

Assessing Patient Radiation Exposure in Endoscopic Retrograde Cholangiopancreatography: A Multicenter Retrospective Analysis of Procedural Complexity and Clinical Factors
 , ,
, ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Data Collection
2.2. Statistical Analysis
3. Results
3.1. Clinical Features of Patients and Procedural Characteristics
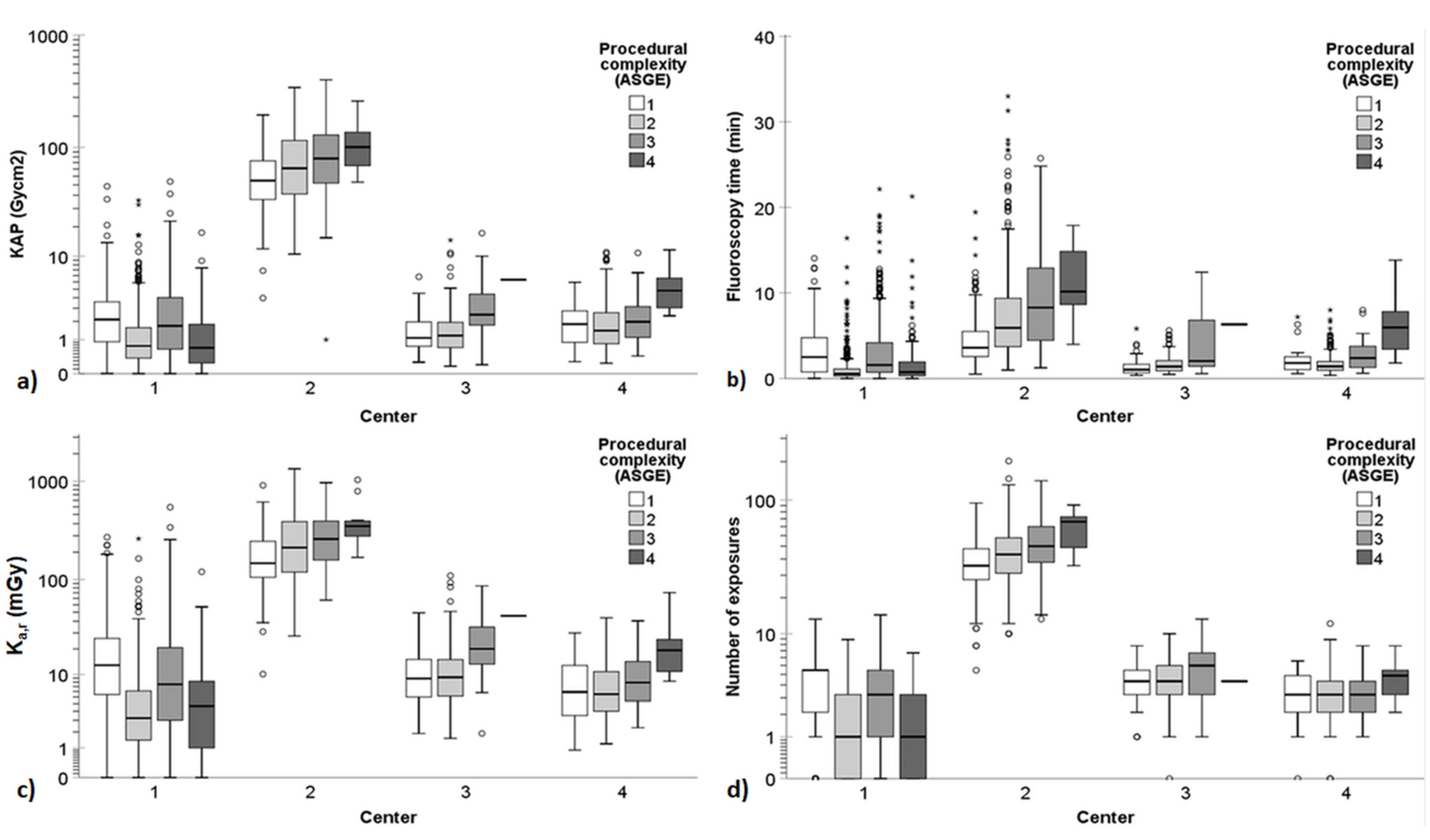
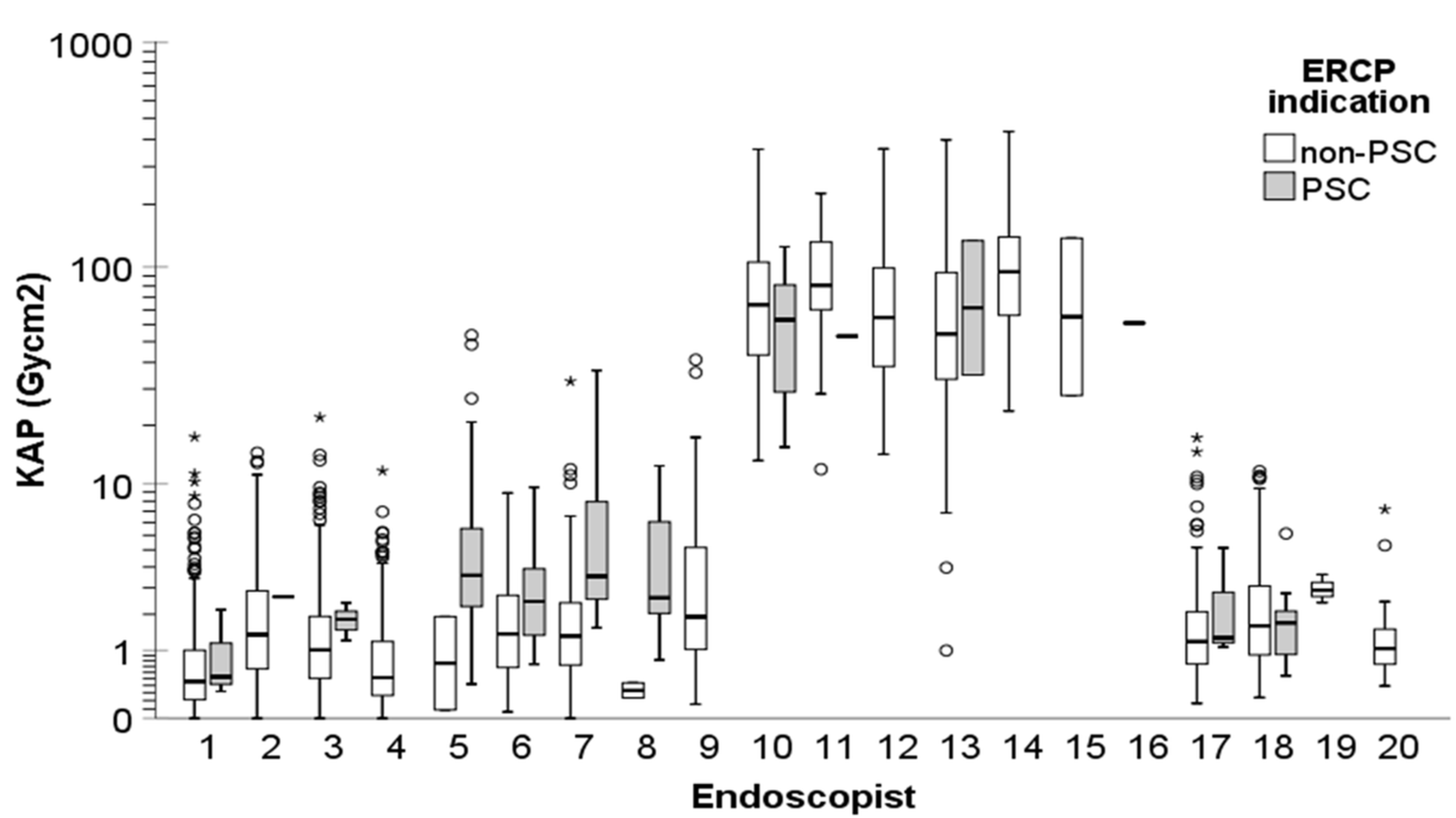
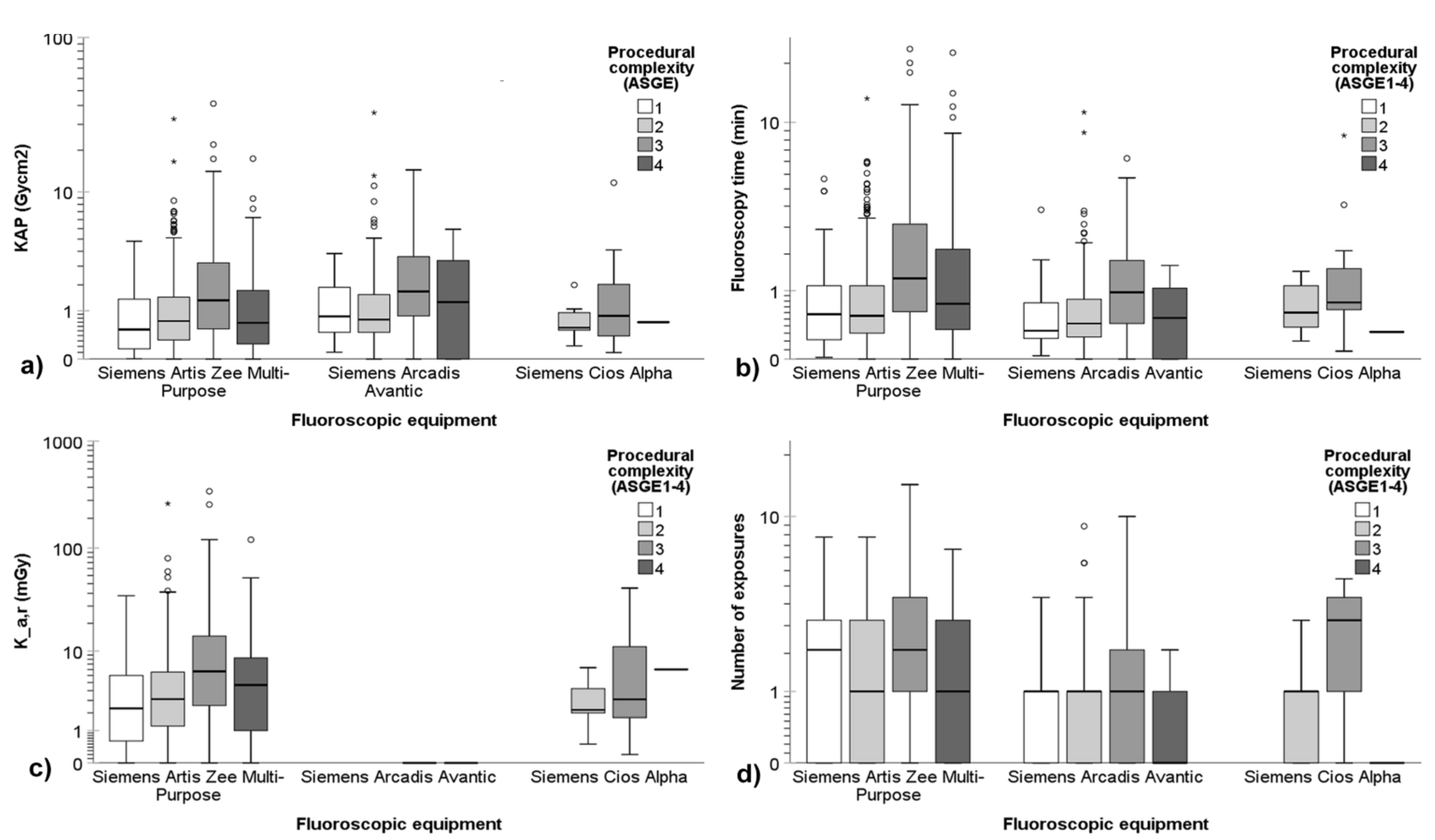
3.2. Radiation Exposure Quantities of the Procedures
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Donato, G.; Occhipinti, P.; Correale, L.; Spadaccini, M.; Repici, A.; Anderloni, A.; Fugazza, A.; Mosca, P.; Tringali, A.; Costamagna, G.; et al. A prospective study on quality in endoscopic retrograde cholangiopancreatography (ERCP): Trend in Italy from the REQUEST study. Endosc. Int. Open 2021, 9, E1563–E1571. [Google Scholar] [CrossRef] [PubMed]
- Abbarh, S.; Seleem, M.; Al Balkhi, A.; Al Mtawa, A.; Al Khathlan, A.; Qutub, A.; Al Sayari, K.; Al Otaibi, N.; AlEid, A.; Al Ghamdi, A.; et al. ERCP quality indicators: The experience of a high-volume tertiary care center in Saudi Arabia. Arab J. Gastroenterol. 2019, 20, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, S.; Takenaka, M.; Hosono, M.; Nishida, T. Radiation exposure during image-guided endoscopic procedures: The next quality indicator for endoscopic retrograde cholangiopancreatography. World J. Clin. Cases 2018, 6, 1087–1093. [Google Scholar] [CrossRef] [PubMed]
- Gilissen, L.P.; Meijer, S.; Flink, H.; Friederich, P.; Ramaker, J.; Schoon, E.; Stronkhorst, A. The Dutch national ERCP quality registration using self-assessment does not correlate with clinical ERCP outcome. Trends Med. 2020, 20, 1–6. [Google Scholar] [CrossRef]
- Pokala, S.K.; Jones, B.; Wani, S. Quality in advanced endoscopy. Tech. Innov. Gastrointest. Endosc. 2022, 24, 300–308. [Google Scholar] [CrossRef]
- Faulx, A.L.; Lightdale, J.R.; Acosta, R.D.; Agrawal, D.; Bruining, D.H.; Chandrasekhara, V.; Eloubeidi, M.A.; Gurudu, S.R.; Kelsey, L.; Khashab, M.A.; et al. Guidelines for privileging, credentialing, and proctoring to perform GI endoscopy. Gastrointest. Endosc. 2017, 85, 273–281. [Google Scholar] [CrossRef] [PubMed]
- Adler, D.G.; Lieb, J.G., II.; Cohen, J.; Pike, I.M.; Park, W.G.; Rizk, M.K.; Sawhney, M.S.; Scheiman, J.M.; Shaheen, N.J.; Sherman, S.; et al. Quality indicators for ERCP. Am. J. Gastroenterol. 2015, 110, 91–101. [Google Scholar] [CrossRef]
- Domagk, D.; Oppong, K.W.; Aabakken, L.; Czakó, L.; Gyökeres, T.; Manes, G.; Meier, P.; Poley, J.W.; Ponchon, T.; Tringali, A.; et al. Performance measures for endoscopic retrograde cholangiopancreatography and endoscopic ultrasound: A European Society of Gastrointestinal Endoscopy (ESGE) Quality Improvement Initiative. United Eur. Gastroenterol. J. 2018, 6, 1448–1460. [Google Scholar] [CrossRef]
