
The Clinical Impact of the Pulmonary Embolism Severity Index on the Length of Hospital Stay of Patients with Pulmonary Embolism: A Randomized Controlled Trial
 ,
,  , , ,
, , ,
Abstract
1. Introduction
2. Methods
2.1. Participants
2.2. Interventions
2.3. Outcomes
2.4. Sample Size
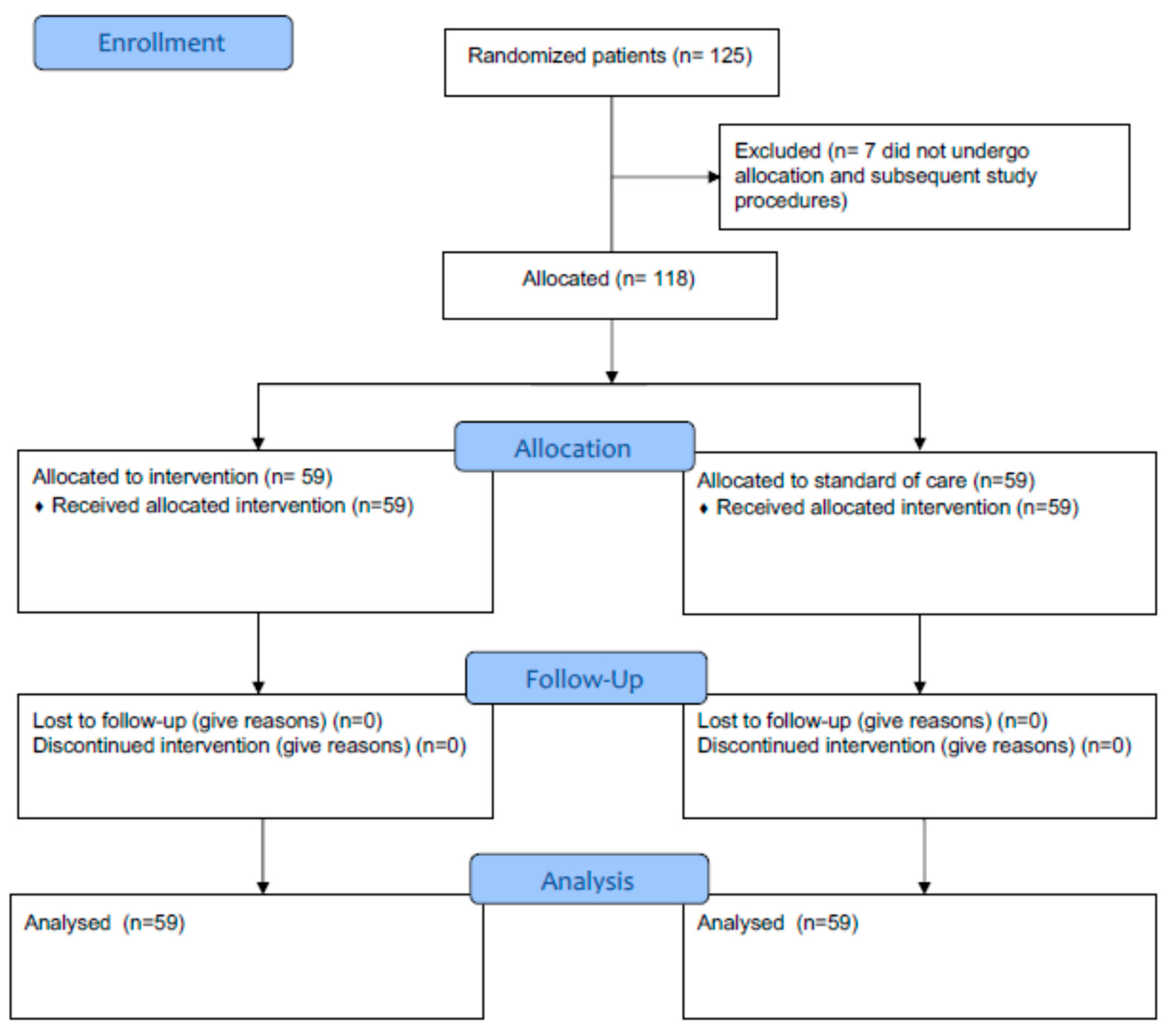
2.5. Randomization
2.6. Statistical Analysis
3. Results
Secondary Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wendelboe, A.M.; Raskob, G.E. Global burden of thrombosis: Epidemiologic aspects. Circ. Res. 2016, 118, 1340–1347. [Google Scholar] [CrossRef] [PubMed]
- Khan, F.; Tritschler, T.; Kahn, S.R.; Rodger, M.A. Venous thromboembolism. Lancet 2021, 398, 64–77. [Google Scholar] [CrossRef] [PubMed]
- Becattini, C.; Agnelli, G.; Lankeit, M.; Masotti, L.; Pruszczyk, P.; Casazza, F.; Vanni, S.; Nitti, C.; Kamphuisen, P.; Vedovati, M.C.; et al. Acute pulmonary embolism: Mortality prediction by the 2014 European Society of Cardiology risk stratification model. Eur. Respir. J. 2016, 48, 780–786. [Google Scholar] [CrossRef] [PubMed]
- Martinez Licha, C.R.; McCurdy, C.M.; Maldonado, S.M.; Lee, L.S. Current Management of Acute Pulmonary Embolism. Ann. Thorac. Cardiovasc. Surg. 2020, 26, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Yoo, H.H.; Nunes-Nogueira, V.S.; Fortes Villas Boas, P.J.; Broderick, C. Outpatient versus inpatient treatment for acute pulmonary embolism. Cochrane Database Syst. Rev. 2022, 5, CD010019. [Google Scholar] [PubMed]
- Peacock, W.F.; Singer, A.J. Reducing the hospital burden associated with the treatment of pulmonary embolism. J. Thromb. Haemost. 2019, 17, 720–736. [Google Scholar] [CrossRef]
- Konstantinides, S.V.; Meyer, G.; Becattini, C.; Bueno, H.; Geersing, G.J.; Harjola, V.P.; Huisman, M.V.; Humbert, M.; Jennings, C.S.; Jiménez, D.; et al. ESC Scientific Document Group. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur. Heart J. 2020, 41, 543–603. [Google Scholar] [CrossRef] [PubMed]
- de Miguel-Diez, J.; Jimenez-Garcia, R.; Jimenez, D.; Monreal, M.; Guijarro, R.; Otero, R.; Hernandez-Barrera, V.; Trujillo-Santos, J.; Lopez de Andres, A.; Carrasco-Garrido, P. Trends in hospital admissions for pulmonary embolism in Spain from 2002 to 2011. Eur. Respir. J. 2014, 44, 942–950. [Google Scholar] [CrossRef] [PubMed]
