

One Incremental Stride for Doxycycline, One Substantial Advancement for Thyroid Eye Disease

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

References
- Perros, P.; Neoh, C.; Dickinson, J. Thyroid eye disease. BMJ 2009, 338, b560. [Google Scholar] [CrossRef]
- Bahn, R.S. Graves’ ophthalmopathy. N. Engl. J. Med. 2010, 362, 726–738. [Google Scholar] [CrossRef]
- Bartalena, L.; Baldeschi, L.; Boboridis, K.; Eckstein, A.; Kahaly, G.J.; Marcocci, C.; Perros, P.; Salvi, M.; Wiersinga, W.M. The 2016 European Thyroid Association/European group on Graves’ orbitopathy guidelines for the management of graves’ orbitopathy. Eur. Thyroid. J. 2016, 5, 9–26. [Google Scholar] [CrossRef]
- Douglas, R.S.; Gupta, S. The pathophysiology of thyroid eye disease, implications for immunotherapy. Curr. Opin. Ophthalmol. 2011, 22, 385–390. [Google Scholar] [CrossRef]
- Wiersinga, W.M.; Bartalena, L. Epidemiology and prevention of Graves’ ophthalmopathy. Thyroid 2002, 12, 855–860. [Google Scholar] [CrossRef]
- Butt, S.; Patel, B.C. Exophthalmos. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Li, Q.; Ye, H.; Ding, Y.; Chen, G.; Liu, Z.; Xu, J.; Chen, R.; Yang, H. Clinical characteristics of moderate-to-severe thyroid associated ophthalmopathy in 354 Chinese cases. PLoS ONE 2017, 12, e0176064. [Google Scholar] [CrossRef]
- Bartley, G.B.; Fatourechi, V.; Kadrmas, E.F.; Jacobsen, S.J.; Ilstrup, D.M.; Garrity, J.A.; Gorman, C.A. Clinical features of Graves’ ophthalmopathy in an incidence cohort. Am. J. Ophthalmol. 1996, 121, 284–290. [Google Scholar] [CrossRef]
- McKeag, D.; Lane, C.; Lazarus, J.H.; Baldeschi, L.; Boboridis, K.; Dickinson, A.J.; Hullo, A.I.; Kahaly, G.; Krassas, G.; Marcocci, C.; et al. Clinical features of dysthyroid optic neuropathy, a European Group on Graves’ Orbitopathy (EUGOGO) survey. Br. J. Ophthalmol. 2007, 91, 455–458. [Google Scholar] [CrossRef]
- Sahli, E.; Gunduz, K. Thyroid-associated ophthalmopathy. Turk. J. Ophthalmol. 2017, 47, 94–105. [Google Scholar] [CrossRef]
- Smith, T.J.; Hegedüs, L. Graves’ disease. N. Engl. J. Med. 2016, 375, 1552–1565. [Google Scholar] [CrossRef]
- Trobe, J.D.; Glaser, J.S.; Laflamme, P. Dysthyroid optic neuropathy. clinical profile and rationale for management. Arch. Ophthalmol. 1978, 96, 1199–1209. [Google Scholar] [CrossRef] [PubMed]
