
Novelties and Perspectives of Intestinal Ultrasound in the Personalised Management of Patients with Inflammatory Bowel Diseases—A Systematic Review

 , , , , ,
, , , , , 
Abstract
1. Introduction
2. Materials and Methods
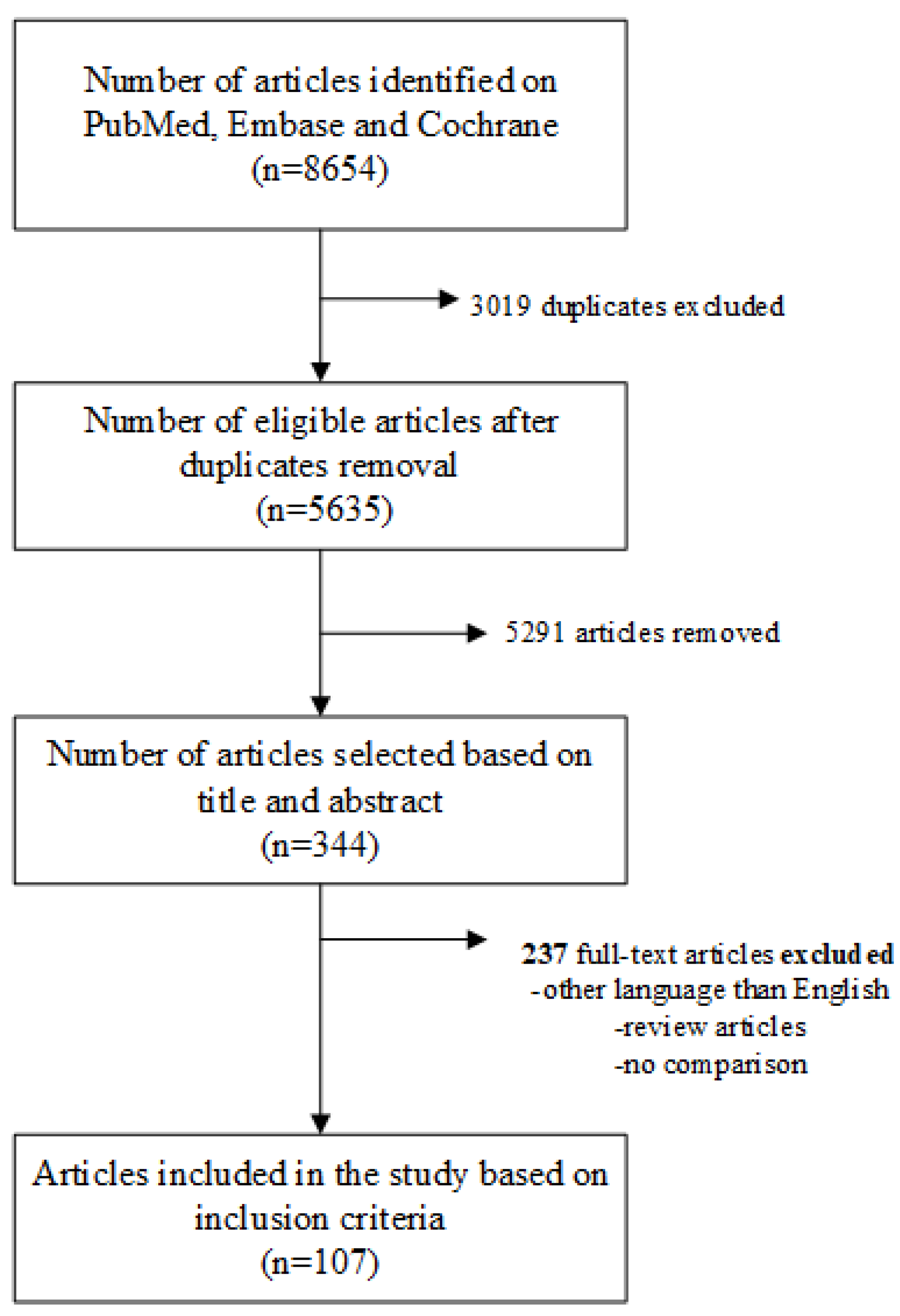
2.1. Literature Search and Search Terms
2.2. Inclusions and Exclusion Criteria
2.3. Study Selection and Data Extraction
3. Results
3.1. The Role of Ultrasound in Crohn’s Disease
3.1.1. Disease Activity Evaluation
3.1.2. Prediction of Disease Evolution and Prognosis
3.1.3. Complications Evaluation
3.1.4. Evaluation of Treatment Response
3.1.5. Postoperative Recurrence Detection
3.2. The Role of Ultrasound in Ulcerative Colitis
3.2.1. Disease Activity Evaluation
3.2.2. Prediction of Disease Evolution and Prognosis
3.2.3. Evaluation of Treatment Response
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
References
- Ampersand. Available online: https://ampersandhealth.co.uk/myibdcare/resources/ibd-statistics-2022-crohns-and-ulcerative-colitis/ (accessed on 20 February 2024).
- Guan, Q. A Comprehensive Review and Update on the Pathogenesis of Inflammatory Bowel Disease. J. Immunol. Res. 2019, 2019, 7247238. [Google Scholar] [CrossRef] [PubMed]
- Porter, R.J.; Kalla, R.; Ho, G. Ulcerative colitis: Recent advances in the understanding of disease pathogenesis [version 1; peer review: 2 approved]. F1000Research 2020, 9, 294. [Google Scholar] [CrossRef] [PubMed]
- Du, L.; Ha, C. Epidemiology and Pathogenesis of Ulcerative Colitis. Gastroenterol. Clin. N. Am. 2020, 49, 643–654. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, K.; Katsurdada, T.; Nishida, M.; Omotehara, S.; Onishi, R.; Mabe, K.; Onodera, A.; Sato, M.; Eto, K.; Suya, M.; et al. Usefulness of transabdominal ultrasonography for assessing ulcerative colitis: A prospective, multicenter study. J. Gastroenterol. 2019, 54, 521–529. [Google Scholar] [CrossRef] [PubMed]
- Saleh, A.; Abraham, B.P. Utility of Intestinal Ultrasound in Clinical Decision-Making for Inflammatory Bowel Disease. Crohn’s Colitis 2023, 360, otad027. [Google Scholar] [CrossRef] [PubMed]
- Vaughan, R.; Tjandra, D.; Patwardhan, A.; Mingos, N.; Gibson, R.; Boussioutas, A.; Ardalan, Z.; Al-Ani, A.; Gibson, P.R.; Christensen, B. Toward transmural healing: Sonographic healing is associated with improved long-term outcomes in patients with Crohn’s disease. Aliment. Pharmacol. Ther. 2022, 56, 84–94. [Google Scholar] [CrossRef] [PubMed]
- Castiglione, F.; Mainenti, P.; Testa, A.; Imperatore, N.; De Palma, G.D.; Rea, M.; Nardone, O.M.; Sanges, M.; Caporaso, N.; Rispo, A. Cross-sectional evaluation of transmural healing in patients with Crohn’s disease on maintenance treatment with anti-TNF alpha agents. Dig. Liver Dis. 2017, 49, 484–489. [Google Scholar] [CrossRef] [PubMed]
- Goertz, R.S.; Hensel, S.; Wildner, D.; Neurath, M.F.; Strobel, D. Bowel wall thickening and hyperemia assessed by high-frequency ultrasound indicate histological inflammation in Crohn’s ileitis. Abdom. Radiol. 2021, 46, 1855–1863. [Google Scholar] [CrossRef] [PubMed]
- Limberg, B. Diagnostik von chronisch-entzündlichen Darmerkrankungen durch Sonographie [Diagnosis of chronic inflammatory bowel disease by ultrasonography]. Z. Gastroenterol. 1999, 37, 495–508. [Google Scholar]
- Hakim, A.; Alexakis, C.; Pilcher, J.; Tzias, D.; Mitton, S.; Paul, T.; Saxena, S.; Pollok, R.; Kumar, S. Comparison of small intestinal contrast ultrasound with magnetic resonance enterography in pediatric Crohn’s disease. J. Gastroenterol. Hepatol. 2020, 4, 126–131. [Google Scholar] [CrossRef]
- Wilkens, R.; Peters, D.A.; Nielsen, A.H.; Hovgaard, V.P.; Glerup, H.; Krogh, K. Dynamic Contrast-Enhanced Magnetic Resonance Enterography and Dynamic Contrast-Enhanced Ultrasonography in Crohn’s Disease: An Observational Comparison Study. Ultrasound Int. Open 2017, 3, e13–e24. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Ponorac, S.; Gosnak, R.D.; Urlep, D.; Kljucevsek, D. Contrast-enhanced ultrasonography in the evaluation of Crohn disease activity in children: Comparison with histopathology. Pediatr. Radiol. 2021, 51, 410–418. [Google Scholar] [CrossRef] [PubMed]
- Goertz, R.S.; Klett, D.; Wildner, D.; Atreya, R.; Neurath, M.F.; Strobel, D. Quantitative contrast-enhanced ultrasound for monitoring vedolizumab therapy in inflammatory bowel disease patients: A pilot study. Acta Radiol. 2018, 59, 1149–1156. [Google Scholar] [CrossRef] [PubMed]
- Zezos, P.; Zittan, E.; Islam, S.; Hudson, J.; Ben-Bassat, O.; Nazarian, A.; Steinhart, H.A.; Silverberg, M.S.; Atri, M. Associations between quantitative evaluation of bowel wall microvascular flow by contrast-enhanced ultrasound and indices of disease activity in Crohn’s disease patients using both bolus and infusion techniques. J. Clin. Ultrasound 2019, 47, 453–460. [Google Scholar] [CrossRef] [PubMed]
- Goertz, R.S.; Lueke, C.; Schellhaas, B.; Pfeifer, L.; Wildner, D.; Neurath, M.F.; Strobel, D. Acoustic radiation force impulse (ARFI) shear wave elastography of the bowel wall in healthy volunteers and in ulcerative colitis. Acta Radiol. Open 2019, 8. [Google Scholar] [CrossRef] [PubMed]
- Yamada, K.; Ishikawa, T.; Kawashima, H.; Ohno, E.; Iida, T.; Ishikawa, E.; Mizutani, Y.; Sawada, T.; Maeda, K.; Yamamura, T.; et al. Evaluation of ulcerative colitis activity using transabdominal ultrasound shear wave elastography. Quant. Imaging Med. Surg. 2022, 12, 618–626. [Google Scholar] [CrossRef] [PubMed]
- Allocca, M.; Dell’Avalle, C.; Craviotto, V.; Furfaro, F.; Zilli, A.; D’Amico, F.; Bonovas, S.; Peyrin-Biroulet, L.; Fiorino, G.; Danese, S. Predictive value of Milan ultrasound criteria in ulcerative colitis: A prospective observational cohort study. United Eur. Gastroenterol. J. 2022, 10, 190–197. [Google Scholar] [CrossRef] [PubMed]