- Aujesky, D.; Obrosky, D.S.; Stone, R.A.; Auble, T.E.; Perrier, A.; Cornuz, J.; Roy, P.M.; Fine, M.J. Derivation and validation of a prognostic model for pulmonary embolism. Am. J. Respir. Crit. Care Med. 2005, 172, 1041–1046. [Google Scholar] [CrossRef]
- Kohn, C.G.; Mearns, E.S.; Parker, M.W.; Hernandez, A.V.; Coleman, C.I. Prognostic accuracy of clinical prediction rules for early post-pulmonary embolism all-cause mortality: A bivariate meta-analysis. Chest 2015, 147, 1043–1062. [Google Scholar] [CrossRef]
- Wicki, J.; Perrier, A.; Perneger, T.V.; Bounameaux, H.; Junod, A.F. Predicting adverse outcome in patients with acute pulmonary embolism: A risk score. Thromb. Haemost. 2000, 84, 548–552. [Google Scholar] [CrossRef] [PubMed]
- McGinn, T.G.; Guyatt, G.H.; Wyer, P.C.; Naylor, C.D.; Stiell, I.G.; Richardson, W.S. Users’ guides to the medical literature: XXII: How to use articles about clinical decision rules. Evidence-Based Medicine Working Group. JAMA 2000, 284, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G. Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD): The TRIPOD statement. BMJ 2015, 350, g7594. [Google Scholar] [CrossRef] [PubMed]
- Donadini, M.P.; Dentali, F.; Castellaneta, M.; Gnerre, P.; La Regina, M.; Masotti, L.; Pieralli, F.; Pomero, F.; Re, R.; Guasti, L.; et al. LORPELHS study group. Pulmonary embolism prognostic factors and length of hospital stay: A cohort study. Thromb. Res. 2017, 156, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Dentali, F.; Ageno, W.; Pomero, F.; Fenoglio, L.; Squizzato, A.; Bonzini, M. Time trends and case fatality rate of in-hospital treated pulmonary embolism during 11 years of observation in Northwestern Italy. Thromb. Haemost. 2016, 115, 399–405. [Google Scholar] [PubMed]
- Jiménez, D.; de Miguel-Díez, J.; Guijarro, R.; Trujillo-Santos, J.; Otero, R.; Barba, R.; Muriel, A.; Meyer, G.; Yusen, R.D.; Monreal, M.; et al. Trends in the management and outcomes of acute pulmonary embolism: Analysis from the RIETE registry. J. Am. Coll. Cardiol. 2016, 67, 162–170. [Google Scholar] [CrossRef] [PubMed]
- Becattini, C.; Agnelli, G.; Maggioni, A.P.; Dentali, F.; Fabbri, A.; Enea, I.; Pomero, F.; Ruggieri, M.P.; di Lenarda, A.; Cimini, L.A.; et al. COPE Investigators. Contemporary Management and Clinical Course of Acute Pulmonary Embolism: The COPE Study. Thromb. Haemost. 2023, 123, 613–626. [Google Scholar] [PubMed]
