
Radiation-Related Fractures after Radical Radiotherapy for Cervical and Endometrial Cancers: Are There Any Differences?

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Bone Density Measurement and Cross-Sectional Imaging Analysis
2.3. Statistics
3. Results
3.1. Patient Selection Data
3.2. Cross-Sectional Imaging Analysis, Pretreatment Bone Density Measurement and Statistical Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Wilailak, S.; Kengsakul, M.; Kehoe, S. Worldwide initiatives to eliminate cervical cancer. Int. J. Gynaecol. Obstet. 2021, 155, 102–106. [Google Scholar] [CrossRef] [PubMed]
- da Mata, S.; Ferreira, J.; Nicolás, I.; Esteves, S.; Esteves, G.; Lérias, S.; Silva, F.; Saco, A.; Cochicho, D.; Cunha, M.; et al. P16 and HPV Genotype Significance in HPV-Associated Cervical Cancer—A Large Cohort of Two Tertiary Referral Centers. Int. J. Mol. Sci. 2021, 22, 2294. [Google Scholar] [CrossRef] [PubMed]
- Koskas, M.; Amant, F.; Mirza, M.R.; Creutzberg, C.L. Cancer of the corpus uteri: 2021 update. Int. J. Gynaecol. Obstet. 2021, 155, 45–60. [Google Scholar] [CrossRef] [PubMed]
- Dörk, T.; Hillemanns, P.; Tempfer, C.; Breu, J.; Fleisch, M.C. Genetic Susceptibility to Endometrial Cancer: Risk Factors and Clinical Management. Cancers 2020, 12, 2407. [Google Scholar] [CrossRef]
- Bhatla, N.; Aoki, D.; Sharma, D.N.; Sankaranarayanan, R. Cancer of the cervix uteri. Int. J. Gynaecol. Obstet. 2018, 143, 22–36. [Google Scholar] [CrossRef] [PubMed]
- Malikova, H.; Burghardtova, M.; Fejfarova, K.; Nadova, K.; Weichet, J. Advanced cervical cancer in young women: Imaging study of late and very late radiation-related side effects after successful treatment by combined radiotherapy. Quant. Imaging Med. Surg. 2021, 11, 21–31. [Google Scholar] [CrossRef]
- Pillai, A.K.; Anderson, M.E.; Reddick, M.A.; Sutphin, P.D.; Kalva, S.P. Ureteroarterial fistula: Diagnosis and management. Am. J. Roentgenol. 2015, 204, W592–W5928. [Google Scholar] [CrossRef]
