
Evaluation of Whole Brain Intravoxel Incoherent Motion (IVIM) Imaging

Abstract
1. Introduction
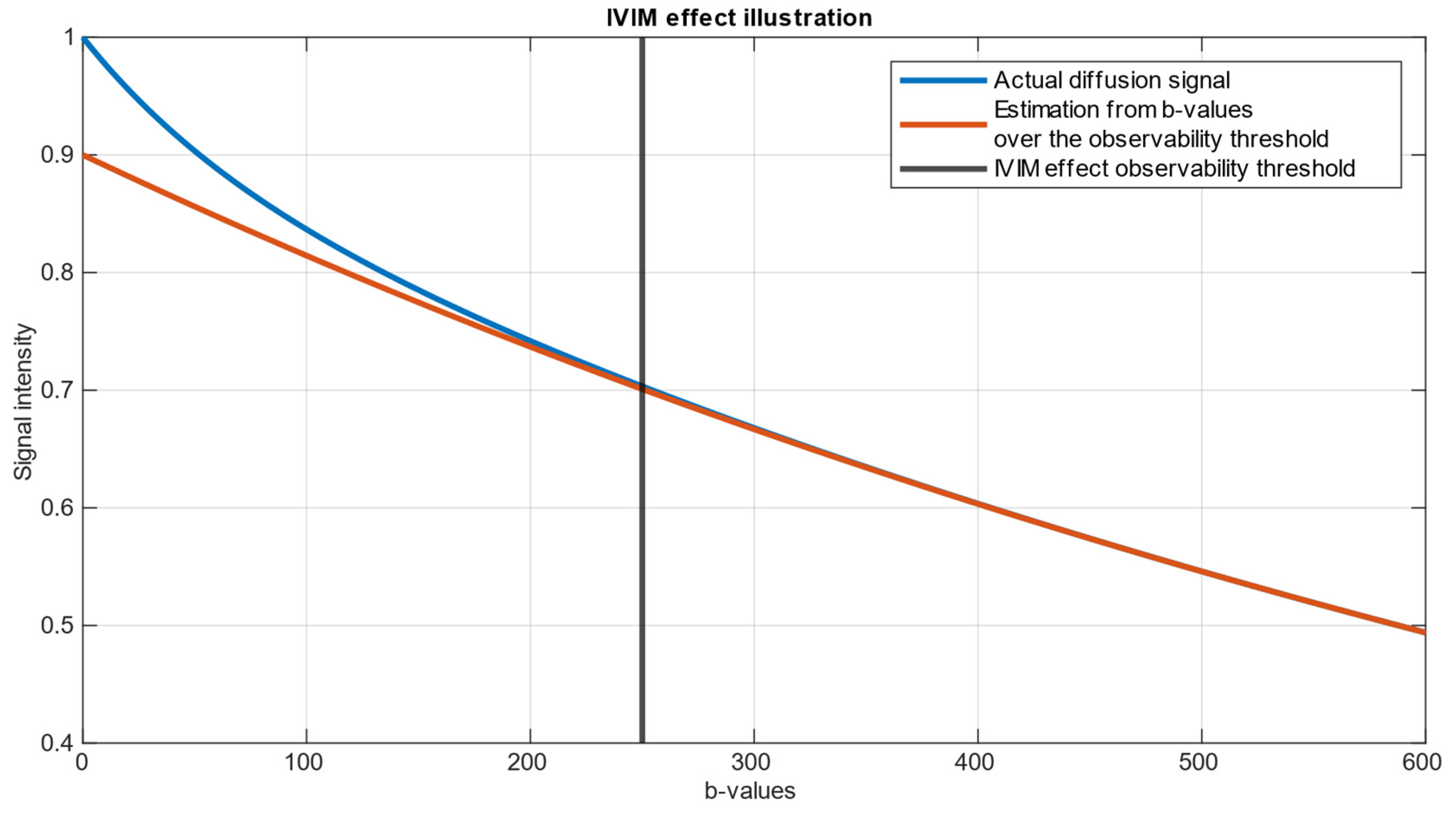
- represents the measured signal intensity in the DWI image for a given .
- stands for b-value—diffusion weighting factor, determined by the strength and timing of the diffusion gradients prior to signal echo.
- is the signal intensity in the absence of diffusion weighting ().
- represents the fraction of signal coming from quick-diffusing water molecules, which are assumed to be circulating in the blood, also referred to as the perfusion fraction.
- is the pseudo-diffusion coefficient, which reflects the diffusion of water in capillaries and small vessels.
- represents the true diffusion coefficient, which characterizes the diffusion of extravascular water molecules.
2. Materials and Methods
- represents the “ground truth” signal,
- represents the noised signal,
- are, respectively, real and imaginary parts of noise.