- Allocca, M.; Filippi, E.; Constantino, A.; Bonovas, S.; Fiorino, G.; Furfaro, F.; Peyrin-Biroulet, L.; Fraquelli, M.; Caprioli, F.; Danese, S. Milan ultrasound criteria are accurate in assessing disease activity in ulcerative colitis: External validation. United Eur. Gastroenterol. J. 2021, 9, 438–442. [Google Scholar] [CrossRef] [PubMed]
- Allocca, M.; Fiorino, G.; Bonovas, S.; Furfaro, F.; Gilardi, D.; Argollo, M.; Magnoni, P.; Peyrin-Biroulet, L.; Danese, S. Accuracy of humanitas ultrasound criteria in assessing disease activity and severity in ulcerative colitis: A prospective study. J. Crohn’s Colitis 2018, 12, 1385–1391. [Google Scholar] [CrossRef]
- Allocca, M.; Craviotto, V.; Bonovas, S.; Furfaro, F.; Zilli, A.; Peyrin-Biroulet, L.; Fiorino, G.; Danese, S. Predictive Value of Bowel Ultrasound in Crohn’s Disease: A 12-Month Prospective Study. Clin. Gastroenterol. Hepatol. 2022, 20, e723–e740. [Google Scholar] [CrossRef]
- Turner, D.; Ricciuto, A.; Lewis, A.; D’Amico, F.; Dhaliwal, J.; Griffiths, A.M.; Bettenworth, D.; Sandborn, W.J.; Sands, B.E.; Reinisch, W.; et al. STRIDE-II: An Update on the Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE) Initiative of the International Organization for the Study of IBD (IOIBD): Determining Therapeutic Goals for Treat-to-Target strategies in IBD. Gastroenterology 2021, 160, 1570–1583. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, T.; Fusco, S.; Blumenstock, G.; Sadik, S.; Malek, N.P.; Froehlich, E. Evaluation of bowel wall thickness by ultrasound as early diagnostic tool for therapeutic response in Crohn’s disease patients treated with ustekinumab. Z. Gastroenterol. 2022, 60, 1212–1220. [Google Scholar] [CrossRef] [PubMed]
- Paredes, J.M.; Ripolles, T.; Algarra, A.; Diaz, R.; Moreno, N.; Latorre, P.; Martinez, M.J.; Llopis, P.; Lopez, A.; Moreno-Osset, E. Intestinal ultrasonography and fecal calprotectin for monitoring inflammation of ileal Crohn’s disease: Two complementary tests. Intest. Res. 2022, 20, 361–369. [Google Scholar] [CrossRef] [PubMed]
- Barber, J.L.; Maclachlan, J.; Planche, K.; Furman, M.; Crespi, D.; Bab, N.; Beal, I. There is good agreement between MR enterography and bowel ultrasound with regards to disease location and activity in paediatric inflammatory bowel disease. Clin. Radiol. 2017, 72, 590–597. [Google Scholar] [CrossRef] [PubMed]
- Helwig, U.; Fischer, I.; Hammer, L.; Kolterer, S.; Rath, S.; Maaser, C.; Kucharzik, T. Transmural Response and Transmural Healing Defined by Intestinal Ultrasound: New Potential Therapeutic Targets? J. Crohn’s Colitis 2022, 16, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Kucharzik, T.; Wilkens, R.; D’Agostino, M.-A.; Maconi, G.; Le Bars, M.; Lahaye, M.; Bravata, I.; Nazar, M.; Ni, L.; Ercole, E.; et al. Early Ultrasound Response and Progressive Transmural Remission after Treatment with Ustekinumab in Crohn’s Disease. Clin. Gastroenterol. Hepatol. 2023, 21, 153–163.e112. [Google Scholar] [CrossRef] [PubMed]
- Rispo, A.; Imperatore, N.; Testa, A.; Bucci, L.; Luglio, G.; De Palma, G.D.; Rea, M.; Nardone, O.M.; Caporaso, N.; Castiglione, F. Combined Endoscopic/Sonographic-based Risk Matrix Model for Predicting One-year Risk of Surgery: A Prospective Observational Study of a Tertiary Centre Severe/Refractory Crohn’s Disease Cohort. J. Crohn’s Colitis 2018, 12, 784–793. [Google Scholar] [CrossRef] [PubMed]
- Orlando, S.; Fraquelli, M.; Coletta, M.; Branchi, F.; Magarotoo, A.; Conti, C.B.; Mazza, S.; Conte, D.; Basilisco, G.; Caprioli, F. Ultrasound Elasticity Imaging Predicts Therapeutic Outcomes of Patients with Crohn’s Disease Treated with Anti-Tumour Necrosis Factor Antibodies. J. Crohn’s Colitis 2018, 12, 63–70. [Google Scholar] [CrossRef]
- Kakkadasam Ramaswamy, P.; Vizhi N, K.; Yelsangikar, A.; Krishnamurthy, A.N.; Bhat, V.; Bhat, N. Utility of bowel ultrasound in assessing disease activity in Crohn’s disease. Indian J. Gastroenterol. 2020, 39, 495–502. [Google Scholar] [CrossRef]
- Liu, C.; Ding, S.-S.; Zhang, K.; Liu, L.-N.; Guo, L.-H.; Sun, L.-P.; Zhang, Y.-F.; Sun, X.-M.; Ren, W.-W.; Zhao, C.-K.; et al. Correlation between ultrasound consolidated score and simple endoscopic score for determining the activity of Crohn’s disease. Br. J. Radiol. 2020, 93, 20190614. [Google Scholar] [CrossRef]
- Kucharzik, T.; Witting, B.M.; Helwig, U.; Borner, N.; Rossler, A.; Rath, S.; Maaser, C. Use of Intestinal Ultrasound to Monitor Crohn’s Disease Activity. Clin. Gastroenterol. Hepatol. 2017, 15, 535–542.e532. [Google Scholar] [CrossRef] [PubMed]
- Ripollés, T.; Poza, J.; Ferrer, C.S.; Martinez-Perez, M.J.; Martin-Algibez, A.; de la Paez, B.H. Evaluation of Crohn’s Disease Activity: Development of an Ultrasound Score in a Multicenter Study. Inflamm. Bowel Dis. 2021, 27, 145–154. [Google Scholar] [CrossRef] [PubMed]
- Ripollés, T.; Martinez-Perez, M.J.; Paredes, J.M.; Vizuete, J.; Martin, G. The Role of Intravenous Contrast Agent in the Sonographic Assessment of Crohn’s Disease Activity: Is Contrast Agent Injection Necessary? J. Crohn’s Colitis 2019, 13, 585–592. [Google Scholar] [CrossRef] [PubMed]
- Wilkens, R.; Hagemann-Madsen, R.H.; Peters, D.A.; Nielsen, A.H.; Nørager, C.B.; Glerup, H.; Krogh, K. Validity of Contrast-enhanced Ultrasonography and Dynamic Contrast-enhanced MR Enterography in the Assessment of Transmural Activity and Fibrosis in Crohn’s Disease. J. Crohn’s Colitis 2018, 12, 48–56. [Google Scholar] [CrossRef]
