
Comparative Review of the Current and Future Strategies to Evaluate Bone Marrow Infiltration at Diffuse Large B-Cell Lymphoma Diagnosis
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population
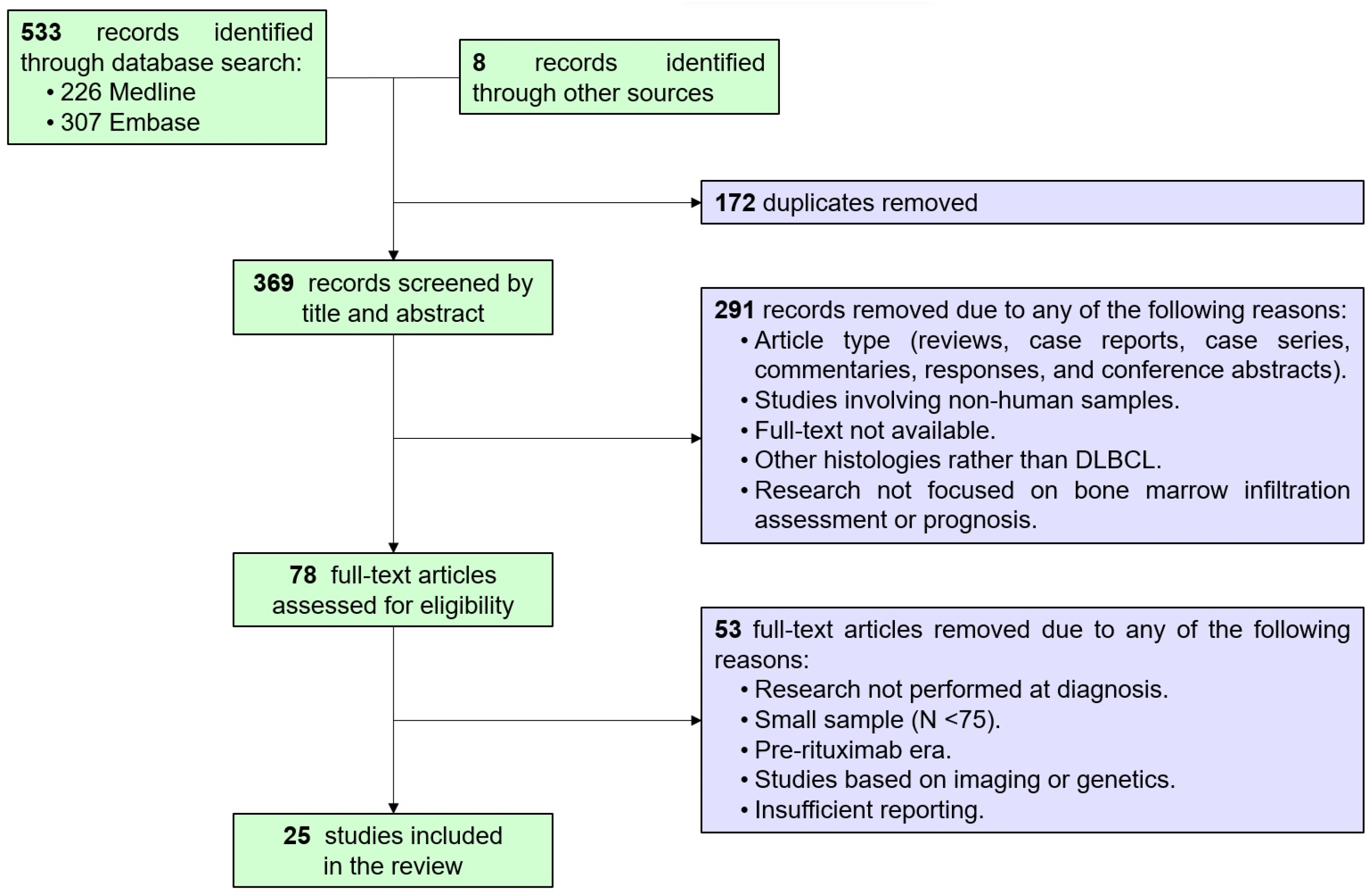
2.2. Bibliographic Search Strategy and Selection
2.3. Statistical Analysis
3. Results
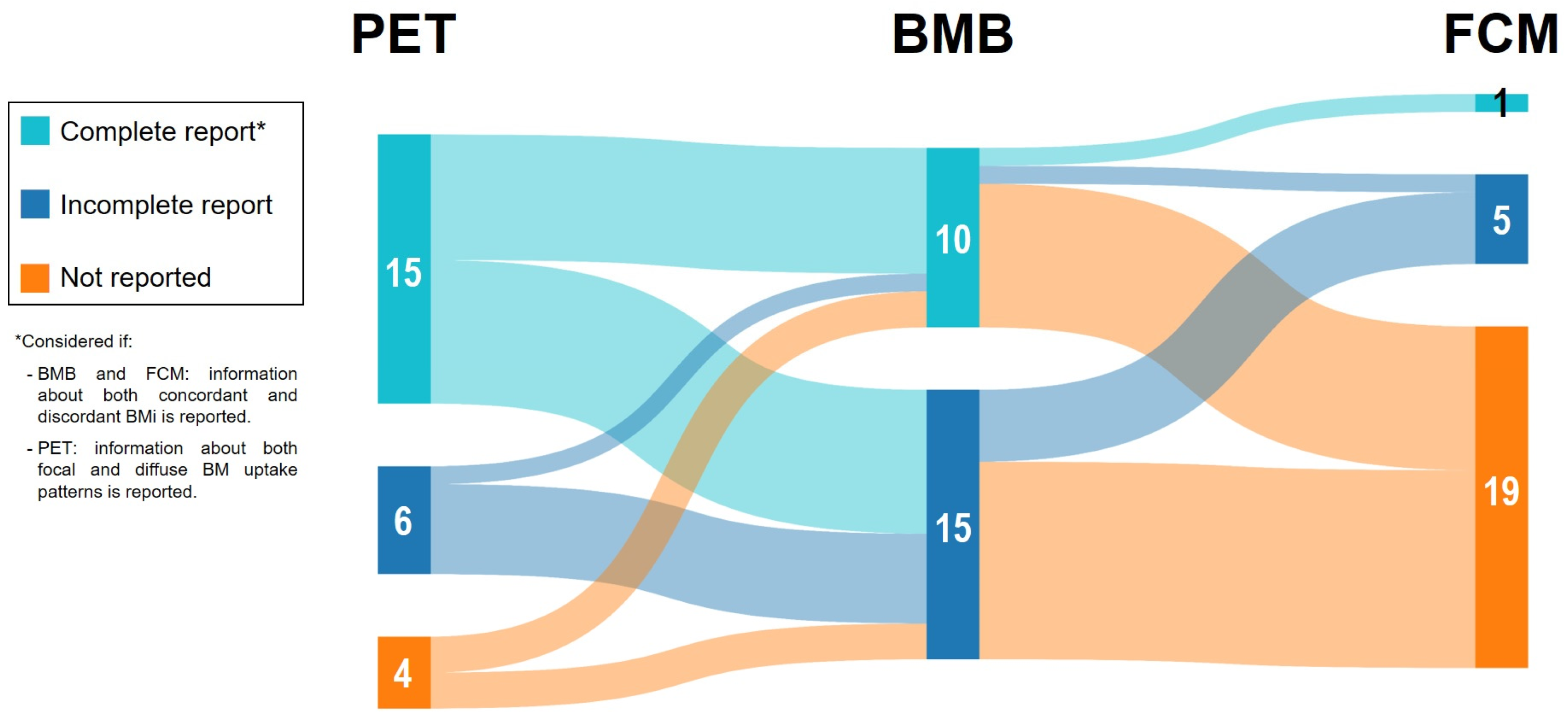
3.1. Description of the Included Studies, Characteristics of the DLBCL Populations, and BM Evaluation
3.2. Concordance Analysis among BMB, FCM, and PET When Assessing BMi at DLBCL Diagnosis
3.2.1. Concordance between BMB and FCM in the Setting of DLBCL BMi Assessment
3.2.2. Concordance between BMB and PET in the Setting of DLBCL BMi Assessment
3.2.3. Concordance between FCM and PET in the Setting of DLBCL BMi Assessment
3.3. Diagnostic Accuracy of BMB and PET for Detecting BMi at DLBCL Diagnosis
3.4. Prognostic Impact of BMi at DLBCL Diagnosis According to BMB, FCM, and PET in Comparative Studies
3.4.1. Outcomes According to BMi by BMB and FCM in Newly Diagnosed DLBCL
3.4.2. Outcomes According to BMi by BMB and PET in Newly Diagnosed DLBCL
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Bastos-Oreiro, M.; Muntañola, A.; Panizo, C.; Gonzalez-Barca, E.; de Villambrosia, S.G.; Córdoba, R.; López, J.L.B.; González-Sierra, P.; Terol, M.J.; Gutierrez, A.; et al. RELINF: Prospective Epidemiological Registry of Lymphoid Neoplasms in Spain. A Project from the GELTAMO Group. Ann. Hematol. 2020, 99, 799–808. [Google Scholar] [CrossRef]
- Sehn, L.H.; Salles, G. Diffuse Large B-Cell Lymphoma. N. Engl. J. Med. 2021, 384, 842–858. [Google Scholar] [CrossRef]
- Lamy, T.; Damaj, G.; Soubeyran, P.; Gyan, E.; Cartron, G.; Bouabdallah, K.; Gressin, R.; Cornillon, J.; Banos, A.; Le Du, K.; et al. R-CHOP 14 with or without Radiotherapy in Nonbulky Limited-Stage Diffuse Large B-Cell Lymphoma. Blood 2018, 131, 174–181. [Google Scholar] [CrossRef]
- Poeschel, V.; Held, G.; Ziepert, M.; Witzens-Harig, M.; Holte, H.; Thurner, L.; Borchmann, P.; Viardot, A.; Soekler, M.; Keller, U.; et al. Four versus Six Cycles of CHOP Chemotherapy in Combination with Six Applications of Rituximab in Patients with Aggressive B-Cell Lymphoma with Favourable Prognosis (FLYER): A Randomised, Phase 3, Non-Inferiority Trial. Lancet 2019, 394, 2271–2281. [Google Scholar] [CrossRef] [PubMed]
- Tilly, H.; Morschhauser, F.; Sehn, L.H.; Friedberg, J.W.; Trněný, M.; Sharman, J.P.; Herbaux, C.; Burke, J.M.; Matasar, M.; Rai, S.; et al. Polatuzumab Vedotin in Previously Untreated Diffuse Large B-Cell Lymphoma. N. Engl. J. Med. 2022, 386, 351–363. [Google Scholar] [CrossRef]
- Bobillo, S.; Khwaja, J.; Ferreri, A.J.M.; Cwynarski, K. Prevention and Management of Secondary Central Nervous System Lymphoma. Haematologica 2023, 108, 673–689. [Google Scholar] [CrossRef]
- Tilly, H.; Gomes da Silva, M.; Vitolo, U.; Jack, A.; Meignan, M.; Lopez-Guillermo, A.; Walewski, J.; André, M.; Johnson, P.W.; Pfreundschuh, M.; et al. Diffuse Large B-Cell Lymphoma (DLBCL): ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2015, 26 (Suppl. 5), v116–v125. [Google Scholar] [CrossRef] [PubMed]
- Bain, B.J. Morbidity Associated with Bone Marrow Aspiration and Trephine Biopsy—A Review of UK Data for 2004. Haematologica 2006, 91, 1293–1294. [Google Scholar]
- Brunetti, G.A.; Tendas, A.; Meloni, E.; Mancini, D.; Maggiore, P.; Scaramucci, L.; Giovannini, M.; Niscola, P.; Cartoni, C.; Alimena, G. Pain and Anxiety Associated with Bone Marrow Aspiration and Biopsy: A Prospective Study on 152 Italian Patients with Hematological Malignancies. Ann. Hematol. 2011, 90, 1233–1235. [Google Scholar] [CrossRef] [PubMed]
- Berthet, L.; Cochet, A.; Kanoun, S.; Berriolo-Riedinger, A.; Humbert, O.; Toubeau, M.; Dygai-Cochet, I.; Legouge, C.; Casasnovas, O.; Brunotte, F. In Newly Diagnosed Diffuse Large B-Cell Lymphoma, Determination of Bone Marrow Involvement with 18F-FDG PET/CT Provides Better Diagnostic Performance and Prognostic Stratification Than Does Biopsy. J. Nucl. Med. 2013, 54, 1244–1250. [Google Scholar] [CrossRef] [PubMed]
- El-Galaly, T.C.; Gormsen, L.C.; Hutchings, M. PET/CT for Staging; Past, Present, and Future. Semin. Nucl. Med. 2018, 48, 4–16. [Google Scholar] [CrossRef] [PubMed]
- Adams, H.J.A.; Kwee, T.C. Do Not Abandon the Bone Marrow Biopsy yet in Diffuse Large B-Cell Lymphoma. J. Clin. Oncol. 2015, 33, 1217. [Google Scholar] [CrossRef]
- Adams, H.J.A.; Kwee, T.C. Increased Bone Marrow FDG Uptake at PET/CT Is Not a Sufficient Proof of Bone Marrow Involvement in Diffuse Large B-Cell Lymphoma. Am. J. Hematol. 2015, 90, E182–E183. [Google Scholar] [CrossRef] [PubMed]
- Avigdor, A. Staging DLBCL: Bone Marrow Biopsy or PET-CT? Blood 2013, 122, 4–5. [Google Scholar] [CrossRef]
- Adams, H.J.A.; Kwee, T.C.; de Keizer, B.; Fijnheer, R.; de Klerk, J.M.H.; Nievelstein, R.A.J. FDG PET/CT for the Detection of Bone Marrow Involvement in Diffuse Large B-Cell Lymphoma: Systematic Review and Meta-Analysis. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 565–574. [Google Scholar] [CrossRef]
