
Discrepancies in Splenic Size Measurement: A Comparative Analysis of Ultrasound and Computed Tomography

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
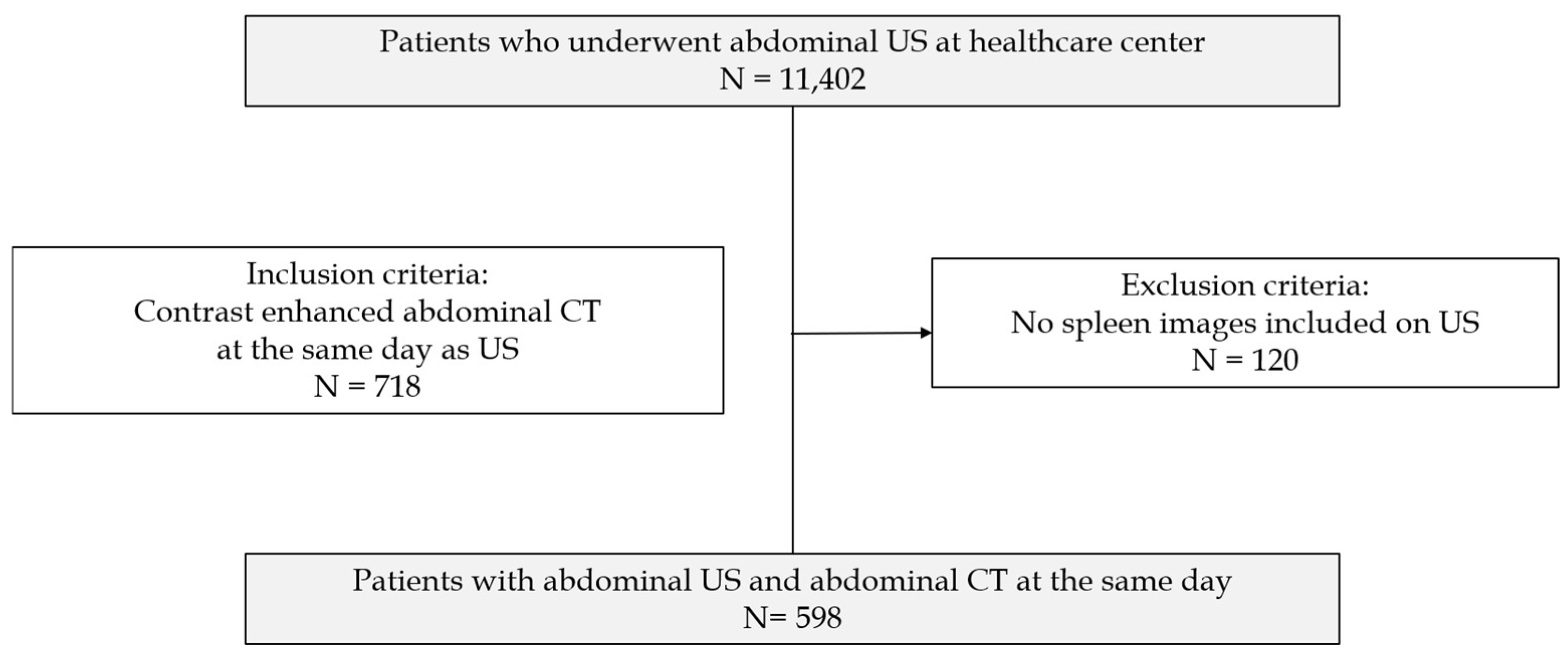
2.1. Study Population and Data Collection
2.2. Ultrasound (US) Examinations
2.3. Computed Tomography (CT) Examinations
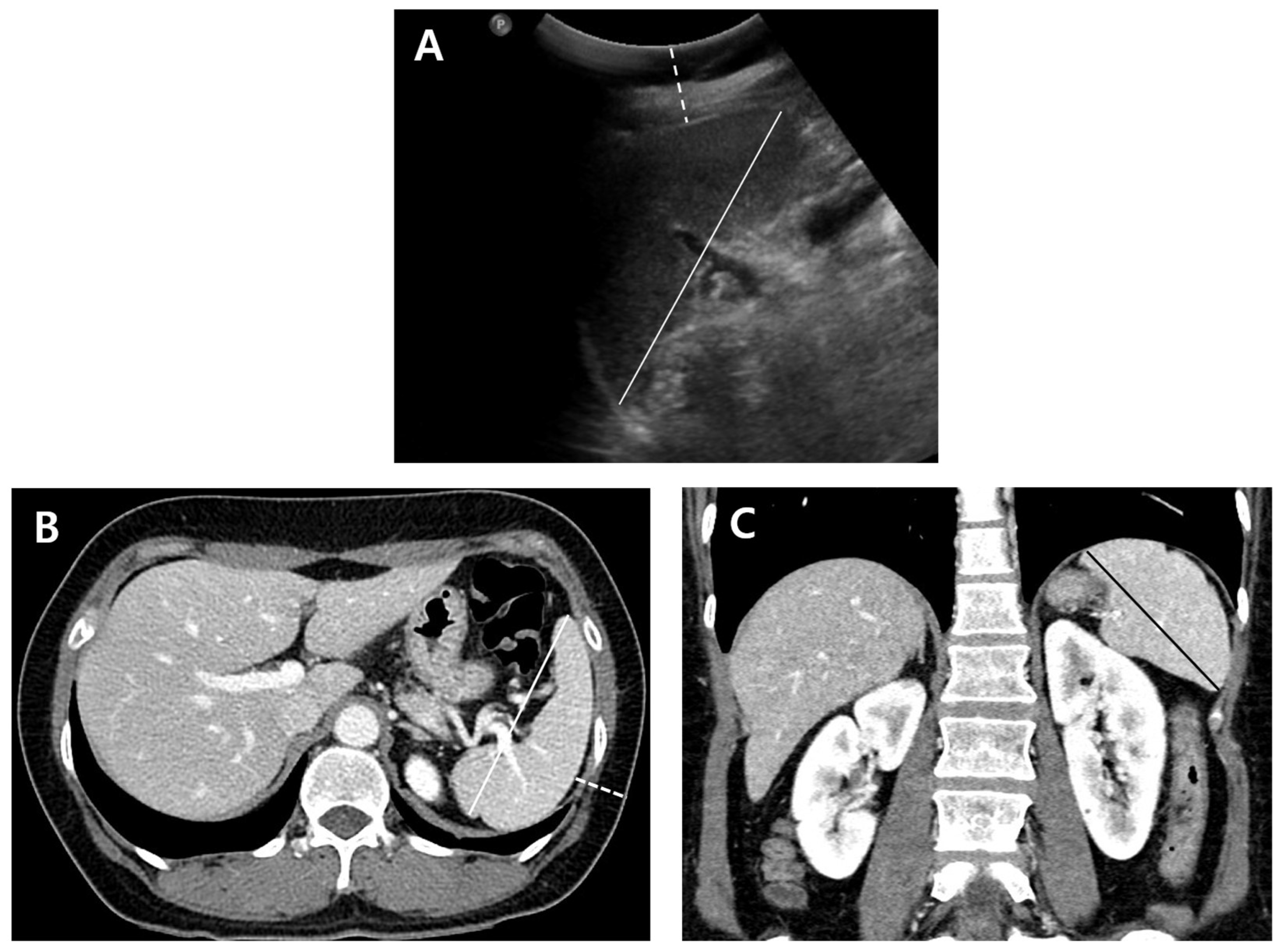
2.4. Image Analysis
2.5. Evaluation of Factors That Affect the Spleen Measurement Discrepancies
2.6. Statistical Analysis
3. Results
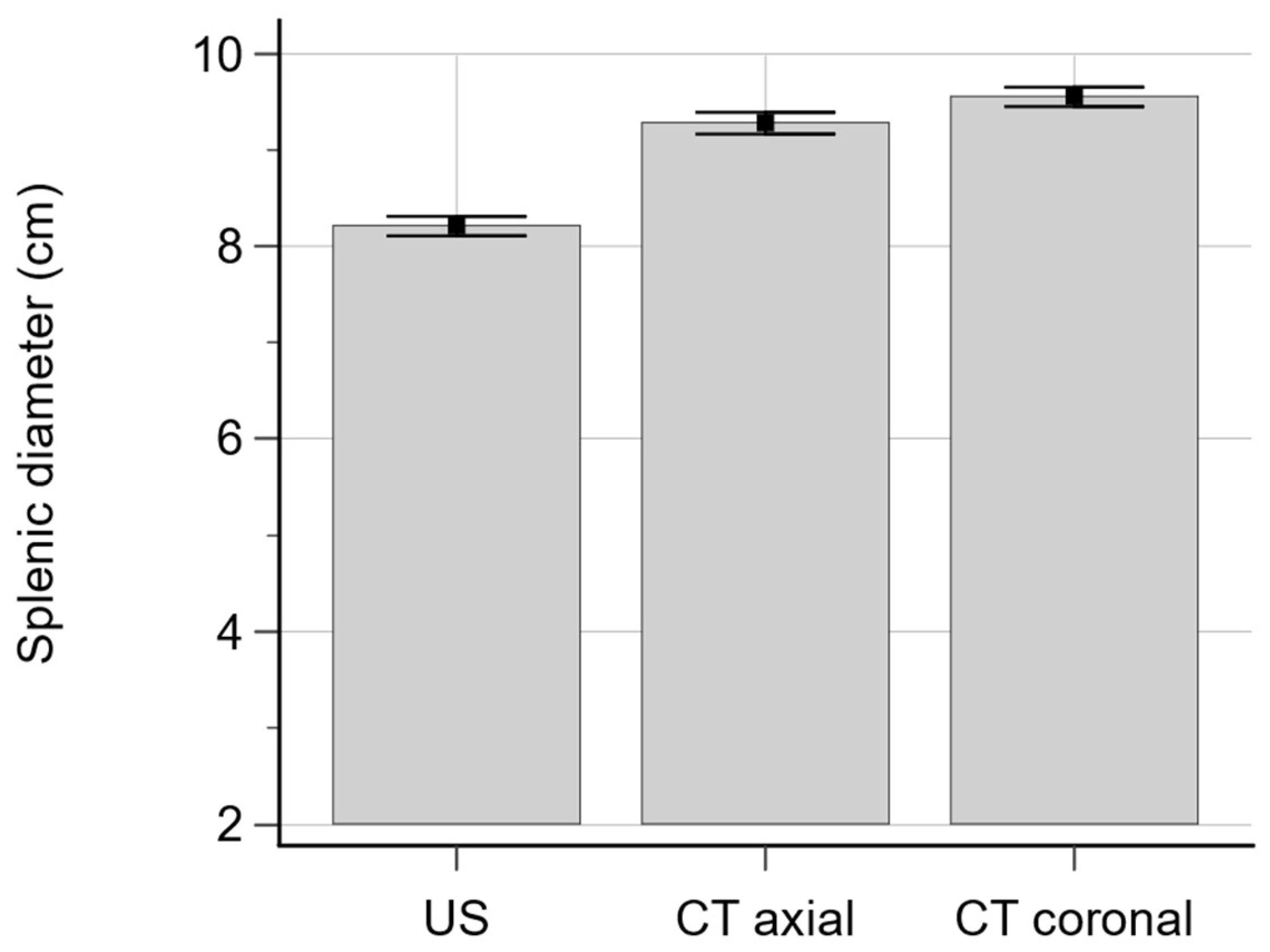
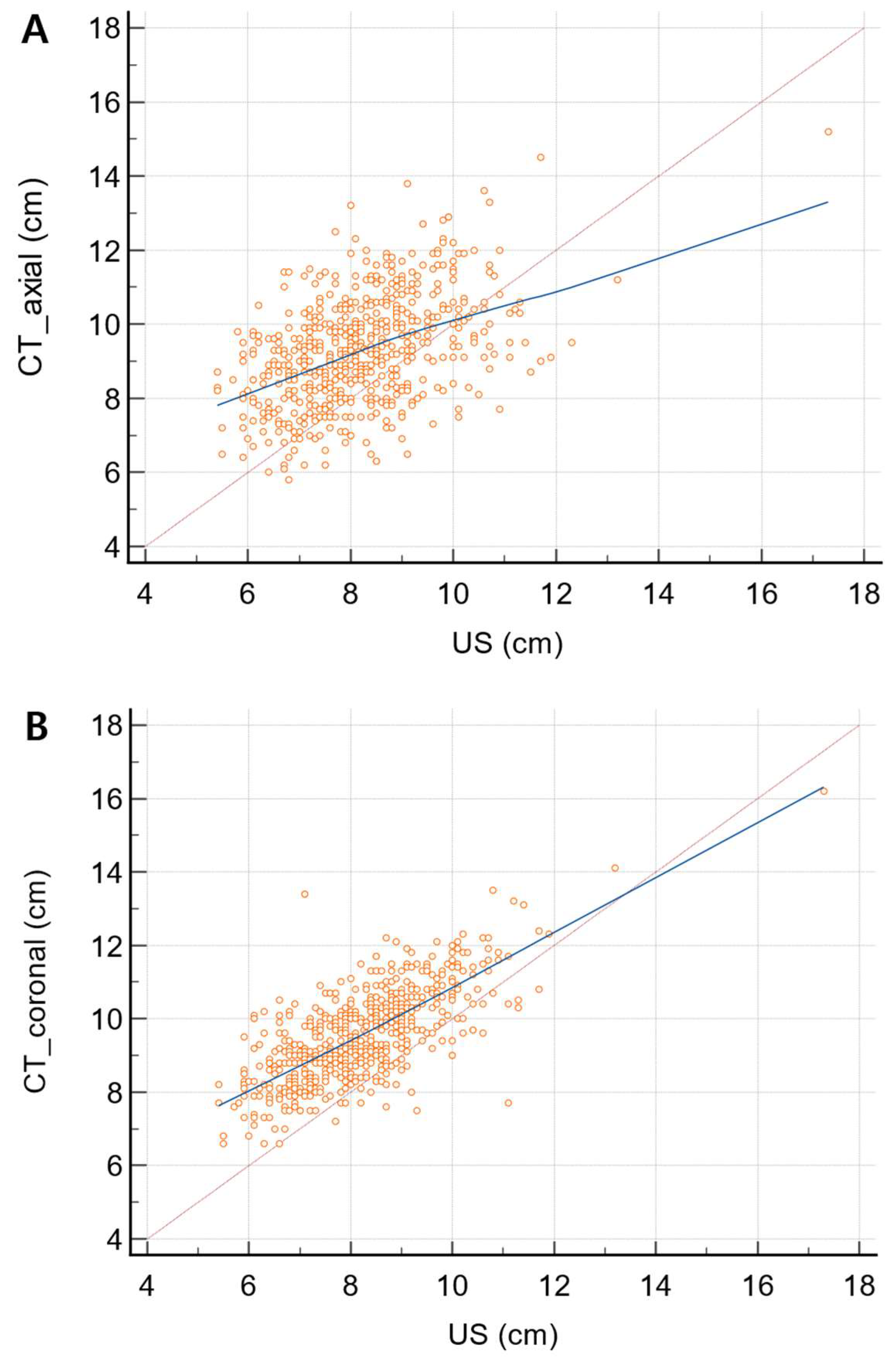
3.1. Comparison and Correlation of Spleen Diameter Measurements between US and CT
3.2. Association of Measurement Discrepancies with Clinical and Imaging Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| US | ultrasound |
| CT | computed tomography |
| BMI | body mass index |
| MRI | magnetic resonance imaging |
| CTax | axial CT scan |
| CTcor | coronal CT scan |
| ICC | intraclass correlation coefficient |
References
- Lamb, P.M.; Lund, A.; Kanagasabay, R.R.; Martin, A.; Webb, J.A.; Reznek, R.H. Spleen size: How well do linear ultrasound measurements correlate with three-dimensional CT volume assessments? Br. J. Radiol. 2002, 75, 573–577. [Google Scholar] [CrossRef] [PubMed]
- Badran, D.H.; Kalbouneh, H.M.; Al-Hadidi, M.T.; Shatarat, A.T.; Tarawneh, E.S.; Hadidy, A.M.; Mahafza, W.S. Ultrasonographic assessment of splenic volume and its correlation with body parameters in a Jordanian population. Saudi Med. J. 2015, 36, 967–972. [Google Scholar] [CrossRef] [PubMed]