- Bhatnagar, G.; Rodriguez-Justo, M.; Bassett, P.; Windsor, A.; Cohen, R.; Halligan, S.; Taylor, S.A. Inflammation and fibrosis in Crohn’s disease: Location-matched histological correlation of small bowel ultrasound features. Abdom. Radiol. 2021, 46, 144–155. [Google Scholar] [CrossRef]
- Van Wassenaer, E.A.; van Rijn, R.R.; de Voogd, F.A.E.; van Schuppen, J.; Kindermann, A.; de Meij, T.G.J.; van Limbergen, J.E.; Gecse, K.B.; D’Haens, G.R.; Benninga, M.A.; et al. Assessing Disease Activity in Pediatric Crohn’s Disease Using Ultrasound: The Pediatric Crohn Disease Intestinal Ultrasound Score. J. Pediatr. Gastroenterol. Nutr. 2023, 76, 582–589. [Google Scholar] [CrossRef] [PubMed]
- Yuksel, I.; Kilincalp, S.; Coskun, Y.; Akinci, H.; Hamamci, M.; Alkan, A. Diagnostic accuracy of intestinal ultrasound and magnetic resonance enterography for the detection of endoscopy-based disease activity in ileocolonic Crohn’s disease. Eur. J. Gastroenterol. Hepatol. 2019, 31, 809–816. [Google Scholar] [CrossRef]
- Calavrezos, L.; Bannas, P.; Warncke, M.; Wiegard, C.; Huber, S.; Manthey, C. Transabdominal Ultrasound and Magnetic Resonance Enterography in Inflammatory Bowel Disease: Results of an Observational Retrospective Single-Center Study. Ultrasound. Int. Open 2022, 8, e22–e28. [Google Scholar] [CrossRef] [PubMed]
- Dell’Era, A.; Cannatelli, R.; Ferretti, F.; Manzotti, C.; Dilillo, D.; Zuccotti, G.; Meneghin, F.; Ardizzone, S.; Maconi, G. Relevance of sonographic parameters for inflammatory bowel disease in children. J. Ultrasound 2023, 26, 815–822. [Google Scholar] [CrossRef]
- Ma, C.; Huang, P.-L.; Kang, N.; Zhang, J.; Xiao, M.; Zhang, J.-Y.; Cao, X.-C.; Dai, X.-C. The clinical value of multimodal ultrasound for the evaluation of disease activity and complications in inflammatory bowel disease. Ann. Palliat. Med. 2020, 9, 4146–4155. [Google Scholar] [CrossRef]
- Novak, K.L.; Kaplan, G.G.; Panaccione, R.; Afshar, E.E.; Tanyingoh, D.; Swain, M.; Kellar, A.; Wilson, S. A Simple Ultrasound Score for the Accurate Detection of Inflammatory Activity in Crohn’s Disease. Inflamm. Bowel Dis. 2017, 23, 2001–2010. [Google Scholar] [CrossRef] [PubMed]
- Sævik, F.; Eriksen, R.; Eide, G.E.; Gilja, O.H.; Nylund, K. Development and validation of a simple ultrasound activity score for crohn’s disease. J. Crohn’s Colitis 2021, 15, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Sævik, F.; Gilja, O.H.; Nylund, K. Gastrointestinal Ultrasound Can Predict Endoscopic Activity in Crohn’s Disease. Ultraschall. Med. 2022, 43, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.L.; Taylor, K.M.; Friedman, A.B.; Majeed, A.; Perera, N.; Gibson, P.R. Non-specific ileitis: Impact of histopathology and gastrointestinal ultrasound in achieving the diagnosis of Crohn’s disease. J. Gastroenterol. Hepatol. 2022, 6, 388–394. [Google Scholar]
- Tsai, T.L.; Marine, M.B.; Wanner, M.R.; Cooper, M.L.; Steiner, S.J.; Ouyang, F.; Jennings, S.G.; Karmazyn, B. Can ultrasound be used as the primary imaging in children with suspected Crohn disease? Pediatr. Radiol. 2017, 47, 917–923. [Google Scholar] [CrossRef] [PubMed]
- Wright, E.K.; Wang, I.; Wong, D.; Bell, S.J.; Connell, W.R.; Thompson, A.J.; Novak, K.L.; Kamm, M.A. Accuracy of point-of-care intestinal ultrasound for Crohn’s disease. Australas. J. Ultrasound Med. 2020, 23, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Xu, C.; Li, L.; Zhang, Y.; Wang, R.; Zhang, H. Diagnostic accuracy of different cross-sectional imaging techniques for disease location and activity in Crohn’s disease and external validation and comparison of MARIAs and IBUS-SAS. Abdom. Radiol. 2023, 48, 821–832. [Google Scholar] [CrossRef] [PubMed]
- Yoon, H.; Kim, J.; Lim, H.J.; Lee, M.-J.; Lim, H.; Noh, J.; Park, S. Contrast-Enhanced Ultrasonography for the Evaluation of Crohn’s Disease in Pediatric Patients. J. Korean Med. Sci. 2023, 38, e219–e230. [Google Scholar] [CrossRef] [PubMed]
- Freitas, M.; de Castro, F.D.; Silva, V.M.; Arieira, C.; Gonçalves, T.C.; Leite, S.; Moreira, M.J.; Cotter, J. Ultrasonographic scores for ileal Crohn’s disease assessment: Better, worse or the same as contrast-enhanced ultrasound? BMC Gastroenterol. 2022, 22, 252. [Google Scholar] [CrossRef]
- Servais, L.; Boschetti, G.; Meunier, C.; Gay, C.; Cotte, E.; François, Y.; Rozieres, A.; Fontaine, J.; Cuminal, L.; Chauvenet, M. Intestinal Conventional Ultrasonography, Contrast-Enhanced Ultrasonography and Magnetic Resonance Enterography in Assessment of Crohn’s Disease Activity: A Comparison with Surgical Histopathology Analysis. Dig. Dis. Sci. 2022, 67, 2492–2502. [Google Scholar] [CrossRef]
- Grandmougin, A.; D’Amico, F.; Remen, T.; Danese, S.; Bonneton, M.; Gallroy, M.A.; Peyrin-Birouler, L.; Laurent, V. Role of Cross-Sectional Imaging in Pediatric Inflammatory Bowel Disease. Dig. Dis. Sci. 2022, 67, 2462–2470. [Google Scholar] [CrossRef] [PubMed]
- Rueda García, J.L.; Suárez-Ferrer, C.; Cordón, J.P.; Martín-Arranz, E.; Azofra, M.S.; Ramírez, L.G.; Noci, J.; Martín-Arranz, M.D. Doppler Activity and Ultrasonographic Detection of Intra-Abdominal Fistulas Are Predictors of Surgery in Crohn’s Disease. Dig. Dis. 2021, 39, 204–210. [Google Scholar] [CrossRef] [PubMed]
- St-Pierre, J.; Delisle, M.; Kheirkhahrahimabadi, H.; Goodsall, T.M.; Bryant, R.V.; Christensen, B.; Vaughan, R.; Al-Ani, A.; Ingram, R.; Heatherington, J.; et al. Bedside Intestinal Ultrasound Performed in an Inflammatory Bowel Disease Urgent Assessment Clinic Improves Clinical Decision-Making and Resource Utilisation. Crohn’s Colitis 2023, 360, otad050. [Google Scholar] [CrossRef] [PubMed]
- Gonen, C.; Surmelioglu, A.; Kichan, K.; Ozer, S.; Aslan, E.; Tilki, M. Impact of intestinal ultrasound with a portable system in the management of Crohn’s disease. Gastroenterol. Rep. 2021, 9, 418–426. [Google Scholar] [CrossRef] [PubMed]