- Chen, Y.; Zhou, M.; Liu, J.; Huang, G. Prognostic Value of Bone Marrow FDG Uptake Pattern of PET/CT in Newly Diagnosed Diffuse Large B-Cell Lymphoma. J. Cancer 2018, 9, 1231–1238. [Google Scholar] [CrossRef]
- Elstrom, R.L.; Tsai, D.E.; Vergilio, J.-A.; Downs, L.H.; Alavi, A.; Schuster, S.J. Enhanced Marrow [18F]Fluorodeoxyglucose Uptake Related to Myeloid Hyperplasia in Hodgkin’s Lymphoma Can Simulate Lymphoma Involvement in Marrow. Clin. Lymphoma 2004, 5, 62–64. [Google Scholar] [CrossRef] [PubMed]
- Akin, O.; Brennan, S.B.; Dershaw, D.D.; Ginsberg, M.S.; Gollub, M.J.; Schöder, H.; Panicek, D.M.; Hricak, H. Advances in Oncologic Imaging: Update on 5 Common Cancers. CA Cancer J. Clin. 2012, 62, 364–393. [Google Scholar] [CrossRef]
- Jerusalem, G.; Beguin, Y.; Najjar, F.; Hustinx, R.; Fassotte, M.F.; Rigo, P.; Fillet, G. Positron Emission Tomography (PET) with 18F-Fluorodeoxyglucose (18F-FDG) for the Staging of Low-Grade Non-Hodgkin’s Lymphoma (NHL). Ann. Oncol. 2001, 12, 825–830. [Google Scholar] [CrossRef] [PubMed]
- Cerci, J.J.; Györke, T.; Fanti, S.; Paez, D.; Meneghetti, J.C.; Redondo, F.; Celli, M.; Auewarakul, C.; Rangarajan, V.; Gujral, S.; et al. Combined PET and Biopsy Evidence of Marrow Involvement Improves Prognostic Prediction in Diffuse Large B-Cell Lymphoma. J. Nucl. Med. 2014, 55, 1591–1597. [Google Scholar] [CrossRef]
- Cheson, B.D.; Pfistner, B.; Juweid, M.E.; Gascoyne, R.D.; Specht, L.; Horning, S.J.; Coiffier, B.; Fisher, R.I.; Hagenbeek, A.; Zucca, E.; et al. Revised Response Criteria for Malignant Lymphoma. J. Clin. Oncol. 2007, 25, 579–586. [Google Scholar] [CrossRef]
- Cabezas-Quintario, M.A.; Gomez, P.; Yuste-Del Pozo, V.; Valencia-Mesa, A.L.; Sosa, G.; Ricard, P.; Hijas-Gómez, A.I.; Pinedo, F.; Arguelles, M. Bone Marrow Trephine Biopsy Involvement by Lymphoma: Pattern of Involvement and Concordance with Flow Cytometry, in 10 Years from a Single Institution. Clin. Transl. Oncol. 2016, 18, 537–540. [Google Scholar] [CrossRef]
- Talaulikar, D.; Dahlstrom, J.E. Staging Bone Marrow in Diffuse Large B-Cell Lymphoma: The Role of Ancillary Investigations. Pathology 2009, 41, 214–222. [Google Scholar] [CrossRef]
- Pittaluga, S.; Tierens, A.; Dodoo, Y.L.; Delabie, J.; De Wolf-Peeters, C. How Reliable Is Histologic Examination of Bone Marrow Trephine Biopsy Specimens for the Staging of Non-Hodgkin Lymphoma? A Study of Hairy Cell Leukemia and Mantle Cell Lymphoma Involvement of the Bone Marrow Trephine Specimen by Histologic, Immunohistochemical, and Polymerase Chain Reaction Techniques. Am. J. Clin. Pathol. 1999, 111, 179–184. [Google Scholar] [CrossRef]
- Tierens, A.M.; Holte, H.; Warsame, A.; Ikonomou, I.M.; Wang, J.; Chan, W.C.; Delabie, J. Low Levels of Monoclonal Small B Cells in the Bone Marrow of Patients with Diffuse Large B-Cell Lymphoma of Activated B-Cell Type but Not of Germinal Center B-Cell Type. Haematologica 2010, 95, 1334–1341. [Google Scholar] [CrossRef] [PubMed]
- Stacchini, A.; Demurtas, A.; Godio, L.; Martini, G.; Antinoro, V.; Palestro, G. Flow Cytometry in the Bone Marrow Staging of Mature B-Cell Neoplasms. Cytom. B Clin. Cytom. 2003, 54, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Shim, H.; Oh, J.-I.; Park, S.H.; Jang, S.; Park, C.-J.; Huh, J.; Suh, C.; Chi, H.-S. Prognostic Impact of Concordant and Discordant Cytomorphology of Bone Marrow Involvement in Patients with Diffuse, Large, B-Cell Lymphoma Treated with R-CHOP. J. Clin. Pathol. 2013, 66, 420–425. [Google Scholar] [CrossRef] [PubMed]
- Sehn, L.H.; Scott, D.W.; Chhanabhai, M.; Berry, B.; Ruskova, A.; Berkahn, L.; Connors, J.M.; Gascoyne, R.D. Impact of Concordant and Discordant Bone Marrow Involvement on Outcome in Diffuse Large B-Cell Lymphoma Treated with R-CHOP. JCO 2011, 29, 1452–1457. [Google Scholar] [CrossRef] [PubMed]
- Chung, R.; Lai, R.; Wei, P.; Lee, J.; Hanson, J.; Belch, A.R.; Turner, A.R.; Reiman, T. Concordant but Not Discordant Bone Marrow Involvement in Diffuse Large B-Cell Lymphoma Predicts a Poor Clinical Outcome Independent of the International Prognostic Index. Blood 2007, 110, 1278–1282. [Google Scholar] [CrossRef] [PubMed]
- Yao, Z.; Deng, L.; Xu-Monette, Z.Y.; Manyam, G.C.; Jain, P.; Tzankov, A.; Visco, C.; Bhagat, G.; Wang, J.; Dybkaer, K.; et al. Concordant Bone Marrow Involvement of Diffuse Large B-Cell Lymphoma Represents a Distinct Clinical and Biological Entity in the Era of Immunotherapy. Leukemia 2018, 32, 353–363. [Google Scholar] [CrossRef]
- Chigrinova, E.; Mian, M.; Scandurra, M.; Greiner, T.C.; Chan, W.C.; Vose, J.M.; Inghirami, G.; Chiappella, A.; Baldini, L.; Ponzoni, M.; et al. Diffuse Large B-cell Lymphoma with Concordant Bone Marrow Involvement Has Peculiar Genomic Profile and Poor Clinical Outcome. Hematol. Oncol. 2011, 29, 38–41. [Google Scholar] [CrossRef]