- Eckstein, A.; Quadbeck, B.; Mueller, G.; Rettenmeier, A.W.; Hoermann, R.; Mann, K.; Steuhl, P.; Esser, J. Impact of smoking on the response to treatment of thyroid associated ophthalmopathy. Br. J. Ophthalmol. 2003, 87, 773–776. [Google Scholar] [CrossRef] [PubMed]
- Bartalena, L.; Krassas, G.E.; Wiersinga, W.M.; Marcocci, C.; Salvi, M.; Daumerie, C.; Bournaud, C.; Stahl, M.; Sassi, L.; Veronesi, G.; et al. Efficacy and safety of three different cumulative doses of intravenous methylprednisolone for moderate to severe and active Graves’ orbitopathy. J. Clin. Endocrinol. Metab. 2012, 97, 4454–4463. [Google Scholar] [CrossRef] [PubMed]
- Zang, S.; Ponto, K.A.; Kahaly, G.J. Clinical review, Intravenous glucocorticoids for Graves’ orbitopathy, efficacy and morbidity. J. Clin. Endocrinol. Metab. 2011, 96, 320–332. [Google Scholar] [CrossRef] [PubMed]
- Marcocci, C.; Bartalena, L.; Tanda, M.L.; Manetti, L.; Dell’Unto, E.; Rocchi, R.; Barbesino, G.; Mazzi, B.; Bartolomei, M.P.; Lepri, P.; et al. Comparison of the effectiveness and tolerability of intravenous or oral glucocorticoids associated with orbital radiotherapy in the management of severe Graves’ ophthalmopathy, results of a prospective, single-blind, randomized study. J. Clin. Endocrinol. Metab. 2001, 86, 3562–3567. [Google Scholar] [PubMed]
- Shorr, N.; Seiff, S.R. The four stages of surgical rehabilitation of the patient with dysthyroid ophthalmopathy. Ophthalmology 1986, 93, 476–483. [Google Scholar] [CrossRef] [PubMed]
- Naik, M.N.; Nair, A.G.; Gupta, A.; Kamal, S. Minimally invasive surgery for thyroid eye disease. Indian J. Ophthalmol. 2015, 63, 847–853. [Google Scholar] [CrossRef] [PubMed]
- Shan, S.J.; Douglas, R.S. The pathophysiology of thyroid eye disease. J. Neuroophthalmol. 2014, 34, 177–185. [Google Scholar] [CrossRef] [PubMed]
- Weetman, A.P.; Cohen, S.; Gatter, K.C.; Fells, P.; Shine, B. Immunohistochemical analysis of the retrobulbar tissues in Graves’ ophthalmopathy. Clin. Exp. Immunol. 1989, 75, 222. [Google Scholar] [PubMed]
- Grubeck-Loebenstein, B.; Trieb, K.; Sztankay, A.; Holter, W.; Anderl, H.; Wick, G. Retrobulbar T cells from patients with Graves’ ophthalmopathy are CD8+ and specifically recognize autologous fibroblasts. J. Clin. Investig. 1994, 93, 2738. [Google Scholar] [CrossRef]
- Valentín, S.; Morales, A.; Sánchez, J.L.; Rivera, A. Safety and efficacy of doxycycline in the treatment of rosacea. Clin. Cosmet. Investig. Dermatol. 2009, 2, 129–140. [Google Scholar] [CrossRef] [PubMed]