- Les, A.; Iacob, R.; Saizu, R.; Cotruta, B.; Saizu, A.I.; Iacob, S.; Gheorghe, L.; Gheorghe, C. Bowel Ultrasound: A Non-invasive, Easy to Use Method to Predict the Need to Intensify Therapy in Inflammatory Bowel Disease Patients. J. Gastrointestin. Liver Dis. 2021, 30, 462–469. [Google Scholar] [CrossRef]
- Quaia, E.; Gennari, A.G.; Cova, M.A. Early Predictors of the Long-term Response to Therapy in Patients with Crohn Disease Derived from a Time-Intensity Curve Analysis After Microbubble Contrast Agent Injection. J. Ultrasound Med. 2019, 38, 947–958. [Google Scholar] [CrossRef] [PubMed]
- Allocca, M.; Buono, A.D.; D’Alessio, S.; Spaggiari, P.; Garlatti, V.; Spinelli, A.; Faita, F.; Danese, S. Relationships Between Intestinal Ultrasound Parameters and Histopathologic Findings in a Prospective Cohort of Patients with Crohn’s Disease Undergoing Surgery. J. Ultrasound Med. Off. J. Am. Inst. Ultrasound Med. 2023, 42, 1717–1728. [Google Scholar] [CrossRef] [PubMed]
- Ding, S.S.; Fang, Y.; Wan, J.; Zhao, C.-K.; Xiang, L.-H.; Liu, H.; Pu, H.; Xu, G.; Zhang, K.; Xu, X.-R.; et al. Usefulness of Strain Elastography, ARFI Imaging, and Point Shear Wave Elastography for the Assessment of Crohn Disease Strictures. J. Ultrasound Med. Off. J. Am. Inst. Ultrasound Med. 2019, 38, 2861–2870. [Google Scholar] [CrossRef] [PubMed]
- Jung, J.H.; Ryu, Y.J.; Kim, J.Y.; Yang, H.R. Transperineal ultrasonography for treatment response evaluation in children with perianal Crohn’s disease. Ultrasonography 2022, 41, 770–781. [Google Scholar] [CrossRef]
- Kamel, S.; Sakr, M.; Hamed, W.; Eltabbakh, M.; Askar, S.; Bassuny, A.; Hussein, R.; Elbaz, A. Comparative study between bowel ultrasound and magnetic resonance enterography among Egyptian inflammatory bowel disease patients. World J. Gastroenterol. 2020, 26, 5884–5895. [Google Scholar] [CrossRef]
- Lee, E.H.; Yang, H.R.; Kim, J.Y. Comparison of Transperianal Ultrasound with Colonoscopy and Magnetic Resonance Imaging in Perianal Crohn Disease. J. Pediatr. Gastroenterol. Nutr. 2018, 66, 614–619. [Google Scholar] [CrossRef] [PubMed]
- Quaia, E.; Gennari, A.G.; Cova, M.A.; van Beek, E.J.R. Differentiation of Inflammatory from Fibrotic Ileal Strictures among Patients with Crohn’s Disease Based on Visual Analysis: Feasibility Study Combining Conventional B-Mode Ultrasound, Contrast-Enhanced Ultrasound and Strain Elastography. Ultrasound Med. Biol. 2018, 44, 762–770. [Google Scholar] [CrossRef] [PubMed]
- Rispo, A.; Imperatore, N.; Testa, A.; Mainenti, P.; De Palma, G.D.; Luglio, G.; Maurea, S.; Nardone, O.M.; Caporaso, N.; Castiglione, F. Bowel damage in Crohn’s disease: Direct comparison of ultrasonography-based and magnetic resonance-based lemann index. Inflamm. Bowel Dis. 2017, 23, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.J.; Mao, R.; Li, X.; Cao, Q.; Chen, Z.; Liu, B.; Chen, S.; Chen, B.; He, Y.; Zeng, Z.; et al. Real-time shear wave ultrasound elastography differentiates fibrotic from inflammatory strictures in patients with Crohn’s disease. Inflamm. Bowel Dis. 2018, 24, 2183–2190. [Google Scholar] [CrossRef] [PubMed]
- Yamanashi, K.; Katsurda, T.; Nishida, M.; Onishi, R.; Omotehara, S.; Otagiri, S.; Sakurai, K.; Nagashima, K.; Kinoshita, K.; Takagi, R.; et al. Crohn’s Disease Activity Evaluation by Transabdominal Ultrasonography: Correlation with Double-Balloon Endoscopy. J. Ultrasound Med. 2021, 40, 2595–2605. [Google Scholar] [CrossRef] [PubMed]
- Sidhu, S.D.; Joseph, S.; Dunn, E.; Cuffari, C. The Utility of Contrast Enhanced Ultrasound and Elastography in the Early Detection of Fibro-Stenotic Ileal Strictures in Children with Crohn’s Disease. Pediatr. Gastroenterol. Hepatol. Nutr. 2023, 26, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Serra, C.; Rizzello, F.; Pratico, C.; Felicani, C.; Fiorini, E.; Brugnera, R.; Mazzotta, E.; Giunchi, F.; Fiorentino, M.; D’Errico, A.; et al. Real-time elastography for the detection of fibrotic and inflammatory tissue in patients with stricturing Crohn’s disease. J. Ultrasound 2017, 20, 273–284. [Google Scholar] [CrossRef]
- Lu, C.; Gui, X.; Chen, W.; Fung, T.; Novak, K.; Wilson, S.R. Ultrasound Shear Wave Elastography and Contrast Enhancement: Effective Biomarkers in Crohn’s Disease Strictures. Inflamm. Bowel Dis. 2017, 23, 421–430. [Google Scholar] [CrossRef]
- Luglio, G.; Giglio, M.C.; Rispo, A.; Bucci, C.; Sollazzo, V.; Castiglione, F.; De Palma, G.D.; Bucci, L. Diagnostic Accuracy of 3-Dimensional Endoanal Ultrasound in Identifying Perianal Crohn’s Fistulas. Dis. Colon Rectum 2018, 61, 931–937. [Google Scholar] [CrossRef]
- Dillman, J.R.; Dehkordy, S.F.; Smith, E.A.; DiPietro, M.A.; Sanchez, R.; DeMatos-Maillard, V.; Adler, J.; Zhang, B.; Trout, A.T. Defining the ultrasound longitudinal natural history of newly diagnosed pediatric small bowel Crohn disease treated with infliximab and infliximab–azathioprine combination therapy. Pediatr. Radiol. 2017, 47, 924–934. [Google Scholar] [CrossRef]
- Chen, Y.J.; Chen, B.-L.; Liang, M.-J.; Chen, S.-L.; Li, X.-H.; Qiu, Y.; Pang, L.-L.; Xia, Q.-Q.; He, Y.; Zeng, Z.-R.; et al. Longitudinal Bowel Behavior Assessed by Bowel Ultrasound to Predict Early Response to Anti-TNF Therapy in Patients with Crohn’s Disease: A Pilot Study. Inflamm. Bowel Dis. 2022, 28, S67–S75. [Google Scholar] [CrossRef]
- Paredes, J.M.; Moeno, N.; Latorre, P.; Ripollés, T.; Martinez, M.J.; Vizuete, J.; Moreno-Osset, E. Clinical Impact of Sonographic Transmural Healing after Anti-TNF Antibody Treatment in Patients with Crohn’s Disease. Dig. Dis. Sci. 2019, 64, 2600–2606. [Google Scholar] [CrossRef] [PubMed]