- Singh, G.K.; Yadav, V.; Singh, P.; Bhowmik, K.T. Radiation-Induced Malignancies Making Radiotherapy a “Two-Edged Sword”: A Review of Literature. World J. Oncol. 2017, 8, 1–6. [Google Scholar] [CrossRef]
- Cahan, W.G.; Woodard, H.Q.; Higinbotham, N.L.; Stewart, F.W.; Coley, B.L. Sarcoma arising in irradiated bone: Report of eleven cases. Cancer 1998, 82, 8–34. [Google Scholar] [CrossRef]
- Hall, E.J.; Wuu, C.S. Radiation-induced second cancers: The impact of 3D-CRT and IMRT. Int. J. Radiat. Oncol. Biol. Phys. 2003, 56, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Viswanathan, A.N.; Lee, L.J.; Eswara, J.R.; Horowitz, N.S.; Konstantinopoulos, P.A.; Mirabeau-Beale, K.L.; Rose, B.S.; von Keudell, A.G.; Wo, J.Y. Complications of pelvic radiation in patients treated for gynecologic malignancies. Cancer 2014, 120, 3870–3883. [Google Scholar] [CrossRef]
- Nadova, K.; Burghardtova, M.; Fejfarova, K.; Reginacova, K.; Malikova, H. Late Radiation-Related Toxicities in Patients Treated for Early-Stage Cervical Carcinoma by Surgery and Adjuvant Radiotherapy: A Retrospective Imaging Study. Pathol. Oncol. Res. 2021, 27, 1609915. [Google Scholar] [CrossRef] [PubMed]
- Kwon, J.W.; Huh, S.J.; Yoon, Y.C.; Choi, S.H.; Jung, J.Y.; Oh, D.; Choe, B.K. Pelvic bone complications after radiation therapy of uterine cervical cancer: Evaluation with MRI. Am. J. Roentgenol. 2008, 191, 987–994. [Google Scholar] [CrossRef] [PubMed]
- Papadopoulou, I.; Stewart, V.; Barwick, T.D.; Park, W.H.; Soneji, N.; Rockall, A.G.; Bharwani, N. Post-Radiation Therapy Imaging Appearances in Cervical Carcinoma. Radiographics. 2016, 36, 538–553. [Google Scholar] [CrossRef] [PubMed]
- Chung, Y.K.; Lee, Y.K.; Yoon, B.H.; Suh, D.H.; Koo, K.H. Pelvic Insufficiency Fractures in Cervical Cancer after Radiation Therapy: A Meta-Analysis and Review. Vivo 2021, 35, 1109–1115. [Google Scholar] [CrossRef] [PubMed]
- Uezono, H.; Tsujino, K.; Moriki, K.; Nagano, F.; Ota, Y.; Sasaki, R.; Soejima, T. Pelvic insufficiency fracture after definitive radiotherapy for uterine cervical cancer: Retrospective analysis of risk factors. J. Radiat. Res. 2013, 54, 1102–1109. [Google Scholar] [CrossRef]
