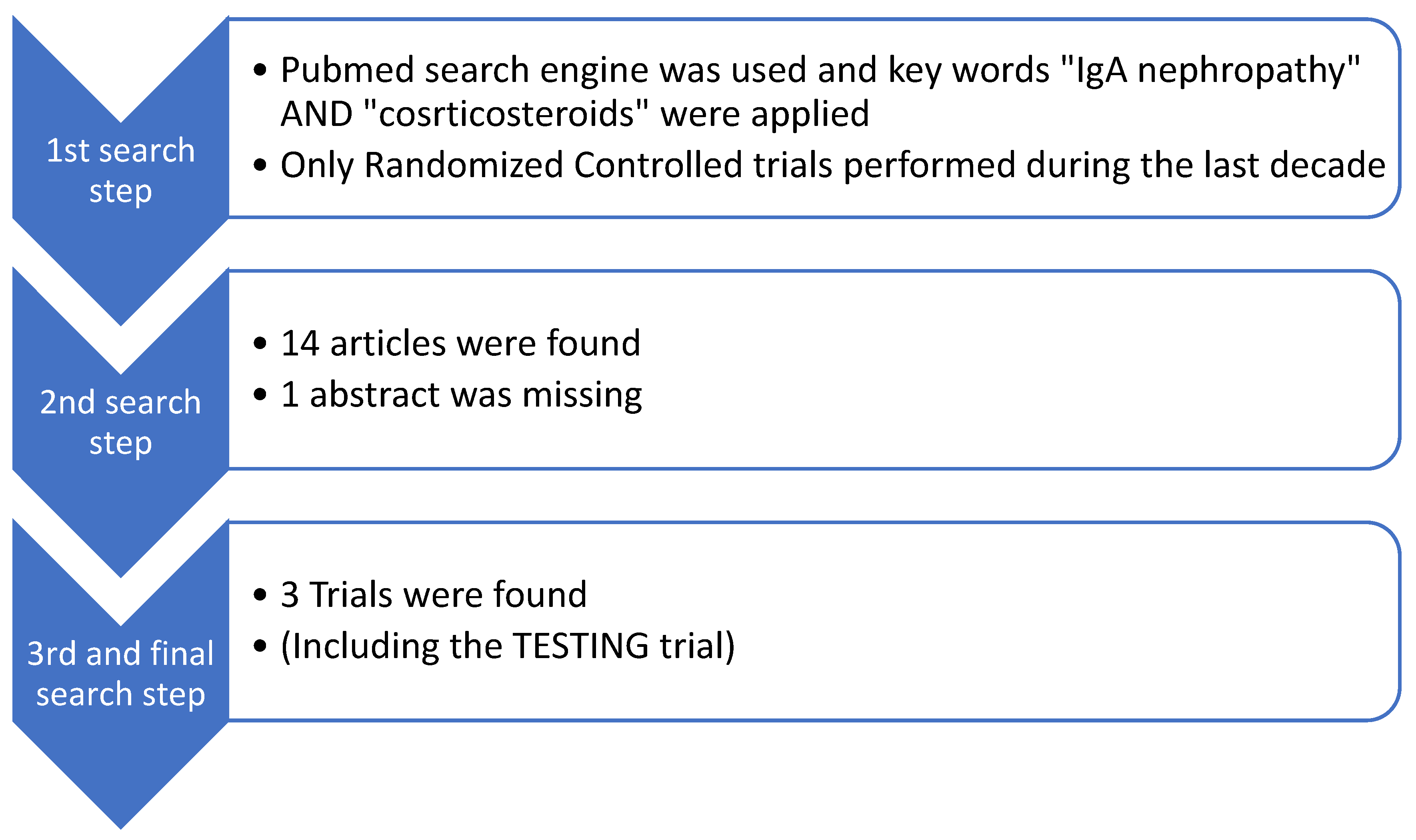
5. Recent Clinical Trials
5.1. Systemic Steroid Treatment
5.2. Targeted-Release Budesonide
- ≥18 years old, >500 mg/day of albuminuria (U-albumin)and <200 μmol/L of serum creatinine (S-creatinine) [39];
- ≥18 years old, eGFR of at least 45 mL/min/1.73 m2 and a urine protein–creatinine ratio (UPCR) of more than 0.5 g/g or at least 0.75 g/day of urinary total protein [48];
- Patients aged ≥ 18 years, estimated glomerular filtration rate (eGFR) of 35–90 mL/min/1.73 m2 and persistent proteinuria (urine protein–creatinine ratio ≥ 0.8 g/g or proteinuria ≥ 1 g/24 h) despite optimized renin–angiotensin system blockade [49].