- Park, M.-J.; Park, S.-H.; Park, P.-W.; Seo, Y.-H.; Kim, K.-H.; Seo, J.-Y.; Jeong, J.-H.; Kim, M.J.; Ahn, J.-Y.; Hong, J. Prognostic Impact of Concordant and Discordant Bone Marrow Involvement and Cell-of-Origin in Korean Patients with Diffuse Large B-Cell Lymphoma Treated with R-CHOP. J. Clin. Pathol. 2015, 68, 733–738. [Google Scholar] [CrossRef] [PubMed]
- Alzahrani, M.; El-Galaly, T.C.; Hutchings, M.; Hansen, J.W.; Loft, A.; Johnsen, H.E.; Iyer, V.; Wilson, D.; Sehn, L.H.; Savage, K.J.; et al. The Value of Routine Bone Marrow Biopsy in Patients with Diffuse Large B-Cell Lymphoma Staged with PET/CT: A Danish-Canadian Study. Ann. Oncol. 2016, 27, 1095–1099. [Google Scholar] [CrossRef]
- Soydal, C.; Koksoy, E.B.; Yasar, A.; Turgal, E.; Erdogan, B.D.; Akbulut, H.; Kucuk, N.O. Prognostic Importance of Bone Marrow Uptake on Baseline 18F-FDG Positron Emission Tomography in Diffuse Large B Cell Lymphoma. Cancer Biother. Radiopharm. 2016, 31, 361–365. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.B.; Barrington, S.F.; Mikhaeel, N.G.; Hunt, A.A.; Cameron, L.; Morris, T.; Carr, R. PET-CT Staging of DLBCL Accurately Identifies and Provides New Insight into the Clinical Significance of Bone Marrow Involvement. Blood 2013, 122, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.; Lee, Y.; Park, Y.; Kim, S.G.; Hwang, K.H.; Park, S.H.; Jeong, J.; Kim, K.-H.; Ahn, J.Y.; Park, S.; et al. Role of FDG-PET/CT in Detecting Lymphomatous Bone Marrow Involvement in Patients with Newly Diagnosed Diffuse Large B-Cell Lymphoma. Ann. Hematol. 2012, 91, 687–695. [Google Scholar] [CrossRef] [PubMed]
- Bo, G.; Ran, Q.; Yang, G.Z.; Fen, L.Y.; Lei, G.; Rong, H.W. Diagnostic Efficacy of 18F-FDG PET/CT in Detecting Bone Marrow Infiltration in Patients with Newly Diagnosed Diffuse Large B-Cell Lymphoma. Biomed. Environ. Sci. 2023, 36, 510–516. [Google Scholar] [CrossRef]
- Han, E.J.; O, J.H.; Yoon, H.; Ha, S.; Yoo, I.R.; Min, J.W.; Choi, J.-I.; Choi, B.-O.; Park, G.; Lee, H.H.; et al. Comparison of FDG PET/CT and Bone Marrow Biopsy Results in Patients with Diffuse Large B Cell Lymphoma with Subgroup Analysis of PET Radiomics. Diagnostics 2022, 12, 222. [Google Scholar] [CrossRef]
- Kim, M.; Ahn, S.-Y.; Ahn, J.-S.; Song, G.-Y.; Jung, S.-H.; Lee, J.-J.; Kim, H.-J.; Lee, J.H.; Shin, M.-G.; Song, S.Y.; et al. Diagnostic Accuracy and Prognostic Relevance of Immunoglobulin Heavy Chain Rearrangement and 18F-FDG-PET/CT Compared with Unilateral Bone Marrow Trephination for Detecting Bone Marrow Involvement in Patients with Diffuse Large B-Cell Lymphoma. J. Korean Med. Sci. 2022, 37, e2. [Google Scholar] [CrossRef]
- Okamoto, H.; Uoshima, N.; Muramatsu, A.; Isa, R.; Fujino, T.; Matsumura-Kimoto, Y.; Tsukamoto, T.; Mizutani, S.; Shimura, Y.; Kobayashi, T.; et al. Combination of Bone Marrow Biopsy and Flow Cytometric Analysis: The Prognostically Relevant Central Approach for Detecting Bone Marrow Invasion in Diffuse Large B-Cell Lymphoma. Diagnostics 2021, 11, 1724. [Google Scholar] [CrossRef]
- Lim, C.H.; Hyun, S.H.; Cho, Y.S.; Choi, J.Y.; Lee, K.-H. Prognostic Significance of Bone Marrow 2-[18F]-Fluoro-2-Deoxy-d-Glucose Uptake in Diffuse Large B-Cell Lymphoma: Relation to Iliac Crest Biopsy Results. Clin. Radiol. 2021, 76, e19–e550. [Google Scholar] [CrossRef]
- Saiki, Y.; Tomita, N.; Uchida, A.; Uemura, Y.; Suzuki, Y.; Hirakawa, T.; Kato, M.; Hoshikawa, M.; Kawano, T.; Nakamura, N.; et al. Biopsy Remains Indispensable for Evaluating Bone Marrow Involvement in DLBCL Patients despite the Use of Positron Emission Tomography. Int. J. Hematol. 2021, 113, 675–681. [Google Scholar] [CrossRef]
- Martín-Moro, F.; Piris-Villaespesa, M.; Marquet-Palomanes, J.; García-Cosío, M.; Villarrubia, J.; Lario, A.; García, I.; Michael, B.; Roldán, E.; García-Vela, J.A.; et al. Bone Marrow Infiltration by Flow Cytometry at Diffuse Large B-cell Lymphoma NOS Diagnosis Implies Worse Prognosis without Considering Bone Marrow Histology. Cytom. Part B Clin. 2020, 98, 525–528. [Google Scholar] [CrossRef]
- Al-Sabbagh, A.; Ibrahim, F.; Szabados, L.; Soliman, D.S.; Taha, R.Y.; Fernyhough, L.J. The Role of Integrated Positron Emission Tomography/Computed Tomography (PET/CT) and Bone Marrow Examination in Staging Large B-Cell Lymphoma. Clin. Med. Insights Oncol. 2020, 14, 117955492095309. [Google Scholar] [CrossRef]
- Min, G.-J.; Jeon, Y.-W.; Park, S.-S.; Shin, S.-H.; Yahng, S.-A.; Yoon, J.-H.; Lee, S.-E.; Cho, B.-S.; Eom, K.-S.; Kim, Y.-J.; et al. Poor Prognosis in Patients with Diffuse Large B Cell Lymphomas with Bone Marrow Involvement Possessing Chromosomal Abnormalities, despite Aggressive Treatment. Ann. Hematol. 2020, 99, 557–570. [Google Scholar] [CrossRef]
- Kandeel, A.A.; Hussein, M.; Zidan, L.; Younis, J.; Edesa, W.; Alsayed, Y. Diagnostic Performance of 18F-2-Fluoro-2-Deoxy-D-Glucose PET/Computerized Tomography in Identifying Bone Marrow Infiltration in New Patients with Diffuse Large B-Cell Lymphoma and Hodgkin Lymphoma. Nucl. Med. Commun. 2020, 41, 269–279. [Google Scholar] [CrossRef]
