
The Diagnostic Value of Soluble Triggering Receptor Expressed on Myeloid Cells for Patients with Acute Stone Pyelonephritis

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Protocol
2.2. Biochemical Analysis
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shields, J.; Maxwell, A.P. Acute pyelonephritis can have serious complications. Practitioner 2010, 254, 19–24. [Google Scholar]
- Mahyar, A.; Ayazi, P.; Ahmadi, R.; Daneshi-Kohan, M.M.; Hashemi, H.J.; Dalirani, R.; Moshiri, S.A.; Habibi, M.; Sahmani, M.; Sahmani, A.A. Are serum procalcitonin and interleukin-1 beta suitable markers for diagnosis of acute pyelonephritis in children? Prague Med. Rep. 2014, 115, 16–23. [Google Scholar] [CrossRef]
- Masajtis-Zagajewska, A.; Kurnatowska, I.; Wajdlich, M.; Nowicki, M. Utility of copeptin and standard inflammatory markers in the diagnostics of upper and lower urinary tract infections. BMC Urol. 2015, 15, 67. [Google Scholar] [CrossRef]
- van der Starre, W.E.; Zunder, S.M.; Vollaard, A.M.; van Nieuwkoop, C.; Stalenhoef, J.E.; Delfos, N.M.; Van’t Wout, J.W.; Spelt, I.C.; Blom, J.W.; Leyten, E.M.; et al. Prognostic value of pro-adrenomedullin, procalcitonin and C-reactive protein in predicting outcome of febrile urinary tract infection. Clin. Microbiol. Infect. 2014, 20, 1048–1054. [Google Scholar] [CrossRef]
- Bouchon, A.; Dietrich, J.; Colonna, M. Cutting edge: Inflammatory responses can be triggered by TREM-1, a novel receptor expressed on neutrophils and monocytes. J. Immunol. 2000, 164, 4991–4995. [Google Scholar] [CrossRef]
- De Vlieger, G.; Vanhorebeek, I.; Wouters, P.J.; Derese, I.; Casaer, M.P.; Debaveye, Y.; Hermans, G.; Meersseman, P.; Moller, H.J.; Van den Berghe, G.; et al. The soluble mannose receptor (sMR/sCD206) in critically ill patients with invasive fungal infections, bacterial infections or non-infectious inflammation: A secondary analysis of the EPaNIC RCT. Crit. Care 2019, 23, 270. [Google Scholar] [CrossRef]
- Tency, I.; Verstraelen, H.; Saerens, B.; Verhasselt, B.; Vaneechoutte, M.; Degomme, O.; Verhelst, R.; Temmerman, M. Elevated soluble triggering receptor expressed on myeloid cells (sTREM)-1 levels in maternal serum during term and preterm labor. PLoS ONE 2013, 8, e56050. [Google Scholar] [CrossRef]
- Gomez-Pina, V.; Soares-Schanoski, A.; Rodriguez-Rojas, A.; Del Fresno, C.; Garcia, F.; Vallejo-Cremades, M.T.; Fernandez-Ruiz, I.; Arnalich, F.; Fuentes-Prior, P.; Lopez-Collazo, E. Metalloproteinases shed TREM-1 ectodomain from lipopolysaccharide-stimulated human monocytes. J. Immunol. 2007, 179, 4065–4073. [Google Scholar] [CrossRef]