- Uncontrolled blood pressure defined as a systolic blood pressure of ≥160 mmHg and/or diastolic blood pressure of ≥100 mmHg, hyperlipidemia, introduction of an ACE inhibitor, ARB, or other blood pressure-lowering substance within the first 3 months, treatment with immunosuppressive or systemic corticosteroid agents, intake of CYP3A4 inhibitors (including grapefruit juice), severe liver disease, uncontrolled (treated or untreated) congestive heart failure, history of malignancies during the last 3 years, history or presence of psychological or psychiatric illness present, alcohol or drug abuse, intake of other investigational drug within 30 days prior to enrolment [39].
- Less than 18 years old, secondary IgAN, eGFR below 20 mL/min/1.73 m2, nephrotic syndrome, rapidly progressive clinical course, less than 0.5 g/d of proteinuria after adequate RAAS blockade, severe histologic lesions of activity or chronicity (endocapillary hypercellularity in over 50% of examined glomeruli, crescents in over 30% of examined glomeruli, presence of fibrinoid necrosis, global glomerulosclerosis in over 50% of examined glomeruli), patients with diabetes mellitus or active infections, patients who received prior immunosuppression [48].
6. Benefits and Disadvantages
7. Our Recommendation
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Intercapillary deposits of IgA-IgC: [Berger J, Hinglais N: J. Urol. Nephrol. (Paris) 74:694–695, 1968 (with comments by Liliane Striker)]. J. Am. Soc. Nephrol. 2000, 11, 1957–1959. Available online: https://journals.lww.com/jasn/pages/articleviewer.aspx?year=2000&issue=10000&article=00022&type=Fulltext (accessed on 20 November 2023). [CrossRef] [PubMed]
- D’Amico, G. The commonest glomerulonephritis in the world: IgA nephropathy. Q. J. Med. 1987, 64, 709–727. [Google Scholar] [PubMed]
- Knoppova, B.; Reily, C.; King, R.G.; Julian, B.A.; Novak, J.; Green, T.J. Pathogenesis of IgA Nephropathy: Current Understanding and Implications for Development of Disease-Specific Treatment. J. Clin. Med. 2021, 10, 4501. [Google Scholar] [CrossRef]
- Lai, K.N.; Tang, S.C.W.; Schena, F.P.; Novak, J.; Tomino, Y.; Fogo, A.B.; Glassock, R.J. IgA nephropathy. Nat. Rev. Dis. Primers 2016, 2, 16001. [Google Scholar] [CrossRef] [PubMed]
- de Sousa-Pereira, P.; Woof, J.M. IgA: Structure, Function, and Developability. Antibodies 2019, 8, 57. [Google Scholar] [CrossRef] [PubMed]
- Immunoglobulin A—An Overview|ScienceDirect Topics. Available online: https://www.sciencedirect.com/topics/immunology-and-microbiology/immunoglobulin-a (accessed on 20 November 2023).