3. Results
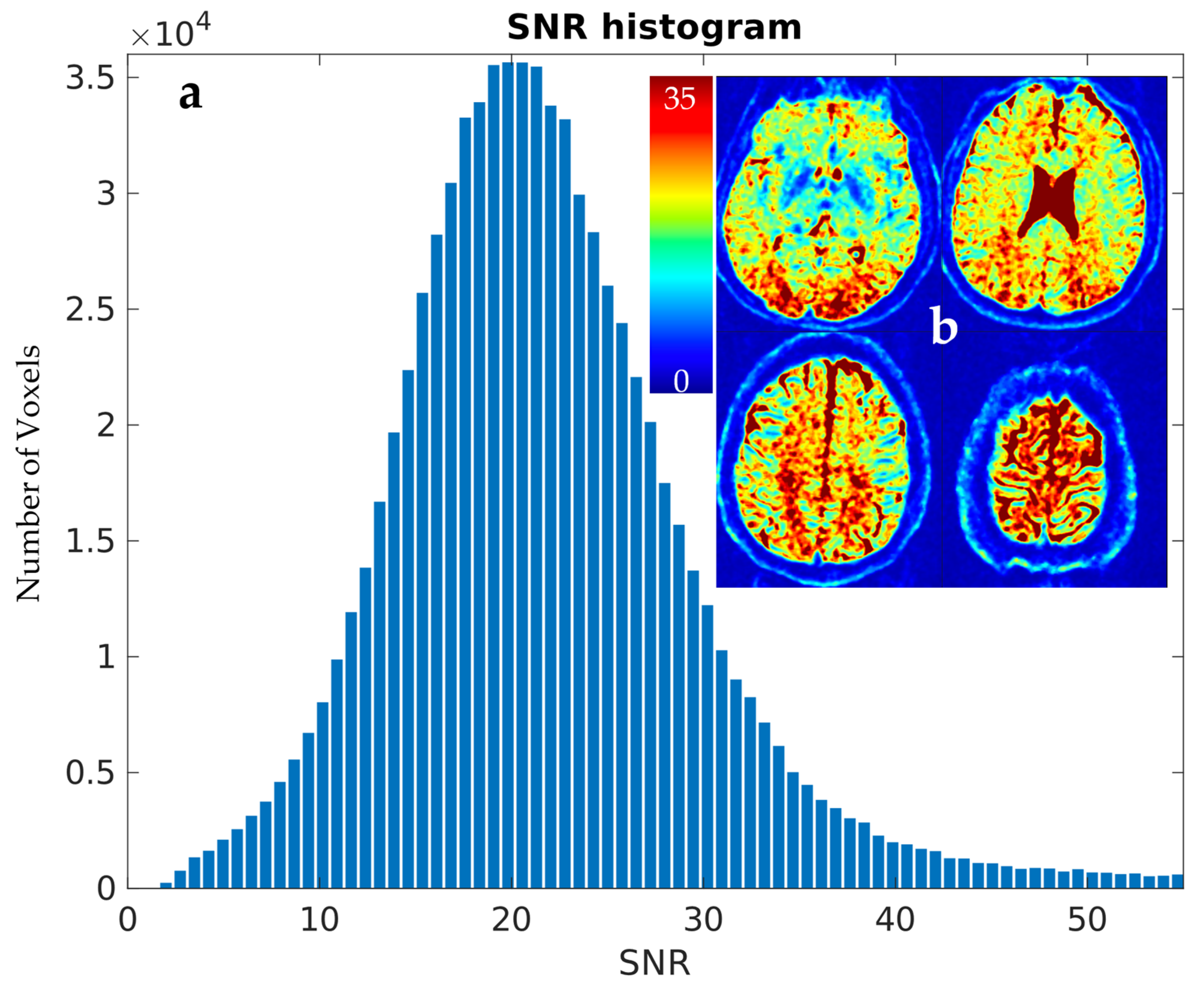
3.1. Estimation of Scanner-Specific SNR
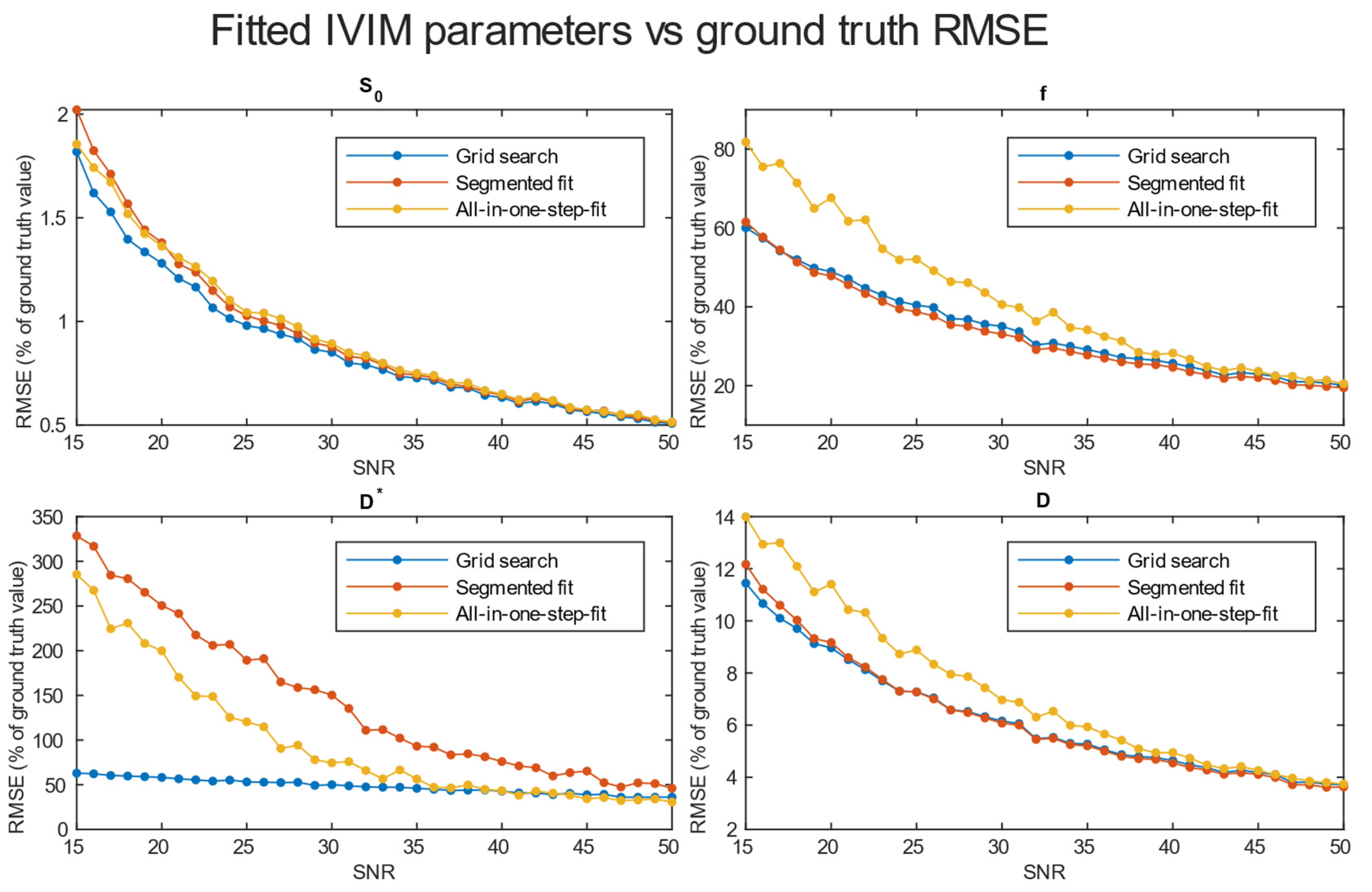
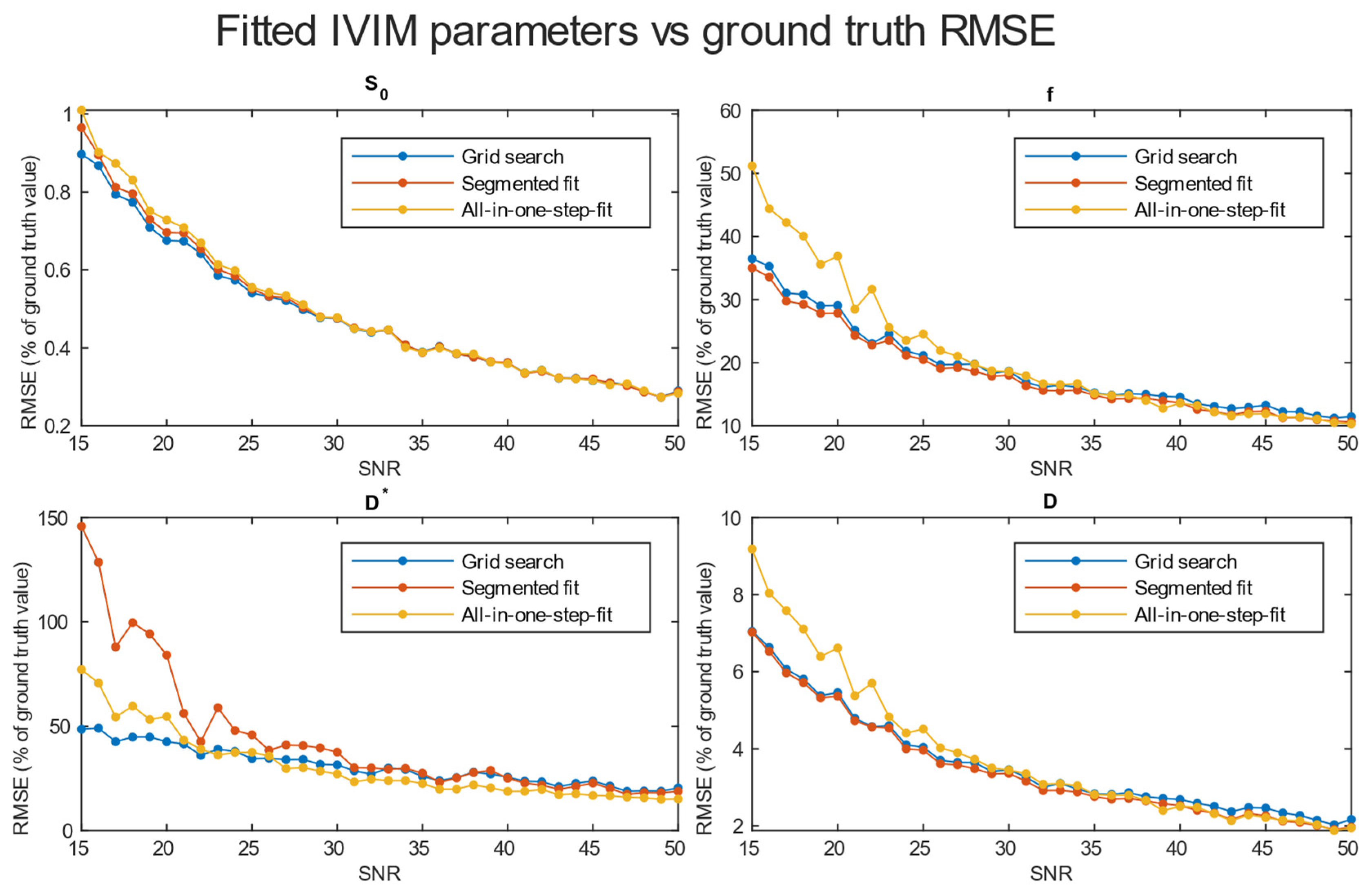
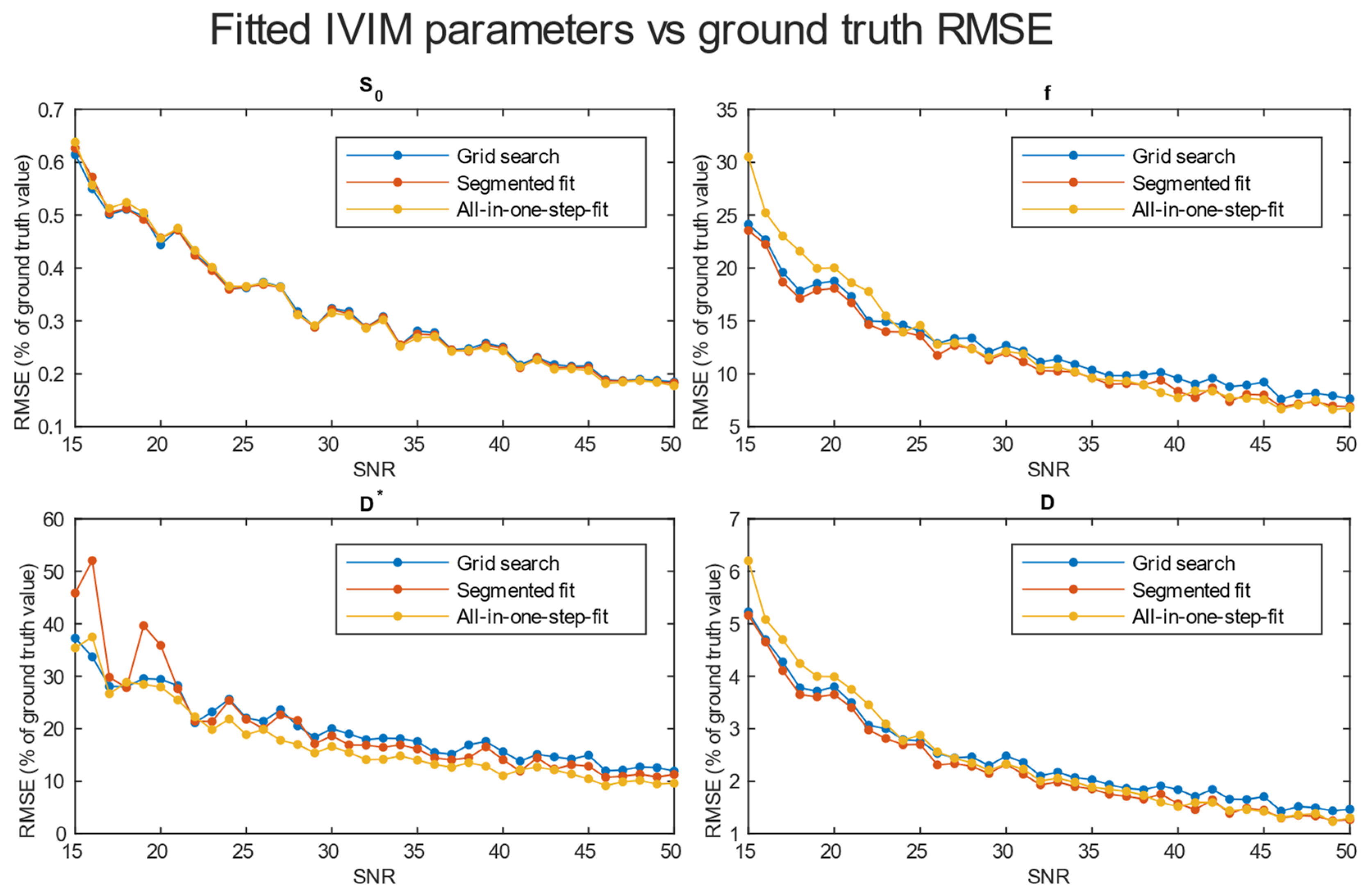
3.2. Evaluation of Accuracy
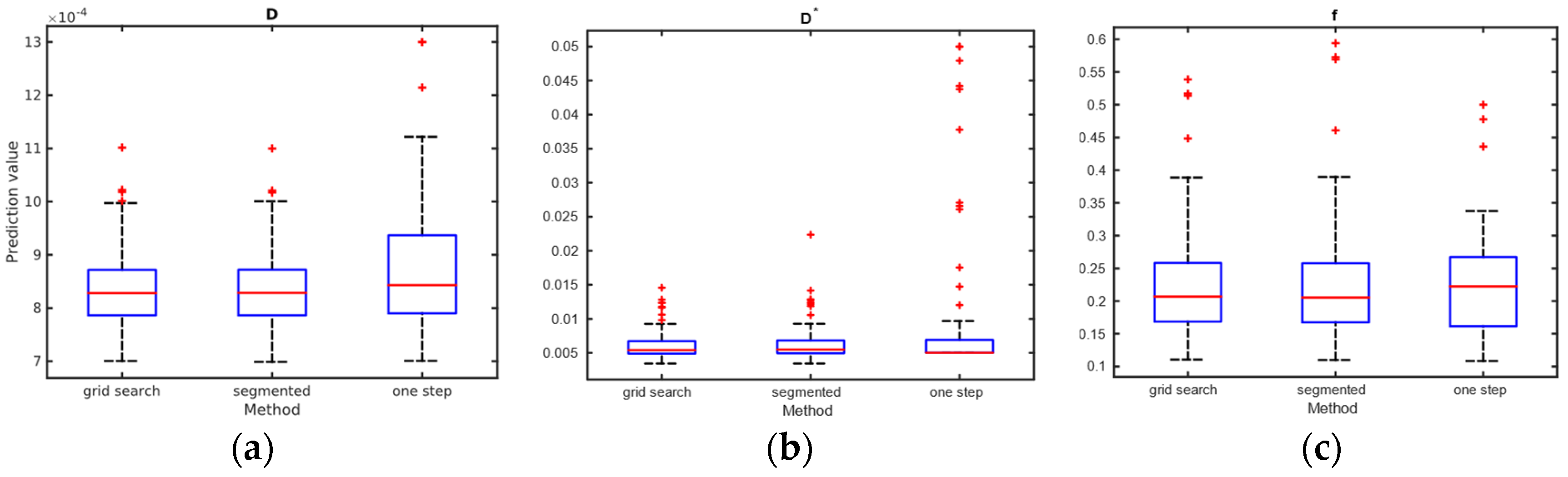
3.3. Results from Study
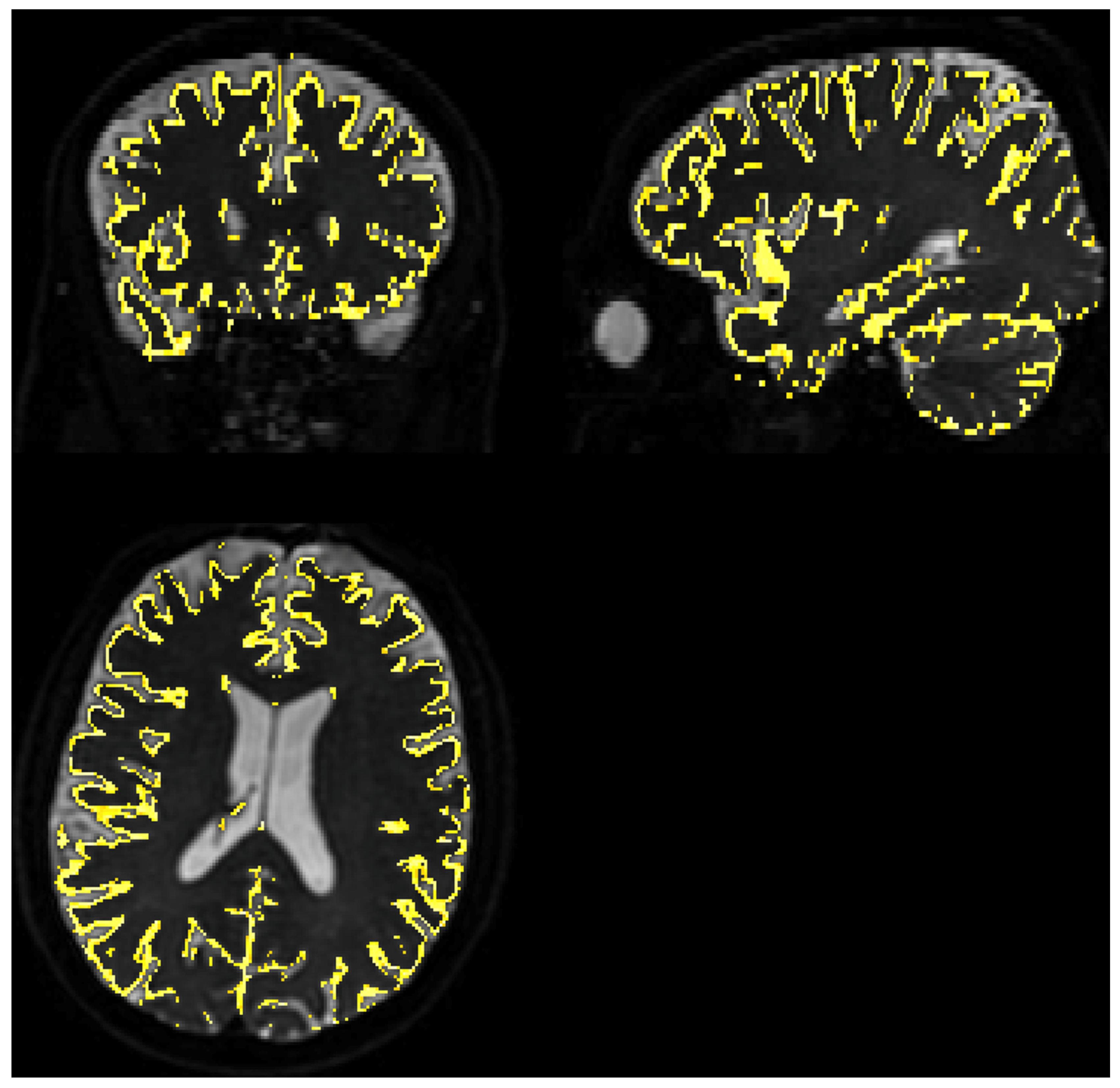
3.3.1. Quality of Matching Subject IVIM DWI Data to T2 MNI Template
3.3.2. Calculation of IVIM Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Essig, M.; Shiroishi, M.S.; Nguyen, T.B.; Saake, M.; Provenzale, J.M.; Enterline, D.; Anzalone, N.; Dörfler, A.; Rovira, À.; Wintermark, M.; et al. Perfusion MRI: The Five Most Frequently Asked Technical Questions. AJR Am. J. Roentgenol. 2013, 200, 24–34. [Google Scholar] [CrossRef] [PubMed]
- Wahsner, J.; Gale, E.M.; Rodríguez-Rodríguez, A.; Caravan, P. Chemistry of MRI Contrast Agents: Current Challenges and New Frontiers. Chem. Rev. 2019, 119, 957–1057. [Google Scholar] [CrossRef] [PubMed]
- Le Bihan, D.; Breton, E.; Lallemand, D.; Grenier, P.; Cabanis, E.; Laval-Jeantet, M. MR Imaging of Intravoxel Incoherent Motions: Application to Diffusion and Perfusion in Neurologic Disorders. Radiology 1986, 161, 401–407. [Google Scholar] [CrossRef]
- Einstein, A. On the Movement of Small Particles Suspended in Stationary Liquids Required by the Molecular-Kinetic Theory of Heat. Ann. Phys. 1905, 322, 549–560. [Google Scholar] [CrossRef]