- van Bremen, T.; Dromann, D.; Luitjens, K.; Dodt, C.; Dalhoff, K.; Goldmann, T.; Schaaf, B. Triggering receptor expressed on myeloid cells-1 (Trem-1) on blood neutrophils is associated with cytokine inducibility in human E. coli sepsis. Diagn. Pathol. 2013, 8, 24. [Google Scholar] [CrossRef]
- Wu, Y.; Wang, F.; Fan, X.; Bao, R.; Bo, L.; Li, J.; Deng, X. Accuracy of plasma sTREM-1 for sepsis diagnosis in systemic inflammatory patients: A systematic review and meta-analysis. Crit. Care 2012, 16, R229. [Google Scholar] [CrossRef]
- Dai, X.; Zeng, Z.; Fu, C.; Zhang, S.; Cai, Y.; Chen, Z. Diagnostic value of neutrophil gelatinase-associated lipocalin, cystatin C, and soluble triggering receptor expressed on myeloid cells-1 in critically ill patients with sepsis-associated acute kidney injury. Crit. Care 2015, 19, 223. [Google Scholar] [CrossRef]
- Gibot, S.; Cravoisy, A.; Levy, B.; Bene, M.C.; Faure, G.; Bollaert, P.E. Soluble triggering receptor expressed on myeloid cells and the diagnosis of pneumonia. N. Engl. J. Med. 2004, 350, 451–458. [Google Scholar] [CrossRef]
- Ramirez, P.; Kot, P.; Marti, V.; Gomez, M.D.; Martinez, R.; Saiz, V.; Catala, F.; Bonastre, J.; Menendez, R. Diagnostic implications of soluble triggering receptor expressed on myeloid cells-1 in patients with acute respiratory distress syndrome and abdominal diseases: A preliminary observational study. Crit. Care 2011, 15, R50. [Google Scholar] [CrossRef]
- Ehsanipour, F.; Noorbakhsh, S.; Zarabi, V.; Movahedi, Z.; Rahimzadeh, N. Comparison the Serum STREM1 Levels Between Children with Upper and Lower UTI. Curr. Pediatr. Rev. 2017, 13, 152–156. [Google Scholar] [CrossRef]
- Chishti, A.S.; Maul, E.C.; Nazario, R.J.; Bennett, J.S.; Kiessling, S.G. A guideline for the inpatient care of children with pyelonephritis. Ann. Saudi Med. 2010, 30, 341–349. [Google Scholar] [CrossRef][Green Version]
- Ozkaramanli Gur, D.; Gur, O.; Guzel, S.; Akyuz, A.; Gurkan, S.; Alpsoy, S.; Gulec, N.S.; Koc, F. Inflammatory Mediators Across the Spectrum of Ankle-Brachial Index. J. Atheroscler. Thromb. 2019, 26, 351–361. [Google Scholar] [CrossRef]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef]
- Shaikh, K.J.; Osio, V.A.; Leeflang, M.M.; Shaikh, N. Procalcitonin, C-reactive protein, and erythrocyte sedimentation rate for the diagnosis of acute pyelonephritis in children. Cochrane Database Syst. Rev. 2020, 9, CD009185. [Google Scholar] [CrossRef]
- Millner, R.; Becknell, B. Urinary Tract Infections. Pediatr. Clin. N. Am. 2019, 66, 1–13. [Google Scholar] [CrossRef]
- Enikeev, D.V.; Glybochko, P.; Alyaev, Y.; Enikeev, M.; Rapoport, L. Imaging technologies in the diagnosis and treatment of acute pyelonephritis. Urologia 2017, 84, 179–184. [Google Scholar] [CrossRef]