- Boyd, J.K.; Cheung, C.K.; Molyneux, K.; Feehally, J.; Barratt, J. An update on the pathogenesis and treatment of IgA nephropathy. Kidney Int. 2012, 81, 833–843. [Google Scholar] [CrossRef] [PubMed]
- Woof, J.M.; Russell, M.W. Structure and function relationships in IgA. Mucosal Immunol. 2011, 4, 590–597. [Google Scholar] [CrossRef]
- Gesualdo, L.; Di Leo, V.; Coppo, R. The mucosal immune system and IgA nephropathy. Semin. Immunopathol. 2021, 43, 657–668. [Google Scholar] [CrossRef]
- Delves, P.J.; Roitt, I.M. (Eds.) Encyclopedia of Immunology, 2nd ed.; Academic Press: San Diego, CA, USA, 1998. [Google Scholar]
- Allen, A.C.; Bailey, E.M.; Brenchley, P.E.; Buck, K.S.; Barratt, J.; Feehally, J. Mesangial IgA1 in IgA nephropathy exhibits aberrant O-glycosylation: Observations in three patients. Kidney Int. 2001, 60, 969–973. [Google Scholar] [CrossRef]
- Floege, J.; Rauen, T.; Tang, S.C.W. Current treatment of IgA nephropathy. Semin. Immunopathol. 2021, 43, 717–728. [Google Scholar] [CrossRef]
- Habas, E.; Ali, E.M.; Farfar, K.; Errayes, M.; Alfitori, J.M.; Habas, E.M.; Ghazouani, H.M.; Akbar, R.M.; Khan, F.; Al Dab, A.; et al. IgA nephropathy pathogenesis and therapy: Review & updates. Medicine 2022, 101, e31219. [Google Scholar] [CrossRef] [PubMed]
- Rovin, B.H.; Adler, S.G.; Barratt, J.; Bridoux, F.; Burdge, K.A.; Chan, T.M.; Cook, H.T.; Fervenza, F.C.; Gibson, K.L.; Glassock, R.J.; et al. KDIGO 2021 Clinical Practice Guideline for the Management of Glomerular Diseases. Kidney Int. 2021, 100, S1–S276. [Google Scholar] [CrossRef] [PubMed]
- Wheeler, D.C.; Stefánsson, B.V.; Jongs, N.; Chertow, G.M.; Greene, T.; Hou, F.F.; McMurray, J.J.V.; Correa-Rotter, R.; Rossing, P.; Toto, R.D.; et al. Effects of dapagliflozin on major adverse kidney and cardiovascular events in patients with diabetic and non-diabetic chronic kidney disease: A prespecified analysis from the DAPA-CKD trial. Lancet Diabetes Endocrinol. 2021, 9, 22–31. [Google Scholar] [CrossRef] [PubMed]
- Barratt, J.; Floege, J. SGLT-2 inhibition in IgA nephropathy: The new standard of care? Kidney Int. 2021, 100, 24–26. [Google Scholar] [CrossRef] [PubMed]
- Floege, J. Antimalarials in IgA Nephropathy: Did Our Supportive Therapy Armamentarium Just Increase? Am. J. Kidney Dis. 2019, 74, 6–8. [Google Scholar] [CrossRef]
- Rauen, T.; Floege, J. Inflammation in IgA nephropathy. Pediatr. Nephrol. 2017, 32, 2215–2224. [Google Scholar] [CrossRef]
- Rauen, T.; Eitner, F.; Fitzner, C.; Sommerer, C.; Zeier, M.; Otte, B.; Panzer, U.; Peters, H.; Benck, U.; Mertens, P.R.; et al. Intensive Supportive Care plus Immunosuppression in IgA Nephropathy. N. Engl. J. Med. 2015, 373, 2225–2236. [Google Scholar] [CrossRef]
- Lv, J.; Zhang, H.; Chen, Y.; Li, G.; Jiang, L.; Singh, A.K.; Wang, H. Combination therapy of prednisone and ACE inhibitor versus ACE-inhibitor therapy alone in patients with IgA nephropathy: A randomized controlled trial. Am. J. Kidney Dis. 2009, 53, 26–32. [Google Scholar] [CrossRef]
- Yamamoto, R.; Nagasawa, Y.; Shoji, T.; Iwatani, H.; Hamano, T.; Kawada, N.; Inoue, K.; Uehata, T.; Kaneko, T.; Okada, N.; et al. Cigarette smoking and progression of IgA nephropathy. Am. J. Kidney Dis. 2010, 56, 313–324. [Google Scholar] [CrossRef]
- Katafuchi, R.; Ikeda, K.; Mizumasa, T.; Tanaka, H.; Ando, T.; Yanase, T.; Masutani, K.; Kubo, M.; Fujimi, S. Controlled, prospective trial of steroid treatment in IgA nephropathy: A limitation of low-dose prednisolone therapy. Am. J. Kidney Dis. 2003, 41, 972–983. [Google Scholar] [CrossRef]