- Alonso-Álvarez, S.; Alcoceba, M.; García-Álvarez, M.; Blanco, O.; Rodríguez, M.; Baile, M.; Caballero, J.C.; Dávila, J.; Vidriales, M.B.; Esteban, C.; et al. Biological Features and Prognostic Impact of Bone Marrow Infiltration in Patients with Diffuse Large B-Cell Lymphoma. Cancers 2020, 12, 474. [Google Scholar] [CrossRef]
- Wang, J.; Kim, D.; Kang, W.J.; Cho, H. Prognostic Value of Bone Marrow F-18 FDG Uptake in Patients with Advanced-Stage Diffuse Large B-Cell Lymphoma. Nucl. Med. Mol. Imaging 2020, 54, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Greenbaum, U.; Levi, I.; Madmoni, O.; Lior, Y.; Al-Athamen, K.; Perry, Z.H.; Hatzkelzon, L.; Shubinsky, G. The Prognostic Significance of Bone Marrow Involvement in Diffuse Large B Cell Lymphoma According to the Flow Cytometry. Leuk. Lymphoma 2019, 60, 2477–2482. [Google Scholar] [CrossRef] [PubMed]
- Chen-Liang, T.; Martín-Santos, T.; Jerez, A.; Rodríguez-García, G.; Senent, L.; Martínez-Millán, C.; Muiña, B.; Orero, M.; Teruel, A.; Martín, A.; et al. Bone Marrow Biopsy Superiority over PET/CT in Predicting Progression-free Survival in a Homogeneously-treated Cohort of Diffuse Large B-cell Lymphoma. Cancer Med. 2017, 6, 2507–2514. [Google Scholar] [CrossRef] [PubMed]
- Vishnu, P.; Wingerson, A.; Lee, M.; Mandelson, M.T.; Aboulafia, D.M. Utility of Bone Marrow Biopsy and Aspirate for Staging of Diffuse Large B Cell Lymphoma in the Era of Positron Emission Tomography with 2-Deoxy-2-[Fluorine-18]Fluoro-Deoxyglucose Integrated with Computed Tomography. Clin. Lymphoma Myeloma Leuk. 2017, 17, 631–636. [Google Scholar] [CrossRef]
- Liang, J.-H.; Sun, J.; Wang, L.; Fan, L.; Chen, Y.-Y.; Qu, X.-Y.; Li, T.-N.; Li, J.-Y.; Xu, W. Prognostic Significance of Bone Marrow Infiltration Detected by PET-CT in Newly Diagnosed Diffuse Large B Cell Lymphoma. Oncotarget 2016, 7, 19072–19080. [Google Scholar] [CrossRef]
- Adams, H.J.A.; Kwee, T.C.; Fijnheer, R.; Dubois, S.V.; Nievelstein, R.A.J.; De Klerk, J.M.H. Bone Marrow 18F-fluoro-2-deoxy-d-glucose Positron Emission Tomography/Computed Tomography Cannot Replace Bone Marrow Biopsy in Diffuse Large B-cell Lymphoma. Am. J. Hematol. 2014, 89, 726–731. [Google Scholar] [CrossRef]
- Arima, H.; Maruoka, H.; Nasu, K.; Tabata, S.; Kurata, M.; Matsushita, A.; Imai, Y.; Takahashi, T.; Ishikawa, T. Impact of Occult Bone Marrow Involvement on the Outcome of Rituximab plus Cyclophosphamide, Doxorubicin, Vincristine and Prednisone Therapy for Diffuse Large B-Cell Lymphoma. Leuk. Lymphoma 2013, 54, 2645–2653. [Google Scholar] [CrossRef] [PubMed]
- Cortés-Romera, M.; Sabaté-Llobera, A.; Mercadal-Vilchez, S.; Climent-Esteller, F.; Serrano-Maestro, A.; Gámez-Cenzano, C.; González-Barca, E. Bone Marrow Evaluation in Initial Staging of Lymphoma: 18F-FDG PET/CT Versus Bone Marrow Biopsy. Clin. Nucl. Med. 2014, 39, e46–e52. [Google Scholar] [CrossRef]
- Wolach, O.; Fraser, A.; Luchiansky, M.; Shapiro, C.; Radnay, J.; Shpilberg, O.; Lishner, M.; Lahav, M. Can Flow Cytometry of Bone Marrow Aspirate Predict Outcome of Patients with Diffuse Large B Cell Lymphoma? A Retrospective Single Centre Study. Hematol. Oncol. 2015, 33, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Cho, M.-C.; Chung, Y.; Jang, S.; Park, C.-J.; Chi, H.-S.; Huh, J.; Suh, C.; Shim, H. Prognostic Impact of Germinal Center B-Cell-like and Non-Germinal Center B-Cell-like Subtypes of Bone Marrow Involvement in Patients with Diffuse Large B-Cell Lymphoma Treated with R-CHOP. Medicine 2018, 97, e13046. [Google Scholar] [CrossRef] [PubMed]
- Kremer, M.; Spitzer, M.; Mandl-Weber, S.; Stecker, K.; Schmidt, B.; Höfler, H.; Quintanilla-Martínez, L.; Fend, F. Discordant Bone Marrow Involvement in Diffuse Large B-Cell Lymphoma: Comparative Molecular Analysis Reveals a Heterogeneous Group of Disorders. Lab. Investig. 2003, 83, 107–114. [Google Scholar] [CrossRef]
- Wang, Y.; Link, B.K.; Witzig, T.E.; Maurer, M.J.; Allmer, C.; King, R.L.; Feldman, A.L.; Habermann, T.M.; Ansell, S.M.; Slager, S.L.; et al. Impact of Concurrent Indolent Lymphoma on the Clinical Outcome of Newly Diagnosed Diffuse Large B-Cell Lymphoma. Blood 2019, 134, 1289–1297. [Google Scholar] [CrossRef]
- El-Azony, A.; Basha, M.A.A.; Almalki, Y.E.; Abdelmaksoud, B.; Hefzi, N.; Alnagar, A.A.; Mahdey, S.; Ali, I.M.; Nasr, I.; Abdalla, A.A.E.-H.M.; et al. The Prognostic Value of Bone Marrow Retention Index and Bone Marrow-to-Liver Ratio of Baseline 18F-FDG PET/CT in Diffuse Large B-Cell Lymphoma. Eur. Radiol. 2023. [Google Scholar] [CrossRef]
- Ke, Q.; Liao, C.-C.; Tan, X.-H.; Guo, B.-P.; Cen, H.; Li, L.-Q. Diagnostic Accuracy of Pelvic Magnetic Resonance Imaging for the Assessment of Bone Marrow Involvement in Diffuse Large B-Cell Lymphoma. PLoS ONE 2021, 16, e0252226. [Google Scholar] [CrossRef] [PubMed]