- British Society of Gastroenterology ERCP Working Party. ERCP—The Way Forward, a Standards Framework. United Kingdom. 2014. Available online: https://www.bsg.org.uk/clinical-resource/ercp-the-way-forward-a-standards-framework/ (accessed on 17 January 2024).
- Springer, J.; Enns, R.; Romagnuolo, J.; Ponich, T.; Barkun, A.N.; Armstrong, D. Canadian credentialing guidelines for endoscopic retrograde cholangiopancreatography. Can. J. Gastroenterol. 2008, 22, 547–551. [Google Scholar] [CrossRef]
- Alharbi, A.; AlAmeel, T.; Aljebreen, A.; Almadi, M. Saudi gastroenterology association position statement on privilege and credentialing for performing endoscopic retrograde cholangiopancreatography in Saudi Arabia. Saudi J. Gastroenterol. 2014, 20, 329–330. [Google Scholar] [CrossRef]
- ICRP. The 2007 recommendations of the International Commission on Radiological Protection. ICRP Publication 103. Ann. ICRP 2007, 37, 1–332. [Google Scholar]
- Brenner, D.J.; Hall, E.J. Computed tomography—An increasing source of radiation exposure. N. Engl. J. Med. 2007, 357, 2277–2284. [Google Scholar] [CrossRef] [PubMed]
- Pearce, M.S.; Salotti, J.A.; Little, M.P.; McHugh, K.; Lee, C.; Kim, K.P.; Howe, N.L.; Ronckers, C.M.; Rajaraman, P.; Craft, A.W.; et al. Radiation exposure from CT scans in childhood and subsequent risk of leukaemia and brain tumours: A retrospective cohort study. Lancet 2012, 380, 499–505. [Google Scholar] [CrossRef]
- Alkhatib, A.A.; Abdel Jalil, A.A.; Faigel, D.O.; Pannala, R.; Crowell, M.; Harrison, M.E. Anatomical location of pathology is predictive of prolonged fluoroscopy time during ERCP: A multicenter American study. Dig. Dis. Sci. 2015, 60, 1787–1792. [Google Scholar] [CrossRef] [PubMed]
- Churrango, G.; Deutsch, J.K.; Dinneen, H.S.; Churrango, J.; Samiullah, S.; Ahlawat, S.K. Minimizing radiation exposure during ERCP by avoiding live or continuous fluoroscopy. J. Clin. Gastroenterol. 2015, 49, e96–e100. [Google Scholar] [CrossRef] [PubMed]
- Jorgensen, J.E.; Rubenstein, J.H.; Goodsitt, M.M.; Elta, G.H. Radiation doses to ERCP patients are significantly lower with experienced endoscopists. Gastrointest. Endosc. 2010, 72, 58–65. [Google Scholar] [CrossRef]
- Jowhari, F.; Hopman, W.M.; Hookey, L. A simple ergonomic measure reduces fluoroscopy time during ERCP: A multivariate analysis. Endosc. Int. Open 2017, 5, E172–E178. [Google Scholar] [CrossRef]
- Katsinelos, P.; Gatopoulou, A.; Gkagkalis, S.; Fasoulas, K.; Beltsis, A.; Zavos, C.; Terzoudis, S.; Lazaraki, G.; Chatzimavroudis, G.; Vasiliadis, I.; et al. A prospective analysis of factors influencing fluoroscopy time during therapeutic ERCP. Ann. Gastroenterol. 2012, 25, 338–344. [Google Scholar]
- Liao, C.; Thosani, N.; Kothari, S.; Friedland, S.; Chen, A.; Banerjee, S. Radiation exposure to patients during ERCP is significantly higher with low-volume endoscopists. Gastrointest. Endosc. 2015, 81, 391–398. [Google Scholar] [CrossRef]