- Lv, J.; Wong, M.G.; Hladunewich, M.A.; Jha, V.; Hooi, L.S.; Monaghan, H.; Zhao, M.; Barbour, S.; Jardine, M.J.; Reich, H.N.; et al. Effect of Oral Methylprednisolone on Decline in Kidney Function or Kidney Failure in Patients With IgA Nephropathy: The TESTING Randomized Clinical Trial. JAMA 2022, 327, 1888–1898. [Google Scholar] [CrossRef]
- Del Vecchio, L.; Rimoldi, C.; Pozzi, C. Nefecon (Targeted-Release Formulation-Budesonide) for the Treatment of IgA Nephropathy. Future Rare Dis. 2021, 1, FRD18. Available online: https://www.futuremedicine.com/doi/10.2217/frd-2021-0013 (accessed on 21 November 2023). [CrossRef]
- Liao, J.; Zhou, Y.; Xu, X.; Huang, K.; Chen, P.; Wu, Y.; Jin, B.; Hu, Q.; Chen, G.; Zhao, S. Current knowledge of targeted-release budesonide in immunoglobulin A nephropathy: A comprehensive review. Front. Immunol. 2022, 13, 926517. [Google Scholar] [CrossRef]
- Kobayashi, Y.; Fujii, K.; Hiki, Y.; Tateno, S. Steroid Therapy in IgA Nephropathy: A Prospective Pilot Study in Moderate Proteinuric Cases. QJM Int. J. Med. 1986, 61, 935–943. Available online: https://academic.oup.com/qjmed/article-abstract/61/1/935/1592449?redirectedFrom=PDF&login=false (accessed on 21 November 2023).
- Coppo, R. Corticosteroids in IgA Nephropathy: Lessons from Recent Studies. J. Am. Soc. Nephrol. 2017, 28, 25–33. [Google Scholar] [CrossRef]
- Vaerman, J.P. The secretory immune system. Antibiot. Chemother. (1971) 1987, 39, 41–50. [Google Scholar]
- Reterink, T.J.; Schroeijers, W.E.; van Es, L.A.; Daha, M.R. Dimeric and polymeric IgA, but not monomeric IgA, enhance the production of IL-6 by human renal mesangial cells. Mediat. Inflamm. 1996, 5, 191–195. [Google Scholar] [CrossRef] [PubMed]
- Leung, J.C.K.; Tang, S.C.W.; Chan, L.Y.Y.; Chan, W.L.; Lai, K.N. Synthesis of TNF-alpha by mesangial cells cultured with polymeric anionic IgA--role of MAPK and NF-kappaB. Nephrol. Dial. Transplant. 2008, 23, 72–81. [Google Scholar] [CrossRef] [PubMed]
- Lai, A.S.H.; Lai, K.N. Molecular basis of IgA nephropathy. Curr. Mol. Med. 2005, 5, 475–487. [Google Scholar] [CrossRef]
- Pabst, O. New concepts in the generation and functions of IgA. Nat. Rev. Immunol. 2012, 12, 821–832. [Google Scholar] [CrossRef] [PubMed]
- Ponticelli, C.; Locatelli, F. Glucocorticoids in the Treatment of Glomerular Diseases. Clin. J. Am. Soc. Nephrol. 2018, 13, 815–822. [Google Scholar] [CrossRef] [PubMed]
- Kant, S.; Kronbichler, A.; Geetha, D. Principles of Immunosuppression in the Management of Kidney Disease: Core Curriculum 2022. Am. J. Kidney Dis. 2022, 80, 393–405. [Google Scholar] [CrossRef] [PubMed]
- Radhakrishnan, J.; Cattran, D.C. The KDIGO practice guideline on glomerulonephritis: Reading between the (guide)lines—Application to the individual patient. Kidney Int. 2012, 82, 840–856. [Google Scholar] [CrossRef]
- Coppo, R. The Gut-Renal Connection in IgA Nephropathy. Semin. Nephrol. 2018, 38, 504–512. [Google Scholar] [CrossRef] [PubMed]
- Emancipator, S.N.; Gallo, G.R.; Lamm, M.E. Experimental IgA nephropathy induced by oral immunization. J. Exp. Med. 1983, 157, 572–582. [Google Scholar] [CrossRef] [PubMed]
- Coppo, R.; Basolo, B.; Rollino, C.; Roccatello, D.; Martina, G.; Amore, A.; Piccoli, G. Dietary gluten and primary IgA nephropathy. N. Engl. J. Med. 1986, 315, 1167–1168. [Google Scholar] [CrossRef] [PubMed]