- Nicolay, N.H.; Sommer, E.; Lopez, R.; Wirkner, U.; Trinh, T.; Sisombath, S.; Debus, J.; Ho, A.D.; Saffrich, R.; Huber, P.E. Mesenchymal stem cells retain their defining stem cell characteristics after exposure to ionizing radiation. Int. J. Radiat. Oncol. Biol. Phys. 2013, 87, 1171–1178. [Google Scholar] [CrossRef]
- Yaprak, G.; Gemici, C.; Temizkan, S.; Ozdemir, S.; Dogan, B.C.; Seseogullari, O.O. Osteoporosis development and vertebral fractures after abdominal irradiation in patients with gastric cancer. BMC Cancer 2018, 18, 972. [Google Scholar] [CrossRef]
- Vitzthum, L.K.; Park, H.; Zakeri, K.; Heide, E.S.; Nalawade, V.; Mundt, A.J.; Vaida, F.; Murphy, J.D.; Mell, L.K. Risk of Pelvic Fracture With Radiation Therapy in Older Patients. Int. J. Radiat. Oncol. Biol. Phys. 2020, 106, 485–492. [Google Scholar] [CrossRef]
- Schmeler, K.M.; Jhingran, A.; Iyer, R.B.; Sun, C.C.; Eifel, P.J.; Soliman, P.T.; Ramirez, P.T.; Frumovitz, M.; Bodurka, D.C.; Sood, A.K. Pelvic fractures after radiotherapy for cervical cancer: Implications for survivors. Cancer 2010, 116, 625–630. [Google Scholar] [CrossRef] [PubMed]
- Salcedo, M.P.; Sood, A.K.; Jhingran, A.; Eifel, P.J.; Klopp, A.H.; Iyer, R.B.; Fellman, B.M.; Jimenez, C.; Schmeler, K.M. Pelvic fractures and changes in bone mineral density after radiotherapy for cervical, endometrial, and vaginal cancer: A prospective study of 239 women. Cancer 2020, 126, 2607–2613. [Google Scholar] [CrossRef] [PubMed]
- Kurrumeli, D.; Oechsner, M.; Weidenbächer, B.; Brambs, C.; Löffler, M.; Combs, S.E.; Borm, K.; Duma, M.N. An easy way to determine bone mineral density and predict pelvic insufficiency fractures in patients treated with radiotherapy for cervical cancer. Strahlenther Onkol. 2021, 197, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Abbouchie, H.; Raju, N.; Lamanna, A.; Chiang, C.; Kutaiba, N. Screening for osteoporosis using L1 vertebral density on abdominal CT in an Australian population. Clin. Radiol. 2022, 77, e540–e548. [Google Scholar] [CrossRef] [PubMed]