- EINSTEIN–PE Investigators; Büller, H.R.; Prins, M.H.; Lensin, A.W.; Decousus, H.; Jacobson, B.F.; Minar, E.; Chlumsky, J.; Verhamme, P.; Wells, P.; et al. Oral rivaroxaban for the treatment of symptomatic pulmonary embolism. N. Engl. J. Med. 2012, 366, 1287–1297. [Google Scholar] [PubMed]
- Agnelli, G.; Buller, H.R.; Cohen, A.; Curto, M.; Gallus, A.S.; Johnson, M.; Masiukiewicz, U.; Pak, R.; Thompson, J.; Raskob, G.E.; et al. AMPLIFY Investigators. Oral apixaban for the treatment of acute venous thromboembolism. N. Engl. J. Med. 2013, 369, 799–808. [Google Scholar] [CrossRef] [PubMed]
- Hokusai-VTE Investigators; Büller, H.R.; Décousus, H.; Grosso, M.A.; Mercuri, M.; Middeldorp, S.; Prins, M.H.; Raskob, G.E.; Schellong, S.M.; Schwocho, L.; et al. Edoxaban versus warfarin for the treatment of symptomatic venous thromboembolism. N. Engl. J. Med. 2013, 369, 1406–1415. [Google Scholar]
- Schulman, S.; Kearon, C.; Kakkar, A.K.; Mismetti, P.; Schellong, S.; Eriksson, H.; Baanstra, D.; Schnee, J.; Goldhaber, S.Z. RE-COVER Study Group. Dabigatran versus warfarin in the treatment of acute venous thromboembolism. N. Engl. J. Med. 2009, 361, 2342–2352. [Google Scholar] [CrossRef] [PubMed]
- Schulman, S.; Kearon, C. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J. Thromb. Haemost. 2005, 3, 692–694. [Google Scholar] [CrossRef] [PubMed]
- Torbicki, A.; Perrier, A.; Konstantinides, S.; Agnelli, G.; Galiè, N.; Pruszczyk, P.; Bengel, F.; Brady, A.J.; Ferreira, D.; Janssens, U.; et al. Guidelines on the diagnosis and management of acute pulmonary embolism: The Task Force for the Diagnosis and Management of Acute Pulmonary Embolism of the European Society of Cardiology (ESC). Eur. Heart J. 2008, 29, 2276–2315. [Google Scholar] [PubMed]
- Barco, S.; Mahmoudpour, S.H.; Planquette, B.; Sanchez, O.; Konstantinides, S.V.; Meyer, G. Prognostic value of right ventricular dysfunction or elevated cardiac biomarkers in patients with low-risk pulmonary embolism: A systematic review and meta-analysis. Eur. Heart J. 2019, 40, 902–910. [Google Scholar] [CrossRef] [PubMed]
- Rivera-Lebron, B.; McDaniel, M.; Ahrar, K.; Alrifai, A.; Dudzinski, D.M.; Fanola, C.; Blais, D.; Janicke, D.; Melamed, R.; Mohrien, K.; et al. Diagnosis, Treatment and Follow Up of Acute Pulmonary Embolism: Consensus Practice from the PERT Consortium. Clin. Appl. Thromb. Hemost. 2019, 25, 1076029619853037. [Google Scholar] [CrossRef] [PubMed]