- Smerud, H.K.; Bárány, P.; Lindström, K.; Fernström, A.; Sandell, A.; Påhlsson, P.; Fellström, B. New treatment for IgA nephropathy: Enteric budesonide targeted to the ileocecal region ameliorates proteinuria. Nephrol. Dial. Transplant. 2011, 26, 3237–3242. [Google Scholar] [CrossRef]
- Li, Y.; Fu, R.; Gao, J.; Wang, L.; Duan, Z.; Tian, L.; Ge, H.; Ma, X.; Zhang, Y.; Li, K.; et al. Effect of pulsed intravenous methylprednisolone with alternative low-dose prednisone on high-risk IgA nephropathy: A 18-month prospective clinical trial. Sci. Rep. 2022, 12, 1. [Google Scholar] [CrossRef]
- Liang, M.; Xiong, L.; Li, A.; Zhou, J.; Huang, Y.; Huang, M.; Zhang, X.; Shi, H.; Su, N.; Wei, Y.; et al. The effectiveness and safety of corticosteroid therapy for IgA nephropathy with crescents: A prospective, randomized, controlled study. BMC Nephrol. 2022, 23, 40. [Google Scholar] [CrossRef]
- Tesar, V.; Troyanov, S.; Bellur, S.; Verhave, J.C.; Cook, H.T.; Feehally, J.; Roberts, I.S.; Cattran, D.; Coppo, R. Corticosteroids in IgA Nephropathy: A Retrospective Analysis from the VALIGA Study. J. Am. Soc. Nephrol. 2015, 26, 2248–2258. [Google Scholar] [CrossRef]
- Venettacci, O.; Larkins, N.; Willis, F. Childhood IgA Nephropathy Successfully Treated with Targeted-Release Budesonide: A Case Report. J. Paediatr. Child Health 2018, 54, 1403. [Google Scholar] [CrossRef]
- Ismail, G.; Obrişcă, B.; Jurubiţă, R.; Andronesi, A.; Sorohan, B.; Vornicu, A.; Sinescu, I.; Hârza, M. Budesonide versus systemic corticosteroids in IgA Nephropathy: A retrospective, propensity-matched comparison. Medicine 2020, 99, e21000. [Google Scholar] [CrossRef]
- Edsbäcker, S.; Andersson, T. Pharmacokinetics of budesonide (Entocort EC) capsules for Crohn’s disease. Clin. Pharmacokinet. 2004, 43, 803–821. [Google Scholar] [CrossRef]
- Hogg, R.J.; Lee, J.; Nardelli, N.; Julian, B.A.; Cattran, D.; Waldo, B.; Wyatt, R.; Jennette, J.C.; Sibley, R.; Hyland, K.; et al. Clinical trial to evaluate omega-3 fatty acids and alternate day prednisone in patients with IgA nephropathy: Report from the Southwest Pediatric Nephrology Study Group. Clin. J. Am. Soc. Nephrol. 2006, 1, 467–474. [Google Scholar] [CrossRef]
- Obrișcă, B.; Vornicu, A.; Mocanu, V.; Dimofte, G.; Andronesi, A.; Bobeică, R.; Jurubiță, R.; Sorohan, B.; Caceaune, N.; Ismail, G. An open-label study evaluating the safety and efficacy of budesonide in patients with IgA nephropathy at high risk of progression. Sci. Rep. 2023, 13, 20119. [Google Scholar] [CrossRef] [PubMed]
- Fellström, B.C.; Barratt, J.; Cook, H.; Coppo, R.; Feehally, J.; de Fijter, J.W.; Floege, J.; Hetzel, G.; Jardine, A.G.; Locatelli, F.; et al. Targeted-release budesonide versus placebo in patients with IgA nephropathy (NEFIGAN): A double-blind, randomised, placebo-controlled phase 2b trial. Lancet 2017, 389, 2117–2127. [Google Scholar] [CrossRef] [PubMed]
- Lafayette, R.; Kristensen, J.; Stone, A.; Floege, J.; Tesař, V.; Trimarchi, H.; Zhang, H.; Eren, N.; Paliege, A.; Reich, H.N.; et al. Efficacy and safety of a targeted-release formulation of budesonide in patients with primary IgA nephropathy (NefIgArd): 2-year results from a randomised phase 3 trial. Lancet 2023, 402, 859–870. [Google Scholar] [CrossRef] [PubMed]
- Coppo, R.; Mariat, C. Systemic corticosteroids and mucosal-associated lymphoid tissue-targeted therapy in immunoglobulin A nephropathy: Insight from the NEFIGAN study. Nephrol. Dial. Transplant. 2020, 35, 1291–1294. [Google Scholar] [CrossRef] [PubMed]
