
The Role of SARS-CoV-2 Nucleocapsidic Antigen and Krebs von den Lungen 6 Serum Levels in Predicting COVID-19 Pneumonia Outcome
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. SARS-CoV-2 Nucleocapsidic Antigen
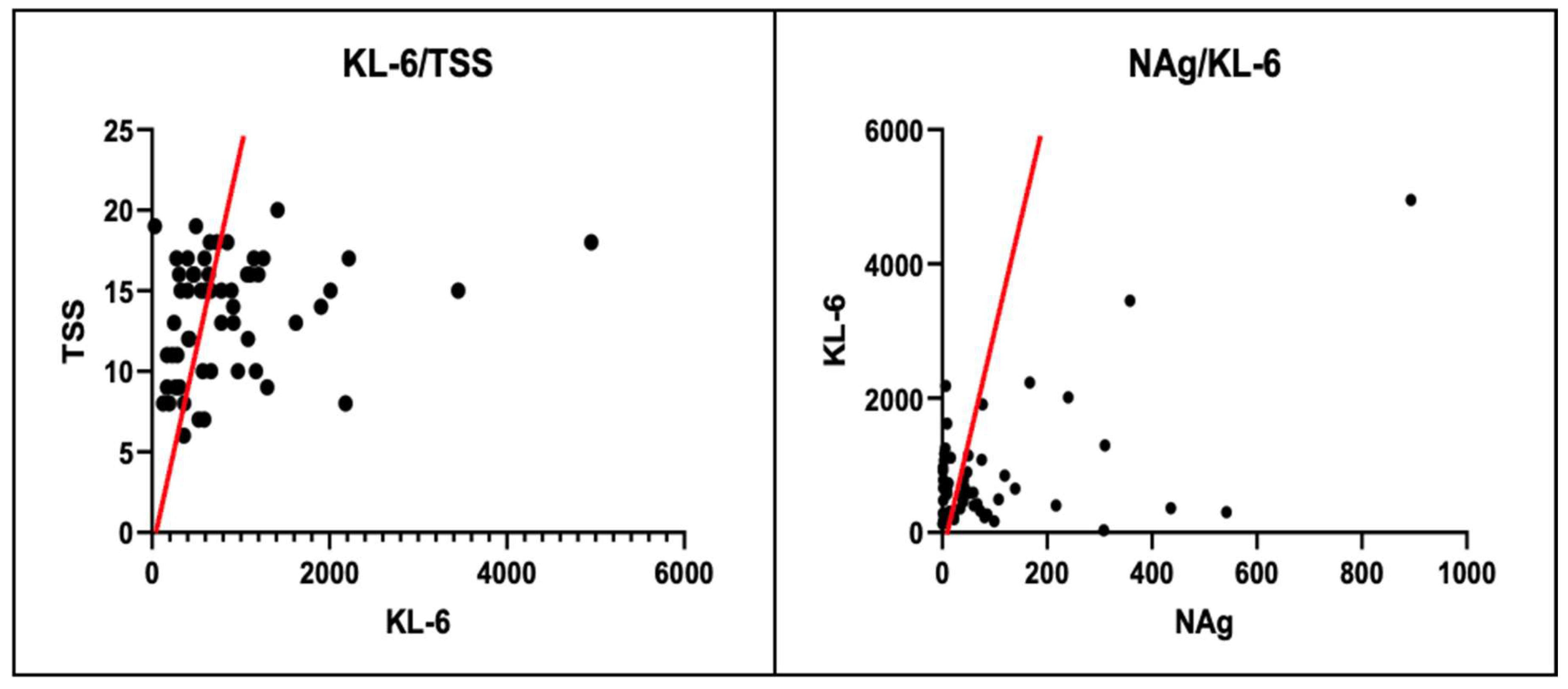
3.2. Krebs von den Lungen-6
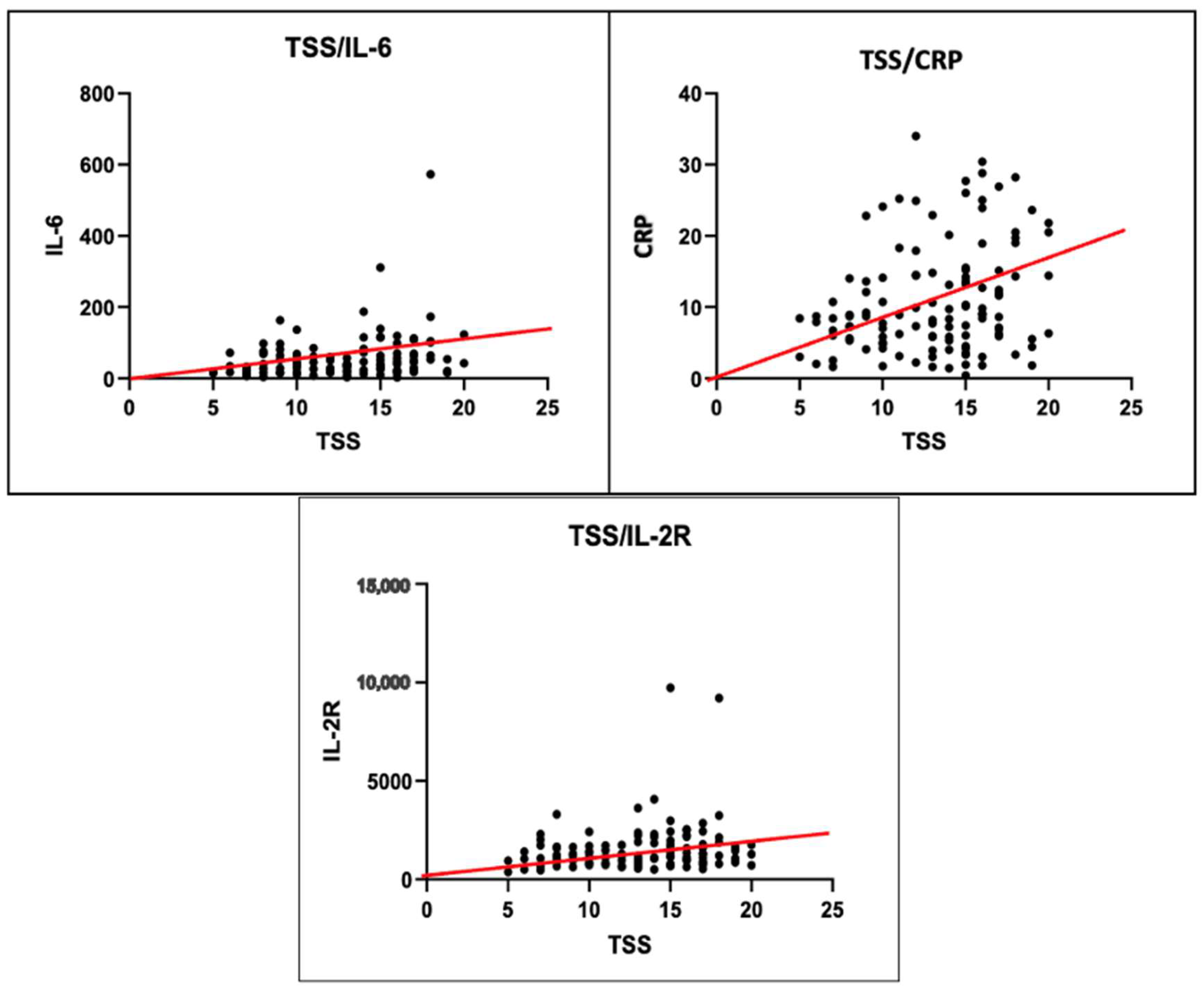
3.3. Total Severity Score

{kind=link}
{kind=link}
{kind=link}
| Disease Severity Markers | NAg | KL-6 | TSS | |||
|---|---|---|---|---|---|---|
| r | p-Value | r | p-Value | r | p-Value | |
| CRP | +0.211 | 0.01 * | +0.104 | 0.43 | +0.250 | 0.005 * |
| PCT | +0.207 | 0.02 * | NR | NR | NR | NR |
| TSS | +0.199 | 0.02 * | +0.268 | 0.04 * | NA | NA |
| KL-6 | +0.278 | 0.01 * | NR | NR | +0.268 | 0.04 * |
| IL-6 | +0.248 | 0.005 * | +0.129 | 0.33 | +0.248 | 0.005 * |
| IL-2R | +0.145 | 0.1 * | NR | NR | NR | NR |
| NAg | NA | NA | +0.278 | 0.03 * | +0.199 | 0.02 * |


3.4. Complications
4. Discussion
4.1. Krebs von den Lungen
4.2. SARS-CoV-2 Nucleocapsidic Antigen
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sharma, A.; Farouk, I.A.; Lal, S.K.; Martinez-Sobrido, L.; Toral, F.A. COVID-19: A Review on the Novel Coronavirus Disease Evolution, Transmission, Detection, Control and Prevention. Viruses 2021, 13, 202. [Google Scholar] [CrossRef]
- Nigro, E.; Perrotta, F.; Polito, R.; D’Agnano, V.; Scialò, F.; Bianco, A.; Daniele, A. Metabolic Perturbations and Severe COVID-19 Disease: Implication of Molecular Pathways. Int. J. Endocrinol. 2020, 2020, 8896536. [Google Scholar] [CrossRef] [PubMed]
- Palladino, R.; Mercogliano, M.; Fiorilla, C.; Frangiosa, A.; Iodice, S.; Sanduzzi Zamparelli, S.; Montella, E.; Triassi, M.; Sanduzzi Zamparelli, A. Association between COVID-19 and Sick Leave for Healthcare Workers in a Large Academic Hospital in Southern Italy: An Observational Study. Int. J. Environ. Res. Public Health 2022, 19, 9670. [Google Scholar] [CrossRef] [PubMed]
- Khalid, M.F.; Selvam, K.; Jeffry, A.J.N.; Salmi, M.F.; Najib, M.A.; Norhayati, M.N.; Aziah, I. Performance of Rapid Antigen Tests for COVID-19 Diagnosis: A Systematic Review and Meta-Analysis. Diagnostics 2022, 12, 110. [Google Scholar] [CrossRef] [PubMed]
- Sanduzzi, A.; Zamparelli, S.S. Nasopharyngeal and Oropharyngeal Swabs, And/Or Serology for SARS COVID-19: What Are We Looking For? Int. J. Environ. Res. Public Health 2020, 17, 3289. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Y.; Jiao, B.; Qu, L.; Yang, D.; Liu, R. The Development of COVID-19 Treatment. Front. Immunol. 2023, 14, 1125246. [Google Scholar] [CrossRef] [PubMed]