- Su, L.X.; Feng, L.; Zhang, J.; Xiao, Y.J.; Jia, Y.H.; Yan, P.; Feng, D.; Xie, L.X. Diagnostic value of urine sTREM-1 for sepsis and relevant acute kidney injuries: A prospective study. Crit. Care 2011, 15, R250. [Google Scholar] [CrossRef]
- Jiang, J.; Wang, X.; Cheng, T.; Han, M.; Wu, X.; Wan, H.; Yu, D. Dynamic Monitoring of sTREM-1 and Other Biomarkers in Acute Cholangitis. Mediat. Inflamm. 2020, 2020, 8203813. [Google Scholar] [CrossRef]
- Cao, C.; Gu, J.; Zhang, J. Soluble triggering receptor expressed on myeloid cell-1 (sTREM-1): A potential biomarker for the diagnosis of infectious diseases. Front. Med. 2017, 11, 169–177. [Google Scholar] [CrossRef]
- Jiyong, J.; Tiancha, H.; Wei, C.; Huahao, S. Diagnostic value of the soluble triggering receptor expressed on myeloid cells-1 in bacterial infection: A meta-analysis. Intensive Care Med. 2009, 35, 587–595. [Google Scholar] [CrossRef]
- Tursun, S.; Alpcan, A.; Özsoy, M.; Badem, N.D.; Kandur, Y.; Acar, B.Ç. Diagnostic value of plasma soluble triggering receptor expressed on myeloid cells-1 in children with urinary tract infections. J. Pediatr. Infect. Dis. 2021, 16, 129–133. [Google Scholar] [CrossRef]
- Sierra-Diaz, E.; Bravo Cuellar, A.; Ortiz Lazareno, P.C.; Garcia Gutierrez, M.; Georgina, H.F.; Anaya Prado, R. Urine TREM-1 as a marker of urinary tract infection in children. J. Int. Med. Res. 2017, 45, 631–638. [Google Scholar] [CrossRef]
- Chastre, J.; Luyt, C.E.; Trouillet, J.L.; Combes, A. New diagnostic and prognostic markers of ventilator-associated pneumonia. Curr. Opin. Crit. Care 2006, 12, 446–451. [Google Scholar] [CrossRef]
- Liu, X.R.; Xu, J.; Wang, Y.M.; Ji, M.S.; Liu, F.S. The effects of paeoniflorin injection on soluble triggering receptor expressed on myeloid-1 (sTREM-1) levels in severe septic rats. Korean J. Physiol. Pharmacol. 2016, 20, 565–571. [Google Scholar] [CrossRef]
- Cetin, N.; Kiraz, Z.K.; Gencler, A. Serum Presepsin, Proadrenomedullin andTriggering Receptor Expressed on Myeloid Cells-1 (TREM-1) as Biomarkers for the Diagnosis of Acute Pyelonephritis. Indian. Pediatr. 2020, 57, 715–718. [Google Scholar] [CrossRef]
- Ford, J.W.; McVicar, D.W. TREM and TREM-like receptors in inflammation and disease. Curr. Opin. Immunol. 2009, 21, 38–46. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Control n = 23 | ASP n = 46 | p |
|---|---|---|---|
| Age, years | 48.8 ± 12.7 | 47.7 ± 16.8 | 0.783 |
| Male gender, n (%) | 15 (65.2) | 27 (58.7) | 0.794 |
| Comorbidity, n (%) | 7 (30.4) | 16 (34.8) | 0.790 |
| Hypertension | 5 (21.7) | 8 (17.4) | 0.748 |
| Diabetes mellitus | 4 (17.4) | 7 (15.2) | 0.999 |
| Urinalysis, n (%) | |||
| Pyuria | - | 46 (100.0) | <0.001 * |
| Positive nitrites | - | 29 (63.0) | <0.001 * |
| Leukocyte esterase | - | 42 (91.3) | <0.001 * |