- Castiglione, F.; Imperatore, N.; Testa, A.; De Palma, G.D.; Nardone, O.M.; Pellegrini, L.; Caporaso, N.; Rispo, A. One-year clinical outcomes with biologics in Crohn’s disease: Transmural healing compared with mucosal or no healing. Aliment. Pharmacol. Ther. 2019, 49, 1026–1039. [Google Scholar] [CrossRef] [PubMed]
- Zorzi, F.; Ghosh, S.; Chiaramonte, C.; Lolli, E.; Ventura, M.; Onali, S.; De Cristofaro, E.; Fantini, M.C.; Biancone, L.; Monteleone, G.; et al. Response Assessed by Ultrasonography as Target of Biological Treatment for Crohn’s Disease. Clin. Gastroenterol. Hepatol. 2020, 18, 2030–2037. [Google Scholar] [CrossRef] [PubMed]
- Bernell, O.; Lapidus, A.; Hellers, G. Risk Factors for Surgery and Postoperative Recurrence in Crohn’s Disease. Ann. Surg. 2000, 231, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Regueiro, M. Management and Prevention of Postoperative Crohn’s Disease. Inflamm. Bowel Dis. 2009, 15, 1583–1590. [Google Scholar] [CrossRef] [PubMed]
- Macedo, C.P.; Costa, M.S.; Gravito-Soares, E.; Gravito-Soares, M.; Ferreira, A.M.; Portela, F.; Figueiredo, P. Role of Intestinal Ultrasound in the Evaluation of Postsurgical Recurrence in Crohn’s Disease: Correlation with Endoscopic Findings. GE Port. J. Gastroenterol. 2022, 29, 178–186. [Google Scholar] [CrossRef] [PubMed]
- Martínez, M.J.; Ripolles, T.; Paredes, J.M.; Moreno-Osset, E.; Pazos, J.M.; Blanc, E. Intravenous Contrast-Enhanced Ultrasound for Assessing and Grading Postoperative Recurrence of Crohn’s Disease. Dig. Dis. Sci. 2019, 64, 1640–1650. [Google Scholar] [CrossRef] [PubMed]
- Aho Fält, U.; Zawadzki, A.; Starck, M.; Bohe, M.; Regnér, S.; Johnson, L.B. Postoperative three-dimensional endoanal ultrasound findings and relation to anal fistula plug failure. Scand. J. Gastroenterol. 2023, 58, 1200–1206. [Google Scholar] [CrossRef]
- Goodsall, T.M.; Day, A.S.; Andrews, J.M.; Ruszkiewicz, A.; Ma, C.; Bryant, R.V. Composite Assessment Using Intestinal Ultrasound and Calprotectin Is Accurate in Predicting Histological Activity in Ulcerative Colitis: A Cohort Study. Inflamm. Bowel Dis. 2024, 30, 190–195. [Google Scholar] [CrossRef]
- Stojkovic Lalosevic, M.; Milutinovic, A.S.; Zaric, V.M.; Lolic, I.; Toplicanin, A.; Dragasevic, S.; Stojkovic, M.; Stojanovic, M.; Aleksic, M.; Stjepanovic, M.; et al. Intestinal Ultrasonography as a Tool for Monitoring Disease Activity in Patients with Ulcerative Colitis. Int. J. Clin. Pract. 2022, 2022, 3339866. [Google Scholar] [CrossRef]
- Kellar, A.; Wilson, S.; Kaplan, G.; DeBruyn, J.; Tanyingoh, D.; Novak, K.L. The Simple Pediatric Activity Ultrasound Score (SPAUSS) for the Accurate Detection of Pediatric Inflammatory Bowel Disease. J. Pediatr. Gastroenterol. Nutr. 2019, 69, e1–e6. [Google Scholar] [CrossRef]
- Fodor, I.; Serban, O.; Serban, D.E.; Farcau, D.; Fufezan, O.; Asavoaie, C.; Man, S.C.; Dumitrascu, D.L. The value of abdominal ultrasonography compared to colonoscopy and faecal calprotectin in following up paediatric patients with ulcerative colitis. Med. Ultrason. 2021, 23, 153–160. [Google Scholar] [CrossRef]
- Takahara, M.; Hiraoka, S.; Ohmori, M.; Takeuchi, K.; Takei, K.; Yasutomi, E.; Igawa, S.; Yamamoto, S.; Yamasaki, Y.; Inokuchi, T.; et al. The Colon Wall Thickness Measured Using Transabdominal Ultrasonography Is Useful for Detecting Mucosal Inflammation in Ulcerative Colitis. Intern. Med. 2022, 61, 2703–2709. [Google Scholar] [CrossRef]
- Scarallo, L.; Maniscalco, V.; Paci, M.; Renzo, S.; Naldini, S.; Barp, J.; Tasciotti, L.; Lionetti, P. Bowel Ultrasound Scan Predicts Corticosteroid Failure in Children with Acute Severe Colitis. J. Pediatr. Gastroenterol. Nutr. 2020, 71, 46–51. [Google Scholar] [CrossRef] [PubMed]
- De Voogd, F.; Wilkens, R.; Gecse, K.; Allocca, M.; Novak, K.; Lu, C.; D’Haens, G.; Maaser, C. A Reliability Study: Strong Inter-Observer Agreement of an Expert Panel for Intestinal Ultrasound in Ulcerative Colitis. J. Crohn’s Colitis 2021, 15, 1284–1290. [Google Scholar] [CrossRef]
- Sathananthan, D.; Rajagopalan, A.; Van De Ven, L.; Martin, S.; Fon, J.; Costello, S.; Bryant, R.V. Point-of-care gastrointestinal ultrasound in inflammatory bowel disease: An accurate alternative for disease monitoring. J. Gastroenterol. Hepatol. 2020, 4, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Miyoshi, J.; Ozaki, R.; Yonezawa, H.; Mori, H.; Kawamura, N.; Matsuura, M.; Hisamatsu, T. Ratio of submucosal thickness to total bowel wall thickness as a new sonographic parameter to estimate endoscopic remission of ulcerative colitis. J. Gastroenterol. 2022, 57, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Lim, K.Y.; Raja Ali, R.A.; Wong, Z.; Mohd Zaki, F.; Maktar, J.F.; Nawawi, K.N.M. Evaluation of intestinal ultrasound for disease activity assessment in patients with inflammatory bowel disease: A cross-sectional study at a tertiary centre in Malaysia. Saudi J. Gastroenterol. 2023, 29, 300–308. [Google Scholar] [CrossRef]
- Van Wassenaer, E.A.; van Rijn, R.R.; Zwetsloot, S.L.M.; de Voogd, F.A.E.; van Schuppen, J.; Kindermann, A.; de Meij, T.G.J.; van Limbergen, J.E.; Gecse, K.B.; D’Haens, G.R.; et al. Intestinal Ultrasound to Assess Ulcerative Colitis Disease Activity in Children: External Validation and Comparison of 2 Intestinal Ultrasound Activity Indices. Inflamm. Bowel Dis. 2023, 29, 1217–1222. [Google Scholar] [CrossRef]
- Omotehara, S.; Nishida, M.; Kinoshita, K.; Onishi, R.; Onodera, A.; Suya, M.; Hasegawa, T.; Mitsumori, D.; Katsurada, T.; Teshima, T. Validation of US evaluation of ulcerative colitis activity. Ultrasound Med. Biol. 2019, 45, 1537–1544. [Google Scholar] [CrossRef]