- Pflugfelder, S.C.; de Paiva, C.S. Matrix metalloproteinase-9 in the pathophysiology and diagnosis of dry eye syndrome. Met. Med. 2017, 4, 37–46. [Google Scholar] [CrossRef]
- Lindeman, J.H.N.; Abdul-Hussien, H.; Van Bockel, J.H.; Wolterbeek, R.; Kleemann, R. Clinical trial of doxycycline for matrix metalloproteinase-9 inhibition in patients with an abdominal aneurysm doxycycline selectively depletes aortic wall neutrophils and cytotoxic t cells. Circulation 2009, 119, 2209–2216. [Google Scholar] [CrossRef] [PubMed]
- del Rosso, J.Q.; Webster, G.F.; Jackson, M.; Rendon, M.; Rich, P.; Torok, H.; Bradshaw, M. Two randomized phase III clinical trials evaluating anti-inflammatory dose doxycycline (40-mg doxycycline, USP capsules) administered once daily for treatment of rosacea. J. Am. Acad. Dermatol. 2007, 56, 791–802. [Google Scholar] [CrossRef] [PubMed]
- Williams, H.C.; Wojnarowska, F.; Kirtschig, G.; Mason, J.; Godec, T.R.; Schmidt, E.; Chalmers, J.R.; Childs, M.; Walton, S.; Harman, K.; et al. UK Dermatology Clinical Trials Network BLISTER Study Group. Doxycycline versus prednisolone as an initial treatment strategy for bullous pemphigoid, a pragmatic, non-inferiority, randomised controlled trial. Lancet 2017, 389, 1630–1638, Erratum in Lancet 2017, 390, 1948. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.M.; Ciancio, S.G.; Tüter, G.; Ryan, M.E.; Komaroff, E.; Golub, L.M. Subantimicrobial dose doxycycline efficacy as a matrix metalloproteinase inhibitor in chronic periodontitis patients is enhanced when combined with a non-steroidal anti-inflammatory drug. J. Periodontol. 2004, 75, 453–463. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.; Mao, Y.; Ai, S.; Liu, G.; Zhang, J.; Yan, J.; Yang, H.; Li, A.; Zou, Y.; Liang, D. Efficacy of Subantimicrobial Dose Doxycycline for Moderate-to-Severe and Active Graves’ Orbitopathy. Int. J. Endocrinol. 2015, 2015, 285698. [Google Scholar] [CrossRef] [PubMed]
- Kapelko-Słowik, K.; Słowik, M.; Szaliński, M.; Dybko, J.; Wołowiec, D.; Prajs, I.; Bohdanowicz-Pawlak, A.; Biernat, M.; Urbaniak-Kujda, D. Elevated serum concentrations of metalloproteinases (MMP-2, MMP-9) and their inhibitors (TIMP-1, TIMP-2) in patients with Graves’ orbitopathy. Adv. Clin. Exp. Med. 2018, 27, 99–103. [Google Scholar] [CrossRef]
- Huang, Y.; Suguro, R.; Hu, W.; Zheng, J.; Liu, Y.; Guan, M.; Zhou, N.; Zhang, X. Nitric oxide and thyroid carcinoma, A review. Front. Endocrinol. 2023, 13, 1050656. [Google Scholar] [CrossRef]
