
Association of Genetic Risk for Age-Related Macular Degeneration with Morphological Features of the Retinal Microvascular Network
 , , , , , , , and
, , , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Dataset
2.2. PRS Calculation
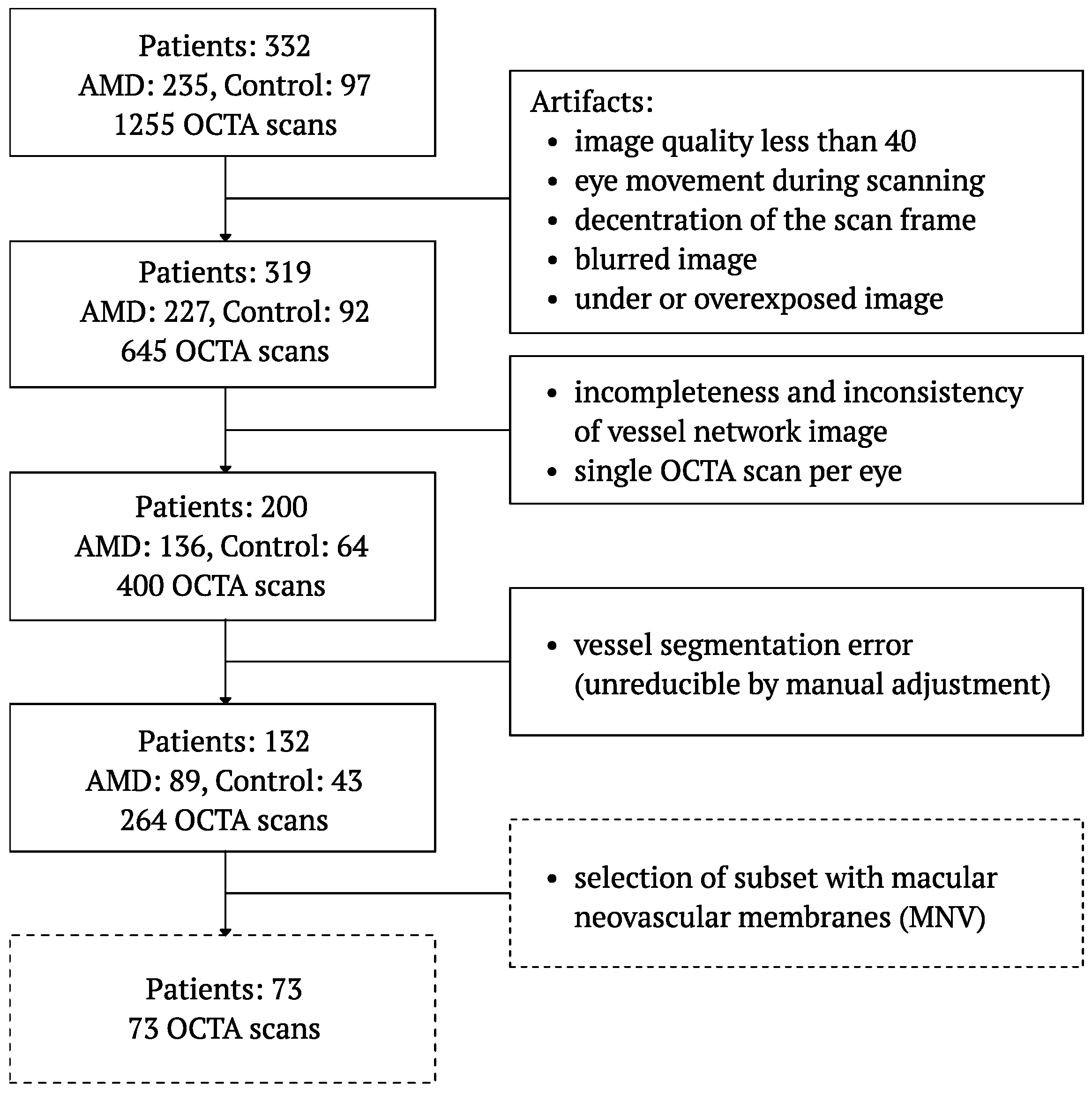
2.3. OCTA Image Selection
2.4. Feature Extraction
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fleckenstein, M.; Keenan, T.D.; Guymer, R.H.; Chakravarthy, U.; Schmitz-Valckenberg, S.; Klaver, C.C.; Wong, W.T.; Chew, E.Y. Age-related macular degeneration. Nat. Rev. Dis. Prim. 2021, 7, 31. [Google Scholar] [CrossRef] [PubMed]
- Pauleikhoff, D.; Harper, C.A.; Marshall, J.; Bird, A.C. Aging changes in Bruch’s membrane: A histochemical and morphologic study. Ophthalmology 1990, 97, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Koller, A.; Lamina, C.; Brandl, C.; Zimmermann, M.E.; Stark, K.J.; Weissensteiner, H.; Würzner, R.; Heid, I.M.; Kronenberg, F. Systemic Evidence for Mitochondrial Dysfunction in Age-Related Macular Degeneration as Revealed by mtDNA Copy Number Measurements in Peripheral Blood. Int. J. Mol. Sci. 2023, 24, 16406. [Google Scholar] [CrossRef] [PubMed]
- Velilla, S.; García-Medina, J.J.; García-Layana, A.; Dolz-Marco, R.; Pons-Vázquez, S.; Pinazo-Durán, M.D.; Gómez-Ulla, F.; Arévalo, J.F.; Díaz-Llopis, M.; Gallego-Pinazo, R.; et al. Smoking and age-related macular degeneration: Review and update. J. Ophthalmol. 2013, 2013, 895147. [Google Scholar] [CrossRef] [PubMed]
- Brandl, C.; Finger, R.P.; Heid, I.M.; Mauschitz, M.M. Age-Related Macular Degeneration in an Ageing Society-Current Epidemiological Research. Klin. Monatsblatter Augenheilkd. 2023, 240, 1052–1059. [Google Scholar]
- Lüdtke, L.; Jürgens, C.; Ittermann, T.; Völzke, H.; Tost, F. Age-related macular degeneration and associated risk factors in the population-based study of health in pomerania (SHIP-Trend). Med Sci. Monit. Int. Med. J. Exp. Clin. Res. 2019, 25, 6383. [Google Scholar] [CrossRef] [PubMed]
- Bullock, J.; Polato, F.; Abu-Asab, M.; Bernardo-Colón, A.; Aflaki, E.; Agbaga, M.P.; Becerra, S.P. Degradation of photoreceptor outer segments by the retinal pigment epithelium requires pigment epithelium-derived factor receptor (PEDF-R). Investig. Ophthalmol. Vis. Sci. 2021, 62, 30. [Google Scholar] [CrossRef] [PubMed]
- Deng, Y.; Qiao, L.; Du, M.; Qu, C.; Wan, L.; Li, J.; Huang, L. Age-related macular degeneration: Epidemiology, genetics, pathophysiology, diagnosis, and targeted therapy. Genes Dis. 2022, 9, 62–79. [Google Scholar] [CrossRef] [PubMed]
- Winkler, T.W.; Grassmann, F.; Brandl, C.; Kiel, C.; Günther, F.; Strunz, T.; Weidner, L.; Zimmermann, M.E.; Korb, C.A.; Poplawski, A.; et al. Genome-wide association meta-analysis for early age-related macular degeneration highlights novel loci and insights for advanced disease. BMC Med. Genom. 2020, 13, 120. [Google Scholar] [CrossRef]