- Faye, M.D.; Alfieri, J. Advances in Radiation Oncology for the Treatment of Cervical Cancer. Curr. Oncol. 2022, 29, 928–944. [Google Scholar] [CrossRef] [PubMed]
- Kronborg, C.J.; Pedersen, B.G.; Klemmensen, J.; Lefévre, A.C.; Wind, K.L.; Spindler, K.G. Pelvic Insufficiency Fractures and Bone Pain after Radiation Therapy for Anal Cancer: Relation to Pelvic Bone Dose-Volume Parameters. Adv. Radiat. Oncol. 2022, 8, 101110. [Google Scholar] [CrossRef] [PubMed]
- Kronborg, C.J.S.; Jørgensen, J.B.; Petersen, J.B.B.; Jensen, L.N.; Iversen, L.H.; Pedersen, B.G.; Spindler, K.-L.G. Pelvic insufficiency fractures, dose volume parameters and plan optimization after radiotherapy for rectal cancer. Clin. Transl. Radiat. Oncol. 2019, 19, 72–76. [Google Scholar] [CrossRef] [PubMed]
- Sini, C.; Fiorino, C.; Perna, L.; Noris Chiorda, B.; Deantoni, C.L.; Bianchi, M.; Sacco, V.; Briganti, A.; Montorsi, F.; Calandrino, R.; et al. Dose-volume effects for pelvic bone marrow in predicting hematological toxicity in prostate cancer radiotherapy with pelvic node irradiation. Radiother. Oncol. 2016, 118, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Sapienza, L.G.; Salcedo, M.P.; Ning, M.S.; Jhingran, A.; Klopp, A.H.; Calsavara, V.F.; Schmeler, K.M.; Leite Gomes, M.J.; de Freitas Carvalho, E.; Baiocchi, G. Pelvic Insufficiency Fractures After External Beam Radiation Therapy for Gynecologic Cancers: A Meta-analysis and Meta-regression of 3929 Patients. Int. J. Radiat. Oncol. Biol. Phys. 2020, 106, 475–484. [Google Scholar] [CrossRef]
- Lukka, H.; Hirte, H.; Fyles, A.; Thomas, G.; Elit, L.; Johnston, M.; Fung, M.F.; Browman, G. Cancer Care Ontario Practice Guidelines Initiative Gynecology Disease Site Group. Concurrent cisplatin-based chemotherapy plus radiotherapy for cervical cancer--a meta-analysis. Clin. Oncol. 2002, 14, 203–212. [Google Scholar] [CrossRef]