- Lorenzo-Zúñiga, V.; Álvarez, M.A.; de Vega, V.M.; Seoane, A.; Bory, F.; Boix, J. Predictive factors of radiation dose in ERCP: A prospective study in 2 tertiary centers. Surg. Laparosc. Endosc. Percutaneous Tech. 2013, 23, 266–270. [Google Scholar] [CrossRef]
- Oztas, E.; Parlak, E.; Kucukay, F.; Arhan, M.; Daglı, U.; Etik, D.O.; Onder, F.O.; Olcer, T.; Sasmaz, N. The impact of endoscopic retrograde cholangiopancreatography education on radiation exposure to experienced endoscopist: ‘trainee effect’. Dig. Dis. Sci. 2012, 57, 1134–1143. [Google Scholar] [CrossRef] [PubMed]
- Tsapaki, V.; Paraskeva, K.D.; Tsalafoutas, I.A.; Paspatis, G.; Scotiniotis, H.; Georgopoulos, P.; Finou, P.; Karagianis, J.A. The impact of X-ray unit type used for endoscopic retrograde cholangiopancreatography procedures on patient doses. Radiat. Prot. Dosim. 2016, 171, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Saukko, E.; Grönroos, J.M.; Salminen, P.; Henner, A.; Nieminen, M.T. Patient radiation dose and fluoroscopy time during ERCP: A single-center, retrospective study of influencing factors. Scand. J. Gastroenterol. 2018, 53, 495–504. [Google Scholar] [CrossRef] [PubMed]
- Barakat, M.T.; Gugig, R.; Imperial, J.; Berquist, W.E. Fluoroscopy time during endoscopic retrograde cholangiopancreatography performed for children and adolescents is significantly higher with low-volume endoscopists. J. Pediatr. Gastroenterol. Nutr. 2021, 72, 244–249. [Google Scholar] [CrossRef] [PubMed]
- Syed, A.R.; Garg, M.S.; Patel, P.; Singh, S.; Blackwood, M.; Munigala, S.; Thakkar, P.; Farah, K.; Aoun, E.; Kulkarni, A.; et al. Fluoroscopy dose and time characteristics during endoscopic retrograde cholangiopancreatography (ERCP). Surg. Laparosc. Endosc. Percutaneous Tech. 2019, 29, 22–25. [Google Scholar] [CrossRef] [PubMed]
- Hadjiconstanti, A.C.; Messaris, G.A.T.; Thomopoulos, K.C.; Panayiotakis, G.S. Patient radiation doses in therapeutic endoscopic retrograde cholangiopancreatography in Patras and the key role of the operator. Radiat. Prot. Dosim. 2017, 177, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.; Park, J.; Ahn, J.; Jung, K.; Jung, J.H.; Lee, J.C.; Hwang, J.H.; Kim, J. Prediction model using clinical factors for radiation exposure during endoscopic retrograde cholangiopancreatography. J. Gastroenterol. Hepatol. 2022, 37, 1342–1348. [Google Scholar] [CrossRef] [PubMed]
- Kaasalainen, T.; Pekkarinen, A.; Kylänpää, L.; Rainio, M.; Tenca, A.; Jokelainen, K.; Barner-Rasmussen, N.; Puustinen, L.; Udd, M.; Lindström, O. Occupational dose from gastrointestinal endoscopy procedures with special emphasis on eye lens doses in endoscopic retrograde cholangiopancreatography. Endosc. Int. Open 2023, 11, E237–E246. [Google Scholar] [CrossRef]