- Sarati, L.I.; Martinez, C.R.; Artés, N.; Arreche, N.; López-Costa, J.J.; Balaszczuk, A.M.; Fellet, A.L. Hypothyroidism, Age-related influence on cardiovascular nitric oxide system in rats. Metabolism 2012, 61, 1301–1311. [Google Scholar] [CrossRef]
- Baghcheghi, Y.; Beheshti, F.; Salmani, H.; Soukhtanloo, M.; Hosseini, M. Protective effect of pparg agonists on cerebellar tissues oxidative damage in hypothyroid rats. Neurol. Res. Int. 2016, 2016, 1952561. [Google Scholar] [CrossRef] [PubMed]
- Kayser, L.; Francis, D.; Broholm, H. Immunohistochemical localization of inducible and endothelial constitutive nitric oxide synthase in neoplastic and autoimmune thyroid disorders. Apmis 2000, 108, 785–791. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Gómez, I.; Sainz, J.; Wangensteen, R.; Moreno, J.M.; Duarte, J.; Osuna, A.; Vargas, F. Increased pressor sensitivity to chronic nitric oxide deficiency in hyperthyroid rats. Hypertension 2003, 42, 220–225. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Park, C.Y. Nitric oxide, an old drug but with new horizons in ophthalmology-a narrative review. Ann. Transl. Med. 2023, 11, 352. [Google Scholar] [CrossRef]
- Amin, A.R.; Attur, M.G.; Thakker, G.D.; Patel, P.D.; Vyas, P.R.; Patel, R.N.; Patel, I.R.; Abramson, S.B. A novel mechanism of action of tetracyclines, effects on nitric oxide synthases. Proc. Natl. Acad. Sci. USA 1996, 93, 14014–14019. [Google Scholar] [CrossRef] [PubMed]
- Greenwald, R.A.; Golub, L.M. Low dose doxycycline inhibits pyridinoline excretion in selected patients with rheumatoid arthritis. Ann. N. Y. Acad. Sci. 1994, 732, 1–507. [Google Scholar] [CrossRef] [PubMed]
- Murrell, G.A.C.; Jang, D.; Williams, R.J. Nitric oxide activates metalloprotease enzymes in articular cartilage. Biochem. Biophys. Res. Commun. 1995, 206, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Asghar, M.Y.; Lassila, T.; Törnquist, K. Calcium Signaling in the Thyroid, Friend and Foe. Cancers 2021, 13, 1994. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Tao, A.; Vaeth, M.; Feske, S. Calcium regulation of T cell metabolism. Curr. Opin. Physiol. 2020, 17, 207–223. [Google Scholar] [CrossRef]
- Lanzolla, G.; Marinò, M.; Marcocci, C. Selenium in the Treatment of Graves’ Hyperthyroidism and Eye Disease. Front. Endocrinol. 2021, 11, 608428. [Google Scholar] [CrossRef]
