
Opportunistic Screening for Acute Vertebral Fractures on a Routine Abdominal or Chest Computed Tomography Scans Using an Automated Deep Learning Model


Abstract
1. Introduction
2. Materials and Methods
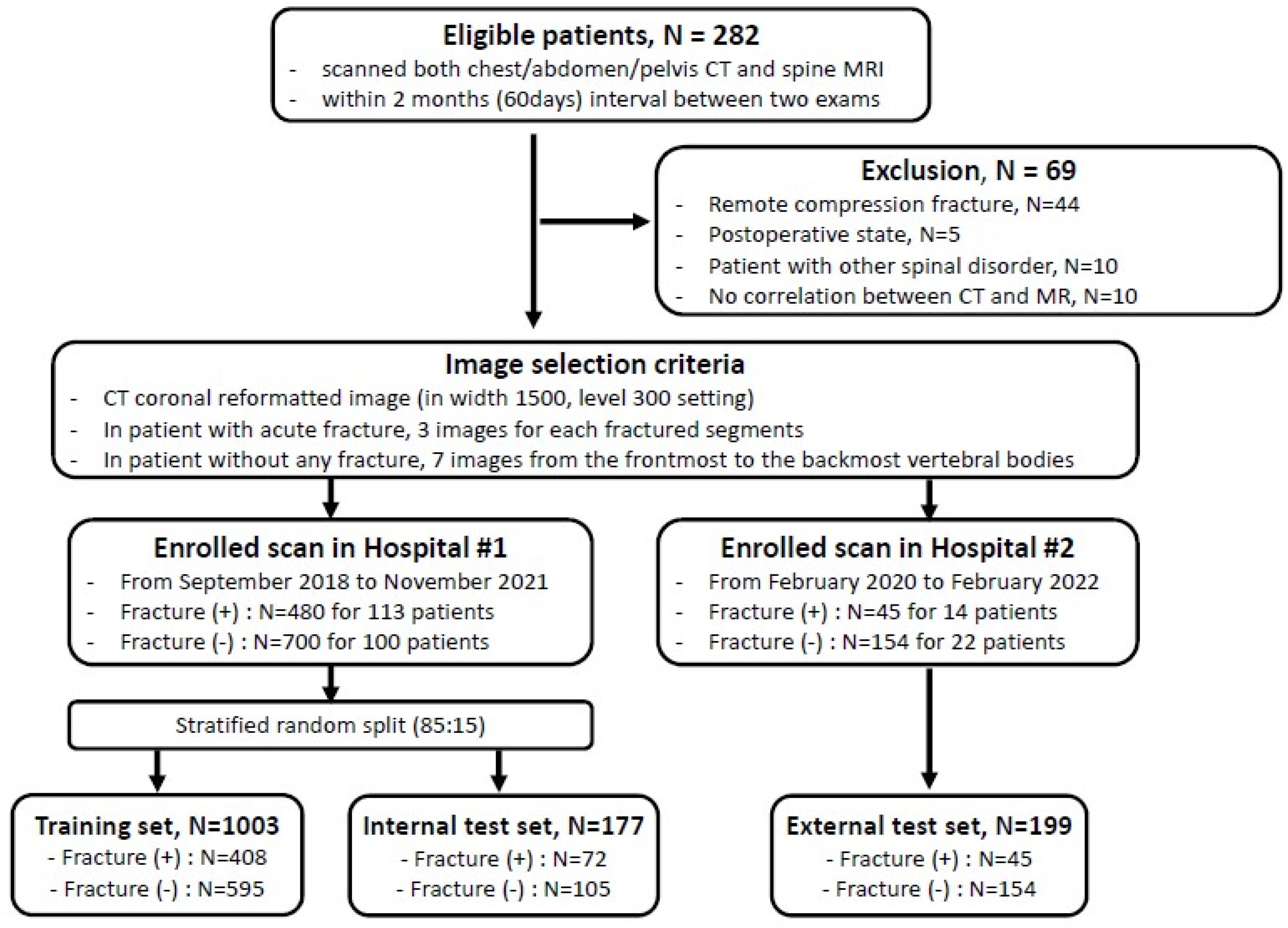
2.1. Patient Datasets
2.2. Image Selection
2.3. Deep Learning Model Development
2.4. Observer Study
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Stand-Alone AI Performance
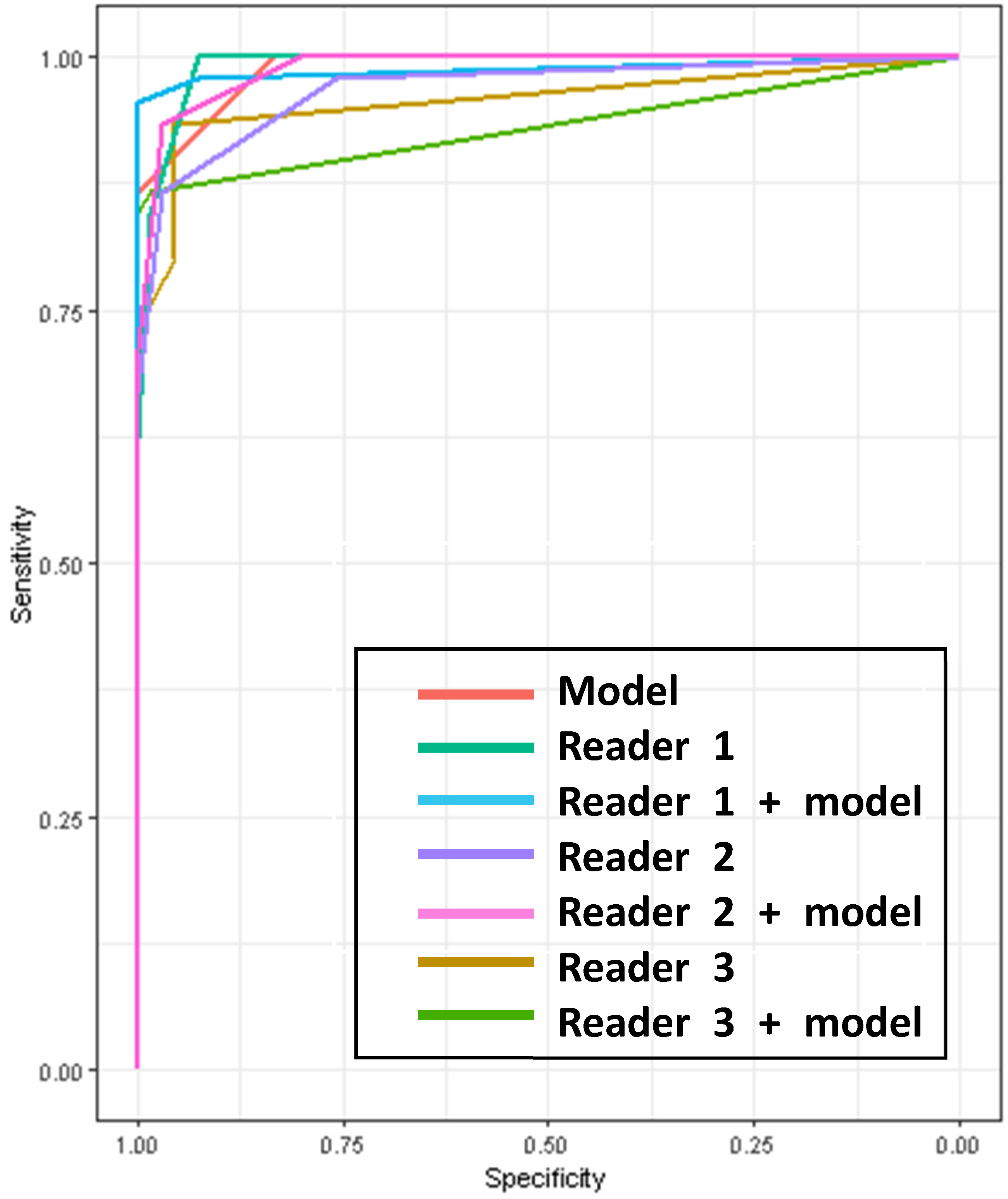
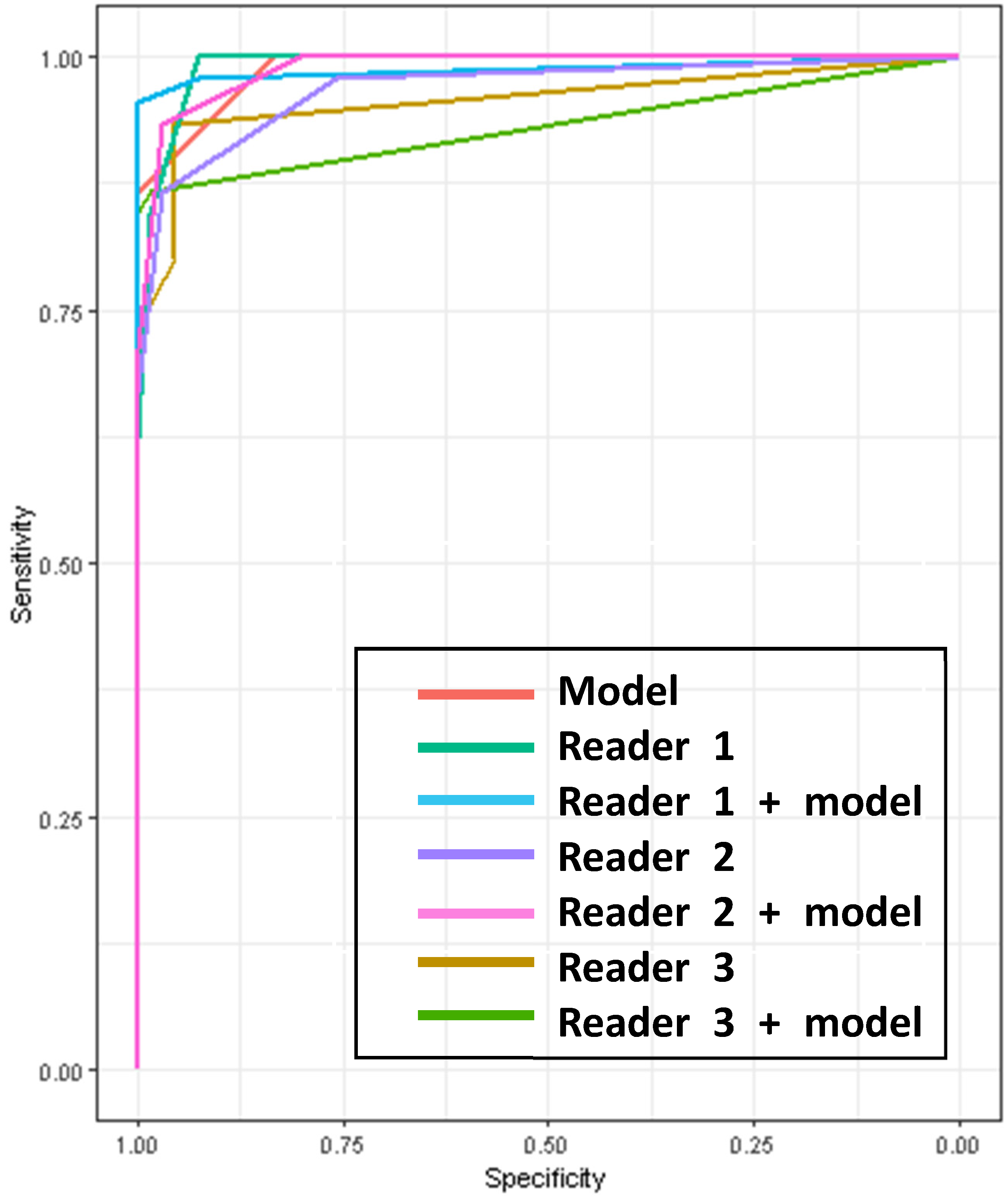
3.3. Observer Study
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Prevention and management of osteoporosis. World Health Organ. Tech. Rep. Ser. 2003, 921, 1–164. [Google Scholar]
- Delmas, P.D. Treatment of postmenopausal osteoporosis. Lancet 2002, 359, 2018–2026. [Google Scholar] [CrossRef] [PubMed]
- Link, T.M.; Guglielmi, G.; van Kuijk, C.; Adams, J.E. Radiologic assessment of osteoporotic vertebral fractuzres: Diagnostic and prognostic implications. Eur. Radiol. 2005, 15, 1521–1532. [Google Scholar] [CrossRef] [PubMed]
- Friedrich, M.; Gittler, G.; Pieler-Bruha, E. Misleading history of pain location in 51 patients with osteoporotic vertebral fractures. Eur. Spine J. 2006, 15, 1797–1800. [Google Scholar] [CrossRef]
- Delmas, P.D.; van de Langerijt, L.; Watts, N.B.; Eastell, R.; Genant, H.; Grauer, A.; Cahall, D.L. Underdiagnosis of Vertebral Fractures Is a Worldwide Problem: The IMPACT Study. J. Bone Miner. Res. 2005, 20, 557–563. [Google Scholar] [CrossRef] [PubMed]
- Bartalena, T.; Giannelli, G.; Rinaldi, M.F.; Rimondi, E.; Rinaldi, G.; Sverzellati, N.; Gavelli, G. Prevalence of thoracolumbar vertebral fractures on multidetector CT: Underreporting by radiologists. Eur. J. Radiol. 2009, 69, 555–559. [Google Scholar] [CrossRef] [PubMed]