- Vañó, E.; Miller, D.L.; Martin, C.J.; Rehani, M.M.; Kang, K.; Rosenstein, M.; Ortiz-López, P.; Mattsson, S.; Padovani, R.; Rogers, A. ICRP publication 135: Diagnostic reference levels in medical imaging. Ann. ICRP 2017, 46, 1–144. [Google Scholar] [CrossRef]
- Schutz, S.M.; Abbott, R.M. Grading ERCPs by degree of difficulty: A new concept to produce more meaningful outcome data. Gastrointest. Endosc. 2000, 51, 535–539. [Google Scholar] [CrossRef]
- Cotton, P.B.; Eisen, G.; Romagnuolo, J.; Vargo, J.; Baron, T.; Tarnasky, P.; Schutz, S.; Jacobson, B.; Bott, C.; Petersen, B. Grading the complexity of endoscopic procedures: Results of an ASGE working party. Gastrointest. Endosc. 2011, 73, 868–874. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Zhan, X.; Song, C.; Li, G.; Hong, J.; Chen, Y.; Zhou, X. The assessment of the ASGE-grading system of ERCP: A large-sample retrospective study. Surg. Endosc. 2022, 36, 6480–6487. [Google Scholar] [CrossRef] [PubMed]
- Olsson, G.; Arnelo, U.; Swahn, F.; Törnqvist, B.; Lundell, L.; Enochsson, L. The HOUSE classification: A novel endoscopic retrograde cholangiopancreatography (ERCP) complexity grading scale. BMC Gastroenterol. 2017, 17, 38. [Google Scholar] [CrossRef]
- O’Connor, U.; Gallagher, A.; Malone, L.; O’Reilly, G. Occupational radiation dose to eyes from endoscopic retrograde cholangiopancreatography procedures in light of the revised eye lens dose limit from the International Commission on Radiological Protection. Br. J. Radiol. 2013, 86, 20120289. [Google Scholar] [CrossRef] [PubMed]
- National Council on Radiation Protection and Measurements. Ionizing Radiation Exposure of the Population of the United States. NCRP Report No. 160; National Council on Radiation Protection and Measurements: Bethesda, MD, USA, 2009. [Google Scholar]
- The United Nations Scientific Committee on the Effects of Atomic Radiation. UNSCEAR 2016; United Nations Environment Programme (UNEP) Booklet: Radiation Effects and Sources; United Nations: New York, NY, USA, 2016; Available online: https://www.unscear.org/unscear/en/publications/booklet.html (accessed on 11 March 2024).
- Martin, C.J.; Harrison, J.D.; Rehani, M.M. Effective dose from radiation exposure in medicine: Past, present, and future. Phys. Med. 2020, 79, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Martin, C.J. Effective dose in medicine. Ann. ICRP 2020, 49, 126–140. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Total |
|---|---|
| Gender (n = 2640) [n (%)] | |
| Female | 1243 (47.1) |
| Male | 1397 (52.9) |
| Age (y, n = 2640) [median (IQR)] | 66.0 (52.0–76.7) |
| BMI (kg/m2, n = 2512) [median (IQR)] | 25.4 (22.6–28.8) |
| Native papilla (n = 2640) [n (%)] | |
| Yes | 1491 (56.5) |
| No | 1133 (42.9) |
| Other (e.g., hepaticojejunostomy) | 16 (0.6) |
| Previous EST (n = 2630) [n (%)] | |
| No | 1591 (60.5) |
| Biliary EST only | 774 (29.4) |