- Brown, R. XXVII. A Brief Account of Microscopical Observations Made in the Months of June, July and August 1827, on the Particles Contained in the Pollen of Plants; and on the General Existence of Active Molecules in Organic and Inorganic Bodies. Philos. Mag. 1828, 4, 161–173. [Google Scholar] [CrossRef]
- Stejskal, E.O.; Tanner, J.E. Spin Diffusion Measurements: Spin Echoes in the Presence of a Time-Dependent Field Gradient. J. Chem. Phys. 1965, 42, 288–292. [Google Scholar] [CrossRef]
- Le Bihan, D.; Breton, E.; Lallemand, D.; Aubin, M.L.; Vignaud, J.; Laval-Jeantet, M. Separation of Diffusion and Perfusion in Intravoxel Incoherent Motion MR Imaging. Radiology 1988, 168, 497–505. [Google Scholar] [CrossRef]
- Le Bihan, D. What Can We See with IVIM MRI? NeuroImage 2019, 187, 56–67. [Google Scholar] [CrossRef]
- Iima, M. Perfusion-Driven Intravoxel Incoherent Motion (IVIM) MRI in Oncology: Applications, Challenges, and Future Trends. Magn. Reson. Med. Sci. 2020, 20, 125–138. [Google Scholar] [CrossRef]
- Federau, C.; O’Brien, K.; Meuli, R.; Hagmann, P.; Maeder, P. Measuring Brain Perfusion with Intravoxel Incoherent Motion (IVIM): Initial Clinical Experience. J. Magn. Reson. Imaging 2014, 39, 624–632. [Google Scholar] [CrossRef]