- Age-Related Eye Disease Study Research Group. Risk factors associated with age-related macular degeneration: A case-control study in the age-related eye disease study: Age-related eye disease study report number 3. Ophthalmology 2000, 107, 2224–2232. [Google Scholar] [CrossRef]
- Serra, R.; Rallo, V.; Pinna, A.; Steri, M.; Piras, M.G.; Marongiu, M.; Coscas, F.; Gorospe, M.; Schlessinger, D.; Fiorillo, E.; et al. Polygenic risk score and biochemical/environmental variables predict a low-risk profile of age-related macular degeneration in Sardinia. Graefe’s Arch. Clin. Exp. Ophthalmol. 2023, 261, 691–698. [Google Scholar] [CrossRef]
- Yu, C.; Robman, L.; He, W.; Woods, R.L.; Wolfe, R.; Phung, J.; Makeyeva, G.A.; Hodgson, L.A.; McNeil, J.J.; Guymer, R.H.; et al. Predictive performance of an updated polygenic risk score for age-related macular degeneration. Ophthalmology 2024, in press. [Google Scholar] [CrossRef]
- Shijo, T.; Sakurada, Y.; Yoneyama, S.; Kikushima, W.; Sugiyama, A.; Matsubara, M.; Fukuda, Y.; Mabuchi, F.; Kashiwagi, K. Association between polygenic risk score and one-year outcomes following as-needed aflibercept therapy for exudative age-related macular degeneration. Pharmaceuticals 2020, 13, 257. [Google Scholar] [CrossRef] [PubMed]
- Ulanczyk, Z.; Grabowicz, A.; Mozolewska-Piotrowska, K.; Safranow, K.; Kawa, M.P.; Pałucha, A.; Krawczyk, M.; Sikora, P.; Matczynska, E.; Machaliński, B.; et al. Genetic factors associated with age-related macular degeneration: Identification of a novel PRPH2 single nucleotide polymorphism associated with increased risk of the disease. Acta Ophthalmol. 2021, 99, 739–749. [Google Scholar] [CrossRef]
- Zekavat, S.M.; Sekimitsu, S.; Ye, Y.; Raghu, V.; Zhao, H.; Elze, T.; Segrè, A.V.; Wiggs, J.L.; Natarajan, P.; Del Priore, L.; et al. Photoreceptor layer thinning is an early biomarker for age-related macular degeneration: Epidemiologic and genetic evidence from UK Biobank OCT data. Ophthalmology 2022, 129, 694–707. [Google Scholar] [CrossRef] [PubMed]
- Tang, W.; Ma, J.; Gu, R.; Lei, B.; Ding, X.; Xu, G. Light-induced lipocalin 2 facilitates cellular apoptosis by positively regulating reactive oxygen species/Bim signaling in retinal degeneration. Investig. Ophthalmol. Vis. Sci. 2018, 59, 6014–6025. [Google Scholar] [CrossRef]
- Faatz, H.; Rothaus, K.; Ziegler, M.; Book, M.; Heimes-Bussmann, B.; Pauleikhoff, D.; Lommatzsch, A. Vascular analysis of type 1, 2, and 3 macular neovascularization in age-related macular degeneration using swept-source optical coherence tomography angiography shows new insights into differences of pathologic vasculature and may lead to a more personalized understanding. Biomedicines 2022, 10, 694. [Google Scholar] [CrossRef]