- Niederau, C.; Sonnenberg, A.; Muller, J.E.; Erckenbrecht, J.F.; Scholten, T.; Fritsch, W.P. Sonographic measurements of the normal liver, spleen, pancreas, and portal vein. Radiology 1983, 149, 537–540. [Google Scholar] [CrossRef] [PubMed]
- Castagnoli, F.; Doran, S.; Lunn, J.; Minchom, A.; O’Brien, M.; Popat, S.; Messiou, C.; Koh, D.M. Splenic volume as a predictor of treatment response in patients with non-small cell lung cancer receiving immunotherapy. PLoS ONE 2022, 17, e0270950. [Google Scholar] [CrossRef]
- Aslan, V.; Karabork Kilic, A.C.; Ozet, A.; Uner, A.; Gunel, N.; Yazici, O.; Savas, G.; Bayrak, A.; Eraslan, E.; Oksuzoglu, B.; et al. The role of spleen volume change in predicting immunotherapy response in metastatic renal cell carcinoma. BMC Cancer 2023, 23, 1045. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, A.J., Jr.; Rodrigues, C.J.; Germano, M.A.; Rasera Junior, I.; Cerri, G.G. Sonographic assessment of normal spleen volume. Clin. Anat. 1995, 8, 252–255. [Google Scholar] [CrossRef] [PubMed]
- Ishibashi, H.; Higuchi, N.; Shimamura, R.; Hirata, Y.; Kudo, J.; Niho, Y. Sonographic assessment and grading of spleen size. J. Clin. Ultrasound 1991, 19, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Loftus, W.K.; Chow, L.T.; Metreweli, C. Sonographic measurement of splenic length: Correlation with measurement at autopsy. J. Clin. Ultrasound 1999, 27, 71–74. [Google Scholar] [CrossRef]
- Konus, O.L.; Ozdemir, A.; Akkaya, A.; Erbas, G.; Celik, H.; Isik, S. Normal liver, spleen, and kidney dimensions in neonates, infants, and children: Evaluation with sonography. Am. J. Roentgenol. 1998, 171, 1693–1698. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, H.K.; Markowitz, R.I.; Kolberg, H.; Park, C.; Hubbard, A.; Bellah, R.D. Normal splenic size in infants and children: Sonographic measurements. Am. J. Roentgenol. 1991, 157, 119–121. [Google Scholar] [CrossRef]
