
Cardiac SARS-CoV-2 Infection, Involvement of Cytokines in Postmortem Immunohistochemical Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
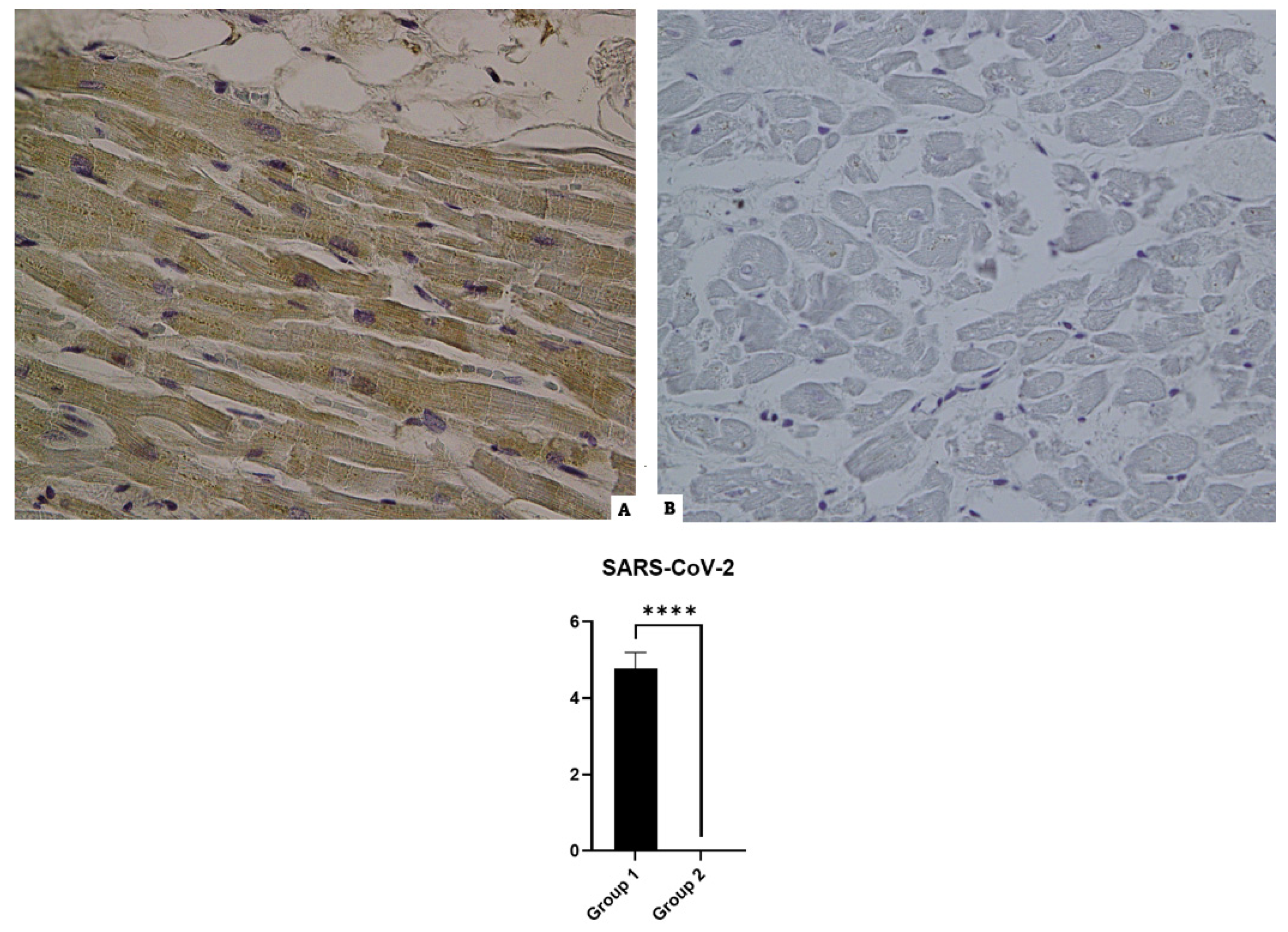
3.1. SARS-CoV-2 (Nucleocapsid)

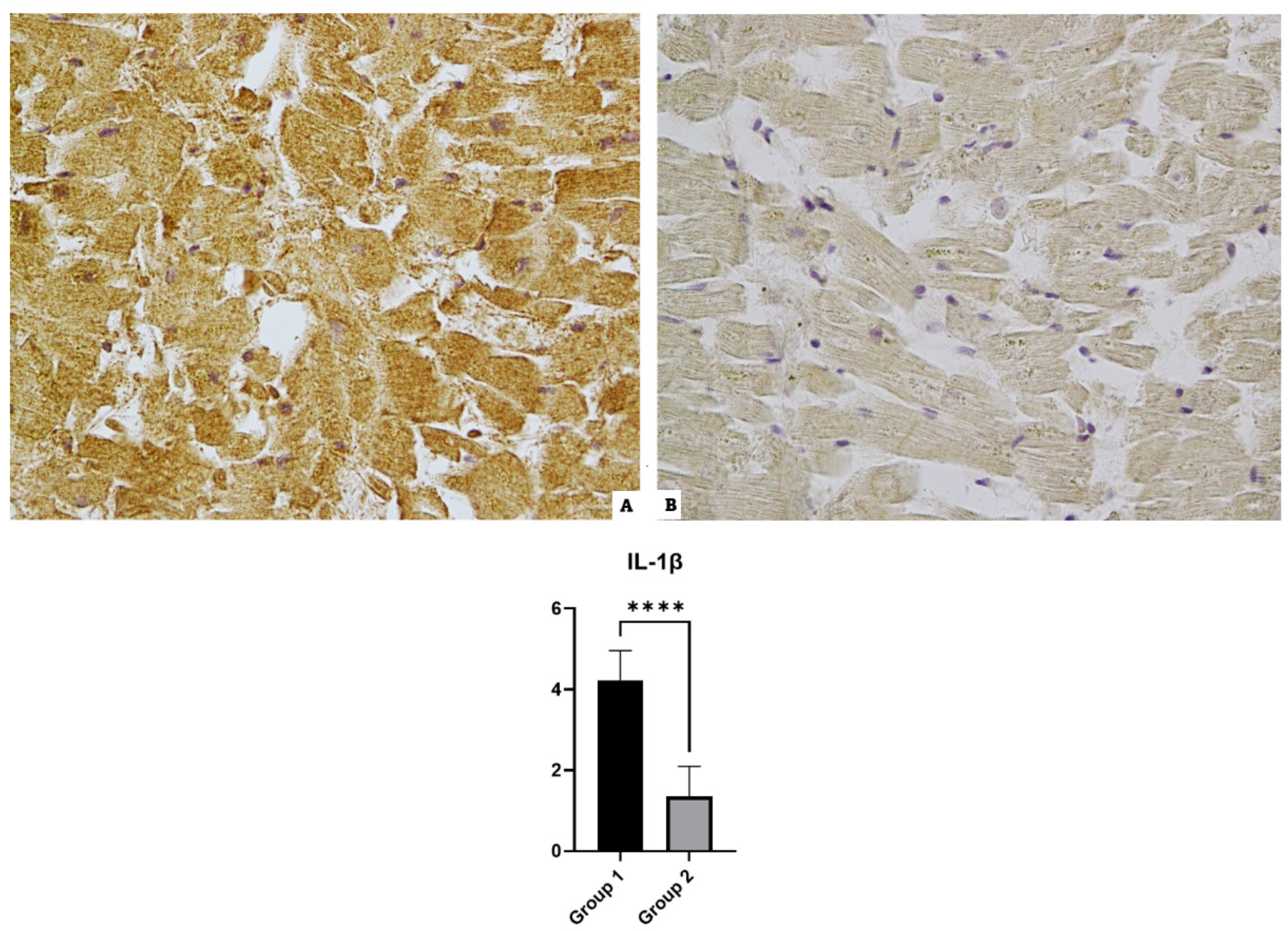
3.2. IL-1β

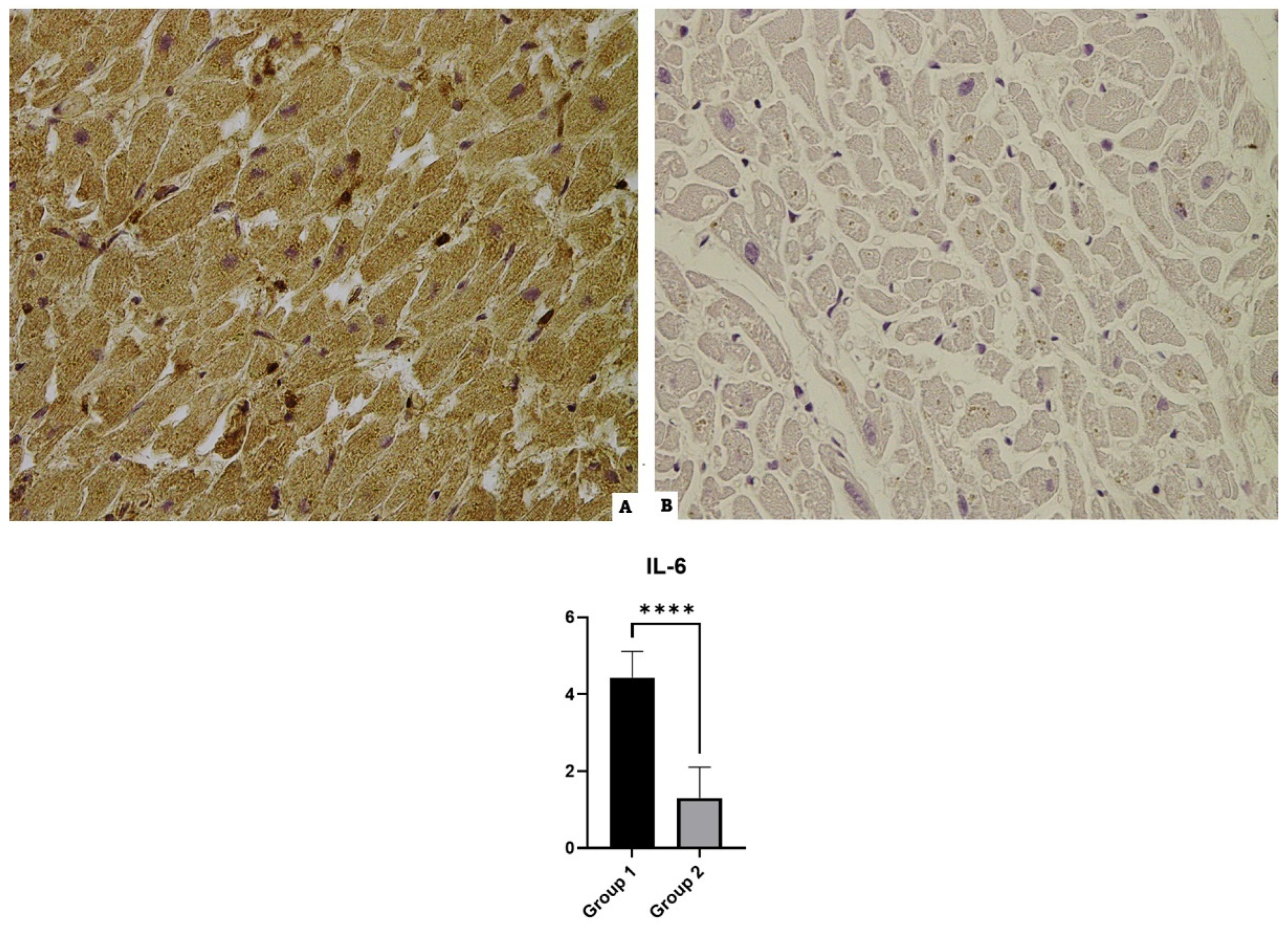
3.3. IL-6

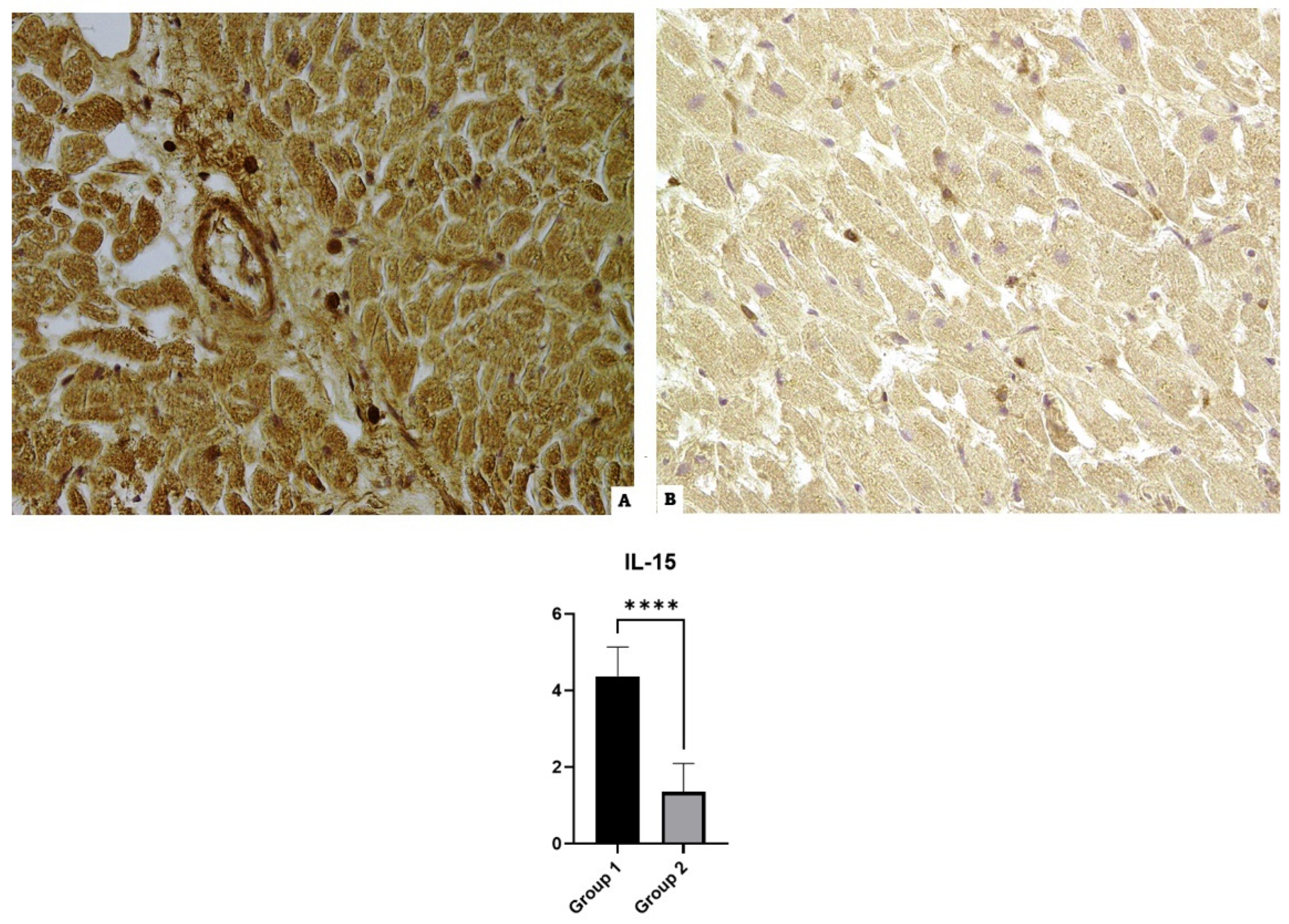
3.4. IL-15

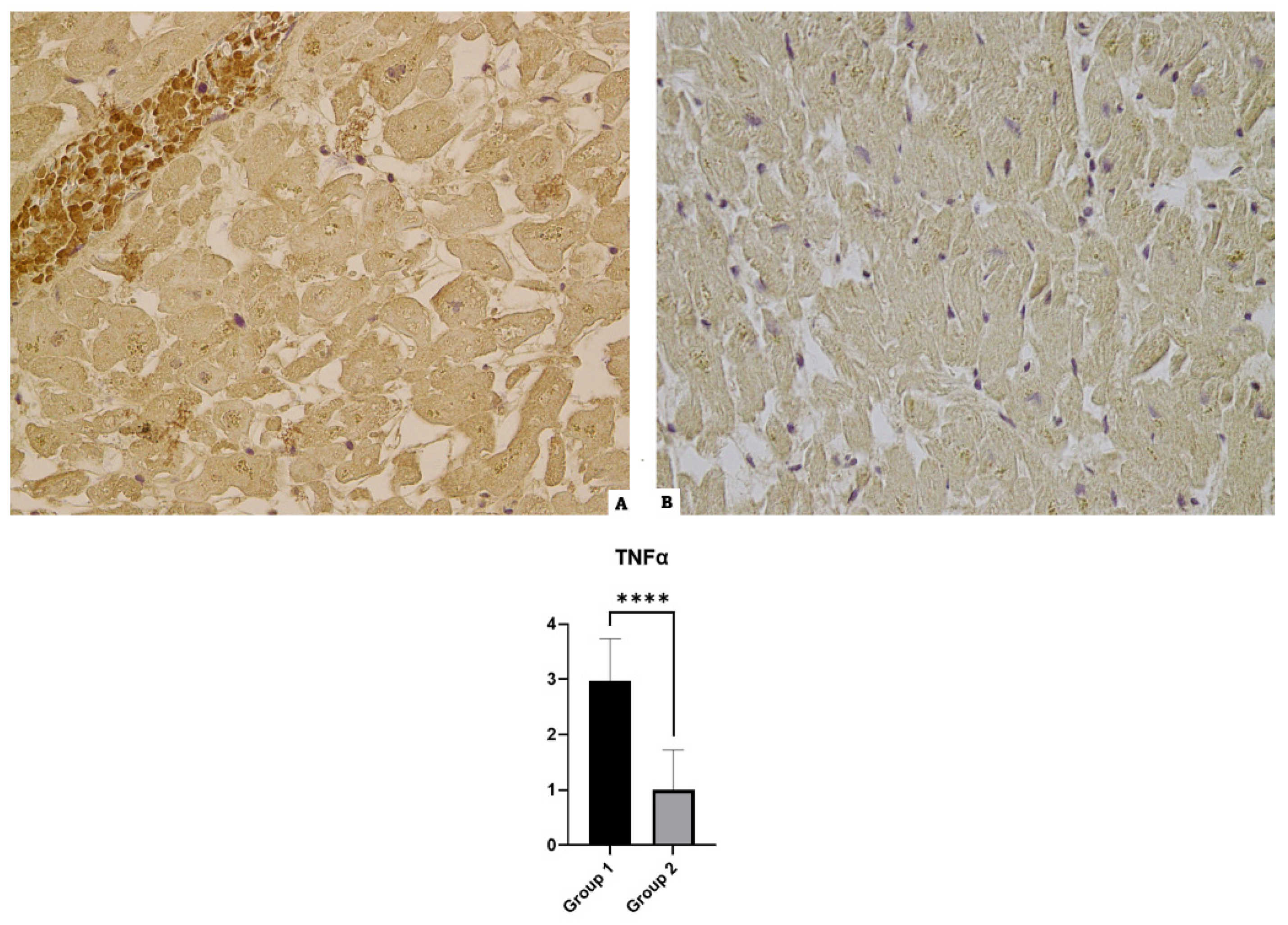
3.5. TNF-α

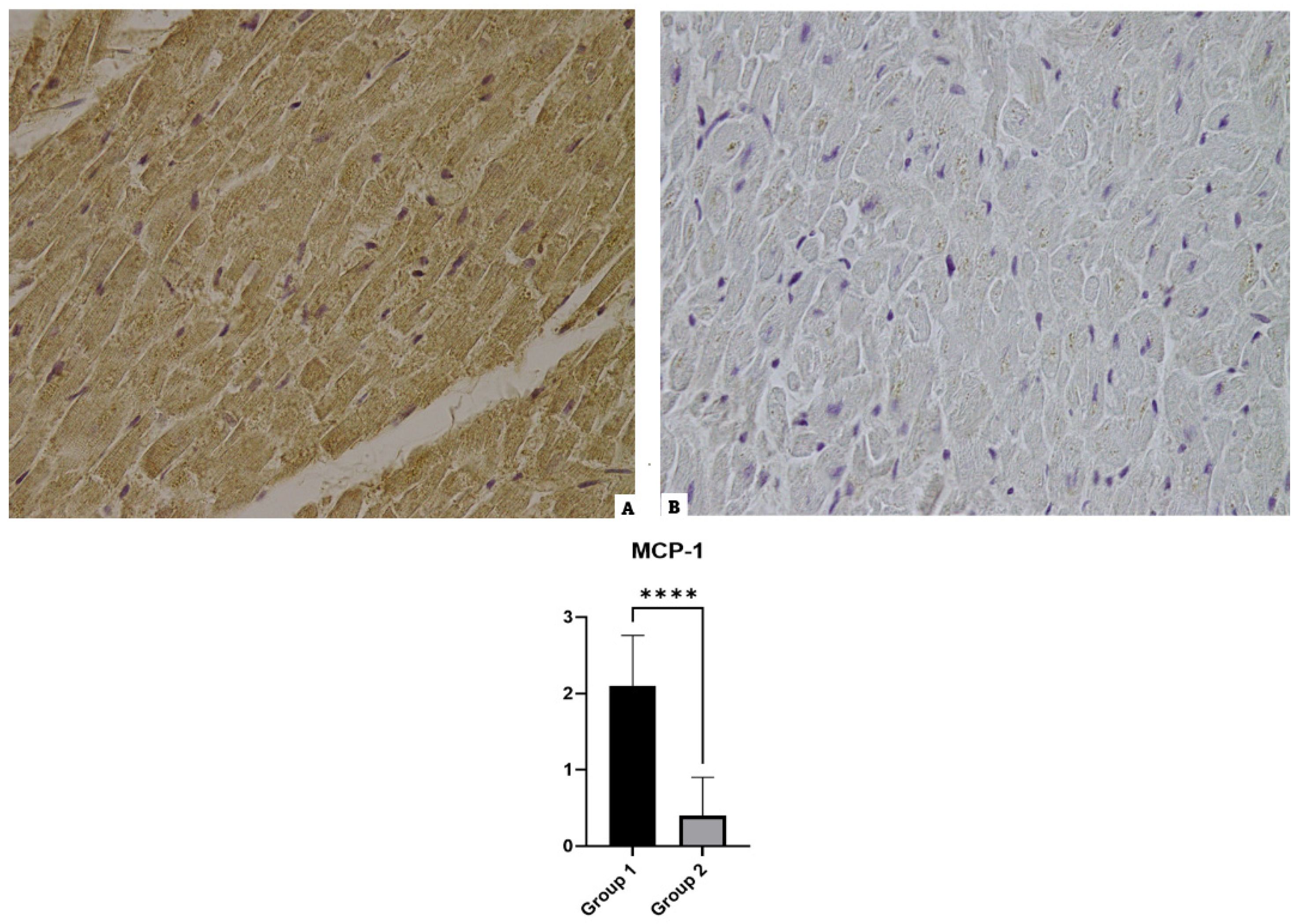
3.6. MCP-1

3.7. IL-10 and CD-45
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gupta, A.; Madhavan, M.V.; Sehgal, K.; Nair, N.; Mahajan, S.; Sehrawat, T.S.; Bikdeli, B.; Ahluwalia, N.; Ausiello, J.C.; Wan, E.Y.; et al. Extrapulmonary Manifestations of COVID-19. Nat. Med. 2020, 26, 1017–1032. [Google Scholar] [CrossRef] [PubMed]
- Nelwan, E.J.; Tunjungputri, R.N.; Tetrasiwi, E.N.; Lauditta, R.K.; Nainggolan, L. Extrapulmonary Manifestations COVID-19. Acta Medica Indones. 2022, 54, 314–315. [Google Scholar]
- Vosko, I.; Zirlik, A.; Bugger, H. Impact of COVID-19 on Cardiovascular Disease. Viruses 2023, 15, 508. [Google Scholar] [CrossRef] [PubMed]
- Atri, D.; Siddiqi, H.K.; Lang, J.P.; Nauffal, V.; Morrow, D.A.; Bohula, E.A. COVID-19 for the Cardiologist: Basic Virology, Epidemiology, Cardiac Manifestations, and Potential Therapeutic Strategies. JACC Basic Transl. Sci. 2020, 5, 518–536. [Google Scholar] [CrossRef]
- Inciardi, R.M.; Lupi, L.; Zaccone, G.; Italia, L.; Raffo, M.; Tomasoni, D.; Cani, D.S.; Cerini, M.; Farina, D.; Gavazzi, E.; et al. Cardiac Involvement in a Patient With Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 819–824. [Google Scholar] [CrossRef] [PubMed]
- AlSamman, M.; Caggiula, A.; Ganguli, S.; Misak, M.; Pourmand, A. Non-Respiratory Presentations of COVID-19, a Clinical Review. Am. J. Emerg. Med. 2020, 38, 2444–2454. [Google Scholar] [CrossRef] [PubMed]