- Zamparelli, S.S.; Capitelli, L.; Coppola, N.; Venditto, C.; Santoro, C.; Annunziata, G.; Bruzzese, D.; Cuomo, N.; Gentile, I.; Bocchino, M.; et al. A Phase II Study on the Effect of Taurisolo® Administered via AEROsol in Hospitalized Patients with Mild to Moderate COVID-19 Pneumonia: The TAEROVID-19 Study. Cells 2022, 11, 1499. [Google Scholar] [CrossRef]
- Sarkar, S.; Khanna, P.; Singh, A.K. The Impact of Neutrophil-Lymphocyte Count Ratio in COVID-19: A Systematic Review and Meta-Analysis. J. Intensive Care Med. 2022, 37, 857–869. [Google Scholar] [CrossRef]
- Mueller, A.A.; Tamura, T.; Crowley, C.P.; DeGrado, J.R.; Haider, H.; Jezmir, J.L.; Keras, G.; Penn, E.H.; Massaro, A.F.; Kim, E.Y. Inflammatory Biomarker Trends Predict Respiratory Decline in COVID-19 Patients. Cell Rep. Med. 2020, 1, 100144. [Google Scholar] [CrossRef]
- Ihling, C.; Tänzler, D.; Hagemann, S.; Kehlen, A.; Hüttelmaier, S.; Arlt, C.; Sinz, A. Mass Spectrometric Identification of SARS-CoV-2 Proteins from Gargle Solution Samples of COVID-19 Patients. J. Proteome Res. 2020, 19, 4389–4392. [Google Scholar] [CrossRef]
- Wu, W.; Cheng, Y.; Zhou, H.; Sun, C.; Zhang, S. The SARS-CoV-2 Nucleocapsid Protein: Its Role in the Viral Life Cycle, Structure and Functions, and Use as a Potential Target in the Development of Vaccines and Diagnostics. Virol. J. 2023, 20, 6. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, T. Viewing SARS-CoV-2 Nucleocapsid Protein in Terms of Molecular Flexibility. Biology 2021, 10, 454. [Google Scholar] [CrossRef] [PubMed]
- Letko, M.; Marzi, A.; Munster, V. Functional Assessment of Cell Entry and Receptor Usage for SARS-CoV-2 and Other Lineage B Betacoronaviruses. Nat. Microbiol. 2020, 5, 562–569. [Google Scholar] [CrossRef] [PubMed]
- Baggen, J.; Vanstreels, E.; Jansen, S.; Daelemans, D. Cellular Host Factors for SARS-CoV-2 Infection. Nat. Microbiol. 2021, 6, 1219–1232. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.K.; Hou, M.H.; Chang, C.F.; Hsiao, C.D.; Huang, T.H. The SARS Coronavirus Nucleocapsid Protein—Forms and Functions. Antivir. Res. 2014, 103, 39–50. [Google Scholar] [CrossRef]
- Thathiah, A.; Blobel, C.P.; Carson, D.D. Tumor Necrosis Factor-Alpha Converting Enzyme/ADAM 17 Mediates MUC1 Shedding. J. Biol. Chem. 2003, 278, 3386–3394. [Google Scholar] [CrossRef] [PubMed]
- Ballester, B.; Milara, J.; Cortijo, J. The Role of Mucin 1 in Respiratory Diseases. Eur. Respir. Rev. 2021, 30, 200149. [Google Scholar] [CrossRef] [PubMed]