- Williams, A.L.; Al-Busaidi, A.; Sparrow, P.J.; Adams, J.E.; Whitehouse, R.W. Under-reporting of osteoporotic vertebral fractures on computed tomography. Eur. J. Radiol. 2009, 69, 179–183. [Google Scholar] [CrossRef] [PubMed]
- Müller, D.; Bauer, J.S.; Zeile, M.; Rummeny, E.J.; Link, T.M. Significance of sagittal reformations in routine thoracic and abdominal multislice CT studies for detecting osteoporotic fractures and other spine abnormalities. Eur. Radiol. 2008, 18, 1696–1702. [Google Scholar] [CrossRef] [PubMed]
- Obaid, H.; Husamaldin, Z.; Bhatt, R. Underdiagnosis of vertebral collapse on routine multidetector computed tomography scan of the abdomen. Acta Radiol. 2008, 49, 795–800. [Google Scholar] [CrossRef]
- Carberry, G.A.; Pooler, B.D.; Binkley, N.; Lauder, T.B.; Bruce, R.J.; Pickhardt, P.J.; Petritsch, B.; Kosmala, A.; Weng, A.M.; Krauss, B.; et al. Unreported Vertebral Body Compression Fractures at Abdominal Multidetector CT. Radiology 2013, 268, 120–126. [Google Scholar] [CrossRef]
- Baum, T.; Bauer, J.S.; Klinder, T.; Dobritz, M.; Rummeny, E.J.; Noël, P.B.; Lorenz, C. Automatic detection of osteoporotic vertebral fractures in routine thoracic and abdominal MDCT. Eur. Radiol. 2014, 24, 872–880. [Google Scholar] [CrossRef] [PubMed]
- Tomita, N.; Cheung, Y.Y.; Hassanpour, S. Deep neural networks for automatic detection of osteoporotic vertebral fractures on CT scans. Comput. Biol. Med. 2018, 98, 8–15. [Google Scholar] [CrossRef]