- Adams, H.J.A.; Kwee, T.C.; Lokhorst, H.M.; Westerweel, P.E.; Fijnheer, R.; Kersten, M.J.; Verkooijen, H.M.; Stoker, J.; Nievelstein, R.A.J. Potential Prognostic Implications of Whole-Body Bone Marrow MRI in Diffuse Large B-Cell Lymphoma Patients with a Negative Blind Bone Marrow Biopsy. J. Magn. Reason. Imaging 2014, 39, 1394–1400. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.A.; Yang, W.I.; Song, J.; Min, Y.H.; Yoon, S.O. The Prognostic Significance of Monoclonal Immunoglobulin Gene Rearrangement in Conjunction with Histologic B-cell Aggregates in the Bone Marrow of Patients with Diffuse Large B-cell Lymphoma. Cancer Med. 2016, 5, 1066–1073. [Google Scholar] [CrossRef]
- Kim, S.Y.; Kim, H.J.; Kang, H.J.; Kim, J.S.; Eom, H.S.; Kim, T.M.; Yoon, S.-S.; Suh, C.; Lee, D.S.; Korean Society of Hematology Lymphoma Working Party. Clinical Significance of Cytogenetic Aberrations in Bone Marrow of Patients with Diffuse Large B-Cell Lymphoma: Prognostic Significance and Relevance to Histologic Involvement. J. Hematol. Oncol. 2013, 6, 76. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Ref. * | Region | Study Type | Period | N | DLBCL Population Characteristics | Bone Marrow Assessment | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Male/Female Ratio | Median Age (Range) | COO † | Ann Arbor | IPI | Frontline | Follow-Up (Months) | Histology | Flow Cytometry | PET-FDG | |||||||||||
| Not Specified or Global | Concordant | Discordant | Not Specified or Global | Concordant | Discordant | Not Specified or Global | Focal | Diffuse | ||||||||||||
| Bo et al. [37] | China | Retrospective | 2019–2022 | 102 | 1.2 | 29.4% ≥ 60 yo | GCB: 35% Non-GCB: 65% | I–II: 14% III: 0% IV: 86% | 3–5: 28% | - | - | 21% (28% after second punction) | - | - | 18% (24% after second punction) | - | - | 26% | 23% | 3% |
| Han et al. [38] | South Korea | Retrospective | 2014–2020 | 328 | 1.3 | 59 (44–74) | - | I–II: 52% III–IV: 48% | 3–5: 41% | - | - | 14% | - | - | - | - | - | 18% | 11% | 7% |
| Kim et al. [39] | South Korea | Prospective | 2017–2018 | 94 | 1.8 | 66 (24–85) | - | I–II: 47% III–IV: 53% | 3–5: 61% | R-CHOP | 35 (23–47) | 10% | 6% | 3% | - | - | - | 17% | 12% | 5% |
| Okamoto et al. [40] | Japan | Retrospective | 2012–2018 | 221 | 1.6 | 72 (26–97) | - | I–II: 42% III–IV: 58% | Poor R-IPI 53% | R-CHOP or R-CHOP-like 83% | 31 (N = 184 subcohort R-CHOP or R-CHOP-like) | 8% | - | - | 12% | - | - | - | - | - |
| Lim et al. [41] | South Korea | Retrospective | 2009–2014 | 512 | 1.2 | 57 (47–67) | - | I–II: 56% III–IV: 44% | 3–5: 32% | R-CHOP | 52 (1–127) | 12% (bilateral) | 11% | 1% | - | - | - | 13% | 8% | 2% |
| 2% heterogeneous | ||||||||||||||||||||
| Saiki et al. [42] | Japan | Retrospective | 2008–2017 | 84 | 1.2 | 70 (19–86) | - | I–II: 47% III–IV: 53% | - | Mostly R-CHOP | - | 26% | 19% | 7% | - | - | - | 19% | 8% | 11% |
| Martin-Moro et al. [43] | Spain | Retrospective | 2013–2017 | 82 (38 PET data) | 1.2 | 63 (33–85) | GCB: 49% Non-GCB: 51% | I–II: 50% III–IV: 50% | aaIPI 2–3: 41% | R-CHOP or R-CHOP-like | 33 (NR) | 13% | - | - | 24% | - | - | 16% | - | - |
| Al-Sabbagh et al. [44] | Qatar | Retrospective | 2013–2017 | 89 | 2.6 | 48 (18–77) | - | I–II: 39% III–IV: 61% | - | - | - | 13% | - | - | - | - | - | 26% (focal and heterogeneous) | - | - |
| Min et al. [45] | South Korea | Retrospective | 2009–2016 | 600 | 1.4 | 59 (17–88) | GCB: 36% Non-GCB: 64% | I–II: 44% III–IV: 56% | 3–5: 50% | R-CHOP | 50 (0.2–123) | 15% (bilateral) | - | - | - | - | - | 16% | 10% | 3% |
| Both 3% | ||||||||||||||||||||
| Kandeel et al. [46] | Egypt | Retrospective | 2015–2018 | 88 | 0.7 | 50 (21–70) | GCB: 43% Non-GCB: 57% | I–II: 14% III–IV: 86% | - | Mostly R-CHOP | 11 (2–20) | 25% | - | - | - | - | - | - | 30% | - |
| Alonso-Alvarez et al. [47] | Spain | Retrospective | 1999–2014 | 232 | 1 | 66% >60yo | GCB: 37% Non-GCB: 63% | I–II: 29% III–IV: 71% | Poor R-IPI: 41% | 81% R-CHOP or R-CHOP-like | 58 (1–152) | 25% | 16% | 9% | 25% | 10% | 15% | - | - | - |
| Wang et al. [48] | South Korea | Retrospective | 2011–2017 | 140 | 1.4 | 65 (22–86) | GCB: 9% Non-GCB: 91% | I–II: 0% III–IV: 100% | >3: 45% | R-CHOP | 49 (1–98) | 36% (bilateral) | - | - | - | - | - | - | 31% | - |
| Greenbaum et al. [49] | Israel | Retrospective | 2005–2014 | 81 | 1.5 | 65 (23–87) | - | I–II: 38% III–IV: 62% | Median 3 | 91% R-CHOP | - | 26% | - | - | 63% | - | - | - | - | - |
| Chen et al. [16] | China | Retrospective | 2007–2016 | 193 | 0.9 | 58 (14–87) | GCB: 32% Non-GCB: 68% | I–II: 44% III–IV: 56% | 3–5: 43% | R-CHOP | 30 (12–124) | 7% | - | - | - | - | - | 24% | 15% | 9% |
| Chen-Liang et al. [50] | Spain | Retrospective | 2007–2015 | 268 | 1 | 61 (18–85) | - | I–II: 25% III–IV: 75% | 3–5: 42% | 76% R-CHOP | 25 (1–91) | 13% | - | - | - | - | - | 22% | 17% | 6% |
| Vishnu et al. [51] | USA | Retrospective | 2004–2013 | 99 | 1.7 | 62 (24–88) | - | - | Poor R-IPI: 24% | - | 91 (28–140) | 14% | - | - | - | - | - | 24% | - | - |