- Kato, K.; Lillehoj, E.P.; Lu, W.; Kim, K.C. MUC1: The First Respiratory Mucin with an Anti-Inflammatory Function. J. Clin. Med. 2017, 6, 110. [Google Scholar] [CrossRef]
- Zhang, T.; Shen, P.; Duan, C.; Gao, L. KL-6 as an Immunological Biomarker Predicts the Severity, Progression, Acute Exacerbation, and Poor Outcomes of Interstitial Lung Disease: A Systematic Review and Meta-Analysis. Front. Immunol. 2021, 12, 745233. [Google Scholar] [CrossRef]
- Castellví, I.; Castillo, D.; Corominas, H.; Mariscal, A.; Orozco, S.; Benito, N.; Pomar, V.; Baucells, A.; Mur, I.; de la Rosa-Carrillo, D.; et al. Krebs von Den Lungen-6 Glycoprotein Circulating Levels Are Not Useful as Prognostic Marker in COVID-19 Pneumonia: A Large Prospective Cohort Study. Front. Med. 2022, 9, 973918. [Google Scholar] [CrossRef]
- d’Alessandro, M.; Bergantini, L.; Cameli, P.; Curatola, G.; Remediani, L.; Sestini, P.; Bargagli, E.; Bennett, D.; Bianchi, F.; Perillo, F.; et al. Peripheral Biomarkers’ Panel for Severe COVID-19 Patients. J. Med. Virol. 2021, 93, 1230. [Google Scholar] [CrossRef]
- D’Agnano, V.; Scialò, F.; Perna, F.; Atripaldi, L.; Sanduzzi, S.; Allocca, V.; Vitale, M.; Pastore, L.; Bianco, A.; Perrotta, F. Exploring the Role of Krebs von Den Lungen-6 in Severe to Critical COVID-19 Patients. Life 2022, 12, 1141. [Google Scholar] [CrossRef] [PubMed]
- Perna, F.; Bruzzaniti, S.; Piemonte, E.; Maddaloni, V.; Atripaldi, L.; Sale, S.; Sanduzzi, A.; Nicastro, C.; Pepe, N.; Bifulco, M.; et al. Serum Levels of SARS-CoV-2 Nucleocapsid Antigen Associate with Inflammatory Status and Disease Severity in COVID-19 Patients. Clin. Immunol. 2021, 226, 108720. [Google Scholar] [CrossRef]
- Chung, M.; Bernheim, A.; Mei, X.; Zhang, N.; Huang, M.; Zeng, X.; Cui, J.; Xu, W.; Yang, Y.; Fayad, Z.A.; et al. CT Imaging Features of 2019 Novel Coronavirus (2019-NCoV). Radiology 2020, 295, 202–207. [Google Scholar] [CrossRef] [PubMed]
- Modig, K.; Lambe, M.; Ahlbom, A.; Ebeling, M. Excess Mortality for Men and Women above Age 70 According to Level of Care during the First Wave of COVID-19 Pandemic in Sweden: A Population-Based Study. Lancet Reg. Health-Europe 2021, 4, 100072. [Google Scholar] [CrossRef]
- Bauer, P.; Brugger, J.; König, F.; Posch, M. An International Comparison of Age and Sex Dependency of COVID-19 Deaths in 2020: A Descriptive Analysis. Sci. Rep. 2021, 11, 19143. [Google Scholar] [CrossRef] [PubMed]
- Liu, K.; Chen, Y.; Lin, R.; Han, K. Clinical Features of COVID-19 in Elderly Patients: A Comparison with Young and Middle-Aged Patients. J. Infect. 2020, 80, e14–e18. [Google Scholar] [CrossRef] [PubMed]