- Murata, K.; Endo, K.; Aihara, T.; Suzuki, H.; Sawaji, Y.; Matsuoka, Y.; Nishimura, H.; Takamatsu, T.; Konishi, T.; Maekawa, A.; et al. Artificial intelligence for the detection of vertebral fractures on plain spinal radiography. Sci. Rep. 2020, 10, 20031. [Google Scholar] [CrossRef] [PubMed]
- Burns, J.E.; Yao, J.; Summers, R.M.; Pickhardt, P.J.; Graffy, P.M.; Perez, A.A.; Lubner, M.G.; Elton, D.C.; Zea, R.; Lee, S.J.; et al. Vertebral Body Compression Fractures and Bone Density: Automated Detection and Classification on CT Images. Radiology 2017, 284, 788–797. [Google Scholar] [CrossRef]
- Guermazi, A.; Tannoury, C.; Kompel, A.J.; Murakami, A.M.; Ducarouge, A.; Gillibert, A.; Li, X.; Tournier, A.; Lahoud, Y.; Jarraya, M.; et al. Improving Radiographic Fracture Recognition Performance and Efficiency Using Artificial Intelligence. Radiology 2022, 302, 627–636. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.-Y.; Hsu, B.W.-Y.; Yin, Y.-K.; Lin, F.-H.; Yang, T.-H.; Yang, R.-S.; Lee, C.-K.; Tseng, V.S. Application of deep learning algorithm to detect and visualize vertebral fractures on plain frontal radiographs. PLOS ONE 2021, 16, e0245992. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zhang, Y.; Zhang, E.; Chen, Y.; Wang, Q.; Liu, K.; Yu, H.J.; Yuan, H.; Lang, N.; Su, M.-Y. Differential diagnosis of benign and malignant vertebral fracture on CT using deep learning. Eur. Radiol. 2021, 31, 9612–9619. [Google Scholar] [CrossRef] [PubMed]
- Seo, J.W.; Lim, S.H.; Jeong, J.G.; Kim, Y.J.; Kim, K.G.; Jeon, J.Y. A deep learning algorithm for automated measurement of vertebral body compression from X-ray images. Sci. Rep. 2021, 11, 13732. [Google Scholar] [CrossRef]