- Jin, R.F.; Chen, Y.M.; Chen, R.P.; Ye, H.J. Endoscopic ultrasonography in the evaluation of condition and prognosis of ulcerative colitis. World J. Clin. Cases 2022, 10, 4818–4826. [Google Scholar] [CrossRef] [PubMed]
- Bots, S.; De Voogd, F.; De Jong, M.; Ligtvoet, V.; Löwenberg, M.; Duijvestein, M.; Ponsioen, C.Y.; D’Haens, G.; Gecse, K.B. Point-of-care Intestinal Ultrasound in IBD Patients: Disease Management and Diagnostic Yield in a Real-world Cohort and Proposal of a Point-of-care Algorithm. J. Crohn’s Colitis 2022, 16, 606–615. [Google Scholar] [CrossRef] [PubMed]
- Piazza, O.; Sed, N.; Noviello, D.; Filippi, E.; Conforti, F.; Furfaro, F.; Fraquelli, M.; Costantino, A.; Danese, S.; Vecchi, M.; et al. Superior predictive value of transmural over endoscopic severity for colectomy risk in ulcerative colitis: A multicenter prospective cohort study. J. Crohn’s Colitis 2024, 18, 291–299. [Google Scholar] [CrossRef] [PubMed]
- Ilvemark, J.F.K.F.; Wilkens, R.; Thielsen, P.; Dige, A.; Boysen, T.; Brynskov, J.; Bjerrum, J.T.; Seidelin, J.B. Early Intestinal Ultrasound Predicts Intravenous Corticosteroid Response in Hospitalised Patients with Severe Ulcerative Colitis. J. Crohn’s Colitis 2022, 16, 1725–1734. [Google Scholar] [CrossRef]
- Smith, R.L.; Taylor, K.M.; Friedman, A.B.; Swaine, A.P.; Gibson, D.J.; Gibson, P.R. Early Assessment with Gastrointestinal Ultrasound in Patients Hospitalised for a Flare of Ulcerative Colitis and Predicting the Need for Salvage Therapy: A Pilot Study. Ultrasound Med. Biol. 2021, 47, 1108–1114. [Google Scholar] [CrossRef]
- Yan, B.M.; Sey, M.S.L.; Beletrutti, P.; Brahm, G.; Guizzetti, L.; Jairath, V. Reliability of the endoscopic ultrasound ulcerative colitis (eus-uc) score for assessment of inflammation in patients with ulcerative colitis. Endosc. Int. Open 2021, 9, E1116–E1122. [Google Scholar] [CrossRef]
- De Voogd, F.; Joshi, H.; Van Wassenaer, E.; Bots, S.; D’Haens, G.; Gecse, K. Intestinal Ultrasound to Evaluate Treatment Response During Pregnancy in Patients with Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2022, 28, 1045–1052. [Google Scholar] [CrossRef]
- Miles, A.; Bhatnagar, G.; Halligan, S.; Gupta, A.; Tolan, D.; Zealley, I.; Taylor, S.A. Magnetic resonance enterography, small bowel ultrasound and colonoscopy to diagnose and stage Crohn’s disease: Patient acceptability and perceived burden. Eur. Radiol. 2019, 29, 1083–1093. [Google Scholar] [CrossRef]
- Rajagopalan, A.; Sathananthan, D.; An, Y.-K.; Van De Ven, L.; Martin, S.; Fon, J.; Costello, S.P.; Begun, J.; Bryant, R.V. Gastrointestinal ultrasound in inflammatory bowel disease care: Patient perceptions and impact on disease-related knowledge. JGH Open 2020, 4, 267–272. [Google Scholar] [CrossRef]
- Friedman, A.B.; Asthana, A.; Knowles, S.R.; Robbins, A.; Gibson, P.R. Effect of point-of-care gastrointestinal ultrasound on decision-making and management in inflammatory bowel disease. Aliment. Pharmacol. Ther. 2021, 54, 652–666. [Google Scholar] [CrossRef] [PubMed]
- Allocca, M.; Fiorino, G.; Bonifacio, C.; Furfaro, F.; Gilardi, D.; Argollo, M.; Peyrin-Biroulet, L.; Danese, S. Comparative Accuracy of Bowel Ultrasound Versus Magnetic Resonance Enterography in Combination with Colonoscopy in Assessing Crohn’s Disease and Guiding Clinical Decision-making. J. Crohn’s Colitis 2018, 12, 1280–1287. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.C.; Chang, C.W.; Chen, M.J.; Wang, H.Y. Intestinal ultrasound in inflammatory bowel disease: A novel and increasingly important tool. J. Med. Ultrasound 2023, 31, 86–91. [Google Scholar]
- Kellar, A.; Dolinger, M.; Novak, K.L.; Chavannes, M.; Dubinsky, M.; Huynh, H. Intestinal Ultrasound for the Pediatric Gastroenterologist: A Guide for Inflammatory Bowel Disease Monitoring in Children: Expert Consensus on Behalf of the International Bowel Ultrasound Group (IBUS) Pediatric Committee. J. Pediatr. Gastroenterol. Nutr. 2023, 76, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Dolinger, M.T.; Calabrese, E.; Pizzolante, F.; Abreu, M.T. Current and Novel Uses of Intestinal Ultrasound in Inflammatory Bowel Disease. Gastroenterol. Hepatol. 2023, 19, 447–457. [Google Scholar]
- Dolinger, M.T.; Kayal, M. Intestinal ultrasound as a non-invasive tool to monitor inflammatory bowel disease activity and guide clinical decision making. World J. Gastroenterol. 2023, 29, 2272–2282. [Google Scholar] [CrossRef] [PubMed]
- Nardone, O.M.; Calabrese, G.; Testa, A.; Caiazzo, A.; Fierro, G.; Rispo, A.; Castiglione, F. The Impact of Intestinal Ultrasound on the Management of Inflammatory Bowel Disease: From Established Facts toward New Horizons. Front. Med. 2022, 9, 898092. [Google Scholar] [CrossRef] [PubMed]
- Carter, D.; Katz, L.H.; Bardan, E.; Salomon, E.; Goldstein, S.; Horin, S.B.; Kopylov, U.; Eliakim, R. The accuracy of intestinal ultrasound compared with small bowel capsule endoscopy in assessment of suspected Crohn’s disease in patients with negative ileocolonoscopy. Therap. Adv. Gastroenterol. 2018, 11, 1756284818765908. [Google Scholar] [CrossRef]
- Flanagan, E.; Wright, E.K.; Begun, J.; Bryant, R.V.; An, Y.-K.; Ross, A.L.; Kiburg, K.; Bell, S. Monitoring Inflammatory Bowel Disease in Pregnancy Using Gastrointestinal Ultrasonography. J. Crohn’s Colitis 2020, 14, 1405–1412. [Google Scholar] [CrossRef]
- Leung, Y.; Shim, H.H.; Wilkens, R.; Tanyingoh, D.; Afshar, E.E.; Sharifi, N.; Pauls, M.; Novak, K.L.; Kaplan, G.G.; Panaccione, R.; et al. The role of bowel ultrasound in detecting subclinical inflammation in pregnant women with Crohn’s disease. J. Can. Assoc. Gastroenterol. 2019, 2, 153–160. [Google Scholar] [CrossRef]