| Pancreatic EST only | 147 (5.6) |
| Biliary and pancreatic EST | 118 (4.5) |
| Anesthetic technique (n = 2632) [n (%)] | |
| Endoscopist-directed | 714 (27.1) |
| Anesthesiologist-directed | 1918 (72.9) |
| Indication (n = 3026) [n (%)] | |
| CBD stone | 1084 (35.8) |
| Biliary stricture | 818 (27.0) |
| PSC | 321 (10.6) |
| Post LCC | 116 (3.8) |
| Post LTx | 84 (2.8) |
| Chronic pancreatitis | 235 (7.8) |
| Acute pancreatitis | 89 (2.9) |
| Pseudocyst | 126 (4.2) |
| Other | 153 (5.1) |
| Total cannulation time (min, n = 756) [median (IQR)] | 1.08 (0.25–5.67) |
| Types of interventions (n = 5519) [n (%)] | |
| Biliary EST | 1387 (25.1) |
| CBD stone extraction | 1033 (18.7) |
| Biliary plastic stent placement, exchange, or removal | 800 (14.5) |
| ERC cytology | 691 (12.5) |
| Biliary dilatation | 407 (7.4) |
| Metal stent placement | 359 (6.5) |
| Pancreatic stent placement, exchange, or removal | 259 (4.7) |
| Pancreatic EST | 190 (3.4) |
| Pancreatic dilatation | 158 (2.9) |
| ERP cytology | 62 (1.1) |
| Pseudocystogastrostomy | 26 (0.5) |
| Prophylactic pancreatic stent | 29 (0.6) |
| Spyglass | 56 (1.0) |
| Double-balloon ERCP | 62 (1.1) |
| Total procedural time (min, n = 2555) [median (IQR)] | 22.0 (15.0–33.0) |
| Operator of fluoroscopy equipment (n = 2640) [n (%)] | |
| Endoscopist | 2195 (83.1) |
| Radiographer | 445 (16.9) |
| Endoscopist | Non-PSC/PSC | ASGE Complexity (Non-PSC/PSC) | HOUSE Complexity (Non-PSC/PSC) | |||||
|---|---|---|---|---|---|---|---|---|
| Level 1 | Level 2 | Level 3 | Level 4 | Level 1 | Level 2 | Level 3 | ||
| Center 1 | ||||||||
| #1 | 209/4 | 9/0 | 69/0 | 72/2 | 59/2 | 82/0 | 53/1 | 74/3 |
| #2 | 230/1 | 17/1 | 98/0 | 95/0 | 20/0 | 108/0 | 68/1 | 54/0 |
| #3 | 331/3 | 48/0 | 118/0 | 148/1 | 17/2 | 169/0 | 114/1 | 48/2 |
| #4 | 252/0 | 15/0 | 170/0 | 65/0 | 2/0 | 180/0 | 42/0 | 30/0 |
| #5 | 2/178 | 1/117 | 0/9 | 0/52 | 1/0 | 0/1 | 1/176 | 1/1 |
| #6 | 25/54 | 1/35 | 5/4 | 2/15 | 17/0 | 6/0 | 2/54 | 17/0 |
| #7 | 94/19 | 6/17 | 63/0 | 24/2 | 1/0 | 71/0 | 15/19 | 8/0 |
| #8 | 2/29 | 0/18 | 0/1 | 0/10 | 2/0 | 1/0 | 0/29 | 1/0 |
| #9 | 67/0 | 0/0 | 23/0 | 38/0 | 6/0 | 22/0 | 27/0 | 18/0 |
| Center2 | ||||||||
| #10 | 191/6 | 33/1 | 129/2 | 23/3 | 6/0 | 145/0 | 18/6 | 28/0 |
| #11 | 75/1 | 22/0 | 47/0 | 5/0 | 1/1 | 64/0 | 2/0 | 9/1 |
| #12 | 172/0 | 47/0 | 110/0 | 15/0 | 0/0 | 148/0 | 4/0 | 20/0 |
| #13 | 184/2 | 23/0 | 133/2 | 25/0 | 3/0 | 127/0 | 44/2 | 13/0 |
| #14 | 62/0 | 14/0 | 34/0 | 13/0 | 1/0 | 56/0 | 4/0 | 2/0 |
| #15 | 2/0 | 0/0 | 2/0 | 0/0 | 0/0 | 2/0 | 0/0 | 0/0 |
| #16 | 1/0 | 0/0 | 0/0 | 1/0 | 0/0 | 1/0 | 0/0 | 0/0 |
| Center 3 | ||||||||
| #17 | 167/4 | 40/3 | 107/1 | 19/0 | 1/0 | 156/1 | 9/2 | 2/1 |
| Center 4 | ||||||||
| #18 | 236/20 | 17/13 | 164/5 | 45/2 | 10/0 | 191/0 | 6/16 | 39/4 |
| #19 | 3/0 | 1/0 | 2/0 | 0/0 | 0/0 | 3/0 | 0/0 | 0/0 |