- Downey, M.T. Estimation of splenic weight from ultrasonographic measurements. Can. Assoc. Radiol. J. 1992, 43, 273–277. [Google Scholar] [PubMed]
- Schlesinger, A.E.; Hildebolt, C.F.; Siegel, M.J.; Pilgrim, T.K. Splenic volume in children: Simplified estimation at CT. Radiology 1994, 193, 578–580. [Google Scholar] [CrossRef] [PubMed]
- Breiman, R.S.; Beck, J.W.; Korobkin, M.; Glenny, R.; Akwari, O.E.; Heaston, D.K.; Moore, A.V.; Ram, P.C. Volume determinations using computed tomography. Am. J. Roentgenol. 1982, 138, 329–333. [Google Scholar] [CrossRef] [PubMed]
- Prassopoulos, P.; Cavouras, D. CT assessment of normal splenic size in children. Acta Radiol. 1994, 35, 152–154. [Google Scholar] [CrossRef] [PubMed]
- Strijk, S.P.; Wagener, D.J.; Bogman, M.J.; de Pauw, B.E.; Wobbes, T. The spleen in Hodgkin disease: Diagnostic value of CT. Radiology 1985, 154, 753–757. [Google Scholar] [CrossRef] [PubMed]
- Prassopoulos, P.; Daskalogiannaki, M.; Raissaki, M.; Hatjidakis, A.; Gourtsoyiannis, N. Determination of normal splenic volume on computed tomography in relation to age, gender and body habitus. Eur. Radiol. 1997, 7, 246–248. [Google Scholar] [CrossRef]
- Sandrasegaran, K.; Kwo, P.W.; DiGirolamo, D.; Stockberger, S.M., Jr.; Cummings, O.W.; Kopecky, K.K. Measurement of liver volume using spiral CT and the curved line and cubic spline algorithms: Reproducibility and interobserver variation. Abdom. Imaging 1999, 24, 61–65. [Google Scholar] [CrossRef] [PubMed]