- Babapoor-Farrokhran, S.; Gill, D.; Walker, J.; Rasekhi, R.T.; Bozorgnia, B.; Amanullah, A. Myocardial Injury and COVID-19: Possible Mechanisms. Life Sci. 2020, 253, 117723. [Google Scholar] [CrossRef] [PubMed]
- Shi, S.; Qin, M.; Shen, B.; Cai, Y.; Liu, T.; Yang, F.; Gong, W.; Liu, X.; Liang, J.; Zhao, Q.; et al. Association of Cardiac Injury with Mortality in Hospitalized Patients with COVID-19 in Wuhan, China. JAMA Cardiol. 2020, 5, 802–810. [Google Scholar] [CrossRef] [PubMed]
- Khalil, F.; Oleszak, F.; Stys, T.; Stys, A. COVID-19 and Cardiovascular Disease: A Comprehensive Review. South Dak. J. Med. 2022, 75, 54–60. [Google Scholar]
- Hamming, I.; Timens, W.; Bulthuis, M.L.C.; Lely, A.T.; Navis, G.J.; van Goor, H. Tissue Distribution of ACE2 Protein, the Functional Receptor for SARS Coronavirus. A First Step in Understanding SARS Pathogenesis. J. Pathol. 2004, 203, 631–637. [Google Scholar] [CrossRef]
- Frisoni, P.; Neri, M.; D’Errico, S.; Alfieri, L.; Bonuccelli, D.; Cingolani, M.; Di Paolo, M.; Gaudio, R.M.; Lestani, M.; Marti, M.; et al. Cytokine Storm and Histopathological Findings in 60 Cases of COVID-19-Related Death: From Viral Load Research to Immunohistochemical Quantification of Major Players IL-1β, IL-6, IL-15 and TNF-α. Forensic Sci. Med. Pathol. 2022, 18, 4–19. [Google Scholar] [CrossRef] [PubMed]
- Lindner, D.; Fitzek, A.; Bräuninger, H.; Aleshcheva, G.; Edler, C.; Meissner, K.; Scherschel, K.; Kirchhof, P.; Escher, F.; Schultheiss, H.-P.; et al. Association of Cardiac Infection With SARS-CoV-2 in Confirmed COVID-19 Autopsy Cases. JAMA Cardiol. 2020, 5, 1281–1285. [Google Scholar] [CrossRef]
- Violi, F.; Cangemi, R.; Calvieri, C. Pneumonia, Thrombosis and Vascular Disease. J. Thromb. Haemost. JTH 2014, 12, 1391–1400. [Google Scholar] [CrossRef] [PubMed]