| #20 | 15/0 | 0/0 | 14/0 | 1/0 | 0/0 | 13/0 | 2/0 | 0/0 |
| Center and Complexity Level (ERCPs Without PSC/with PSC) | Fluoroscopy Time, min | KAP, Gy·cm2 | Ka,r, mGy | Number of Exposures | ||||
|---|---|---|---|---|---|---|---|---|
| w/o PSC | PSC | w/o PSC | PSC | w/o PSC | PSC | w/o PSC | PSC | |
| Center 1 (1212/288) | 0.7 (0.4–1.6) | 4.8 (2.7–7.6) | 0.9 (0.4–1.9) | 3.0 (2.0–5.5) | 3.7 (1.6–9.1) | 19.9 (12.5–39.0) | 2 (0–3) | 5 (5–6) |
| Level 1 (97/188) | 0.5 (0.2–1.1) | 4.1 (2.3–6.1) | 0.6 (0.2–1.4) | 2.6 (1.8–4.7) | 2.2 (0.6–5.5) | 16.8 (10.6–32.3) | 1 (0–3) | 5 (4–6) |
| Level 2 (546/14) | 0.5 (0.3–1.0) | 7.0 (4.4–8.7) | 0.7 (0.4–1.5) | 4.7 (2.5–5.8) | 2.9 (1.2–6.0) | 32.3 (22.6–53.8) | 1 (0–2) | 6 (5–6) |
| Level 3 (444/82) | 1.2 (0.6–2.9) | 7.5 (5.2–9.8) | 1.3 (0.6–3.0) | 4.0 (2.4–6.7) | 5.9 (2.4–14.2) | 31.5 (17.3–53.3) | 2 (1–4) | 5 (5–6) |
| Level 4 (125/4) | 0.7 (0.3–1.9) | 1.3 (1.0–2.7) | 0.7 (0.2–1.7) | 1.1 (0.4–2.0) | 4.3 (1.0–8.4) | 6.0 (3.9–8.3) | 1 (0–3) | 4 (3–4) |
| p-value (complexity levels) | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | 0.002 |
| p-value (PSC vs. w/o PSC) | <0.001 | <0.001 | <0.001 | <0.001 | ||||
| Center 2 (687/9) | 5.5 (3.5–9.4) | 4.5 (3.9–6.9) | 64.4 (38.1–106.7) | 49.6 (32.5–83.0) | 207.1 (120.1–350.7) | 264.3 (118.7–461.4) | 40 (29–52) | 38 (36–59) |
| Level 1 (139/1) | 3.6 (2.6–5.5) | 3.1 (3.1–3.1) | 50.3 (33.7–76.2) | 49.6 (49.6–49.6) | 146.1 (104.6–246.8) | 243.4 (243.4–243.4) | 33 (26–44) | 38 (38–38) |
| Level 2 (455/4) | 5.9 (3.7–9.4) | 6.5 (6.5–18.9) | 64.8 (38.0–114.7) | 103.1 (57.8–127.1) | 207.3 (117.8–381.8) | 510.1 (290.1–580.7) | 40 (29–52) | 62 (48–76) |
| Level 3 (82/3) | 8.3 (4.9–13.9) | 2.0 (2.0–4.5) | 81.6 (48.3–132.4) | 27.1 (15.0–67.2) | 259.5 (161.5–439.3) | 113.0 (61.5–273.1) | 47 (35–65) | 35 (23–36) |
| Level 4 (11/1) | 10.3 (9.1–16.2) | 4.0 (4.0–4.0) | 108.1 (68.7–143.6) | 48.7 (48.7–48.7) | 363.3 (289.3–400.8) | 264.3 (264.3–264.3) | 70 (47–78) | 43 (43–43) |
| p-value (complexity levels) | <0.001 | 0.099 | <0.001 | 0.338 | <0.001 | 0.338 | <0.001 | 0.118 |
| p-value (PSC vs. w/o PSC | 0.771 | 0.430 | 0.456 | 0.532 | ||||
| Center 3 (167/4) | 1.4 (0.8–2.3) | 2.9 (2.0–4.0) | 1.2 (0.7–2.0) | 1.3 (1.2–2.2) | 9.7 (5.7–16.0) | 11.0 (10.3–14.3) | 4 (3–6) | 5 (4–6) |
| Level 1 (40/3) | 0.9 (0.7–1.5) | 2.1 (1.7–3.8) | 1.0 (0.7–1.9) | 1.3 (1.1–1.3) | 8.9 (5.3–15.2) | 10.8 (8.6–11.1) | 4 (3–5) | 5 (1–5) |
| Level 2 (107/1) | 1.4 (0.9–2.0) | 4.7 (4.7–4.7) | 1.2 (0.7–1.8) | 4.7 (4.7–4.7) | 9.3 (5.6–14.4) | 23.9 (23.9–23.9) | 4 (3–5) | 8 (8–8) |
| Level 3 (19/0) | 2.0 (1.4–6.8) | – | 2.3 (1.7–4.1) | – | 19.1 (13.0–32.3) | – | 6 (3–7) | – |
| Level 4 (1/0) | 6.3 (6.3–6.3) | – | 5.8 (5.8–5.8) | – | 42.2 (42.2–42.2) | – | 4 (4–4) | – |
| p-value (complexity levels) | 0.002 | 0.500 | 0.003 | 0.500 | 0.003 | 0.500 | 0.320 | 0.500 |