- Jaff, M.R.; McMurtry, M.S.; Archer, S.L.; Cushman, M.; Goldenberg, N.; Goldhaber, S.Z.; Jenkins, J.S.; Kline, J.A.; Michaels, A.D.; Thistlethwaite, P.; et al. Management of massive and submassive pulmonary embolism, iliofemoral deep vein thrombosis, and chronic thromboembolic pulmonary hypertension: A scientific statement from the American Heart Association. Circulation 2011, 123, 1788–1830. [Google Scholar] [CrossRef] [PubMed]
- Vinson, D.R.; Mark, D.G.; Chettipally, U.K.; Huang, J.; Rauchwerger, A.S.; Reed, M.E.; Lin, J.S.; Kene, M.V.; Wang, D.H.; Sax, D.R.; et al. Increasing Safe Outpatient Management of Emergency Department Patients With Pulmonary Embolism: A Controlled Pragmatic Trial. Ann. Intern. Med. 2018, 169, 855–865. [Google Scholar] [CrossRef] [PubMed]
- Jiménez, D.; Rodríguez, C.; León, F.; Jara-Palomares, L.; López-Reyes, R.; Ruiz-Artacho, P.; Elías, T.; Otero, R.; García-Ortega, A.; Rivas-Guerrero, A.; et al. Randomised controlled trial of a prognostic assessment and management pathway to reduce the length of hospital stay in normotensive patients with acute pulmonary embolism. Eur. Respir. J. 2022, 59, 2100412. [Google Scholar] [CrossRef]
- Bookhart, B.K.; Haskell, L.; Bamber, L.; Wang, M.; Schein, J.; Mody, S.H. Length of stay and economic consequences with rivaroxaban vs enoxaparin/vitamin K antagonist in patients with DVT and PE: Findings from the North American EINSTEIN clinical trial program. J. Med. Econ. 2014, 17, 691–695. [Google Scholar] [CrossRef]


{kind=link}
| Patients, n | PESI (n = 59) | Routine Practice (n = 59) | p |
|---|---|---|---|
| Age, ys—mean (SD) | 75.6 (13.1) | 75.7 (12.7) | 0.966 |
| Sex, female—n (%) | 31 (52.5) | 25 (42.4) | 0.356 |
| Weight—mean (SD) | 75.4 (15.5) | 76.3 (9.8) | 0.706 |
| Unprovoked PE—n (%) | 38 (64.4) | 40 (69.0) | 0.845 |
| Active cancer—n (%) | 12 (20.3) | 11 (18.6) | 0.816 |
| Concomitant DVT—n (%) | 35 (59.3) | 30 (50.9) | 0.459 |
| Incidental PE—n (%) | 14 (23.7) | 6 (10.2) | 0.085 |
| SBP < 90 mmHg | 2 (3.4) | 1 (1.7) | 0.768 |
| RVD * on TTE—n (%) | 10 (21.3) | 16 (33.3) | 0.266 |
| RVD on lab biomarkers | 13 (48.2) | 14 (37.8) | 0.826 |
| PESI—mean (SD) | 115.1 (49.9) | 115.4 (44.3) § | 0.972 |
| PESI class III, IV, V—n (%) | 39 (66.1) | 44 (74.6) § | 0.420 |
| DOAC treatment—n (%) | 37 (62.7) | 34 (57.6) | 0.706 |
| Outcomes | PESI (n = 59) | Routine Practice (n = 59) | p |
|---|---|---|---|
| LOS, days—median (IQR) | 8 (6–12) | 8 (6–12) | 0.63 |
| Discharge < 48 h—n (%) | 0 (0.0) | 0 (0.0) | |
| In-hospital clinical outcomes | |||