- Shrivastava, S.; Mahantshetty, U.; Engineer, R.; Chopra, S.; Hawaldar, R.; Hande, V.; Kerkar, R.A.; Maheshwari, A.; Shylasree, T.S.; Ghosh, J.; et al. Gynecologic Disease Management Group. Cisplatin Chemoradiotherapy vs Radiotherapy in FIGO Stage IIIB Squamous Cell Carcinoma of the Uterine Cervix: A Randomized Clinical Trial. JAMA Oncol. 2018, 4, 506–513. [Google Scholar] [CrossRef] [PubMed]
- Misra, S.; Lal, P.; Kumar Ep, S.; Rastogi, N.; Tiwari, A.; Singh, S.; Das, K.J.M.; Kumar, S. Comparative assessment of late toxicity in patients of carcinoma cervix treated by radiotherapy versus chemo-radiotherapy—Minimum 5 years follow up. Cancer Treat. Res. Commun. 2018, 14, 30–36. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| CC Group N = 63 | EC Group N = 64 | p-Value | |
|---|---|---|---|
| Age (years) | 52.8 ± 13.2 | 66.0 ± 9.9 | <0.001 |
| Lymph node RT (N of subjects) | 46 | 8 | <0.001 |
| BRT (N of subjects) | 60 (intracavitary) | 62 (vaginal) | 0.635 |
| Total RT dose (Gy) | 80.0 ± 14.1 | 62.1 ± 13.9 | <0.001 |
| Hormonal substitution (N of subjects) | 10 | 1 | 0.004 |
| Concomitant chemotherapy (N of subjects) | 59 | 0 | <0.001 |
| Adjuvant chemotherapy (N of subjects) | 0 | 24 | <0.001 |
| Radical surgery | 0 | 64 | <0.001 |
| Menopause (years) | 45.4 ± 7.9 | 52.0 ± 4.4 | <0.001 |
| BMI (kg/m2) | 24.9 ± 5.9 | 30.3 ± 6.8 | <0.001 |
| Time of imaging follow-up (months) | 32.8 ± 15.6 | 26.0 ± 18.1 | 0.055 |
| N of imaging exams | 9.2 ± 4.7 | 4.5 ± 2.4 | <0.001 |
| CC Group | EC Group | p-Value | |
|---|---|---|---|
| Osteonecrosis (N of subjects) | 0 | 2 | 0.496 |
| PIF (N of subjects) | 18 | 15 | 0.613 |
| Sacral PIF (N of subjects) | 15 | 12 | 0.574 |
| Pubic PIF (N of subjects) | 1 | 2 | 0.577 |
| Vertebral compression fracture (N of subjects) | 3 | 5 | 0.506 |
| A | |||
| CC Group | Subgroup with Fractures | Subgroup without Fractures | p-Value |
| N | 18 | 45 | - |
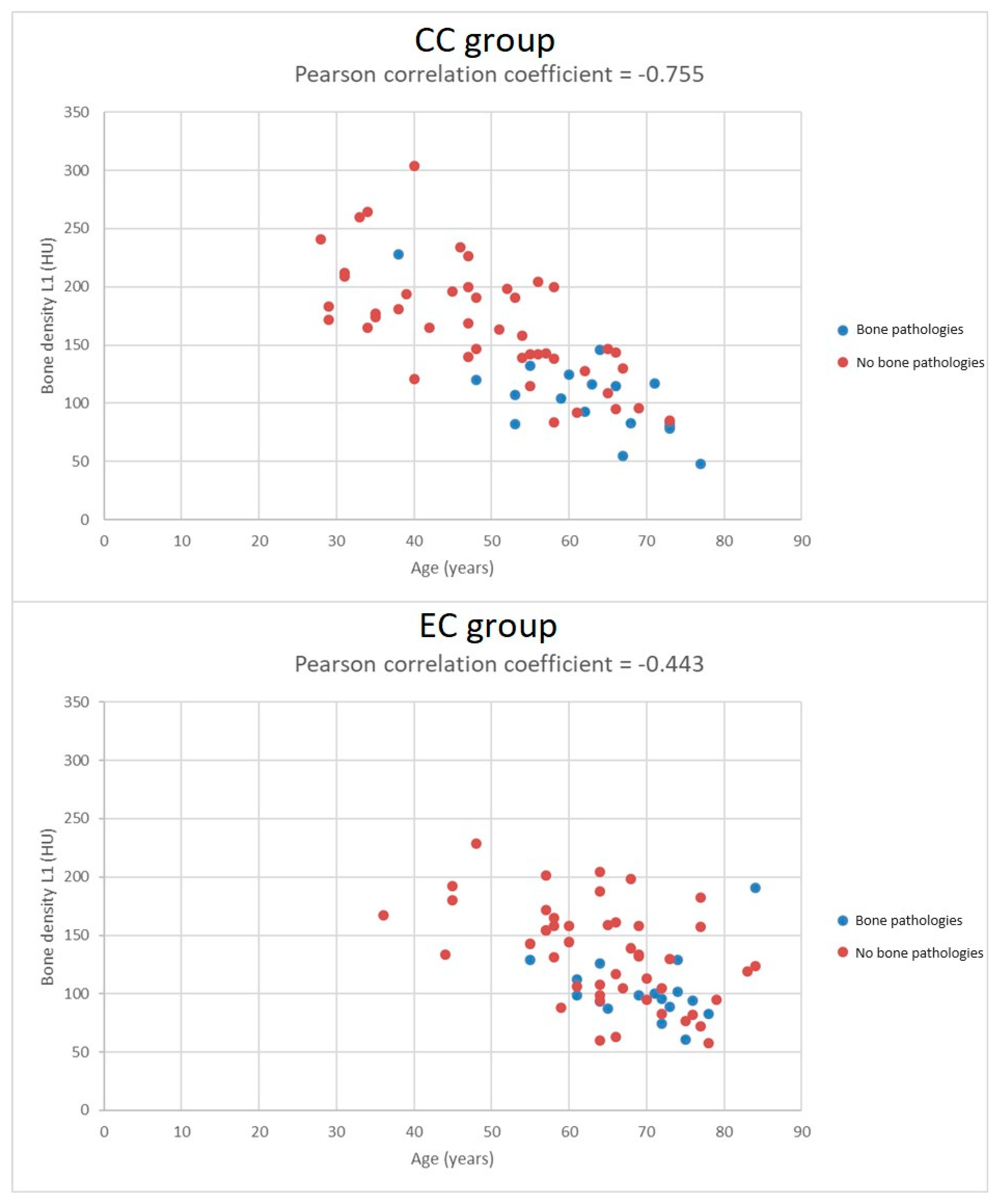