- Bonanad, C.; García-Blas, S.; Tarazona-Santabalbina, F.; Sanchis, J.; Bertomeu-González, V.; Fácila, L.; Ariza, A.; Núñez, J.; Cordero, A. The Effect of Age on Mortality in Patients With COVID-19: A Meta-Analysis with 611,583 Subjects. J. Am. Med. Dir. Assoc. 2020, 21, 915–918. [Google Scholar] [CrossRef]
- Kragholm, K.; Andersen, M.P.; Gerds, T.A.; Butt, J.H.; Østergaard, L.; Polcwiartek, C.; Phelps, M.; Andersson, C.; Gislason, G.H.; Torp-Pedersen, C.; et al. Association between Male Sex and Outcomes of Coronavirus Disease 2019 (COVID-19)—A Danish Nationwide, Register-Based Study. Clin. Infect. Dis. 2021, 73, E4025–E4030. [Google Scholar] [CrossRef]
- Peckham, H.; de Gruijter, N.M.; Raine, C.; Radziszewska, A.; Ciurtin, C.; Wedderburn, L.R.; Rosser, E.C.; Webb, K.; Deakin, C.T. Male Sex Identified by Global COVID-19 Meta-Analysis as a Risk Factor for Death and ITU Admission. Nat. Commun. 2020, 11, 6317. [Google Scholar] [CrossRef]
- Castillo, L.; Carcillo, J. Secondary Hemophagocytic Lymphohistiocytosis and Severe Sepsis/ Systemic Inflammatory Response Syndrome/Multiorgan Dysfunction Syndrome/Macrophage Activation Syndrome Share Common Intermediate Phenotypes on a Spectrum of Inflammation. Pediatr. Crit. Care Med. 2009, 10, 387–392. [Google Scholar] [CrossRef]
- Luo, M.; Liu, J.; Jiang, W.; Yue, S.; Liu, H.; Wei, S. IL-6 and CD8+ T Cell Counts Combined Are an Early Predictor of in-Hospital Mortality of Patients with COVID-19. JCI Insight 2020, 5, e139024. [Google Scholar] [CrossRef] [PubMed]
- Dogan, S.; Bal, T.; Çabalak, M.; Dikmen, N.; Yaqoobi, H.; Ozcan, O. Oxidative Stress Index Can Be a New Marker Related to Disease Severity in COVID-19. Turk. J. Biochem. 2021, 46, 349–357. [Google Scholar] [CrossRef]
- Le, R.Q.; Li, L.; Yuan, W.; Shord, S.S.; Nie, L.; Habtemariam, B.A.; Przepiorka, D.; Farrell, A.T.; Pazdur, R. FDA Approval Summary: Tocilizumab for Treatment of Chimeric Antigen Receptor T Cell-Induced Severe or Life-Threatening Cytokine Release Syndrome. Oncologist 2018, 23, 943. [Google Scholar] [CrossRef]
- Ali, N. Elevated Level of C-Reactive Protein May Be an Early Marker to Predict Risk for Severity of COVID-19. J. Med. Virol. 2020, 92, 2409–2411. [Google Scholar] [CrossRef] [PubMed]