| Positive uroculture ‡ | - | 28 (60.9) | <0.001 * |
| Radiological findings, n (%) | |||
| Stone | - | 46 (100.0) | <0.001 * |
| Hydronephrosis | - | 9 (19.6) | <0.001 * |
| Hypoechogenic areas | - | 3 (6.5) | <0.001 * |
| Thickening of pelvic wall | - | 2 (4.3) | <0.001 * |
| Variables | Control n = 23 | ASP | p 1 | p 2 | ∆p | |
|---|---|---|---|---|---|---|
| Pre-Treatment n = 46 | Post-Treatment n = 46 | |||||
| Leukocyte counts, ×103/µL | 7.2 (6.3–8.4) | 12.4 (11.3–16.4) | 7.6 (7.0–8.5) | <0.001 * | 0.387 | <0.001 * |
| CRP, mg/L | 1.5 (0.8–2.5) | 129.7 (77.8–230.0) | 4.5 (3.4–8.9) | <0.001 * | <0.001 * | <0.001 * |
| Procalcitonin, μg/L | 0.03 (0.02–0.04) | 0.26 (0.10–2.60) | 0.04 (0.03–0.08) | <0.001 * | 0.080 | <0.001 * |
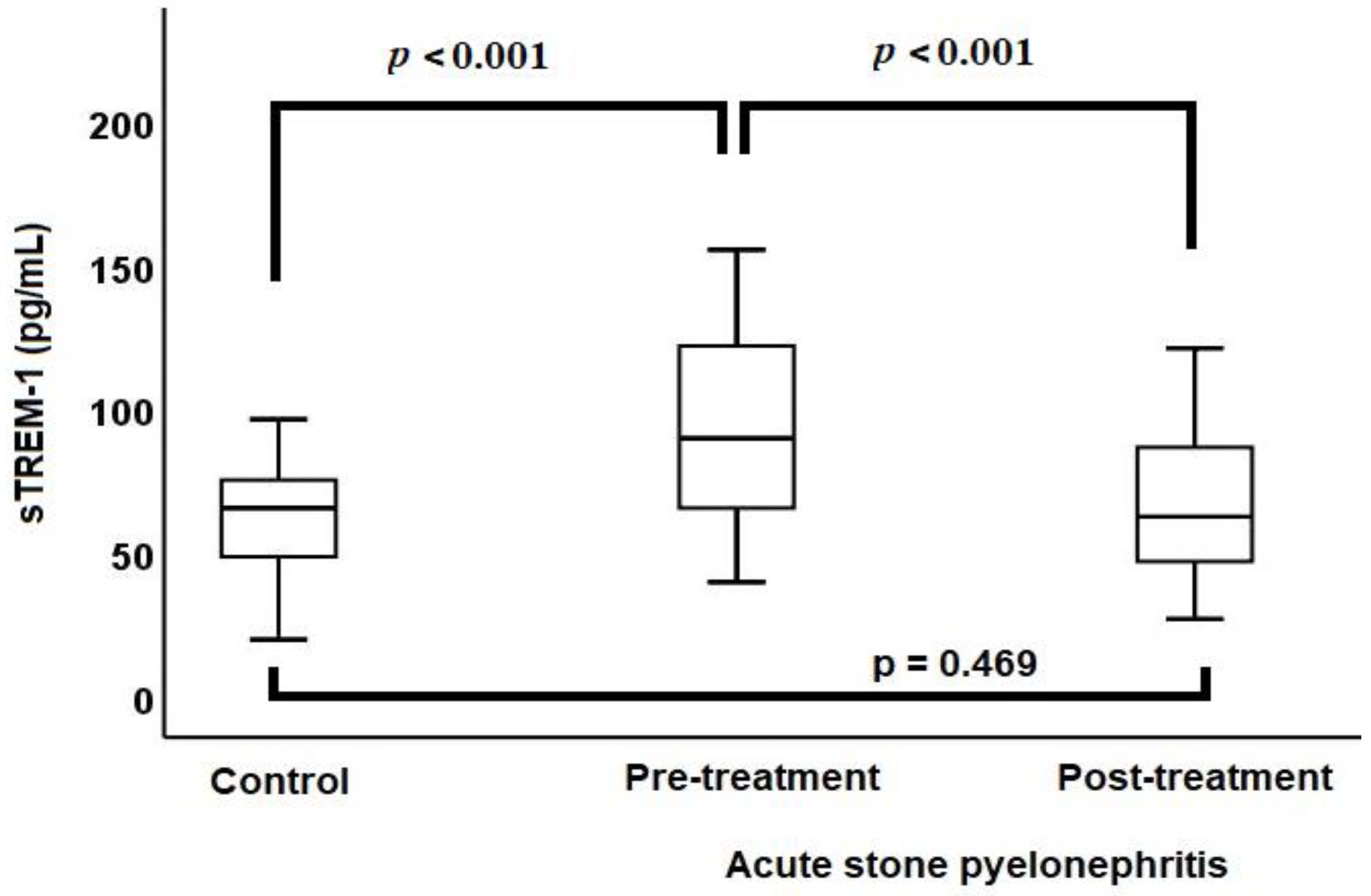
| sTREM-1, pg/mL | 68.4 (50.0–75.4) | 98.6 (70.6–124.8) | 65.7 (48.4–90.3) | <0.001 * | 0.469 | <0.001 * |
| Variables | sTREM-1 | |||
|---|---|---|---|---|
| Control | ASP | |||
| r | p | r | p | |
| Pre-treatment | ||||
| Leukocyte counts | 0.14 | 0.556 | 0.325 | 0.028 * |
| CRP | −0.297 | 0.204 | 0.412 | 0.004 * |
| Procalcitonin | −0.148 | 0.533 | 0.535 | <0.001 * |
| Post-treatment change | ||||
| Leukocyte counts | - | - | 0.279 | 0.132 |
| CRP | - | - | 0.265 | 0.157 |
| Procalcitonin | - | - | 0.311 | 0.036 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Özsoy, M.; Ataman, M.; Şahin, S.K.; Şenocak, İ.; Varlibaş, A.; Yuvanç, E.; Çifci, A.; Başaralı, M.K.; Kırtıl, G.; Yilmaz, E. The Diagnostic Value of Soluble Triggering Receptor Expressed on Myeloid Cells for Patients with Acute Stone Pyelonephritis. Diagnostics 2024, 14, 777. https://doi.org/10.3390/diagnostics14070777
Özsoy M, Ataman M, Şahin SK, Şenocak İ, Varlibaş A, Yuvanç E, Çifci A, Başaralı MK, Kırtıl G, Yilmaz E. The Diagnostic Value of Soluble Triggering Receptor Expressed on Myeloid Cells for Patients with Acute Stone Pyelonephritis. Diagnostics. 2024; 14(7):777. https://doi.org/10.3390/diagnostics14070777
Chicago/Turabian StyleÖzsoy, Metin, Miraç Ataman, Serhat Kazım Şahin, İbrahim Şenocak, Artuner Varlibaş, Ercan Yuvanç, Aydın Çifci, Mustafa Kemal Başaralı, Gül Kırtıl, and Erdal Yilmaz. 2024. "The Diagnostic Value of Soluble Triggering Receptor Expressed on Myeloid Cells for Patients with Acute Stone Pyelonephritis" Diagnostics 14, no. 7: 777. https://doi.org/10.3390/diagnostics14070777
APA StyleÖzsoy, M., Ataman, M., Şahin, S. K., Şenocak, İ., Varlibaş, A., Yuvanç, E., Çifci, A., Başaralı, M. K., Kırtıl, G., & Yilmaz, E. (2024). The Diagnostic Value of Soluble Triggering Receptor Expressed on Myeloid Cells for Patients with Acute Stone Pyelonephritis. Diagnostics, 14(7), 777. https://doi.org/10.3390/diagnostics14070777