- Dong, Q.; Luo, G.; Lane, N.E.; Lui, L.-Y.; Marshall, L.M.; Kado, D.M.; Cawthon, P.; Perry, J.; Johnston, S.K.; Haynor, D.; et al. Deep Learning Classification of Spinal Osteoporotic Compression Fractures on Radiographs using an Adaptation of the Genant Semiquantitative Criteria. Acad. Radiol. 2022, 29, 1819–1832. [Google Scholar] [CrossRef]
- Crandall, D. Acute versus chronic vertebral compression fractures treated with kyphoplasty: Early results*1. Spine J. 2004, 4, 418–424. [Google Scholar] [CrossRef]
- Hardy, C.; Hazelton, J.P.; Gefen, R. Added Value of Dedicated Spine CT to Detect Fracture in Patients with CT Chest, Abdomen, and Pelvis in the Trauma Setting. Curr. Probl. Diagn. Radiol. 2019, 48, 554–557. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Binkley, N.; Lubner, M.G.; Bruce, R.J.; Ziemlewicz, T.J.; Pickhardt, P.J. Opportunistic screening for osteoporosis using the sagittal reconstruction from routine abdominal CT for combined assessment of vertebral fractures and density. Osteoporos. Int. 2016, 27, 1131–1136. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Internal Test Hospital | External Test Hospital | ||
|---|---|---|---|---|
| Without Fracture | With Fracture | Without Fracture | With Fracture | |
| No. of patients | 100 | 113 | 22 | 14 |
| Age (years) * | 56.1 ± 14.6 | 61.2 ± 19.5 | 61.2 ± 18.0 | 73.9 ± 12.6 |
| No. of Men (%) | 57/100 (57) | 60/113 (53.1) | 9/22 (40.9) | 8/14 (57.1) |
| CT-MR scan interval (days) * | 13.9 ± 16.0 | 8.0 ± 11.4 | 9.8 ± 11.4 | 4.2 ± 3.9 |
| No. of CT scan-ordered department (%) | ||||
| 22/100 (22) | 26/113 (23.0) | 0 | 0 |
| 28/100 (28) | 32/113 (28.3) | 0 | 0 |