- Li, Y.T.; Cercueil, J.-P.; Yuan, J.; Chen, W.; Loffroy, R.; Wáng, Y.X.J. Liver Intravoxel Incoherent Motion (IVIM) Magnetic Resonance Imaging: A Comprehensive Review of Published Data on Normal Values and Applications for Fibrosis and Tumor Evaluation. Quant. Imaging Med. Surg. 2017, 7, 59–78. [Google Scholar] [CrossRef]
- Rydhög, A.S.; van Osch, M.J.P.; Lindgren, E.; Nilsson, M.; Lätt, J.; Ståhlberg, F.; Wirestam, R.; Knutsson, L. Intravoxel Incoherent Motion (IVIM) Imaging at Different Magnetic Field Strengths: What Is Feasible? Magn. Reson. Imaging 2014, 32, 1247–1258. [Google Scholar] [CrossRef] [PubMed]
- Birenbaum, D.; Bancroft, L.W.; Felsberg, G.J. Imaging in Acute Stroke. West. J. Emerg. Med. 2011, 12, 67–76. [Google Scholar]
- Meeus, E.M.; Novak, J.; Withey, S.B.; Zarinabad, N.; Dehghani, H.; Peet, A.C. Evaluation of Intravoxel Incoherent Motion Fitting Methods in Low-Perfused Tissue: IVIM Fitting in Low-Perfused Tissue. J. Magn. Reson. Imaging 2017, 45, 1325–1334. [Google Scholar] [CrossRef] [PubMed]
- Bai, Y.; Pei, Y.; Liu, W.V.; Liu, W.; Xie, S.; Wang, X.; Zhong, L.; Chen, J.; Zhang, L.; Masokano, I.B.; et al. MRI: Evaluating the Application of FOCUS-MUSE Diffusion-Weighted Imaging in the Pancreas in Comparison with FOCUS, MUSE, and Single-Shot DWIs. J. Magn. Reson. Imaging 2023, 57, 1156–1171. [Google Scholar] [CrossRef]