- Henderson, J.M.; Heymsfield, S.B.; Horowitz, J.; Kutner, M.H. Measurement of liver and spleen volume by computed tomography. Assessment of reproducibility and changes found following a selective distal splenorenal shunt. Radiology 1981, 141, 525–527. [Google Scholar] [CrossRef]
- Cools, L.; Osteaux, M.; Divano, L.; Jeanmart, L. Prediction of splenic volume by a simple CT measurement: A statistical study. J. Comput. Assist. Tomogr. 1983, 7, 426–430. [Google Scholar] [CrossRef]
- Mohammed, W.; Ismail, N.; Zidan, M.; Elgyoum, A.; Hassan, H.; Abdelrahman, O. Estimation of Spleen Volume Using MRI Segmentation: Would One Slice Be Enough? Cureus 2022, 14, e32165. [Google Scholar] [CrossRef]
- Chen, X.L.; Chen, T.W.; Li, Z.L.; Zhang, X.M.; Chen, N.; Zeng, N.L.; Li, H.; Tang, H.J.; Pu, Y.; Li, C.P. Spleen size measured on enhanced MRI for quantitatively staging liver fibrosis in minipigs. J. Magn. Reson. Imaging 2013, 38, 540–547. [Google Scholar] [CrossRef] [PubMed]
- Silverman, S.; DeNardo, G.L.; Siegel, E. Determination of spleen size by scintigraphy. Cancer Biother. Radiopharm. 1999, 14, 407–411. [Google Scholar] [CrossRef] [PubMed]
- Strauss, L.G.; Clorius, J.H.; Frank, T.; van Kaick, G. Single photon emission computerized tomography (SPECT) for estimates of liver and spleen volume. J. Nucl. Med. 1984, 25, 81–85. [Google Scholar] [PubMed]
- Markisz, J.A.; Treves, S.T.; Davis, R.T. Normal hepatic and splenic size in children: Scintigraphic determination. Pediatr. Radiol. 1987, 17, 273–276. [Google Scholar] [CrossRef] [PubMed]