| 0 | 5/113 (4.4) | 12/22 (54.5) | 11/14 (78.6) |
| 50/100 (50) | 50/113 (44.2) | 10/22 (45.5) | 3/14 (21.4) |
| No. per fractured segment | Total 160 | Total 15 | ||
| 6/160 (3.8) | 0 | ||
| 32/160 (20) | 3/15 (20) | ||
| 42/160 (26.3) | 4/15 (26.7) | ||
| 36/160 (22.5) | 5/15 (33.3) | ||
| 20/160 (12.5) | 1/15 (6.7) | ||
| 18/160 (11.3) | 0 | ||
| 3/160 (1.9) | 1/15 (6.7) | ||
| 3/160 (1.9) ** | 1/15 (6.7) *** | ||
| Total (n = 111) | AI | Reader 1 | Reader 2 | Reader 3 | ||||
|---|---|---|---|---|---|---|---|---|
| Without AI | With AI | Without AI | With AI | Without AI | With AI | |||
| AUROC | 0.9889 (0.9762–0.9977) | 0.9912 (0.977–0.999) | 0.9872 (0.9637–1) | 0.968 (0.9437–0.9937) | 0.9897 (0.9777–0.996) | 0.9576 (0.9142–0.9936) | 0.9322 (0.8871–0.9768) | |
| Sensitivity | 84.44 (70.54–93.51) | 95.56 (84.85–99.46) | 86.67 (73.21–94.95) | 93.33 (81.73–98.60) | 80 (65.4–90.42) | 86.67 (73.21–94.95) | ||
| : p-value | 0.07 | 0.25 | 0.25 | |||||
| Specificity | 100 (94.56–100) | 98.48 (97.84–99.96) | 100 (94.56–100) | 96.97 (89.48–99.63) | 96.97 (89.48–99.63) | 95.45 (87.29–99.05) | 98.48 (91.84–99.96) | |
| : p-value | 1 | NA | 0.48 | |||||
| Accuracy | 94.59 (88.61–97.99) | 92.79 (86.29–96.84) | 98.2 (93.64–99.78) | 92.79 (86.29–96.84) | 95.5 (89.80–98.52) | 89.19 (81.88–94.29) | 93.69 (87.44–97.43) | |
| : p-value | 0.04 | 0.25 | 0.07 | |||||
| PPV | 100 (90.97–100) | 97.44 (86.52–99.94) | 100 (91.78–100) | 95.12 (83.47–99.4) | 95.45 (84.53–99.44) | 92.31 (79.13–98.38) | 97.5 (86.84–99.94) | |
| : p-value | 0.96 | 1 | 0.59 | |||||
| NPV | 91.67 (82.74–96.88) | 90.28 (80.99–96.0) | 97.06 (89.78–99.64) | 91.43 (82.27–96.79) | 95.52 (87.47–99.07) | 87.5 (77.59–94.12) | 91.55 (82.51–96.84) | |