| Death—n (%) | 4 (6.8) | 2 (3.4) | 0.68 |
| Recurrent VTE—n (%) | 0 (0.0) | 1 (1.7) | 0.99 |
| Major bleeding—n (%) | 0 (0.0) | 2 (3.4) | 0.50 |
| Heparin injection site hematoma *—n (%) | 2 (14.3) | 0 (0.0) | 0.49 |
| Heparin-induced thrombocytopenia—n (%) | 0 (0.0) | 0 (0.0) | |
| Hospital-acquired infections—n (%) | 4 (6.8) | 7 (11.9) | 0.34 |
| Iatrogenic complications—n (%) § | 1 (2.1) | 0 (0.0) | 0.99 |
| Immobilization syndrome—n (%) ¶ | 13 (24.5) | 11 (20.4) | 0.60 |
| Pressure sores—n (%) ¶ | 5 (9.4) | 7 (13.2) | 0.54 |
| 90-day clinical outcomes | |||
| Death—n (%) | 5 (9.4) | 3 (5.3) | 0.48 |
| Recurrent VTE—n (%) | 0 (0.0) | 2 (3.4) | 0.50 |
| Major bleeding—n (%) | 0 (0.0) | 2 (3.4) | 0.50 |
| New hospital admission—n (%) | 4 (7.6) | 4 (7.0) | 0.99 |
| PESI (n = 59) | Routine Practice (n = 59) | p | |
|---|---|---|---|
| Home—n (%) | 48 (87.3) | 49 (86.0) | 0.84 * |
| Subacute/post-acute care facilities—n (%) | 2 (3.6) | 2 (3.5) | |
| Rehabilitation clinics—n (%) | 0 (0.0) | 0 (0.0) | |
| Nursing home—n (%) | 5 (9.1) | 6 (10.5) |
| PESI (n = 59) | Routine Practice (n = 59) | p | |
|---|---|---|---|
| Absence of caregiver—n (%) | 10 (17.2) | 10 (17.2) | 0.97 |
| Socio-familiar issues impacting discharge—n (%) | 10 (17.2) | 8 (14.3) | 0.66 |
| Incidental PE—n (%) | 14 (23.7) | 6 (10.2) | 0.05 |
| Hemodynamically unstable PE—n (%) | 2 (3.4) | 1 (1.7) | 0.99 |
| RVD—n (%) | 17 (28.8) | 22 (37.3) | 0.33 |
| Age, ys—mean (SD) | 75.6 (13.1) | 75.7 (12.7) | 0.95 |
| Active cancer—n (%) | 12 (20.3) | 11 (18.6) | 0.82 |
| Clinical complications—n (%) | 14 (28.6) | 18 (35.3) | 0.47 |
| Anemia (<12 g/dL)—n (%) | 17 (29.8) | 19 (32.2) | 0.84 |
| Thrombocytopenia (<100.000/mm3)—n (%) | 2 (3.6) | 2 (3.4) | 0.96 |
| Leucocytosis (>12.000/mm3)—n (%) | 10 (18.2) | 13 (22.0) | 0.61 |
| Likert Scale | PESI (n = 59) | Routine Practice (n = 59) | p |
|---|---|---|---|
| Satisfied about hospitalization—mean (SD) (1, no; 5, very much) | 3.8 (0.7) | 3.8 (0.7) | 0.89 |
|
Appropriate LOS (1, too low; 5, too high) | 3.2 (0.7) | 3.2 (0.5) | 0.83 |
|
Worried about PE recurrence (1, no; 5, very much) | 2.9 (1.0) | 2.9 (0.8) | 0.88 |
|
Worried about bleeding (1, no; 5, very much) | 2.7 (1.0) | 2.7 (0.8) | 0.75 |
| Outcomes | DOAC (n = 71) | LMWH +/− VKA (n = 47) | p |
|---|---|---|---|
| LOS, days—median (IQR) | 8 (5–11) | 9 (7–12) | 0.04 |
| Discharge < 48 h—n (%) | 0 (0.0) | 0 (0.0) | |