- Paganelli, C.; Zampini, M.A.; Morelli, L.; Buizza, G.; Fontana, G.; Anemoni, L.; Imparato, S.; Riva, G.; Iannalfi, A.; Orlandi, E.; et al. Optimizing b-values Schemes for Diffusion MRI of the Brain with Segmented Intravoxel Incoherent Motion (IVIM) Model. J. Appl. Clin. Med. Phys. 2023, 24, e13986. [Google Scholar] [CrossRef]
- Veraart, J.; Fieremans, E.; Novikov, D.S. Diffusion MRI Noise Mapping Using Random Matrix Theory. Magn. Reson. Med. 2016, 76, 1582–1593. [Google Scholar] [CrossRef] [PubMed]
- Veraart, J.; Novikov, D.S.; Christiaens, D.; Ades-Aron, B.; Sijbers, J.; Fieremans, E. Denoising of Diffusion MRI Using Random Matrix Theory. NeuroImage 2016, 142, 394–406. [Google Scholar] [CrossRef]
- Cordero-Grande, L.; Christiaens, D.; Hutter, J.; Price, A.N.; Hajnal, J.V. Complex Diffusion-Weighted Image Estimation via Matrix Recovery under General Noise Models. NeuroImage 2019, 200, 391–404. [Google Scholar] [CrossRef]
- Kellner, E.; Dhital, B.; Kiselev, V.G.; Reisert, M. Gibbs-Ringing Artifact Removal Based on Local Subvoxel-Shifts. Magn. Reson. Med. 2016, 76, 1574–1581. [Google Scholar] [CrossRef]
- Tournier, J.-D.; Smith, R.; Raffelt, D.; Tabbara, R.; Dhollander, T.; Pietsch, M.; Christiaens, D.; Jeurissen, B.; Yeh, C.-H.; Connelly, A. MRtrix3: A Fast, Flexible and Open Software Framework for Medical Image Processing and Visualisation. NeuroImage 2019, 202, 116137. [Google Scholar] [CrossRef]