- Tang, N.; Li, D.; Wang, X.; Sun, Z. Abnormal Coagulation Parameters Are Associated with Poor Prognosis in Patients with Novel Coronavirus Pneumonia. J. Thromb. Haemost. JTH 2020, 18, 844–847. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.; Wu, D.; Chen, H.; Yan, W.; Yang, D.; Chen, G.; Ma, K.; Xu, D.; Yu, H.; Wang, H.; et al. Clinical Characteristics of 113 Deceased Patients with Coronavirus Disease 2019: Retrospective Study. BMJ 2020, 368, m1091. [Google Scholar] [CrossRef]
- Wichmann, D.; Sperhake, J.-P.; Lütgehetmann, M.; Steurer, S.; Edler, C.; Heinemann, A.; Heinrich, F.; Mushumba, H.; Kniep, I.; Schröder, A.S.; et al. Autopsy Findings and Venous Thromboembolism in Patients With COVID-19: A Prospective Cohort Study. Ann. Intern. Med. 2020, 173, 268–277. [Google Scholar] [CrossRef]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial Cell Infection and Endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef]
- Bryce, C.; Grimes, Z.; Pujadas, E.; Ahuja, S.; Beasley, M.B.; Albrecht, R.; Hernandez, T.; Stock, A.; Zhao, Z.; AlRasheed, M.R.; et al. Pathophysiology of SARS-CoV-2: The Mount Sinai COVID-19 Autopsy Experience. Mod. Pathol. 2021, 34, 1456–1467. [Google Scholar] [CrossRef]
- Kuck, K.-H. Arrhythmias and Sudden Cardiac Death in the COVID-19 Pandemic. Herz 2020, 45, 325–326. [Google Scholar] [CrossRef]
- Beri, A.; Kotak, K. Cardiac Injury, Arrhythmia, and Sudden Death in a COVID-19 Patient. Hear. Case Rep. 2020, 6, 367–369. [Google Scholar] [CrossRef]
- Shirazi, S.; Mami, S.; Mohtadi, N.; Ghaysouri, A.; Tavan, H.; Nazari, A.; Kokhazadeh, T.; Mollazadeh, R. Sudden Cardiac Death in COVID-19 Patients, a Report of Three Cases. Future Cardiol. 2021, 17, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Bradley, B.T.; Maioli, H.; Johnston, R.; Chaudhry, I.; Fink, S.L.; Xu, H.; Najafian, B.; Deutsch, G.; Lacy, J.M.; Williams, T.; et al. Histopathology and Ultrastructural Findings of Fatal COVID-19 Infections in Washington State: A Case Series. Lancet 2020, 396, 320–332. [Google Scholar] [CrossRef]