- Pockros, B.M.; Finch, D.J.; Weiner, D.E. Dialysis and Total Health Care Costs in the United States and Worldwide: The Financial Impact of a Single-Payer Dominant System in the US. J. Am. Soc. Nephrol. 2021, 32, 2137–2139. [Google Scholar] [CrossRef] [PubMed]
- Ramjee, L.; Vurgun, N.; Ngai, C.; Patel, M.; Tremblay, G. Cost-Effectiveness Analysis of Nefecon versus Best Supportive Care for People with Immunoglobulin A Nephropathy (IgAN) in the United States. Clin. Outcomes Res. 2023, 15, 213–226. [Google Scholar] [CrossRef] [PubMed]
- League, R.J.; Eliason, P.; McDevitt, R.C.; Roberts, J.W.; Wong, H. Assessment of Spending for Patients Initiating Dialysis Care. JAMA Netw. Open 2022, 5, e2239131. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | Number of Participants | Drug Administered | Daily Dosage | Treatment Duration | Follow-Up | Clinical Outcomes (Statistically Significant) | Major Adverse Events | |
|---|---|---|---|---|---|---|---|---|
| Yan Li et al. [40] | 87 | 45 (1st group) | Intravenous methylprednisolone and prednisone | 0.5 g of methylprednisolone intravenously for three consecutive days at the beginning of the course and at 3 months. In addition, they received oral prednisone at a dose of 15 mg every other day. | 6 months | 12 months | No statistically significant differences were observed. However, cumulative dosages of glucocorticoid were significantly increased in the second group. | More side effects were recorded in this group (infections, weight gain, and Cushing syndrome). |
| 42 (2nd group) | Oral administration of prednisone | Oral administration of 0.8–1.0 mg/kg of prednisone per day with a maximum daily dosage of 70 mg (full-dose treatment). | 6 months (this treatment was administered for 2 months and then tapered by 5 mg every 10 days for the next 4 months) | |||||
| Mengjun Liang [41] | 68 | 34 (1st group) 34 (2nd group) | Administration of methylprednisolone intravenously and oral prednisone. | The treatment starts with 0.25 g/day of methylprednisolone intravenously for 3 consecutive days in respective months and oral prednisone 0.5 mg/kg/day on consecutive days. The first group received steroid IV pulses at the 1st, 2nd, and 3rd months, and the second one at 1st, 3rd, and 5th months, respectively. | 6 months | No | The first group exhibited more optimistic findings, although without statistical significance. | There were no significant differences in the side effects between the 2 groups. |
| Authors | Number of Participants | Drug Administered | Daily Dosage | Treatment Duration | Placebo Group | Compared Group Receiving Other Immunosuppressive Drug | Follow-Up | Clinical Outcomes (Statistically Significant) | Major Adverse Events |
|---|---|---|---|---|---|---|---|---|---|
| Smerud et al. [39] | 16 | Nefecon | 8 mg | 6 months | No | No | 3 months | Urine albumin reduction was 529 mg/day (p = 0.04) and after 2 months of follow-up was even higher. Reduction in serum creatinine of 6% after treatment (p = 0.003) | No |