| Alzahrani et al. [33] | Canada and Denmark | Retrospective | 2007–2013 | 530 | 1.2 | 65 (16–90) | - | I–II: 37% III–IV: 63% | 3–5: 43% | - | 24 (3–78) | 16% | 10% | 7% | - | - | - | - | 28% | - |
| Liang et al. [52] | China | Retrospective | 2005–2014 | 169 | 1.3 | 55 (18–85) | GCB: 40% Non-GCB: 60% | I–II: 36% III–IV: 64% | 4–5: 17% | R-CHOP (60%) or DA-EPOCH-R (40%) | 38 (12–113) | 12% (some bilateral) | - | - | - | - | - | 21% | 20% | 2% |
| Cerci et al. [20] | Brazil, Chile, Hungary, India, Italy, South Korea, Philippines, and Thailand | Prospective | 2008–2011 | 327 | 1.1 | 55 (IQR 44–63) | - | I–II: 36% III–IV: 64% | 3–5: 34% | R-CHOP recommended | 35 (NR) | 11% | - | - | - | - | - | 26% | 21% | 6% |
| Adams et al. [53] | The Netherlands | Retrospective | 2007–2013 | 78 | 1.2 | 69 (33–88) | - | I–II: 23% III–IV: 77% | NCCN-IPI >3: 71% | 91% R-CHOP | 28 (5–74) | 21% (3% undetermined) | 14% | 4% | - | - | - | 44% | 39% | 5% |
| Arima et al. [54] | Japan | Retrospective | 2006–2011 | 96 ‡ | 1.5 | 69 (22–89) | - | I–II: 39% III–IV: 61% | 3–5: 52% | R-CHOP | 36 (1–72) | 20% | 15% | 5% | 28% | - | - | - | - | - |
| Berthet et al. [10] | France | Retrospective | 2006–2011 | 133 | 1 | 57 (18–87) | - | I–II: 26% III–IV: 74% | 3–5: 40% | R-CHOP or R-CHOP-like | 24 (1–67) | 6% | 4% | 2% | - | - | - | 32% | 24% | 8% |
| Khan et al. [35] | United Kingdom | Retrospective | 2005–2012 | 130 | 1.5 | 59 (22–87) | - | I–II: 45% III–IV: 55% | 3–5: 40% | 95% R-CHOP | - | 11% | 11% | 0% | - | - | - | 25% | 21.5% | 1.5% |
| Both 2% | ||||||||||||||||||||
| Hong et al. [36] | South Korea | Retrospective | 2007–2011 | 89 | 0.8 | 59 (26–83) | GCB: 49% Non-GCB: 51% | I–II: 47% III–IV: 52% | Poor R-IPI: 35% | R-CHOP | 16 (NR) | 16% (bilateral) | 10% | 6% | - | - | - | 19% | 11% | 8% |
| Cortes Romera et al. [55] | Spain | - | 2004–2010 | 84 | 1 | 63 (19–78) | - | I–II: 50% III–IV: 50% | - | R-CHOP | NR (9–34) | - | 19% | - | - | - | - | 29% | 23% | 6% |
| Ref. | Concordant Results | Discordant Results | Cohen’s Kappa Index | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| BMB+/FCM+ | BMB+/PET+ | FCM+/PET+ | BMB−/FCM− | BMB−/PET− | FCM−/PET− | BMB+/FCM− | BMB+/PET− | BMB−/FCM+ | BMB−/PET+ | FCM+/PET− | FCM−/PET+ | BMB/FCM | BMB/PET | FCM/PET | |
| Bo et al. [37] | - | 16% (23% after second punction) | 14% (20% after second punction) | - | 71% | 72% | - | 5% | - | 10% (3% after second punction) | 4% | 12% (6% after second punction) | - | 0.59 (0.8 after second punction) | 0.54 (0.74 after second punction) |
| Han et al. [38] | - | 7% | - | - | 76% | - | - | 6% | - | 11% | - | - | - | 0.36 * | - |
| Kim et al. [39] | - | 5% | - | - | 79% | - | - | 4% | - | 12% | - | - | - | 0.32 * | - |
| Okamoto et al. [40] | 3% | - | - | 83% | - | - | 5% | - | 9% | - | - | - | 0.25 | - | - |
| Lim et al. [41] | - | 7% | - | - | 83% | - | - | 5% | - | 6% | - | - | - | 0.51 * | - |
| Saiki et al. [42] | - | 10% | - | - | 64% | - | - | 17% | - | 10% | - | - | - | 0.26 * | - |
| Martín-Moro et al. [43] | 13% | 5% | 8% | 76% | 79% | 71% | 0% | 5% | 15% | 11% | 13% | 8% | 0.65 * | 0.31 * | 0.30 * |
| Al-Sabbagh et al. [44] | - | 12% | - | - | 73% | - | - | 1% | - | 13% | - | - | - | 0.55 * | - |
| Min et al. [45] | - | 9% | - | - | 76% | - | - | 7% | - | 8% | - | - | - | 0.43 * | - |
| Kandeel et al. [46] | - | 14% | - | - | 59% | - | - | 11% | - | 16% | - | - | - | 0.31 * | - |
| Alonso-Alvarez et al. [47] | 18% | - | - | 69% | - | - | 6% | - | 7% | - | - | - | 0.65 * | - | - |
| Wang et al. [48] | - | 21% | - | - | 54% | - | - | 14% † | - | 10% | - | - | - | 0.46 * | - |
| Greenbaum et al. [49] | 26% | - | - | 37% | - | - | 0% | - | 37% | - | - | - | 0.4 * | - | - |
| Chen et al. [16] | - | 7% | - | - | 76% | - | - | 1% | - | 17% | - | - | - | 0.36 * | - |
| Chen-Liang et al. [50] | - | 9% | - | - | 74% | - | - | 4% | - | 13% | - | - | - | 0.41 * | - |
| Vishnu et al. [51] | - | 12% | - | - | 74% | - | - | 2% | - | 12% | - | - | - | 0.55 * | - |
| Alzahrani et al. [33] | - | 9% | - | - | 66% | - | - | 7% | - | 18% | - | - | - | 0.30 * | - |
| Liang et al. [52] | - | 11% | - | - | 78% | - | - | 1% | - | 10% | - | - | - | 0.59 * | - |
| Cerci et al. [20] | - | 8% | - | - | 71% | - | - | 3% | - | 19% | - | - | - | 0.31 * | - |
| Adams et al. [53] | - | 14% | - | - | 50% | - | - | 6% | - | 29% | - | - | - | 0.22 * | - |
| Arima et al. [54] | 18% | - | - | 70% | - | - | 2% | - | 10% | - | - | - | 0.66 * | - | - |
| Berthet et al. [10] | - | 5% (4% subcohort PET focal) | - | - | 67% (74% subcohort PET focal) | - | - | 1% (2% subcohort PET focal) | - | 27% (20% subcohort PET focal) | - | - | - | 0.19 * (0.23 * subcohort PET focal) | - |
| Khan et al. [35] | - | 9% | - | - | 73% | - | - | 2% | - | 16% | - | - | - | 0.42 * | - |
| Hong et al. [36] | - | 8% | - | - | 73% | - | - | 8% | - | 11% | - | - | - | 0.34 * | - |