- Werlein, C.; Ackermann, M.; Stark, H.; Shah, H.R.; Tzankov, A.; Haslbauer, J.D.; von Stillfried, S.; Bülow, R.D.; El-Armouche, A.; Kuenzel, S.; et al. Inflammation and Vascular Remodeling in COVID-19 Hearts. Angiogenesis 2023, 26, 233–248. [Google Scholar] [CrossRef]
- Jiang, Z.; Wu, L.; van der Leeden, B.; van Rossum, A.C.; Niessen, H.W.M.; Krijnen, P.A.J. NOX2 and NOX5 Are Increased in Cardiac Microvascular Endothelium of Deceased COVID-19 Patients. Int. J. Cardiol. 2023, 370, 454–462. [Google Scholar] [CrossRef] [PubMed]
- Puzyrenko, A.; Jacobs, E.R.; Padilla, N.; Devine, A.; Aljadah, M.; Gantner, B.N.; Pan, A.Y.; Lai, S.; Dai, Q.; Rubenstein, J.C.; et al. Collagen-Specific HSP47(+) Myofibroblasts and CD163(+) Macrophages Identify Profibrotic Phenotypes in Deceased Hearts with SARS-CoV-2 Infections. J. Am. Heart Assoc. 2023, 12, e027990. [Google Scholar] [CrossRef]
- Hartmann, C.; Miggiolaro, A.F.R.D.S.; Motta, J.d.S.; Baena Carstens, L.; Busatta Vaz De Paula, C.; Fagundes Grobe, S.; Hermann de Souza Nunes, L.; Lenci Marques, G.; Libby, P.; Zytynski Moura, L.; et al. The Pathogenesis of COVID-19 Myocardial Injury: An Immunohistochemical Study of Postmortem Biopsies. Front. Immunol. 2021, 12, 748417. [Google Scholar] [CrossRef]
- Hendren, N.S.; Drazner, M.H.; Bozkurt, B.; Cooper, L.T.J. Description and Proposed Management of the Acute COVID-19 Cardiovascular Syndrome. Circulation 2020, 141, 1903–1914. [Google Scholar] [CrossRef]
- Wong, D.W.L.; Klinkhammer, B.M.; Djudjaj, S.; Villwock, S.; Timm, M.C.; Buhl, E.M.; Wucherpfennig, S.; Cacchi, C.; Braunschweig, T.; Knüchel-Clarke, R.; et al. Multisystemic Cellular Tropism of SARS-CoV-2 in Autopsies of COVID-19 Patients. Cells 2021, 10, 1900. [Google Scholar] [CrossRef]
- Mezache, L.; Nuovo, G.J.; Suster, D.; Tili, E.; Awad, H.; Radwański, P.B.; Veeraraghavan, R. Histologic, Viral, and Molecular Correlates of Heart Disease in Fatal COVID-19. Ann. Diagn. Pathol. 2022, 60, 151983. [Google Scholar] [CrossRef]