- Campochiaro, P.A. Ocular neovascularization. J. Mol. Med. 2013, 91, 311–321. [Google Scholar] [CrossRef]
- Prenner, J.L.; Halperin, L.S.; Rycroft, C.; Hogue, S.; Liu, Z.W.; Seibert, R. Disease burden in the treatment of age-related macular degeneration: Findings from a time-and-motion study. Am. J. Ophthalmol. 2015, 160, 725–731. [Google Scholar] [CrossRef]
- Steinmetz, J.D.; Bourne, R.R.; Briant, P.S.; Flaxman, S.R.; Taylor, H.R.; Jonas, J.B.; Abdoli, A.A.; Abrha, W.A.; Abualhasan, A.; Abu-Gharbieh, E.G.; et al. Causes of blindness and vision impairment in 2020 and trends over 30 years, and prevalence of avoidable blindness in relation to VISION 2020: The Right to Sight: An analysis for the Global Burden of Disease Study. Lancet Glob. Health 2021, 9, e144–e160. [Google Scholar] [CrossRef]
- Leroux, P.; Agard, E.; Billant, J.; Levron, A.; Bouvarel, H.; Badri, Y.; Douma, I.; Pradat, P.; Dot, C. Long Intervals between intravitreal injections using a Treat-and-Extend protocol in a Real-life context in AMD: The LIRE study. Ophthalmologica 2023, 247, 44–57. [Google Scholar] [CrossRef] [PubMed]
- Pugazhendhi, A.; Hubbell, M.; Jairam, P.; Ambati, B. Neovascular macular degeneration: A review of etiology, risk factors, and recent advances in research and therapy. Int. J. Mol. Sci. 2021, 22, 1170. [Google Scholar] [CrossRef] [PubMed]
- Colijn, J.M.; Buitendijk, G.H.; Prokofyeva, E.; Alves, D.; Cachulo, M.L.; Khawaja, A.P.; Cougnard-Gregoire, A.; Merle, B.M.; Korb, C.; Erke, M.G.; et al. Prevalence of age-related macular degeneration in Europe: The past and the future. Ophthalmology 2017, 124, 1753–1763. [Google Scholar] [CrossRef] [PubMed]
- Tun, Y.Z.; Aimmanee, P. A Complete Review of Automatic Detection, Segmentation, and Quantification of Neovascularization in Optical Coherence Tomography Angiography Images. Diagnostics 2023, 13, 3407. [Google Scholar] [CrossRef] [PubMed]
- Spaide, R.F.; Fujimoto, J.G.; Waheed, N.K. Image artifacts in optical coherence tomography angiography. Retina 2015, 35, 2163. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Cui, Y.; Wang, J.C.; Lu, Y.; Zeng, R.; Katz, R.; Wu, D.M.; Eliott, D.; Vavvas, D.G.; Husain, D.; et al. Different scan protocols affect the detection rates of diabetic retinopathy lesions by wide-field swept-source optical coherence tomography angiography. Am. J. Ophthalmol. 2020, 215, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Dabir, S.; Bhatt, V.; Bhatt, D.; Rajan, M.; Samant, P.; Munusamy, S.; Webers, C.; Berendschot, T. Need for manual segmentation in optical coherence tomography angiography of neovascular age-related macular degeneration. PLoS ONE 2020, 15, e0244828. [Google Scholar] [CrossRef] [PubMed]
- Martin, M. Cutadapt removes adapter sequences from high-throughput sequencing reads. EMBnet. J. 2011, 17, 10–12. [Google Scholar] [CrossRef]