| Cortes Romera et al. [55] | - | 18% | - | - | 70% | - | - | 1% | - | 11% | - | - | - | 0.68 * | - |
| Ref. | Definition of True Positive BMi | Sensitivity (CI 95%) | Specificity (CI 95%) | Positive/Negative Predictive Value | Youden’s Index/Diagnostic Accuracy | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| BMB | PET | PET Focal | BMB | PET | PET Focal | BMB | PET | PET Focal | BMB | PET | PET Focal | ||
| Bo et al. [37] | After first direct BM study (BMB and FCM) | - | 62% (43–78) | - | - | 93% (86–97) | - | - | - | - | - | 0.55% (YI) | - |
| After second direct BM study (BMB and FCM) | - | 92% (76–98) | - | - | - | - | - | - | - | 0.86% (YI) | - | ||
| Lim et al. [41] | Bilateral BMB | - | 59% (NR) | - | - | 94% | - | - | 55%/95% | - | - | 90% (DA) | - |
| Saiki et al. [42] | BMB | - | 36% (NR) | - | - | 87% (NR) | - | - | 50%/79% | - | - | - | - |
| Al-Sabbagh et al. [44] | BMB or PET+ any of guided biopsy confirmation/MRI/focal uptake/FDG disappearance with treatment | 50% (29–71) | 96% (79–100) | - | 100% (94–100) | 100% (95–100) | - | 100%/84% | 100%/98% | - | 87% (DA) | 99% (DA) | - |
| Min et al. [45] | Bilateral BMB | - | 52% | - | - | 91% | - | - | - | - | - | - | - |
| Kandeel et al. [46] | BMB or PET+ any of concordant morphologic changes by CT/FDG disappearance with treatment/concordant FDG progression on follow-up | 69% (NR) | - | 67% (NR) | 100% (NR) | - | 90% (NR) | 100%/85% | - | 77%/84% | 89% (DA) | - | 82% (DA) |
| Chen et al. [16] | BMB or PET focal | 44% (NR) | 88% (NR) | - | - | - | - | NR/90% | NR/98% | - | 91% (DA) | 98% (DA) | - |
| Chen-Liang et al. [50] | BMB or PET | 40% (27–53) | 69% (52–85) | - | 95% (91–98) | 85% (80–89) | - | NR/85% | NR/95% | - | 83% (DA)/0.4 (YI) | 83% (DA)/0.5 (YI) | |
| Vishnu et al. [51] | BM aspirate and trephine biopsy | - | 86% (56–97) | - | - | 86% (76–92) | - | - | 50%/98% | - | - | 86% (DA) | |
| Alzahrani et al. [33] | BMB or PET | 48% (41–56) | - | 81% (74–86) | - | - | - | NR/79% | - | NR/91% | - | - | - |
| BMB | - | - | 60% (49–70) | - | - | 79% (75–83) | - | - | 36%/91% | - | - | - | |
| BMB concordant | - | - | 77% (63–87) | - | - | 79% (75–83) | - | - | 29%/97% | - | - | - | |
| PET focal | 36% (28–44) | - | - | 91% (88–94) | - | - | 60%/79% | - | - | - | - | - | |
| Berthet et al. [10] | BMB or PET focal + confirmed by guided biopsy/targeted MRI/after chemotherapy by concomitant disappearance of uptake | 24% (9–39) | - | 94% (86–100) | 100% (100–100) | - | 99% (97–100) | 100%/80% | - | 97%/98% | 81% (DA) | - | 98% (DA) |
| Khan et al. [35] | BMB or PET | 40% (NR) | 94% (NR) | - | 100% (NR) | 100% (NR) | - | NR | NR | - | 84% (DA) | 99% (DA) | - |
| Cortes Romera et al. [55] | BMB | - | 95% | - | - | 86% | - | - | 54%/99% | - | - | 87% (DA) | |
| Ref. | N | Adverse Factor Related to BM Assessment (Compared with Its Complementary Good Prognosis Reference in Each Case) | Survival Endpoints | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Event-Free Survival or Progression-Free Survival | Overall Survival | ||||||||
| Prognosis | UV HR (CI 95%) | MV HR (CI 95%) | Prognosis | UV HR (CI 95%) | MV HR (CI 95%) | ||||
| Okamoto et al. * [40] | 184 (subcohort R-CHOP or R-CHOP-like) | BMB+ | 20% (2-year) C-index 0.68 | 4.3 (2.1–8.8) | 2.3 (1.3–6.5) 1 | 24% (2-year) C-index 0.74 | 5.2 (2.6–10.5) | 3 (1.3–6.8) 1 | |
| FCM+ | C-index 0.70 | 3.1 (1.6–5.8) | 2.8 (1.4–5.2) 1 | C-index 0.74 | 2.2 (1.1–4.5) | 1.9 (0.9–3.7) 1 | |||
| Lim et al. ‡ [41] | 512 | BMB+ | - | 3.1 (1.8–5.4) | 1.7 (1.1–2.6) 2 | 52% (2-year) 37% (5-year) | - | - | |
| PET | PET+ | 29% (2-year) | 2.8 (1.6–4.7) | 1.7 (1.1–2.6) 2 | - | - | - | ||
| PET+ focal | - | 2.1 (1.1–3.9) | - | - | - | - | |||
| PET+ diffuse | - | 3.1 (0.8–11) | - | - | - | - | |||
| PET+ heterogeneous | - | 4.2 (1–16.9) | - | - | - | - | |||
| Martin-Moro et al. * [43] | 82 | BMB+/FCM+ | 27% (18-month) | 2.2 (1.4–3.3) | - | 55% (18-month) | 1.9 (1.2–3) | - | |
| BMB−/FCM+ | 23% (18-month) | 4.9 (1.7–14.2) | - | 46% (18-month) | 4.4 (1.5–12.4) | - | |||
| FCM+ | - | 4.8 (2.3–10) | 1.9 (1.3–2.9) 3 2 (1.3–3.1) 4 | - | 3.8 (1.8–8.3) | 1.7 (1.1–2.7) 3 1.7 (1.1–2.7) 4 | |||
| Min et al. * [45] | 600 | BMB+ | - | - | - | 56% (4-year) | - | 1 (0.8–1.3) 5 | |
| PET+ | 43% (4-year) | - | - | 65% (4-year) | - | - | |||
| Kandeel et al. • [46] | 88 | BMB+ | 64% (18-month) | 1.4 (0.5–3.5) | - | - | - | - | |
| PET+ focal | 73% (18-month) | 1 (0.4–2.5) | - | - | - | - | |||
| Alonso-Alvarez et al. * [47] | 189 (subcohort R-CHOP or R-CHOP-like) | Concordant | BMB+ concordant | 32% (5-year) | - | 2.2 (1.1–4.3) 6 | 51% (5-year) | - | 1.6 (0.7–3.4) 6 |
| BMB+ concordant GCB | 25% (5-year) | - | 2.9 (1–8.7) 7 | 38% (5-year) | - | 1.2 (0.3–4.4) 7 | |||
| BMB+ concordant non-GCB | 33% (5-year) | - | 3 (1.4–6.4) 7 | 49% (5-year) | - | 1.6 (0.7–3.9) 7 | |||
| Discordant | BMB/FCM+ discordant | 62% (5-year) | - | 1.5 (0.7–3) 6 | 73% (5-year) | - | 1.5 (0.7–3.2) 6 | ||