- Sharifpour, M.; Rangaraju, S.; Liu, M.; Alabyad, D.; Nahab, F.B.; Creel-Bulos, C.M.; Jabaley, C.S. C-Reactive Protein as a Prognostic Indicator in Hospitalized Patients with COVID-19. PLoS ONE 2020, 15, e0242400. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.; Park, S.; Hayden, A.; Giustini, D.; Trinkaus, M.; Pudek, M.; Mattman, A.; Schneider, M.; Chen, L.Y.C. Clinical Utility of Soluble Interleukin-2 Receptor in Hemophagocytic Syndromes: A Systematic Scoping Review. Ann. Hematol. 2017, 96, 1241–1251. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Z.; Yu, H.; Chen, H.; Qi, W.; Chen, L.; Chen, G.; Yan, W.; Chen, T.; Ning, Q.; Han, M.; et al. Longitudinal Changes of Inflammatory Parameters and Their Correlation with Disease Severity and Outcomes in Patients with COVID-19 from Wuhan, China. Crit. Care 2020, 24, 525. [Google Scholar] [CrossRef]
- Sayah, W.; Berkane, I.; Guermache, I.; Sabri, M.; Lakhal, F.Z.; Yasmine Rahali, S.; Djidjeli, A.; Lamara Mahammed, L.; Merah, F.; Belaid, B.; et al. Interleukin-6, Procalcitonin and Neutrophil-to-Lymphocyte Ratio: Potential Immune-Inflammatory Parameters to Identify Severe and Fatal Forms of COVID-19. Cytokine 2021, 141, 155428. [Google Scholar] [CrossRef]
- Samsudin, I.; Vasikaran, S.D. Clinical Utility and Measurement of Procalcitonin. Clin. Biochem. Rev. 2017, 38, 59. [Google Scholar]
- Querol-Ribelles, J.M.; Tenias, J.M.; Grau, E.; Querol-Borras, J.M.; Climent, J.L.; Gomez, E.; Martinez, I. Plasma D-Dimer Levels Correlate with Outcomes in Patients with Community-Acquired Pneumonia. Chest 2004, 126, 1087–1092. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical Features of Patients Infected with 2019 Novel Coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.H.; Qin, C.; Chen, M.; Wang, W.; Tian, D.S. D-Dimer Level Is Associated with the Severity of COVID-19. Thromb. Res. 2020, 195, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Ambrosino, P.; Sanduzzi Zamparelli, S.; Mosella, M.; Formisano, R.; Molino, A.; Spedicato, G.A.; Papa, A.; Motta, A.; Di Minno, M.N.D.; Maniscalco, M. Clinical Assessment of Endothelial Function in Convalescent COVID-19 Patients: A Meta-Analysis with Meta-Regressions. Ann. Med. 2022, 54, 3234–3249. [Google Scholar] [CrossRef] [PubMed]
- Groff, D.; Sun, A.; Ssentongo, A.E.; Ba, D.M.; Parsons, N.; Poudel, G.R.; Lekoubou, A.; Oh, J.S.; Ericson, J.E.; Ssentongo, P.; et al. Short-Term and Long-Term Rates of Postacute Sequelae of SARS-CoV-2 Infection: A Systematic Review. JAMA Netw. Open 2021, 4, e2128568. [Google Scholar] [CrossRef]
- Elke, G.; Bloos, F.; Wilson, D.C.; Brunkhorst, F.M.; Briegel, J.; Reinhart, K.; Loeffler, M.; Kluge, S.; Nierhaus, A.; Jaschinski, U.; et al. The Use of Mid-Regional Proadrenomedullin to Identify Disease Severity and Treatment Response to Sepsis—A Secondary Analysis of a Large Randomised Controlled Trial. Crit. Care 2018, 22, 79. [Google Scholar] [CrossRef] [PubMed]