| In-hospital clinical outcomes | |||
| Death—n (%) | 1 (1.4) | 5 (10.6) | 0.04 |
| Recurrent VTE—n (%) | 0 (0.0) | 1 (2.1) | 0.40 |
| Major bleeding—n (%) | 0 (0.0) | 2 (4.3) | 0.16 |
| Heparin injection site hematoma—n (%) | 0 (0.0) | 2 (20.0) | 0.15 |
| Heparin-induced thrombocytopenia—n (%) | 0 (0.0) | 0 (0.0) | |
| Hospital-acquired infections—n (%) | 7 (9.9) | 4 (8.5) | 0.99 |
| Iatrogenic complications—n (%) | 1 (1.8) | 0 (0.0) | 0.99 |
| Immobilization syndrome—n (%) | 11 (17.5) | 13 (29.6) | 0.14 |
| Pressure sores—n (%) | 2 (3.2) | 10 (22.7) | 0.003 |
| 90-day clinical outcomes | |||
| Death—n (%) | 1 (1.6) | 7 (14.9) | 0.02 |
| Recurrent VTE—n (%) | 0 (0.0) | 2 (4.3) | 0.18 |
| Major bleeding—n (%) | 0 (0.0) | 2 (4.3) | 0.16 |
| New hospital admission—n (%) | 8 (12.7) | 0 (0.0) | 0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Donadini, M.P.; Mumoli, N.; Fenu, P.; Pomero, F.; Re, R.; Palmiero, G.; Spadafora, L.; Mazzi, V.; Grittini, A.; Bertù, L.; et al. The Clinical Impact of the Pulmonary Embolism Severity Index on the Length of Hospital Stay of Patients with Pulmonary Embolism: A Randomized Controlled Trial. Diagnostics 2024, 14, 776. https://doi.org/10.3390/diagnostics14070776
Donadini MP, Mumoli N, Fenu P, Pomero F, Re R, Palmiero G, Spadafora L, Mazzi V, Grittini A, Bertù L, et al. The Clinical Impact of the Pulmonary Embolism Severity Index on the Length of Hospital Stay of Patients with Pulmonary Embolism: A Randomized Controlled Trial. Diagnostics. 2024; 14(7):776. https://doi.org/10.3390/diagnostics14070776
Chicago/Turabian StyleDonadini, Marco Paolo, Nicola Mumoli, Patrizia Fenu, Fulvio Pomero, Roberta Re, Gerardo Palmiero, Laura Spadafora, Valeria Mazzi, Alessandra Grittini, Lorenza Bertù, and et al. 2024. "The Clinical Impact of the Pulmonary Embolism Severity Index on the Length of Hospital Stay of Patients with Pulmonary Embolism: A Randomized Controlled Trial" Diagnostics 14, no. 7: 776. https://doi.org/10.3390/diagnostics14070776
APA StyleDonadini, M. P., Mumoli, N., Fenu, P., Pomero, F., Re, R., Palmiero, G., Spadafora, L., Mazzi, V., Grittini, A., Bertù, L., Aujesky, D., Dentali, F., Ageno, W., & Squizzato, A. (2024). The Clinical Impact of the Pulmonary Embolism Severity Index on the Length of Hospital Stay of Patients with Pulmonary Embolism: A Randomized Controlled Trial. Diagnostics, 14(7), 776. https://doi.org/10.3390/diagnostics14070776