- Tavazzi, G.; Pellegrini, C.; Maurelli, M.; Belliato, M.; Sciutti, F.; Bottazzi, A.; Sepe, P.A.; Resasco, T.; Camporotondo, R.; Bruno, R.; et al. Myocardial Localization of Coronavirus in COVID-19 Cardiogenic Shock. Eur. J. Heart Fail. 2020, 22, 911–915. [Google Scholar] [CrossRef]
- Remmelink, M.; De Mendonça, R.; D’Haene, N.; De Clercq, S.; Verocq, C.; Lebrun, L.; Lavis, P.; Racu, M.-L.; Trépant, A.-L.; Maris, C.; et al. Unspecific Post-Mortem Findings despite Multiorgan Viral Spread in COVID-19 Patients. Crit. Care 2020, 24, 495. [Google Scholar] [CrossRef] [PubMed]
- Skok, K.; Stelzl, E.; Trauner, M.; Kessler, H.H.; Lax, S.F. Post-Mortem Viral Dynamics and Tropism in COVID-19 Patients in Correlation with Organ Damage. Virchows Arch. Int. J. Pathol. 2021, 478, 343–353. [Google Scholar] [CrossRef] [PubMed]
- Massoth, L.R.; Desai, N.; Szabolcs, A.; Harris, C.K.; Neyaz, A.; Crotty, R.; Chebib, I.; Rivera, M.N.; Sholl, L.M.; Stone, J.R.; et al. Comparison of RNA In Situ Hybridization and Immunohistochemistry Techniques for the Detection and Localization of SARS-CoV-2 in Human Tissues. Am. J. Surg. Pathol. 2021, 45, 14–24. [Google Scholar] [CrossRef] [PubMed]
- Hua, A.; O’Gallagher, K.; Sado, D.; Byrne, J. Life-Threatening Cardiac Tamponade Complicating Myo-Pericarditis in COVID-19. Eur. Heart J. 2020, 41, 2130. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.; Ma, F.; Wei, X.; Fang, Y. Coronavirus Fulminant Myocarditis Treated with Glucocorticoid and Human Immunoglobulin. Eur. Heart J. 2021, 42, 206. [Google Scholar] [CrossRef]
- Kim, I.-C.; Kim, J.Y.; Kim, H.A.; Han, S. COVID-19-Related Myocarditis in a 21-Year-Old Female Patient. Eur. Heart J. 2020, 41, 1859. [Google Scholar] [CrossRef] [PubMed]