- Wilson, D.C.; Schefold, J.C.; Baldirà, J.; Spinetti, T.; Saeed, K.; Elke, G. Adrenomedullin in COVID-19 Induced Endotheliitis. Crit. Care 2020, 24, 411. [Google Scholar] [CrossRef]
- Calabretta, E.; Moraleda, J.M.; Iacobelli, M.; Jara, R.; Vlodavsky, I.; O’Gorman, P.; Pagliuca, A.; Mo, C.; Baron, R.M.; Aghemo, A.; et al. COVID-19-Induced Endotheliitis: Emerging Evidence and Possible Therapeutic Strategies. Br. J. Haematol. 2021, 193, 43–51. [Google Scholar] [CrossRef]
- Simon, T.P.; Stoppe, C.; Breuer, T.; Stiehler, L.; Dreher, M.; Kersten, A.; Kluge, S.; Karakas, M.; Zechendorf, E.; Marx, G.; et al. Prognostic Value of Bioactive Adrenomedullin in Critically Ill Patients with COVID-19 in Germany: An Observational Cohort Study. J. Clin. Med. 2021, 10, 1667. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Lee, E.Y.; Ha, Y.J.; Kang, E.H.; Lee, Y.J.; Song, Y.W. Serum Kl-6 Levels Reflect the Severity of Interstitial Lung Disease Associated with Connective Tissue Disease. Arthritis Res. Ther. 2019, 21, 58. [Google Scholar] [CrossRef]
- d’Alessandro, M.; Cameli, P.; Refini, R.M.; Bergantini, L.; Alonzi, V.; Lanzarone, N.; Bennett, D.; Rana, G.D.; Montagnani, F.; Scolletta, S.; et al. Serum KL-6 Concentrations as a Novel Biomarker of Severe COVID-19. J. Med. Virol. 2020, 92, 2216–2220. [Google Scholar] [CrossRef]
- Scotto, R.; Pinchera, B.; Perna, F.; Atripaldi, L.; Giaccone, A.; Sequino, D.; Zappulo, E.; Sardanelli, A.; Moriello, N.S.; Stanziola, A.; et al. Serum KL-6 Could Represent a Reliable Indicator of Unfavourable Outcome in Patients with COVID-19 Pneumonia. Int. J. Environ. Res. Public Health 2021, 18, 2078. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Wang, L.; Wang, H.; Li, X.; Zhang, S.; Xu, Y.; Wei, W. Serum SARS-CoV-2 Nucleocapsid Protein: A Sensitivity and Specificity Early Diagnostic Marker for SARS-CoV-2 Infection. Front. Cell Infect. Microbiol. 2020, 10, 470. [Google Scholar] [CrossRef] [PubMed]
- Pan, P.; Shen, M.; Yu, Z.; Ge, W.; Chen, K.; Tian, M.; Xiao, F.; Wang, Z.; Wang, J.; Jia, Y.; et al. SARS-CoV-2 N Protein Promotes NLRP3 Inflammasome Activation to Induce Hyperinflammation. Nat. Commun. 2021, 12, 4664. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Sui, L.; Wu, P.; Wang, W.; Wang, Z.; Yu, Y.; Hou, Z.; Tan, G.; Liu, Q.; Wang, G. A Dual-Role of SARS-CoV-2 Nucleocapsid Protein in Regulating Innate Immune Response. Signal Transduct. Target. Ther. 2021, 6, 331. [Google Scholar] [CrossRef] [PubMed]