- Van der Auwera, G.A.; Carneiro, M.O.; Hartl, C.; Poplin, R.; Del Angel, G.; Levy-Moonshine, A.; Jordan, T.; Shakir, K.; Roazen, D.; Thibault, J.; et al. From FastQ data to high-confidence variant calls: The genome analysis toolkit best practices pipeline. Curr. Protoc. Bioinform. 2013, 43, 11.10.1–11.10.33. [Google Scholar] [CrossRef]
- Wąsowska, A.; Sendecki, A.; Boguszewska-Chachulska, A.; Teper, S. Polygenic Risk Score and Rare Variant Burden Identified by Targeted Sequencing in a Group of Patients with Pigment Epithelial Detachment in Age-Related Macular Degeneration. Genes 2023, 14, 1707. [Google Scholar] [CrossRef]
- Untracht, G.R.; Matos, R.S.; Dikaios, N.; Bapir, M.; Durrani, A.K.; Butsabong, T.; Campagnolo, P.; Sampson, D.D.; Heiss, C.; Sampson, D.M. OCTAVA: An open-source toolbox for quantitative analysis of optical coherence tomography angiography images. PLoS ONE 2021, 16, e0261052. [Google Scholar] [CrossRef] [PubMed]
- Freedman, I.G.; Li, E.; Hui, L.; Adelman, R.A.; Nwanyanwu, K.; Wang, J.C. The Impact of Image Processing Algorithms on Optical Coherence Tomography Angiography Metrics and Study Conclusions in Diabetic Retinopathy. Transl. Vis. Sci. Technol. 2022, 11, 7. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.B.; Kim, Y.W.; Kim, J.M.; Jo, Y.J.; Kim, J.Y. The importance of signal strength in quantitative assessment of retinal vessel density using optical coherence tomography angiography. Sci. Rep. 2018, 8, 12897. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.J.; Lee, J.E.; Sadda, S.R.; Park, S.W.; Byon, I. Impact of signal strength on quantitative retinal and choriocapillaris flow measurement from optical coherence tomography angiography. Sci. Rep. 2022, 12, 4692. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.B.; Kim, Y.W.; Nam, K.Y.; Ryu, C.K.; Jo, Y.J.; Kim, J.Y. Signal strength as an important factor in the analysis of peripapillary microvascular density using optical coherence tomography angiography. Sci. Rep. 2019, 9, 16299. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.J.; Hong, S.K. Polygenic risk score in prostate cancer. Curr. Opin. Urol. 2022, 32, 466–471. [Google Scholar] [CrossRef] [PubMed]
- Bontzos, G.; Kabanarou, S.A.; Garnavou-Xirou, C.; Gkizis, I.; Kontou, E.; Triantafyllou, D.; Xirou, T. Segmentation errors and motion artifacts in OCT-A associated with epiretinal membranes. Can. J. Ophthalmol. 2020, 55, 293–300. [Google Scholar] [CrossRef] [PubMed]
- Wicklein, R.; Yam, C.; Noll, C.; Aly, L.; Banze, N.; Romahn, E.F.; Wolf, E.; Hemmer, B.; Oertel, F.C.; Zimmermann, H.; et al. The OSCAR-MP consensus criteria for quality assessment of retinal optical coherence tomography angiography. Neurol. Neuroimmunol. Neuroinflamm. 2023, 10, e200169. [Google Scholar] [CrossRef]