- Zeng, J.-H.; Liu, Y.-X.; Yuan, J.; Wang, F.-X.; Wu, W.-B.; Li, J.-X.; Wang, L.-F.; Gao, H.; Wang, Y.; Dong, C.-F.; et al. First Case of COVID-19 Complicated with Fulminant Myocarditis: A Case Report and Insights. Infection 2020, 48, 773–777. [Google Scholar] [CrossRef] [PubMed]
- Woudstra, L.; Biesbroek, P.S.; Emmens, R.W.; Heymans, S.; Juffermans, L.J.; van der Wal, A.C.; van Rossum, A.C.; Niessen, H.W.M.; Krijnen, P.A.J. CD45 Is a More Sensitive Marker than CD3 to Diagnose Lymphocytic Myocarditis in the Endomyocardium. Hum. Pathol. 2017, 62, 83–90. [Google Scholar] [CrossRef]
- Van Linthout, S.; Klingel, K.; Tschöpe, C. SARS-CoV-2-Related Myocarditis-like Syndromes Shakespeare’s Question: What’s in a Name? Eur. J. Heart Fail. 2020, 22, 922–925. [Google Scholar] [CrossRef]
- Fox, S.E.; Li, G.; Akmatbekov, A.; Harbert, J.L.; Lameira, F.S.; Brown, J.Q.; Vander Heide, R.S. Unexpected Features of Cardiac Pathology in COVID-19 Infection. Circulation 2020, 142, 1123–1125. [Google Scholar] [CrossRef]
- Dal Ferro, M.; Bussani, R.; Paldino, A.; Nuzzi, V.; Collesi, C.; Zentilin, L.; Schneider, E.; Correa, R.; Silvestri, F.; Zacchigna, S.; et al. SARS-CoV-2, Myocardial Injury and Inflammation: Insights from a Large Clinical and Autopsy Study. Clin. Res. Cardiol. Off. J. Ger. Card. Soc. 2021, 110, 1822–1831. [Google Scholar] [CrossRef]
- Rocha Rodrigues, D.B.; dos Reis, M.A.; Romano, A.; Pereira, S.A.d.L.; Teixeira, V.d.P.A.; Tostes, S.J.; Rodrigues, V.J. In Situ Expression of Regulatory Cytokines by Heart Inflammatory Cells in Chagas’ Disease Patients with Heart Failure. Clin. Dev. Immunol. 2012, 2012, 361730. [Google Scholar] [CrossRef]
- Bezerra, O.C.; França, C.M.; Rocha, J.A.; Neves, G.A.; Souza, P.R.M.; Teixeira Gomes, M.; Malfitano, C.; Loleiro, T.C.A.; Dourado, P.M.; Llesuy, S.; et al. Cholinergic Stimulation Improves Oxidative Stress and Inflammation in Experimental Myocardial Infarction. Sci. Rep. 2017, 7, 13687. [Google Scholar] [CrossRef]