- Olwal, C.O.; Nganyewo, N.N.; Tapela, K.; Djomkam Zune, A.L.; Owoicho, O.; Bediako, Y.; Duodu, S. Parallels in Sepsis and COVID-19 Conditions: Implications for Managing Severe COVID-19. Front. Immunol. 2021, 12, 602848. [Google Scholar] [CrossRef] [PubMed]
- Jehn, L.B.; Costabel, U.; Boerner, E.; Wälscher, J.; Theegarten, D.; Taube, C.; Bonella, F. Serum KL-6 as a Biomarker of Progression at Any Time in Fibrotic Interstitial Lung Disease. J. Clin. Med. 2023, 12, 1173. [Google Scholar] [CrossRef]
- Roberts, C.M.; Levi, M.; McKee, M.; Schilling, R.; Lim, W.S.; Grocott, M.P.W. COVID-19: A Complex Multisystem Disorder. Br. J. Anaesth. 2020, 125, 238–242. [Google Scholar] [CrossRef]
- Zheng, K.I.; Feng, G.; Liu, W.Y.; Targher, G.; Byrne, C.D.; Zheng, M.H. Extrapulmonary Complications of COVID-19: A Multisystem Disease? J. Med. Virol. 2021, 93, 323–335. [Google Scholar] [CrossRef]
- George, J.A.; Khoza, S. SARS-CoV-2 Infection and the Kidneys: An Evolving Picture. Adv. Exp. Med. Biol. 2021, 1327, 107–118. [Google Scholar] [CrossRef]
| Characteristics | Population (μ) | GI (μI) | GII (μII) | p-Value |
|---|---|---|---|---|
| AGE (years) | 64.75 | 60.56 | 71.26 | GII > GI 0.00001 * |
| SEX (F/M) | 36/92 | 18/58 | 18/34 | 0.16 |
| Blood Count (Unit of Measure) | Population (μ) | GI (μI) | GII (μII) | p-Value |
|---|---|---|---|---|
| RBC (×106/microliter) | 4.7 (nr 4.3–5.9) | 4.8 | 4.5 | GI > GII 0.01 * |
| Hb (g/dL) | 13.6 (nr 13–17) | 13.9 | 13.1 | GI > GII 0.01 * |
| WBC (×106/microliter) | 11.18 (nr 4.0–10.5) | 9.5 | 10.3 | 0.47 |
| LYM (%) | 10.2 (nr 20–45) | 9.5 | 8.3 | 0.13 |
| MON (%) | 5.7 (nr 3.4–11) | 6.1 | 5.1 | GI > GII 0.01 * |
| NEU (%) | 84.3 (nr 40–75) | 83.7 | 86.0 | GII > GI 0.04 * |
| EOS (%) | 0.3 (nr 0.0–7-0) | 0.37 | 0.24 | Gi > GII 0.03 * |
| BAS (%) | 0.18 (nr 0.0–1.5) | 0.21 | 0.16 | 0.7 |
| PLT (×103/microliter) | 232 (nr 150–400) | 238 | 206 | GI > GII 0.007 * |
| Blood Chemistries (Unit of Measure) | Population (μ) | GI (μI) | GII (μII) | p-Value |
|---|---|---|---|---|
| ALT (U/L) | 52.5 (nr 10–49) | 54.2 | 30.4 | GI > GII 0.00002 * |
| AST (U/L) | 48.6 (nr 0–34) | 42.34 | 47.9 | 0.17 |
| Albumin (g/dL) | 3.83 (nr 3.2–4.8) | 3.95 | 3.66 | GI > GII 0.009 * |
| Total Proteins (g/dL) | 6.6 (nr 6.4–8.3) | 6.5 | 6.2 | GI > GII 0.008 * |
| Creatinine (mg/dL) | 1.26 (nr 0.6–1.1) | 0.98 | 1.67 | GII > GI 0.0001 * |
| Azotemia (mg/dL) | 65.3 (nr 10–50) | 54.1 | 81.4 | GII > GI 0.000007 * |
| Sodium (mEq/L) | 138.5 (nr 135–145) | 138.2 | 138.8 | 0.11 |
| Potassium (mEq/L) | 4.48 (nr 3.5–5.1) | 4.28 | 4.53 | GII > GI 0.03 * |