- Jenkinson, M.; Beckmann, C.F.; Behrens, T.E.J.; Woolrich, M.W.; Smith, S.M. FSL. NeuroImage 2012, 62, 782–790. [Google Scholar] [CrossRef]
- Tustison, N.J.; Avants, B.B.; Cook, P.A.; Zheng, Y.; Egan, A.; Yushkevich, P.A.; Gee, J.C. N4ITK: Improved N3 Bias Correction. IEEE Trans. Med. Imaging 2010, 29, 1310–1320. [Google Scholar] [CrossRef]
- Avants, B.; Tustison, N.J.; Song, G. Advanced Normalization Tools: V1.0. Insight J. 2009, 2, 1–35. [Google Scholar] [CrossRef]
- The MathWorks Inc. MATLAB Version: R2023a; The MathWorks Inc.: Natick, MA, USA, 2023. [Google Scholar]
- Fonov, V.; Evans, A.; McKinstry, R.; Almli, C.; Collins, D. Unbiased Nonlinear Average Age-Appropriate Brain Templates from Birth to Adulthood. NeuroImage 2009, 47, S102. [Google Scholar] [CrossRef]
- Pijnenburg, R.; Scholtens, L.H.; Ardesch, D.J.; de Lange, S.C.; Wei, Y.; van den Heuvel, M.P. Myelo- and Cytoarchitectonic Microstructural and Functional Human Cortical Atlases Reconstructed in Common MRI Space. NeuroImage 2021, 239, 118274. [Google Scholar] [CrossRef]
- Friston, K.J. (Ed.) Statistical Parametric Mapping: The Analysis of Functional Brain Images, 1st ed; Elsevier: Amsterdam, The Netherlands; Boston, MA, USA, 2007; ISBN 978-0-12-372560-8. [Google Scholar]