| BMB/FCM+ discordant GCB | 76% (5-year) | - | 0.7 (0.1–3) 7 | 76% (5-year) | - | 0.7 (0.1–3.4) 7 | |||
| BMB/FCM+ discordant non-GCB | 46% (5-year) | - | 1.9 (0.9–4.2) 7 | 63% (5-year) | - | 1.6 (0.6–3.7) 7 | |||
| Wang et al. † [48] | 140 (all cases advanced stage) | BMB+ | - | 2.3 (1.4–3.9) | 2.3 (1.4–3.9) 8 | - | 1.7 (1–2.8) | Not significant 8 | |
| PET+ focal | - | 2.1 (1.3–3.6) | Not significant 8 | - | 1.8 (1.1–3) | 1.9 (1.1–3.1) 8 | |||
| BMB+/PET+ | 7 months (median) | - | - | 12 months (median) | - | - | |||
| BMB+/PET- | 14 months (median) | - | - | 27 months (median) | - | - | |||
| BMB−/PET+ | 26 months (median) | - | - | 31 months (median) | - | - | |||
| Greenbaum et al. † [49] | 81 | BMB+/FCM+ | 67 months (median) 47% (1-year) 36% (5-year) 24% (7-year) | - | - | 54 months (median) 43% (1-year) 32% (5-year) 32% (7-year) | - | - | |
| BMB−/FCM+ | 77 months (median) 61% (1-year) 56% (5-year) 49% (7-year) | - | - | 77 months (median) 60% (1-year) 55% (5-year) 54% (7-year) | - | - | |||
| FCM+ | - | - | 2.6 (1–6.8) 9 | - | - | 1.4 (0.7–3) 9 | |||
| Chen et al. † [16] | 193 | BMB+ | 61% (3-year) | 1.8 (0.7–4.6) | - | 61% (3-year) | 4 (1.3–11.9) | - | |
| PET+ focal | 33% (3-year) | 4.4 (2.4–8.2) | 2.3 (1.1–4.7) 10 | 69% (3-year) | 3.7 (1.5–9.3) | Not significant 10 | |||
| PET+ diffuse | 81% (3-year) | 0.9 (0.3–2.4) | - | 94% (3-year) | 0.6 (0.1–4.3) | - | |||
| BMB−/PET+ focal | 0% (3-year) | - | - | 77% (3-year) | - | - | |||
| BMB−/PET+ diffuse | 90% (3-year) | - | - | 100% (3-year) | - | - | |||
| Chen-Liang et al. * [50] | 203 (subcohort R-CHOP) | BMB+ | - | p < 0.001 | 3.6 (1.7–7.6) 11 | - | p = 0.326 | ||
| PET+ | - | p = 0.121 | p > 0.15 11 | - | p = 0.018 | p > 0.15 11 | |||
| Vishnu et al. [51] | 99 (not reported treatment approach) | BMB+ | - | - | - | 65 months (median) 80% (2-year) 66% (5-year) | - | - | |
| PET+ | - | - | - | 67 months (median) 83% (2-year) 79% (5-year) | - | - | |||
| Alzahrani et al. * [33] | 256 (subcohort Ann Arbor IV) | BMB+ or PET+ | 57% (2-year) | - | - | 65% (2-year) | - | - | |
| PET+ | 53% (2-year) | - | - | 63% (2-year) | - | - | |||
| Liang et al. † [52] | 169 | BMB+ | - | 4.5 (2.5–8) | NS 12 | - | 6.2 (3.1–12.7) | NS 12 | |
| PET+ | - | 4 (2.3–6.6) | NS 12 | - | 6.7 (3.4–13.3) | 2.9 (1.2–7) 12 | |||
| 68 (subcohort Ann Arbor IV) | PET+ | 29% (3-year) | - | - | 44% (3-year) | - | - | ||
| Cerci et al. • [20] | 327 | BMB+ | 56% (2-year) | 2.2 (1.3–3.3) | - | 68% (2-year) | - | - | |
| BMB+/PET+ | 45% (2-year) | 2.7 (1.5–4.8) | 1.6 (0.8–3.1) 13 | 55% (2-year) | 3.9 (1.9–8.1) | 2.3 (1–5) 13 | |||
| BMB+/PET+ focal | 46% (2-year) | 2.5 (1.1–5.5) | - | 57% (2-year) | 3 (1.1–8.4) | - | |||
| BMB+/PET- | 80% (2-year) | - | 1.1 (0.4–3.2) 13 | 100% (2-year) | - | 0.5 (0.1–3.7) 13 | |||
| BMB−/PET+ | 81% (2-year) | - | 0.7 (0.4–1.3) 13 | 88% (2-year) | - | 0.7 (0.3–1.7) 13 | |||
| BMB−/PET+ focal | 78% (2-year) | - | - | 87% (2-year) | - | ||||
| Adams et al. * [53] | 71 (subcohort R-CHOP) | BMB+ | - | 3.2 (1.3–7.6) | 3.3 (1.3–8.6) 14 | - | 3.5 (1.3–9.3) | 4.5 (1.6–12.4) 14 | |
| PET+ | - | 0.9 (0.4–2.1) | - | - | 0.7 (0.3–2.2) | - | |||
| Berthet et al. * [10] | 133 | BMB+ | 38% (2-year) | 4.9 (1.6–14.6) | 2.2 (0.8–6) 15 | 63% (2-year) | 4.1 (1.4–12.4) | 2.7 (0.9–8.2) 15 | |
| PET+ | 63% (2-year) | 2.9 (1.2–7) | 2.5 (1.2–5.3) 15 | 76% (2-year) | 2.8 (1.2–6.8) | 2.2 (0.9–5.3) 15 | |||
| Khan et al. † [35] | 44 (subcohort Ann Arbor IV) | BMB+ | - | 3.7 (1.6–8.8) | - | - | 3.9 (1.5–10) | - | |
| PET+ | - | 0.8 (0.3–2) | - | - | 0.9 (0.3–2.5) | - | |||
| PET+/BMB− | - | 0.4 (0.1–1.2) | - | - | 0.4 (0.1–1.6) | - | |||
| Hong et al. * [36] | 89 | BMB+ | 37% (2-year) | - | - | 36% (2-year) | 7.9 (3.2–19.6) | 8.7 (3.2–23.5) 16 | |
| PET+ | 63% (2-year) | - | - | 59% (2-year) | 2 (0.8–5.3) | - | |||
| BMB+/PET+ | 38% (2-year) | - | - | 38% (2-year) | - | - | |||
| BMB+/PET− | 36% (2-year) | - | - | 36% (2-year) | - | - | |||
| BMB−/PET+ | 79% (2-year) | - | - | 73% (2-year) | - | - | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martin-Moro, F.; Lopez-Jimenez, J.; Garcia-Marco, J.A.; Garcia-Vela, J.A. Comparative Review of the Current and Future Strategies to Evaluate Bone Marrow Infiltration at Diffuse Large B-Cell Lymphoma Diagnosis. Diagnostics 2024, 14, 658. https://doi.org/10.3390/diagnostics14060658
Martin-Moro F, Lopez-Jimenez J, Garcia-Marco JA, Garcia-Vela JA. Comparative Review of the Current and Future Strategies to Evaluate Bone Marrow Infiltration at Diffuse Large B-Cell Lymphoma Diagnosis. Diagnostics. 2024; 14(6):658. https://doi.org/10.3390/diagnostics14060658
Chicago/Turabian StyleMartin-Moro, Fernando, Javier Lopez-Jimenez, Jose A. Garcia-Marco, and Jose A. Garcia-Vela. 2024. "Comparative Review of the Current and Future Strategies to Evaluate Bone Marrow Infiltration at Diffuse Large B-Cell Lymphoma Diagnosis" Diagnostics 14, no. 6: 658. https://doi.org/10.3390/diagnostics14060658