- Barber, J.L.; Zambrano-Perez, A.; Olsen, Ø.E.; Kiparissi, F.; Baycheva, M.; Knaflez, D.; Shah, N.; Watson, T.A. Detecting inflammation in inflammatory bowel disease—How does ultrasound compare to magnetic resonance enterography using standardised scoring systems? Pediatr. Radiol. 2018, 48, 843–851. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.A.; Mallett, S.; Bhatnagar, G.; Baldwin-Cleland, R.; Bloom, S.; Gupta, A.; Hamlin, P.J.; Hart, A.L.; Higginson, A.; Jacobs, I.; et al. Diagnostic accuracy of magnetic resonance enterography and small bowel ultrasound for the extent and activity of newly diagnosed and relapsed Crohn’s disease (METRIC): A multicentre trial. Lancet Gastroenterol. Hepatol. 2018, 3, 548–558. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, R.; Abduljabbar, A.; Wazzan, M.; Thabit, R.; Mosli, M.; Saadah, O. Magnetic resonance enterography and bowel ultrasonography in Saudi Arabian patients with Crohn’s disease: A correlation study. Saudi J. Gastroenterol. 2022, 28, 186–192. [Google Scholar] [CrossRef] [PubMed]
- Imsirovic, B.; Zerem, E.; Guso, E.; Djedovic, M.; Cengic, A.; Baljic, R.; Merhemic, Z.; Efendic, A. Comparison of Conventional Ultrasound and Contrast Enhanced Magnetic Resonance (MR) Enterography in Evaluation Patients with Crohn’s Disease. Acta Inform. Med. 2018, 26, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Ding, S.S.; Liu, C.; Zhang, Y.-F.; Sun, L.; Xiang, L.-H.; Liu, H.; Fang, Y.; Ren, W.-W.; Zhao, H.; Sun, X.-M.; et al. Contrast-enhanced ultrasound in the assessment of Crohn’s disease activity: Comparison with computed tomography enterography. Radiol. Medica 2022, 127, 1068–1078. [Google Scholar] [CrossRef]
- Roushan, N.; Ebrahimi Daryani, N.; Azizi, Z.; Pournaghshband, H.; Niksirat, A. Differentiation of Crohn’s disease and ulcerative colitis using intestinal wall thickness of the colon: A Diagnostic accuracy study of endoscopic ultrasonography. Med. J. Islam. Repub. Iran 2019, 33, 57. [Google Scholar] [CrossRef]


{kind=link}
| Study | Study Design | No. of Patients | Age | Significant Parameters | Accuracy | Comparator |
|---|---|---|---|---|---|---|
| Calavrezos et al. [39] | Retrospective | 44 | 29.5 (21–47) | BWT > 3 mm increased CDS | Se 88.1%, Sp 50%, PPV = 86.1, NPV = 54.6, Accuracy 79.6% | CS, MRE |
| Dell’Era et al. [40] | Retrospective | 113 | 10.8 ± 4.0 | Increased BWT (>3 mm) | Se 69.6%, Sp 96.7%, PPV = 84.2%, NPV = 92.6 | CS |
| Altered bowel pattern | Se 78.3%, Sp 93.3%, PPV = 75%, NPV = 94.4% | |||||
| i-fat | Se 65.2%, Sp 92.2%, PPV = 68.2%, NPV = 91.2% | |||||
| Ma et al. [41] | Prospective | 15 | 36.87 ± 16.14 | BWT > 4.7 mm | Se 90%, Sp 80% | CS, CT |
| PE (44.37 dB) | Se 75%, Sp 100% | |||||
| TTP (10.73 s) | Se 94%, Sp 25% | |||||
| AUC (226.15 dBsec) | Se 81%, Sp 75% | |||||
| Novak et al. [42] | Retrospective and prospective | 160 + 87 | 34.9 (25–48) | SSS (based on BWT and CDS) | Se 92.1–93.3%, Sp 76.8–81.6%, PPV = 79.6–88.2%, NPV = 86.3–93.2%, Accuracy 86.2–87.5% | CS |
| Ponorac et al. [13] | Prospective | 24 | 14 (13–17) | BWT, CDS, loss of BWS, i-fat | Se 55.6%, Sp 86.4%, Accuracy 72.5% | Histopathological result |
| Ripolles et al. [33] | Prospective | 72 | 45.6 | Simple CEUS score = (BWT × 0.957) + (CDS × 0.859) + (wash-in × 0.036). | Se 94%, Sp 91%, PPV 95.9%, NPV 87% | CS |
| Saevik et al. [43] | Prospective | 164 | 41.5 (18–83) | SUS-CD = BWT × 1.053 + CDS × 1.934 + i-fat × 1.275 + BWS × 1.225 + 0.242 | Se 95.3%, Sp 70.3%, AUC 0.92 | CS |
| Saevik et al. [44] | Prospective | 145 | 18–83 | BWT ≥ 3 mm | Se 92.2%, Sp 86%, PPV 94%, NPV 82.2% | CS |
| BWT ≥ 4 mm | Se 80.4%, Sp 90.7%, PPV 95.3%, NPV 66.1% | |||||
| CDS | Se 66.7%, Sp 97.7, PPV 98.6%, NPV 55.3% | |||||
| Smith et al. [45] | Retrospective | 8 | 54 (35–65) | BWT 5.0 mm (4.4–6.7) increased CDS | N/A | CS |
| Tsai et al. [46] | Prospective | 41 | 13.7 (4.6–18.9) | Ileal BWT > 1.9 (1.8) mm | Se > 91% | CS, MRE |
| Wright et al. [47] | Retrospective | 65 | - | BWT > 3 mm ± increased CDS, loss of BWS, i-fat, LN | Se 72%, Sp 86.7% | CS |
| Se 87.5%, Sp 61.1% | MRE | |||||
| Xu et al. [48] | Retrospective | 115 | 31 (24–42) | BWT > 3 mm, loss of BWS, i-fat, CDS (Limberg score) | Se 90.9% (91.9% by adding CDS) | CS, MRE, CTE |
| Study | Study Design | No. of Patients | Frequency of Re-Evaluation | IUS Parameters | Outcome with Parameter |
|---|---|---|---|---|---|
| Alloca et al. [19] | Prospective | 225 | Baseline, 12 months | BUSS ≥ 3.52 (0.75 × BWT + 1.65 × BWF) | Overall negative course, treatment escalation |
| Complications at baseline | Overall negative course, surgery | ||||
| Helwig et al. [26] | Prospective | 234 | Baseline, 12 and 52 weeks | Patients with TR or simplified TH at 12 weeks (see text) had a better evolution at 52 weeks | |
| Kucharzik et al. [32] | Prospective | 234 | Baseline, then at 3, 6, and 12 months | BWT, BWS, CDS (Limberg) | Clinical and biochemical improvement |
| Les et al. [56] | Prospective | 89 | Baseline, 6 months | BUS score > 0.45 (=1/(1 + EXP(−0.88 × BWT + 2.02 × Doppler − 6.67) | Need for IBD treatment intensification in 6 months |
| Les et al. [56] | Prospective | 89 | Baseline, 6 months | BUS score > 0.5 (=1/(1 + EXP (−0.75 × BWT + 3.5 × Doppler − 7.31) | Immediate treatment intensification due to active disease |
| BUS score > 0.6 (=1/(1 + EXP (−0.8 × BWT − 1.3 × BWS − 3.82) | Subsequent treatment intensification in a 6-month time frame | ||||
| Rispo et al. [28] | Prospective | 100 | - | BWT ≥ 7 mm, SB extension ≥ 33 cm, stricturing/penetrating disease | Need for surgery in a 1-year time frame |
| Rueda Garcia et al. [53] | Retrospective | 70 | - | Pathological CDS, presence of fistulas or abscesses | Increased risk of surgery |