| p-value (PSC vs. w/o PSC | 0.036 | 0.408 | 0.447 | 0.622 | ||||
| Center 4 (254/20) | 1.6 (1.0–2.6) | 1.8 (1.5–2.2) | 1.5 (0.9–2.8) | 1.7 (0.9–2.0) | 7.0 (3.9–12.5) | 5.6 (3.9–7.4) | 3 (2–4) | 3 (2–4) |
| Level 1 (18/13) | 2.4 (1.0–2.8) | 1.7 (1.4–2.1) | 2.2 (0.9–3.5) | 1.6 (0.9–1.8) | 10.6 (2.9–15.4) | 5.4 (3.4–6.3) | 3 (2–5) | 3 (3–4) |
| Level 2 (180/5) | 1.4 (1.0–2.0) | 1.7 (1.7–1.9) | 1.4 (0.8–2.6) | 1.6 (0.9–1.9) | 5.9 (3.6–11.1) | 6.0 (4.4–8.4) | 3 (2–4) | 2 (2–3) |
| Level 3 (46/2) | 2.2 (1.3–3.8) | 3.1 (2.8–3.4) | 1.8 (1.1–2.9) | 3.8 (1.9–5.6) | 8.0 (4.9–13.7) | 16.7 (8.1–25.3) | 3 (2–4) | 5 (4–5) |
| Level 4 (10/0) | 6.0 (3.4–7.8) | – | 4.5 (2.8–6.0) | – | 18.4 (10.8–23.9) | – | 5 (3–5) | – |
| p-value (complexity levels) | <0.001 | 0.123 | <0.001 | 0.252 | <0.001 | 0.116 | 0.056 | 0.080 |
| p-value (PSC vs. w/o PSC | 0.567 | 0.521 | 0.224 | 0.158 | ||||
| p-value (centers) | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| Center and Complexity Level (ERCPs Without PSC/with PSC) | Fluoroscopy Time, min | KAP, Gy·cm2 | Ka,r, mGy | Number of Exposures | ||||
|---|---|---|---|---|---|---|---|---|
| w/o PSC | PSC | w/o PSC | PSC | w/o PSC | PSC | w/o PSC | PSC | |
| Center 1 (1212/288) | 0.7 (0.4–1.6) | 4.8 (2.7–7.6) | 0.9 (0.4–1.9) | 3.0 (2.0–5.5) | 3.7 (1.6–9.1) | 19.9 (12.5–39.0) | 2 (0–3) | 5 (5–6) |
| Level 1 (639/1) | 0.6 (0.3–1.2) | 4.2 (4.2–4.2) | 0.8 (0.4–1.7) | 3.3 (3.3–3.3) | 3.0 (1.3–6.9) | 20.5 (20.5–20.5) | 1 (0–3) | 5 (5–5) |
| Level 2 (322/281) | 1.1 (0.5–2.1) | 4.8 (2.9–7.6) | 1.1 (0.5–2.2) | 3.0 (2.0–5.6) | 4.8 (2.1–10.5) | 20.5 (13.0–39.4) | 2 (1–3) | 5 (5–6) |
| Level 3 (251/6) | 1.0 (0.4–2.0) | 1.3 (0.8–4.2) | 0.9 (0.4–2.2) | 1.1 (0.5–1.9) | 4.4 (1.8–10.7) | 6.0 (3.0–9.7) | 2 (0–3) | 4 (2–4) |
| p-value (complexity levels) | <0.001 | 0.085 | 0.003 | 0.006 | <0.001 | 0.003 | <0.001 | 0.049 |
| p-value (PSC vs. w/o PSC) | <0.001 | <0.001 | <0.001 | <0.001 | ||||
| Center 2 (687/9) | 5.5 (3.5–9.4) | 4.5 (3.9–6.9) | 64.4 (38.1–106.7) | 49.6 (32.5–83.0) | 207.1 (120.1–350.7) | 264.3 (118.7–461.4) | 40 (29–52) | 38 (36–59) |
| Level 1 (543/0) | 5.0 (3.1–8.3) | – | 60.1 (35.5–102.9) | – | 190.8 (111.2–315.8) | – | 38 (28–49) | – |
| Level 2 (72/8) | 9.0 (5.2–13.3) | 5.3 (3.5–8.6) | 79.0 (55.5–120.2) | 58.4 (29.8–103.1) | 277.3 (168.4–400.8) | 258.3 (115.9–510.1) | 42 (29–59) | 38 (36–62) |
| Level 3 (72/1) | 8.2 (5.7–13.2) | 4.0 (4.0–4.0) | 83.4 (49.4–134.5) | 48.7 (48.7–48.7) | 254.8 (157.6–449.0) | 264.3 (264.3–264.3) | 52 (39–71) | 43 (43–43) |
| p-value (complexity levels) | <0.001 | 0.889 | <0.001 | 0.889 | <0.001 | 1.000 | <0.001 | 1.000 |
| p-value (PSC vs. w/o PSC | 0.771 | 0.430 | 0.456 | 0.532 | ||||
| Center 3 (167/4) | 1.4 (0.8–2.3) | 2.9 (2.0–4.0) | 1.2 (0.7–2.0) | 1.3 (1.2–2.2) | 9.7 (5.7–16.0) | 11.0 (10.3–14.3) | 4 (3–6) | 5 (4–6) |
| Level 1 (156/1) | 1.3 (0.8–2.0) | 1.7 (1.7–1.7) | 1.2 (0.7–2.0) | 1.3 (1.3–1.3) | 9.7 (5.9–16.0) | 11.1 (11.1–11.1) | 4 (3–5) | 5 (5–5) |