- Yetter, E.M.; Acosta, K.B.; Olson, M.C.; Blundell, K. Estimating splenic volume: Sonographic measurements correlated with helical CT determination. Am. J. Roentgenol. 2003, 181, 1615–1620. [Google Scholar] [CrossRef] [PubMed]
- Morozov, S.V.; Izranov, V.A. Methods of Ultrasound Spleen Morphometry. J. Ultrasound Med. 2022, 41, 2123–2133. [Google Scholar] [CrossRef] [PubMed]
- Fateh, S.M.; Mohammed, N.A.; Mahmood, K.A.; Hasan Alpha, H.; Tahir, S.H.; Kakamad, F.H.; Salih, A.M.; Abdullah, H.O.; Abdalla, B.A.; Mohammed, S.H.; et al. Sonographic measurement of splenic size and its correlation with body parameters. Med Int. 2023, 3, 7. [Google Scholar] [CrossRef]
- Eze, C.U.; Agwu, K.K.; Ezeasor, D.N.; Ochie, K.; Aronu, A.E.; Agwuna, K.K.; Nwadike, I.U. Sonographic biometry of spleen among school age children in Nsukka, Southeast, Nigeria. Afr. Health Sci. 2013, 13, 384–392. [Google Scholar] [CrossRef] [PubMed]
- Maymon, R.; Strauss, S.; Vaknin, Z.; Weinraub, Z.; Herman, A.; Gayer, G. Normal sonographic values of maternal spleen size throughout pregnancy. Ultrasound Med. Biol. 2006, 32, 1827–1831. [Google Scholar] [CrossRef]
- Sonmez, G.; Ozturk, E.; Basekim, C.C.; Mutlu, H.; Kilic, S.; Onem, Y.; Kizilkaya, E. Effects of altitude on spleen volume: Sonographic assessment. J. Clin. Ultrasound 2007, 35, 182–185. [Google Scholar] [CrossRef]
- Spielmann, A.L.; DeLong, D.M.; Kliewer, M.A. Sonographic evaluation of spleen size in tall healthy athletes. Am. J. Roentgenol. 2005, 184, 45–49. [Google Scholar] [CrossRef] [PubMed]