- Chabert, S.; Verdu, J.; Huerta, G.; Montalba, C.; Cox, P.; Riveros, R.; Uribe, S.; Salas, R.; Veloz, A. Impact of b-Value Sampling Scheme on Brain IVIM Parameter Estimation in Healthy Subjects. Magn. Reson. Med. Sci. 2020, 19, 216–226. [Google Scholar] [CrossRef] [PubMed]
- The MathWorks Inc. Curve Fitter; The MathWorks Inc.: Natick, MA, USA, 2023. [Google Scholar]
- Bisdas, S.; Klose, U. IVIM Analysis of Brain Tumors: An Investigation of the Relaxation Effects of CSF, Blood, and Tumor Tissue on the Estimated Perfusion Fraction. Magn. Reson. Mater. Phys. Biol. Med. 2015, 28, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Merisaari, H.; Federau, C. Signal to Noise and b-Value Analysis for Optimal Intra-Voxel Incoherent Motion Imaging in the Brain. PLoS ONE 2021, 16, e0257545. [Google Scholar] [CrossRef]
- Cipolla, M.J. Anatomy and Ultrastructure. In The Cerebral Circulation; Morgan & Claypool Life Sciences: San Rafael, CA, USA, 2009. [Google Scholar]
- Chen, Z.; Li, H.; Wu, M.; Chang, C.; Fan, X.; Liu, X.; Xu, G. Caliber of Intracranial Arteries as a Marker for Cerebral Small Vessel Disease. Front. Neurol. 2020, 11, 558858. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Averaging | Grid Search | Segmented | One Step |
|---|---|---|---|
| Single voxel | |||
| S0 | 5.00 | 7.18 | 3.98 |
| F | 81.91 | 96.84 | 98.40 |
| D* | 76.31 | 503.04 | 637.46 |
| D | 18.34 | 24.01 | 19.24 |
| 2 × 2 × 2 | |||
| S0 | 1.28 | 1.38 | 1.36 |
| F | 48.94 | 47.86 | 67.67 |
| D* | 58.19 | 250.51 | 199.91 |