- Sekimitsu, S.; Shweikh, Y.; Shareef, S.; Zhao, Y.; Elze, T.; Segrè, A.; Wiggs, J.; Zebardast, N. Association of retinal optical coherence tomography metrics and polygenic risk scores with cognitive function and future cognitive decline. Br. J. Ophthalmol. 2023, 108, 599–606. [Google Scholar] [CrossRef]
- Saks, D.G.; Schulz, A.; Qassim, A.; Marshall, H.; Hewitt, A.W.; MacGregor, S.; Craig, J.E.; Graham, S.L. Genetic risk of glaucoma is associated with vascular and retinal nerve fibre wedge defects. Acta Ophthalmol. 2023, 102, e185–e194. [Google Scholar] [CrossRef]
- Wang, X.Y.; Wang, L.L.; Xu, L.; Liang, S.Z.; Yu, M.C.; Zhang, Q.Y.; Dong, Q.J. Evaluation of polygenic risk score for risk prediction of gastric cancer. World J. Gastrointest. Oncol. 2023, 15, 276. [Google Scholar] [CrossRef] [PubMed]
- Briggs, S.E.; Law, P.; East, J.E.; Wordsworth, S.; Dunlop, M.; Houlston, R.; Hippisley-Cox, J.; Tomlinson, I. Integrating genome-wide polygenic risk scores and non-genetic risk to predict colorectal cancer diagnosis using UK Biobank data: Population based cohort study. BMJ 2022, 379, e071707. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| AMD | Control | p-Value | |
|---|---|---|---|
| N | 89 | 43 | ∼ |
| Age [years] | 72.47 (7.99) | 71.00 (7.04) | 0.307 |
| Sex [male/female] | 40/49 | 10/33 | 0.026 |
| Visual acuity [logMAR] | 0.48 (0.45) | 0.11 (0.18) | <0.001 |
| Choroidal thickness [m] | 237.23 (105.45) | 273.49 (82.03) | 0.001 |
| AMD | Control | |||||
|---|---|---|---|---|---|---|
| Feature | M | SD | M | SD | p-Value | |
| Diameter [m] | Mean | 47.97 | 7.10 | 46.67 | 1.47 | 0.4858 |
| Median | 48.64 | 6.87 | 47.42 | 1.64 | 0.9512 | |
| Variance | 35.31 | 76.69 | 25.21 | 4.23 | 0.0193 | |
| Skewness | −0.21 | 0.64 | −0.38 | 0.44 | 0.0457 | |
| Kurtosis | 2.69 | 1.85 | 2.51 | 0.94 | 0.1231 | |
| Length [mm] | Mean | 774.44 | 79.50 | 770.44 | 46.24 | 0.5359 |
| Median | 578.41 | 76.37 | 603.62 | 63.09 | 0.0920 | |
| Total | 50.18 | 4.87 | 50.46 | 3.99 | 0.9729 | |
| Variance | 515,754.41 | 195,925.48 | 449,083.87 | 106,514.09 | 0.0521 | |
| Skewness | 1.97 | 0.55 | 1.85 | 0.48 | 0.2512 | |
| Kurtosis | 8.04 | 3.26 | 7.62 | 2.90 | 0.5247 | |
| Tortuosity | Mean | 0.1139 | 0.0121 | 0.1155 | 0.0106 | 0.3614 |
| Variance | 0.0190 | 0.0094 | 0.0181 | 0.0073 | 0.8270 | |
| Skewness | 3.04 | 0.72 | 3.12 | 0.80 | 0.8631 | |
| Kurtosis | 14.219 | 5.671 | 15.267 | 7.002 | 0.6392 | |
| Fractal Dimension | Mean | 1.42 | 0.03 | 1.40 | 0.01 | 0.0024 |
| Variance | 0.525 | 0.024 | 0.516 | 0.005 | 0.0123 | |
| Nodes | 43.76 | 9.19 | 42.64 | 6.13 | 0.4683 | |
| VLD [%] | 2.676 | 0.233 | 2.628 | 0.208 | 0.2574 | |
| VAD [%] | 15.853 | 4.143 | 15.081 | 1.406 | 0.1373 | |
| BD [Nodes/mm] | 0.863 | 0.129 | 0.842 | 0.079 | 0.3289 | |