- Jahic, D.; Kapur, E.; Radjo, I.; Zerem, E. Changes in Splenic Volume After the Treadmill Exercise at Specific Workloads in Elite Long-Distance Runners and Recreational Runners. Med. Arch. 2019, 73, 32–34. [Google Scholar] [CrossRef] [PubMed]
- Chow, K.U.; Luxembourg, B.; Seifried, E.; Bonig, H. Spleen Size Is Significantly Influenced by Body Height and Sex: Establishment of Normal Values for Spleen Size at US with a Cohort of 1200 Healthy Individuals. Radiology 2016, 279, 306–313. [Google Scholar] [CrossRef] [PubMed]
- Bezerra, A.S.; D’Ippolito, G.; Faintuch, S.; Szejnfeld, J.; Ahmed, M. Determination of splenomegaly by CT: Is there a place for a single measurement? Am. J. Roentgenol. 2005, 184, 1510–1513. [Google Scholar] [CrossRef]
- Demissie, S.; Mergu, P.; Hailu, T.; Abebe, G.; Warsa, M.; Fikadu, T. Morphometric assessment of spleen dimensions and its determinants among individuals living in Arba Minch town, southern Ethiopia. BMC Med. Imaging 2021, 21, 186. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | N | |CTax-US| | p-Value | |CTcor-US| | p-Value | |
|---|---|---|---|---|---|---|
| Age | ≥70 | 47 | 1.72 ± 1.29 | 0.01 * | 1.54 ± 0.96 | 0.302 * |
| <70 | 551 | 1.47 ± 1.00 | 1.43 ± 0.87 | |||
| BMI | ≥25 | 197 | 1.65 ± 1.06 | 0.022 * | 1.53 ± 0.99 | 0.135 * |
| <25 | 399 | 1.40 ± 1.00 | 1.40 ± 0.81 | |||
| Depth of spleen from skin on US | ≥3 cm | 81 | 1.77 ± 1.07 | 0.719 * | 1.76 ± 1.1 | 0.04 * |
| <3 cm | 517 | 1.44 ± 1.01 | 1.4 ± 0.83 | |||
| Depth of spleen from skin on CT | ≥3 cm | 103 | 1.51 ± 0.97 | 0.599 * | 1.54 ± 1.15 | 0.016 * |
| <3 cm | 495 | 1.48 ± 1.03 | 1.43 ± 0.81 | |||
| Visibility of splenic hilum on US 1 | 0 | 439 | 1.54 ± 1.07 | 0.006 † | 1.54 ± 0.9 | <0.001 † |