| : p-value | 0.12 | 0.53 | 0.61 | |||||
| Readers | Reader 1 | Reader 2 | Reader 3 | |||
|---|---|---|---|---|---|---|
| −AI | +AI | −AI | +AI | −AI | +AI | |
| AI | 0.72 | 0.90 | 0.27 | 0.98 | 0.10 | 0.03 |
| Reader 1 − AI | - | 0.74 | 0.09 | 0.70 | 0.10 | 0.02 |
| Reader 1 + AI | - | 0.87 | 0.07 | 0.02 | ||
| Reader 2 − AI | - | 0.08 | 0.45 | 0.14 | ||
| Reader 2 + AI | - | 0.03 | 0.01 | |||
| Reader 3 − AI | - | 0.12 | ||||
| Reader 3 + AI | - | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.R.; Yoon, Y.S.; Cha, J.G. Opportunistic Screening for Acute Vertebral Fractures on a Routine Abdominal or Chest Computed Tomography Scans Using an Automated Deep Learning Model. Diagnostics 2024, 14, 781. https://doi.org/10.3390/diagnostics14070781
Kim YR, Yoon YS, Cha JG. Opportunistic Screening for Acute Vertebral Fractures on a Routine Abdominal or Chest Computed Tomography Scans Using an Automated Deep Learning Model. Diagnostics. 2024; 14(7):781. https://doi.org/10.3390/diagnostics14070781
Chicago/Turabian StyleKim, Ye Rin, Yu Sung Yoon, and Jang Gyu Cha. 2024. "Opportunistic Screening for Acute Vertebral Fractures on a Routine Abdominal or Chest Computed Tomography Scans Using an Automated Deep Learning Model" Diagnostics 14, no. 7: 781. https://doi.org/10.3390/diagnostics14070781
APA StyleKim, Y. R., Yoon, Y. S., & Cha, J. G. (2024). Opportunistic Screening for Acute Vertebral Fractures on a Routine Abdominal or Chest Computed Tomography Scans Using an Automated Deep Learning Model. Diagnostics, 14(7), 781. https://doi.org/10.3390/diagnostics14070781