- Marcocci, C.; Kahaly, G.J.; Krassas, G.E.; Bartalena, L.; Prummel, M.; Stahl, M.; Altea, M.A.; Nardi, M.; Pitz, S.; Boboridis, K.; et al. European Group on Graves’ Orbitopathy. Selenium and the Course of Mild Graves’ Orbitopathy. N. Engl. J. Med. 2011, 364, 1920–1931. [Google Scholar] [CrossRef] [PubMed]
- Macovei, M.L.; Azis, Ű. A case report of a patient with severe thyroid eye disease. Rom. J. Ophthalmol. 2022, 66, 153–157. [Google Scholar] [CrossRef] [PubMed]
- Pan, Y.; Chen, Y.X.; Zhang, J.; Lin, M.L.; Liu, G.M.; Xu, X.L.; Fan, X.Q.; Zhong, Y.; Li, Q.; Ai, S.-M.; et al. Doxycycline vs. Placebo at 12 Weeks in Patients with Mild Thyroid-Associated Ophthalmopathy, A Randomized Clinical Trial. JAMA Ophthalmol. 2022, 140, 1076–1083. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Esmaeli, B. Oral Doxycycline for Mild Thyroid Eye Disease. JAMA Ophthalmol. 2022, 140, 1083–1084. [Google Scholar] [CrossRef]
- Wiersinga, W.M. Quality of life in Graves’ Ophthalmopathy. Best Pract. Res. Clin. Endocrinol. Metab. 2012, 26, 59–70. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Total (n = 82) N (%) | Treated (n = 41) N (%) | Untreated (n = 41) N (%) | p Value * | ||
|---|---|---|---|---|---|
| Gender | Female | 72 (87.8) | 35 (85.4) | 37 (90.2) | 0.5023 |
| Male | 10 (12.2) | 6 (14.6) | 4 (9.8) | ||
| Age | Median (IQR) | 50 (44–60) | 50 (44–59) | 52 (45–65) | 0.272 |
| Range | 20–77 | 20–77 | 26–77 | ||
| Smoking status | Positive | 28 (34.1) | 14 (34.1) | 14 (34.1) | 1 |
| Negative | 54 (65.9) | 27 (65.9) | 27 (65.9) |
| Parameter | Timepoint | Treated (n = 41) N (%) | Untreated (n = 41) N (%) | p Value | ||
|---|---|---|---|---|---|---|
| Treated | Untreated | |||||
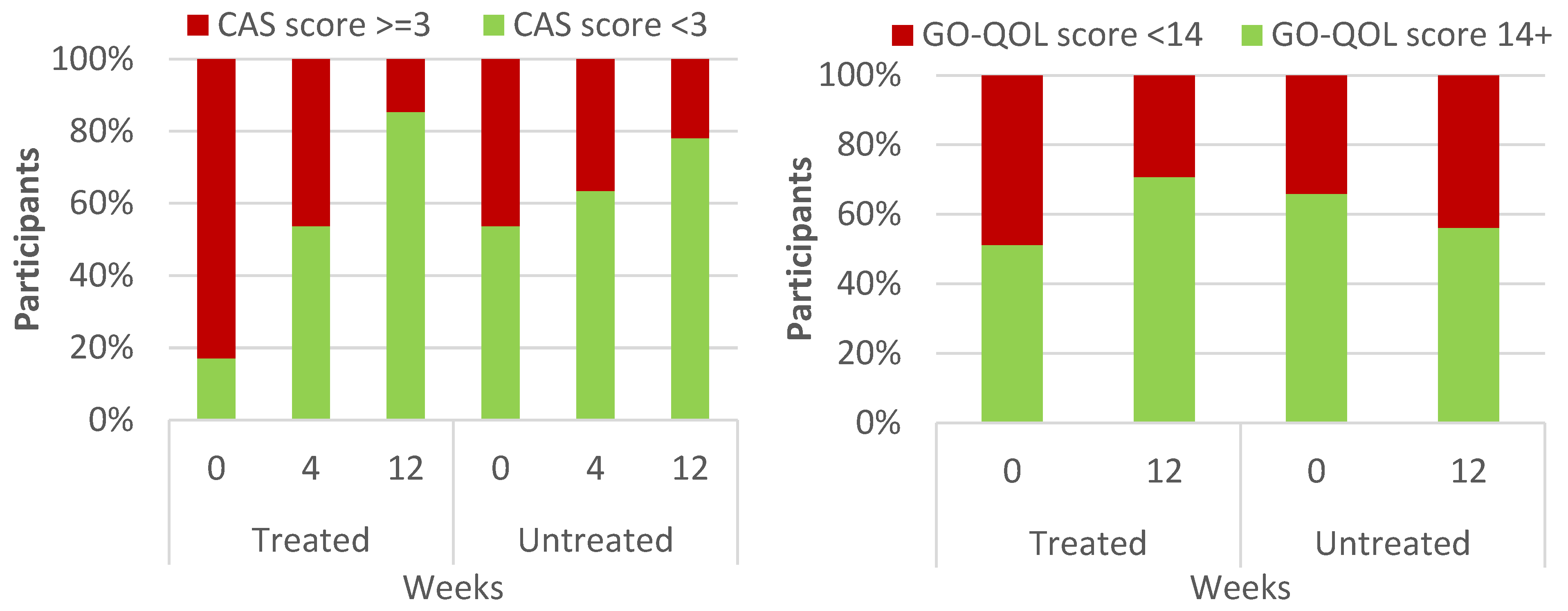
| CAS | >=3 | Baseline | 34 (82.9) | 19 (46.3) | <0.001 1 | 0.003 1 |
| Week 4 | 19 (46.3) | 15 (36.6) | ||||
| Week 12 | 6 (14.6) | 9 (22) | ||||
| GO-QOL | QOL < 14 | Baseline | 20 (48.8) | 14 (34.1) | 0.0078 2 | 0.125 2 |
| Week 12 | 12 (29.3) | 18 (43.9) | ||||
| Impaired ocular motility | Upgaze | Baseline | 9 (22) | 5 (12.2) | 0.0151 | 0.039 1 |
| Week 4 | 5 (12.2) | 2 (4.9) | ||||
| Week 12 | 4 (9.8) | 1 (2.4) | ||||
| Downgaze | Baseline | 3 (7.3) | 1 (2.4) | 0.717 1 | 1 1 | |
| Week 4 | 4 (9.8) | 1 (2.4) | ||||
| Week 12 | 4 (9.8) | 1 (2.4) | ||||
| Adduction | Baseline | 10 (24.4) | 4 (9.8) | 0.018 1 | 0.039 1 | |
| Week 4 | 10 (24.4) | 8 (19.5) | ||||