| 1 | 102 | 1.18 ± 0.81 | 1.22 ± 0.78 | |||
| 2 | 57 | 1.15 ± 0.9 | 1.13 ± 0.7 | |||
| Sonic window of spleen 2 | 0 | 245 | 1.58 ± 1.09 | 0.14 † | 1.61 ± 0.95 | <0.001 † |
| 1 | 282 | 1.47 ± 1.01 | 1.37 ± 0.73 | |||
| 2 | 71 | 1.40 ± 0.96 | 1.19 ± 1.03 | |||
| US operator | 1 | 76 | 1.64 ± 1.04 | 0.64 † | 1.57 ± 0.86 | 0.035 † |
| 2 | 74 | 1.36 ± 0.91 | 1.63 ± 0.78 | |||
| 3 | 111 | 1.46 ± 0.93 | 1.54 ± 0.85 | |||
| 4 | 134 | 1.49 ± 0.98 | 1.28 ± 0.87 | |||
| 5 | 132 | 1.49 ± 1.16 | 1.37 ± 0.96 | |||
| 6 | 50 | 1.39 ± 1.11 | 1.38 ± 0.81 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.W.; Park, H.S.; Park, S.; Yu, M.H.; Kim, Y.J.; Jung, S.I. Discrepancies in Splenic Size Measurement: A Comparative Analysis of Ultrasound and Computed Tomography. Diagnostics 2024, 14, 789. https://doi.org/10.3390/diagnostics14080789
Lee HW, Park HS, Park S, Yu MH, Kim YJ, Jung SI. Discrepancies in Splenic Size Measurement: A Comparative Analysis of Ultrasound and Computed Tomography. Diagnostics. 2024; 14(8):789. https://doi.org/10.3390/diagnostics14080789
Chicago/Turabian StyleLee, Hun Woo, Hee Sun Park, Sungeun Park, Mi Hye Yu, Young Jun Kim, and Sung Il Jung. 2024. "Discrepancies in Splenic Size Measurement: A Comparative Analysis of Ultrasound and Computed Tomography" Diagnostics 14, no. 8: 789. https://doi.org/10.3390/diagnostics14080789
APA StyleLee, H. W., Park, H. S., Park, S., Yu, M. H., Kim, Y. J., & Jung, S. I. (2024). Discrepancies in Splenic Size Measurement: A Comparative Analysis of Ultrasound and Computed Tomography. Diagnostics, 14(8), 789. https://doi.org/10.3390/diagnostics14080789