| Calcium (mg/dL) | 8.82 (nr 8.8–10.4) | 9.05 | 8.51 | GI > GII 0.00007 * |
| Corrected Calcium (mg/dL) | 9.04 (nr 8.8–10.4) | 9.19 | 8.82 | GI > GII 0.01 * |
| Glycemia (mg/dL) | 139 (nr 74–106) | 118 | 143 | GII > GI 0.002 * |
| 25-OH D3 (ng/mL) | 21.52 (nr > 30) | 22 | 18 | GI > GII 0.03 * |
| Laboratory and Radiological Markers (Unit of Measure) | Population (μ) | GI (μI) | GII (μII) | p-Value |
|---|---|---|---|---|
| ESR (mm/h) | 58.4 (nr < 10) | 50.9 | 72.2 | GII > GI 0.005 * |
| RCP (mg/dL) | 10.8 (nr < 1) | 8.8 | 12.4 | GII > GI 0.03 * |
| PCT (ng/mL) | 0.41 (<0.05) | 0.22 | 1.42 | GII > GI 0.001 * |
| Adrenomedullin (ng/mL) | 1.64 (nr < 1.01) | 1.34 | 1.98 | GII > GI 0.0002 * |
| D-Dimer (mg/dL) | 462 (nr < 250) | 230 | 818 | GII > GI 0.000003 * |
| IL-6 (pg/mL) | 58.5 (nr 0–6) | 41.3 | 84.8 | GII > GI 0.0001 * |
| IL-2R (U/I) | 1516.9 (nr 150–600) | 1316.3 | 1813.6 | GII > GI 0.001 * |
| Fibrinogen (mg/dL) | 573 (nr < 100) | 567 | 580 | 0.6 |
| Ferritin (ng/mL) | 841 (nr 5–300) | 1023 | 736 | GI > GII 0.005 * |
| NAg (pg/mL) | 137.96 (nr 0–1) | 73.83 | 400.77 | GII > GI 0.001 * |
| KL-6 (U/mL) | 890 (nr 200–600) | 670 | 1159 | GII > GI 0.02 * |
| TSS | 13 | 11 | 15 | GII > GI 0.00001 * |
| Comorbidities | Population (Prevalence) | GI (Prevalence) | GII (Prevalence) | OR | χ2 | p-Value |
|---|---|---|---|---|---|---|
| Anemia | 64/128 (0.5) | 27/76 (0.35) | 37/52 (0.71) | 4.48 | 15.76 | <0.0001 |
| Renal failure | 30/128 (0.23) | 3/76 (0.03) | 27/52 (0.51) | 26.28 | 39.60 | <0.0001 |
| Disiony | 70/126 (0.51) | 30/76 (0.39) | 40/52 (0.76) | 5.11 | 17.47 | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sanduzzi Zamparelli, S.; Fucci, V.; Rea, G.; Perna, F.; Bocchino, M.; Sanduzzi Zamparelli, A. The Role of SARS-CoV-2 Nucleocapsidic Antigen and Krebs von den Lungen 6 Serum Levels in Predicting COVID-19 Pneumonia Outcome. Diagnostics 2024, 14, 642. https://doi.org/10.3390/diagnostics14060642
Sanduzzi Zamparelli S, Fucci V, Rea G, Perna F, Bocchino M, Sanduzzi Zamparelli A. The Role of SARS-CoV-2 Nucleocapsidic Antigen and Krebs von den Lungen 6 Serum Levels in Predicting COVID-19 Pneumonia Outcome. Diagnostics. 2024; 14(6):642. https://doi.org/10.3390/diagnostics14060642
Chicago/Turabian StyleSanduzzi Zamparelli, Stefano, Vincenzo Fucci, Gaetano Rea, Francesco Perna, Marialuisa Bocchino, and Alessandro Sanduzzi Zamparelli. 2024. "The Role of SARS-CoV-2 Nucleocapsidic Antigen and Krebs von den Lungen 6 Serum Levels in Predicting COVID-19 Pneumonia Outcome" Diagnostics 14, no. 6: 642. https://doi.org/10.3390/diagnostics14060642