| D | 8.97 | 9.16 | 11.41 |
| 3 × 3 × 3 | |||
| S0 | 0.68 | 0.70 | 0.73 |
| F | 29.07 | 27.85 | 36.89 |
| D* | 42.57 | 84.06 | 54.69 |
| D | 5.46 | 5.36 | 6.61 |
| 4 × 4 × 4 | |||
| S0 | 0.44 | 0.46 | 0.46 |
| F | 18.77 | 18.08 | 20.02 |
| D* | 29.42 | 35.88 | 27.96 |
| D | 3.80 | 3.65 | 3.99 |
| Parameters | Grid Search | Segmented | One Step |
|---|---|---|---|
| White matter | |||
| f | 0.16 | 0.16 | 0.14 |
| ] | 5.17 | 5.24 | 5.06 |
| ] | 0.79 | 0.79 | 0.82 |
| Grey matter | |||
| f | 0.09 | 0.08 | 0.05 |
| ] | 3.62 | 3.71 | 5.00 |
| ] | 0.65 | 0.66 | 0.69 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lipiński, K.; Bogorodzki, P. Evaluation of Whole Brain Intravoxel Incoherent Motion (IVIM) Imaging. Diagnostics 2024, 14, 653. https://doi.org/10.3390/diagnostics14060653
Lipiński K, Bogorodzki P. Evaluation of Whole Brain Intravoxel Incoherent Motion (IVIM) Imaging. Diagnostics. 2024; 14(6):653. https://doi.org/10.3390/diagnostics14060653
Chicago/Turabian StyleLipiński, Kamil, and Piotr Bogorodzki. 2024. "Evaluation of Whole Brain Intravoxel Incoherent Motion (IVIM) Imaging" Diagnostics 14, no. 6: 653. https://doi.org/10.3390/diagnostics14060653
APA StyleLipiński, K., & Bogorodzki, P. (2024). Evaluation of Whole Brain Intravoxel Incoherent Motion (IVIM) Imaging. Diagnostics, 14(6), 653. https://doi.org/10.3390/diagnostics14060653