- Sharma, H.S.; Das, D.K. Role of Cytokines in Myocardial Ischemia and Reperfusion. Mediat. Inflamm. 1997, 6, 175–183. [Google Scholar] [CrossRef]
- De Rosa, S.; Spaccarotella, C.; Basso, C.; Calabrò, M.P.; Curcio, A.; Filardi, P.P.; Mancone, M.; Mercuro, G.; Muscoli, S.; Nodari, S.; et al. Reduction of Hospitalizations for Myocardial Infarction in Italy in the COVID-19 Era. Eur. Heart J. 2020, 41, 2083–2088. [Google Scholar] [CrossRef]
- Stefanini, G.G.; Montorfano, M.; Trabattoni, D.; Andreini, D.; Ferrante, G.; Ancona, M.; Metra, M.; Curello, S.; Maffeo, D.; Pero, G.; et al. ST-Elevation Myocardial Infarction in Patients With COVID-19: Clinical and Angiographic Outcomes. Circulation 2020, 141, 2113–2116. [Google Scholar] [CrossRef]
- Parisi, S.G.; Viel, G.; Cecchi, R.; Montisci, M. COVID-19: The Wrong Target for Healthcare Liability Claims. Leg. Med. 2020, 46, 101718. [Google Scholar] [CrossRef]
- Hanson, P.J.; Liu-Fei, F.; Ng, C.; Minato, T.A.; Lai, C.; Hossain, A.R.; Chan, R.; Grewal, B.; Singhera, G.; Rai, H.; et al. Characterization of COVID-19-Associated Cardiac Injury: Evidence for a Multifactorial Disease in an Autopsy Cohort. Lab. Investig. J. Tech. Methods Pathol. 2022, 102, 814–825. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics and Clinical Characteristics of SARS-CoV-2 Cases: Group 1 | |||
|---|---|---|---|
| Gender Male | Number of Cases 30 | ||
| Age | 60–70 Years 10 | 71–80 Years 10 | 81–85 Years 10 |
| Diabetes Mellitus | 2 | 5 | 7 |
| Chronic Kidney disease | 0 | 2 | 5 |
| No comorbidity known | 3 | 0 | 0 |
| Overweight | 5 | 4 | 2 |
| Arterial Hypertension | 3 | 10 | 10 |
| Antibody | Producer | Ab Dilution | Pretreatment | Incubation |
|---|---|---|---|---|
| Anti-IL-1β | Santa Cruz Biotechnology, Inc.® | 1:200 | HIER 0.1 M citrate buffer | 2 h, 20 °C |
| Anti-IL-6 | Santa Cruz Biotechnology, Inc.® | 1:500 | Proteinase K, 15 min. at 20 °C | 2 h, 20 °C |
| Anti-IL-10 | Santa Cruz Biotechnology, Inc.® | 1:50 | Proteinase K, 15 min. at 20 °C | 2 h, 20 °C |