| FAZSCP [mm2] | 0.4737 | 0.3828 | 0.3446 | 0.0015 | 0.0616 | |
| FAZDCP [mm2] | 0.5146 | 0.4261 | 0.4034 | 0.1555 | 0.6727 | |
| Univariate | Multivariate (GEE) | ||||
|---|---|---|---|---|---|
| Feature | Pearson’s r | p -Value | Coefficient | p -Value | |
| Covariants | AMD | ∼ | ∼ | 0.8041 | <0.001 |
| Age | ∼ | ∼ | −0.0013 | 0.915 | |
| Sex | ∼ | ∼ | 0.3924 | 0.014 | |
| PED | ∼ | ∼ | 0.3196 | 0.101 | |
| MNV | ∼ | ∼ | 0.0255 | 0.893 | |
| Diameter [m] | Mean | 0.042 | 0.630 | 1.344 | 0.179 |
| Median | 0.040 | 0.650 | −1.234 | 0.217 | |
| Variance | 0.016 | 0.853 | −0.384 | 0.701 | |
| Skewness | −0.049 | 0.574 | −0.055 | 0.956 | |
| Kurtosis | −0.100 | 0.253 | −0.298 | 0.765 | |
| Length [mm] | Mean | −0.012 | 0.893 | −0.709 | 0.479 |
| Median | −0.078 | 0.372 | 0.345 | 0.730 | |
| Total | −0.124 | 0.157 | −0.308 | 0.758 | |
| Variance | 0.070 | 0.422 | −0.431 | 0.667 | |
| Skewness | 0.093 | 0.288 | 1.831 | 0.067 | |
| Kurtosis | 0.056 | 0.525 | −1.517 | 0.129 | |
| Tortuosity | Mean | 0.075 | 0.396 | 1.315 | 0.188 |
| Variance | 0.043 | 0.621 | −0.008 | 0.994 | |
| Skewness | −0.142 | 0.105 | −1.542 | 0.123 | |
| Kurtosis | −0.144 | 0.101 | 1.157 | 0.247 | |
| Fractal Dimension | Mean | 0.027 | 0.755 | −0.508 | 0.611 |
| Variance | 0.072 | 0.414 | −0.078 | 0.938 | |
| Nodes | −0.027 | 0.756 | 0.430 | 0.667 | |
| VLD [%] | −0.098 | 0.263 | 0.124 | 0.901 | |
| VAD [%] | −0.011 | 0.899 | 0.059 | 0.953 | |
| BD [Nodes/mm] | 0.024 | 0.788 | −0.296 | 0.768 | |
| FAZSCP [mm2] | 0.105 | 0.230 | −0.133 | 0.894 | |
| FAZDCP [mm2] | 0.103 | 0.241 | 0.410 | 0.682 | |
| MNVCC area [mm2] | −0.054 | 0.692 | −0.771 | 0.441 | |
| MNVOR area [mm2] | 0.104 | 0.692 | 1.398 | 0.162 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sendecki, A.; Ledwoń, D.; Tuszy, A.; Nycz, J.; Wąsowska, A.; Boguszewska-Chachulska, A.; Wylęgała, A.; Mitas, A.W.; Wylęgała, E.; Teper, S. Association of Genetic Risk for Age-Related Macular Degeneration with Morphological Features of the Retinal Microvascular Network. Diagnostics 2024, 14, 770. https://doi.org/10.3390/diagnostics14070770
Sendecki A, Ledwoń D, Tuszy A, Nycz J, Wąsowska A, Boguszewska-Chachulska A, Wylęgała A, Mitas AW, Wylęgała E, Teper S. Association of Genetic Risk for Age-Related Macular Degeneration with Morphological Features of the Retinal Microvascular Network. Diagnostics. 2024; 14(7):770. https://doi.org/10.3390/diagnostics14070770
Chicago/Turabian StyleSendecki, Adam, Daniel Ledwoń, Aleksandra Tuszy, Julia Nycz, Anna Wąsowska, Anna Boguszewska-Chachulska, Adam Wylęgała, Andrzej W. Mitas, Edward Wylęgała, and Sławomir Teper. 2024. "Association of Genetic Risk for Age-Related Macular Degeneration with Morphological Features of the Retinal Microvascular Network" Diagnostics 14, no. 7: 770. https://doi.org/10.3390/diagnostics14070770