| Fellström et al. [48] | 149 | Nefecon | 1st group (48 patients) received 16 mg; 2nd group (51 patients) received 8 mg | 9 months | 50 patients | No | 3 months (Patients were tapered from 16 mg/day to 8 mg/day over 2 weeks, and follow-up was assessed 4 weeks later). | At 9 months, TRF-budesonide (16 mg/day plus 8 mg/day) was associated with a 24.4% decrease from baseline in mean UPCR (p = 0.0066). At 9 months, mean UPCR had decreased by 27.3% in 48 patients who received 16 mg/day (p = 0.0092) and by 21.5% in the 51 patients who received 8 mg/day (p = 0.0290); 50 patients who received placebo had an increase in mean UPCR of 2.7% | Two out of thirteen serious adverse events were possibly associated with TRF-budesonide—deep vein thrombosis (16 mg/day) and unexplained deterioration in renal function in follow-up. |
| Ismail et al. [44] | 18 | Budenofalk | 9 mg for 12 months, followed by 3 mg for another 12 months | 24 months | No | Systemic corticosteroids (18 participants) | No further follow-up after the 24-month therapy was recorded | The median reductions in proteinuria at 24 months were 45% in the budesonide group and 11% in the corticosteroid group (p = 0.009). | |
| Lafayette et al. [49] | 182 | Nefecon | 16 mg | 9 months | Yes (182 participants) | No | 15-month observational follow-up | The time-weighted average of eGFR over 2 years showed a statistically significant treatment benefit with Nefecon versus placebo (difference of 5.05 mL/min/1.73 m2 (p < 0.0001). | |
| Obrișcă et al. [47] | 32 | Budenofalk | 9 mg/day for 12 month, subsequently tapered to 3 mg/day for another 12 months | 24 months | No | No | Yes, another 12 months | Reduction in proteinuria, from 1.89 ± 1.5 g/d at baseline to 0.5 ± 0.4 g/d at 36 months (p < 0.001). Treatment with budesonide was associated with a significant decline in proteinuria irrespective of baseline levels. Despite the fact that during the treatment period, the eGFR had a tendency to increase, during the 12 months of post-treatment follow-up, the mean eGFR reduced to baseline levels. |
| Benefits | Limitations | |
|---|---|---|
| Budesonide | Less systemic bio-availability | Unknown dosage and treatment duration |
| Acts at an earlier stage in the pathogenesis cascade | Not supported by KDIGO 2021 guidelines | |
| Fewer side effects, with minor or moderate severity | Few studies with small study groups | |
| More effective treatment regarding albuminuria reduction and GFR maintenance (1 study found) More expensive treatment but it can delay disease progress | Recently studied | |
| Systemic corticosteroids | Many studies have evaluated their efficacy | Severe adverse events |
| Defined dosage and treatment duration | Can be administered under specific circumstances | |
| Supported by KDIGO 2021 guidelines Inexpensive treatment | Systemic availability of the drug |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Keskinis, C.; Moysidou, E.; Christodoulou, M.; Pateinakis, P.; Stangou, M. Diagnosing and Treating IgAN: Steroids, Budesonide, or Maybe Both? Diagnostics 2024, 14, 512. https://doi.org/10.3390/diagnostics14050512
Keskinis C, Moysidou E, Christodoulou M, Pateinakis P, Stangou M. Diagnosing and Treating IgAN: Steroids, Budesonide, or Maybe Both? Diagnostics. 2024; 14(5):512. https://doi.org/10.3390/diagnostics14050512
Chicago/Turabian StyleKeskinis, Christodoulos, Eleni Moysidou, Michalis Christodoulou, Panagiotis Pateinakis, and Maria Stangou. 2024. "Diagnosing and Treating IgAN: Steroids, Budesonide, or Maybe Both?" Diagnostics 14, no. 5: 512. https://doi.org/10.3390/diagnostics14050512
APA StyleKeskinis, C., Moysidou, E., Christodoulou, M., Pateinakis, P., & Stangou, M. (2024). Diagnosing and Treating IgAN: Steroids, Budesonide, or Maybe Both? Diagnostics, 14(5), 512. https://doi.org/10.3390/diagnostics14050512