| Age (years) | 62.4 ± 10.1 | 49. 0 ± 12.4 | <0.001 |
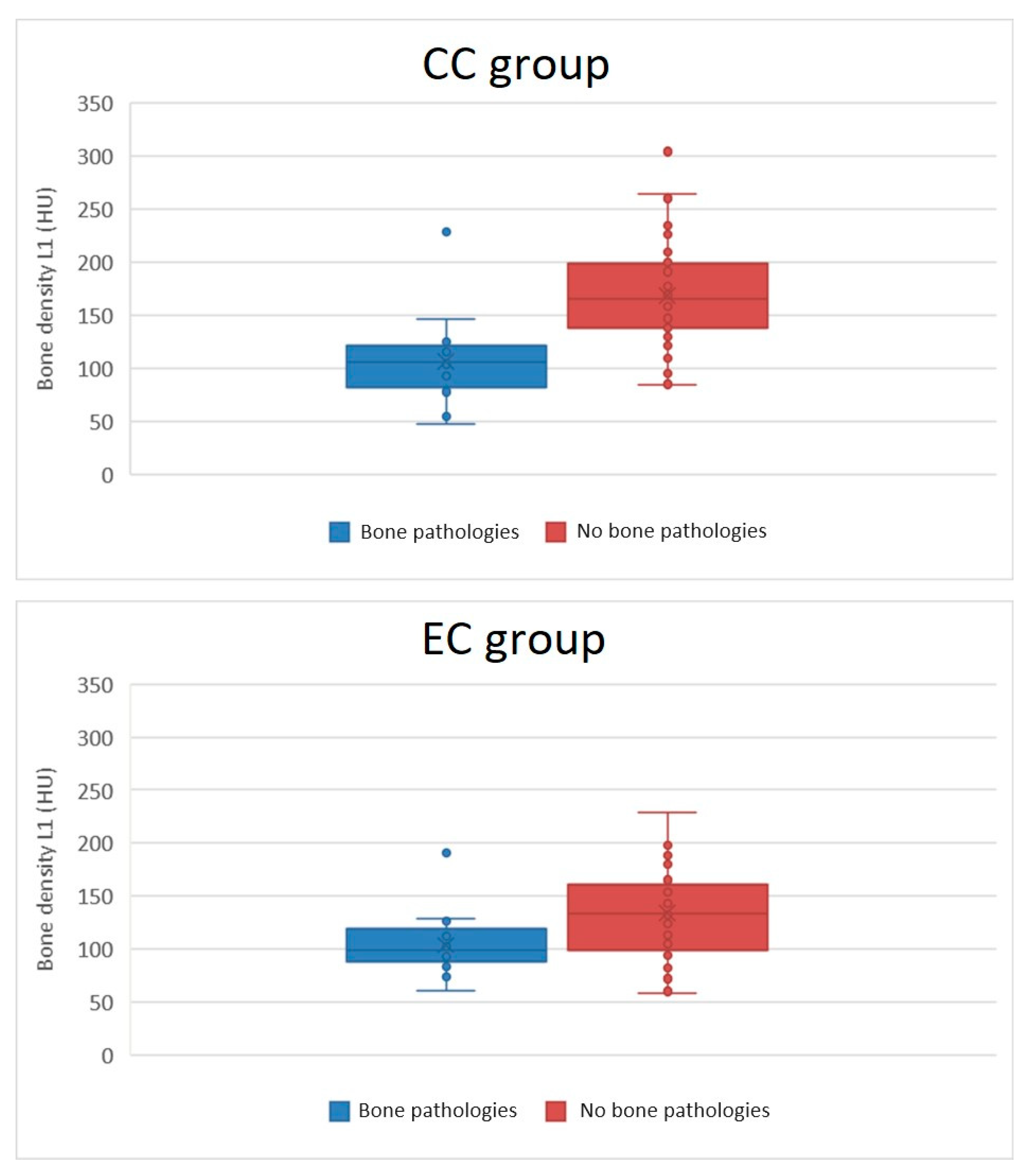
| Density (HU) | 106.3 ± 40.0 | 168.2 ± 49.5 | <0.001 |
| BMI (kg/m2) | 23.8 ± 4.2 | 25.4 ± 6.5 | 0.329 |
| Total RT dose (Gy) | 77.9 ± 5.8 | 80.6 ± 16.2 | 0.489 |
| B | |||
| EC Group | Subgroup with Fractures | Subgroup without Fractures | p-Value |
| N | 17 | 47 | - |
| Age (years) | 70.0 ± 7.3 | 64.6 ± 10.4 | 0.057 |
| Density (HU) | 103.8 ± 29.0 | 133.8 ± 42.3 | 0.009 |
| BMI (kg/m2) | 26.1 ± 4.9 | 31.8 ± 6.9 | 0.003 |
| Total RT dose (Gy) | 62.2 ± 11.4 | 62.1 ± 14.7 | 0.966 |
| C | |||
| CC Subgroup with Fractures | EC Subgroup with Fractures | p-Value | |
| N | 18 | 17 | - |
| Age (years) | 62.4 ± 10.1 | 70.0 ± 7.3 | 0.018 |
| Density (HU) | 106.3 ± 40.0 | 103.8 ± 29.0 | 0.829 |
| BMI (kg/m2) | 23.8 ± 4.2 | 26.1 ± 4.9 | 0.141 |
| Total RT dose (Gy) | 77.9 ± 5.8 | 62.2 ± 11.4 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malikova, H.; Nadova, K.; Reginacova, K.; Kremenova, K.; Rob, L. Radiation-Related Fractures after Radical Radiotherapy for Cervical and Endometrial Cancers: Are There Any Differences? Diagnostics 2024, 14, 810. https://doi.org/10.3390/diagnostics14080810
Malikova H, Nadova K, Reginacova K, Kremenova K, Rob L. Radiation-Related Fractures after Radical Radiotherapy for Cervical and Endometrial Cancers: Are There Any Differences? Diagnostics. 2024; 14(8):810. https://doi.org/10.3390/diagnostics14080810
Chicago/Turabian StyleMalikova, Hana, Katarina Nadova, Klaudia Reginacova, Karin Kremenova, and Lukas Rob. 2024. "Radiation-Related Fractures after Radical Radiotherapy for Cervical and Endometrial Cancers: Are There Any Differences?" Diagnostics 14, no. 8: 810. https://doi.org/10.3390/diagnostics14080810
APA StyleMalikova, H., Nadova, K., Reginacova, K., Kremenova, K., & Rob, L. (2024). Radiation-Related Fractures after Radical Radiotherapy for Cervical and Endometrial Cancers: Are There Any Differences? Diagnostics, 14(8), 810. https://doi.org/10.3390/diagnostics14080810