| Week 12 | 4 (9.8) | 5 (12.2) | ||||
| Abduction | Baseline | 11 (26.8) | 4 (9.8) | 0.002 1 | 0.368 1 | |
| Week 4 | 5 (12.2) | 5 (12.2) | ||||
| Week 12 | 3 (7.3) | 3 (7.3) | ||||
| Diplopia | Present | Baseline | 24 (58.5) | 8 (19.5) | <0.001 1 | 0.017 1 |
| Week 4 | 15 (36.6) | 8 (19.5) | ||||
| Week 12 | 5 (12.2) | 1 (2.4) | ||||
| MRD1 (mm) | Median (IQR) | Baseline | 4 (3–5) | 5 (4–5) | <0.0001 3 | 0.0002 3 |
| Week 4 | 5 (4–6) | 5 (4–5) | ||||
| Week 12 | 5 (4–5) | 5 (4–5) | ||||
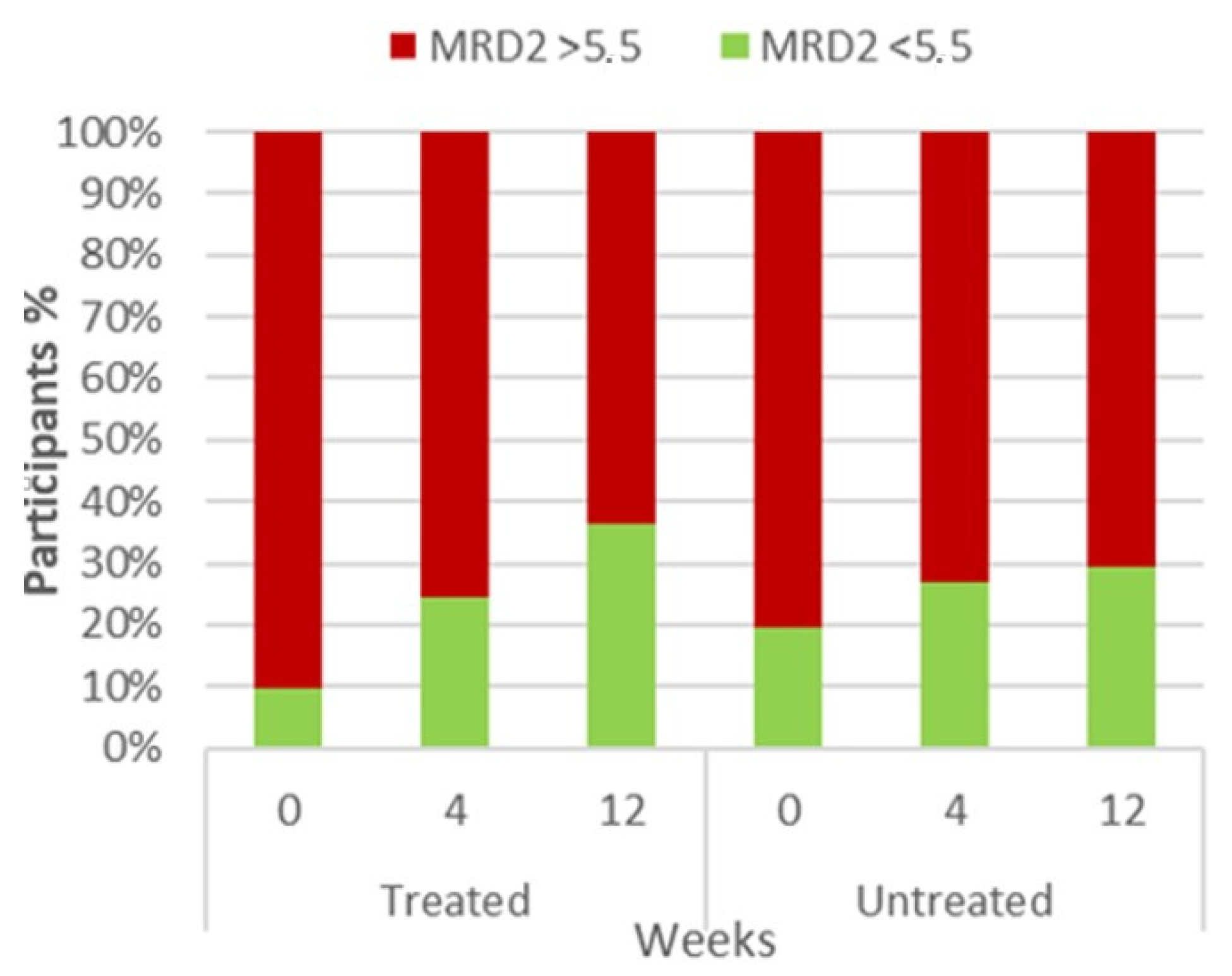
| MRD2 (mm) | Median (IQR) | Baseline | 7 (6.8–8) | 7 (6–9) | <0.0001 3 | 0.1939 3 |
| Week 4 | 6 (5.8–7.3) | 7 (5–9) | ||||
| Week 12 | 6 (5–7) | 7 (5–9) | ||||
| Eyelid aperture (mm) | Median (IQR) | Baseline | 11 (10–12.3) | 12 (10.8–13) | 0.0879 3 | 0.8118 3 |
| Week 4 | 11 (10.8–12) | 11 (11–13) | ||||
| Week 12 | 11 (10–12) | 11 (10.8–13) | ||||
| Levator (mm) | Median (IQR) | Baseline | 16 (13–18) | 17 (14.8–19) | <0.0001 3 | 0.1171 3 |
| Week 4 | 17 (16–19) | 18 (15.8–19.3) | ||||
| Week 12 | 18 (16.8–19.3) | 18 (16–18) | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matoc, I.; Kasa, K.; Kasumović, A.; Prpić, A.; Vukojević, A.; Zrinšćak, O.; Škunca Herman, J.; Doko Mandić, B.; Sabol, I.; Iveković, R.; et al. One Incremental Stride for Doxycycline, One Substantial Advancement for Thyroid Eye Disease. Diagnostics 2024, 14, 791. https://doi.org/10.3390/diagnostics14080791
Matoc I, Kasa K, Kasumović A, Prpić A, Vukojević A, Zrinšćak O, Škunca Herman J, Doko Mandić B, Sabol I, Iveković R, et al. One Incremental Stride for Doxycycline, One Substantial Advancement for Thyroid Eye Disease. Diagnostics. 2024; 14(8):791. https://doi.org/10.3390/diagnostics14080791
Chicago/Turabian StyleMatoc, Ines, Kim Kasa, Armin Kasumović, Ante Prpić, Ante Vukojević, Ognjen Zrinšćak, Jelena Škunca Herman, Blanka Doko Mandić, Ivan Sabol, Renata Iveković, and et al. 2024. "One Incremental Stride for Doxycycline, One Substantial Advancement for Thyroid Eye Disease" Diagnostics 14, no. 8: 791. https://doi.org/10.3390/diagnostics14080791
APA StyleMatoc, I., Kasa, K., Kasumović, A., Prpić, A., Vukojević, A., Zrinšćak, O., Škunca Herman, J., Doko Mandić, B., Sabol, I., Iveković, R., & Vatavuk, Z. (2024). One Incremental Stride for Doxycycline, One Substantial Advancement for Thyroid Eye Disease. Diagnostics, 14(8), 791. https://doi.org/10.3390/diagnostics14080791