| Level 2 (9/2) | 3.6 (1.5–5.1) | 3.4 (2.1–4.7) | 1.0 (0.8–3.1) | 3.0 (1.3–4.7) | 9.3 (5.5–29.0) | 16.3 (8.6–23.9) | 4 (4–6) | 7 (5–8) |
| Level 3 (2/1) | 1.4 (1.1–1.7) | 3.8 (3.8–3.8) | 1.2 (0.5–1.9) | 1.1 (1.1–1.1) | 8.8 (4.7–12.9) | 10.8 (10.8–10.8) | 5 (3–6) | 1 (1–1) |
| p-value (complexity levels) | 0.070 | 0.407 | 0.811 | 0.407 | 0.730 | 0.861 | 0.721 | 0.325 |
| p-value (PSC vs. w/o PSC | 0.036 | 0.408 | 0.447 | 0.622 | ||||
| Center 4 (254/20) | 1.6 (1.0–2.6) | 1.8 (1.5–2.2) | 1.5 (0.9–2.8) | 1.7 (0.9–2.0) | 7.0 (3.9–12.5) | 5.6 (3.9–7.4) | 3 (2–4) | 3 (2–4) |
| Level 1 (207/0) | 1.4 (1.0–2.3) | – | 1.4 (0.8–2.7) | – | 6.1 (3.6–11.4) | – | 3 (2–4) | – |
| Level 2 (8/16) | 1.7 (1.3–1.8) | 1.7 (1.2–2.0) | 1.0 (0.9–1.5) | 1.6 (0.9–1.8) | 4.8 (3.5–7.0) | 5.5 (3.3–6.7) | 3 (2–5) | 3 (3–4) |
| Level 3 (39/4) | 4.0 (1.8–5.5) | 2.4 (1.8–3.1) | 2.6 (1.7–3.9) | 2.0 (1.7–3.9) | 12.7 (8.4–18.0) | 7.7 (6.3–16.7) | 4 (2–5) | 4 (3–5) |
| p-value (complexity levels) | <0.001 | 0.178 | <0.001 | 0.122 | <0.001 | 0.122 | 0.009 | 0.682 |
| p-value (PSC vs. w/o PSC | 0.567 | 0.521 | 0.224 | 0.158 | ||||
| p-value (centers) | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaasalainen, T.; Saukko, E.; Lindström, O.; Udd, M.; Regnér, S.; Saarela, A.; Toth, E.; Wurm Johansson, G.; Manninen, A.-L.; Grönroos, J.; et al. Assessing Patient Radiation Exposure in Endoscopic Retrograde Cholangiopancreatography: A Multicenter Retrospective Analysis of Procedural Complexity and Clinical Factors. Diagnostics 2024, 14, 656. https://doi.org/10.3390/diagnostics14060656
Kaasalainen T, Saukko E, Lindström O, Udd M, Regnér S, Saarela A, Toth E, Wurm Johansson G, Manninen A-L, Grönroos J, et al. Assessing Patient Radiation Exposure in Endoscopic Retrograde Cholangiopancreatography: A Multicenter Retrospective Analysis of Procedural Complexity and Clinical Factors. Diagnostics. 2024; 14(6):656. https://doi.org/10.3390/diagnostics14060656
Chicago/Turabian StyleKaasalainen, Touko, Ekaterina Saukko, Outi Lindström, Marianne Udd, Sara Regnér, Arto Saarela, Ervin Toth, Gabriele Wurm Johansson, Anna-Leena Manninen, Juha Grönroos, and et al. 2024. "Assessing Patient Radiation Exposure in Endoscopic Retrograde Cholangiopancreatography: A Multicenter Retrospective Analysis of Procedural Complexity and Clinical Factors" Diagnostics 14, no. 6: 656. https://doi.org/10.3390/diagnostics14060656
APA StyleKaasalainen, T., Saukko, E., Lindström, O., Udd, M., Regnér, S., Saarela, A., Toth, E., Wurm Johansson, G., Manninen, A.-L., Grönroos, J., & Kylänpää, L. (2024). Assessing Patient Radiation Exposure in Endoscopic Retrograde Cholangiopancreatography: A Multicenter Retrospective Analysis of Procedural Complexity and Clinical Factors. Diagnostics, 14(6), 656. https://doi.org/10.3390/diagnostics14060656