| Anti-IL-15 | Santa Cruz Biotechnology, Inc.® | 1:50 | HIER 0.25 mM EDTA buffer | 2 h, 20 °C |
| Anti-TNF-α | Santa Cruz Biotechnology, Inc.® | 1:500 | HIER 0.1 M citrate buffer | 2 h, 20 °C |
| Anti-MCP-1 | Santa Cruz Biotechnology, Inc.® | 1:50 | HIER 0.25 mM EDTA buffer | 2 h, 20 °C |
| Anti-CD45 | Santa Cruz Biotechnology, Inc.® | 1:500 | HIER 0.25 mM EDTA buffer | 2 h, 20 °C |
| Anti-SARS-CoV-2 | Santa Cruz Biotechnology, Inc.® | 1:100 | HIER 0.25 mM EDTA buffer | Overnight, 20 °C |
| Antibody | COVID-19 Cases Group 1 | Control Cases Group 2 | Statistical Significance Group 1 vs. Group 2 |
|---|---|---|---|
| SARS-CoV-2 | ++++ | − | **** (p < 0.0001) |
| IL-1β | +++ | +/− | **** (p < 0.0001) |
| IL-6 | ++++ | +/− | **** (p < 0.0001) |
| IL-10 | +/− | − | NS (p > 0.05) |
| IL-15 | ++++ | +/− | **** (p < 0.0001) |
| TNF-α | +++ | +/− | **** (p < 0.0001) |
| MCP-1 | ++ | +/− | **** (p < 0.0001) |
| CD45 | + | +/− | NS (p > 0.05) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alfieri, L.; Franceschetti, L.; Frisoni, P.; Bonato, O.; Radaelli, D.; Bonuccelli, D.; D’Errico, S.; Neri, M. Cardiac SARS-CoV-2 Infection, Involvement of Cytokines in Postmortem Immunohistochemical Study. Diagnostics 2024, 14, 787. https://doi.org/10.3390/diagnostics14080787
Alfieri L, Franceschetti L, Frisoni P, Bonato O, Radaelli D, Bonuccelli D, D’Errico S, Neri M. Cardiac SARS-CoV-2 Infection, Involvement of Cytokines in Postmortem Immunohistochemical Study. Diagnostics. 2024; 14(8):787. https://doi.org/10.3390/diagnostics14080787
Chicago/Turabian StyleAlfieri, Letizia, Lorenzo Franceschetti, Paolo Frisoni, Omar Bonato, Davide Radaelli, Diana Bonuccelli, Stefano D’Errico, and Margherita Neri. 2024. "Cardiac SARS-CoV-2 Infection, Involvement of Cytokines in Postmortem Immunohistochemical Study" Diagnostics 14, no. 8: 787. https://doi.org/10.3390/diagnostics14080787