| Vaughan et al. [7] | Retrospective | 202 | - | Sonographic inflammation: abnormal BWT, CDS, BWS, or i-fat | Univariate analysis: use of corticosteroids, reduced hospitalisation-free and surgery-free survival |
| Multivariate analysis: use of corticosteroids | |||||
| Quaia et al. [57] | Prospective | 115 | Baseline and at ≈6 weeks | Higher values of pretreatment PE, AUC wash-in, AUC wash-out | More severe inflammation is associated with a better response to treatment |
| Study | Study Design | No. of Patients | Complication by IUS | Se (%) | Sp (%) | Acc (%) | PPV | NPV |
|---|---|---|---|---|---|---|---|---|
| Alloca et al. [58] | Prospective | 17 | Stenosis | 93 (68–100) | 86 (42–100) | 91 (71–99) | 93 (68–100) | 86 (42–100) |
| Calavrezos et al. [39] | Retrospective | 44 | Stenosis | 57.1 | 91.5 | 87 | 50 | 93.5 |
| Fistula | 57.1 | 100 | 94.4 | 100 | 95 | |||
| Abscess | 60 | 95.5 | 88.9 | 75 | 91.3 | |||
| Ding et al. [59] | Prospective | 25 | p-SWE for differentiating inflammatory from fibrotic stenoses | 75 | 100 | 96 | 100 | 95.5 |
| Hakim et al. [11] | Retrospective | 93 | Stenosis (by SICUS) | 67 | 100 | 94.1 | 100 | 93.3 |
| Jung et al. [60] | Retrospective | 29 | Perianal fistula (TPUS, evolution under treatment) | 63.3 | 93.3 | 73.3 | 95 | 56 |
| Kamel et al. [61] | Prospective | 26 | Fistula | 85.7 | 100 | 95 | 100 | 92.9 |
| Stricture | 100 | 94.4 | 95 | 66.7 | 100 | |||
| Abscess | 100 | 100 | 100 | 100 | 100 | |||
| Lee et al. [62] | Retrospective | 38 | Perianal fistula (TPUS) | 76.3 | 53.3 | - | 84.2 | 40.8 |
| Perianal abscess (TPUS) | 56.3 | 98.1 | - | 90 | 88 | |||
| Quaia et al. [63] | Prospective | 20 | Stenosis detected by B-mode + CEUS + SE | 35/45 | 25/40 | 70/75 | - | - |
| Wright et al. [47] | Retrospective | 65 | Strictures, fistulas, abscesses | 85.7 | 94.3 | - | - | - |
| Type of Response | BWT Normalisation | CDS Normalisation | Normal BWS | No i-fat |
|---|---|---|---|---|
| TR | X | |||
| Simplified TH | X | X | ||
| Extended TH | X | X | X | X |
| Two out of three parameters assessed; one could not be assessed/documented | ||||
| Complete TH | X | X | X | X |
| All three parameters assessed | ||||
| Study | Study Design | No. of Patients | Treatment | IUS Frequency of Re-Evaluation | IUS Outcome | Additional Outcomes |
|---|---|---|---|---|---|---|
| Kucharzik et al. [27] | Interventional (randomised) | 77 | Ustekinumab | Baseline, then at 4, 8, 16, and 32 weeks | TR (reduction of BWT ≥ 25% or normalisation of all IUS parameters) | Progressive improvement of BWT, CDS, BWS, i-fat |
| Dillman et al. [71] | Prospective observational | 28 | Infliximab ± Azathioprine | Baseline, then at ≈2 weeks and ≈1, 3, and 6 months | Reduction of length of bowel wall disease involvement, BWT, CDS | - |
| Hoffman et al. [23] | Interventional (non-randomised) | 23 | Ustekinumab | Before the first (week 0) and second (week 8) administration | Reduction of BWT of at least 1 mm | Decrease in CDAI (at least 70), CRP (≥0.5 mg/dL) |
| Orlando et al. [29] | Interventional (non-randomised) | 30 | Infliximab or Adalimumab | Baseline, then at 14 and 52 weeks | Reduction of BWT (normal BWT considered TH) | SR ≥ 2 indicates non-responders and increased risk of surgery |
| Paredes et al. [73] | Interventional (non-randomised) | 36 | Infliximab or Adalimumab | Baseline, then at 12 weeks and 1 year | TH (BWT ≤ 3 mm, colour Doppler grade 0 or 1), improvement (≥2 mm decrease in BWT and ≥1 grade of CDS) | Partial (100 points CDAI decrease) or complete (150 points) clinical response, clinical remission |
| Zorzi et al. [75] | Prospective observational | 80 | Infliximab or Adalimumab | Baseline and 18 (12–24) months | Improvement (≥1 mm) or normalisation of BWT, decreased length of disease, TH associated with better outcomes | - |
| Castiglione et al. [74] | Prospective observational | 218 | Infliximab or Adalimumab | Every 3 months for at least 1 year | TH is associated with reduced rates of hospitalisation, surgery or need for corticosteroids | MH is also associated with better outcomes than no healing group |
| Chen et al. [72] | Prospective observational | 30 | Infliximab | Baseline, then at weeks 2, 6, and 14 | Decrease in BWT or TH (BWT ≤ 3 mm), SWE as a predictor of non-responsiveness (cut-off 15.2 kPa) | Clinical response (ΔCDAI ≥ −100) or remission (CDAI < 150), mucosal healing |
| Quaia et al. [63] | Prospective observational | 115 | Infliximab or Adalimumab | Baseline and at ≈6 weeks | Decrease in BWT in responders; higher PE, WIAUC and WOAUC in responders at baseline vs. post-treatment | - |
| Study | Study Design | No. of Patients | Active Disease Parameter(s) | Se (%) | Sp (%) | PPV (%) | NPV (%) | AUC | Acc (%) | Comparator |
|---|---|---|---|---|---|---|---|---|---|---|
| Alloca et al. [19] | Prospective | 43 | MUC (=1.4 × BWT + 2 × CDS) > 6.2 (development phase) | 71 | 100 | - | - | 0.891 | - | Mayo Endoscopic Score |
| MUC (=1.4 × BWT + 2 × CDS) > 6.2 (validation phase) | 85 | 94 | - | - | 0.902 | - | ||||
| Sathananthan et al. [88] | Prospective | 39 | BWT > 3 mm + increased CDS (POCUS) | 92 | 86 | 92 | 86 | - | - | CS within 30 days |
| 100 | 100 | 100 | 100 | CS on the same day | ||||||
| Disease extent | 92 | 80 | 80 | 86 | - | - | CS | |||
| Myioshi et al. [89] | Retrospective | 29 | BWT ≥ 3.75 | 73.3 | 93.2 | 88 | 83.7 | - | - | CS |
| LWS | 49.1 | 84.2 | 90 | 36.4 | - | - | ||||
| SMI (=SMT/BWT × 100) ≥ 49.7 | 83.3 | 81.8 | 75.8 | 87.8 | - | - | ||||
| Positive CDS | 76.7 | 90.9 | 85.2 | 85.1 | - | - | ||||
| Lim et al. [90] Lim et al. | Prospective Prospective | 29 29 | BWT > 3 mm, LWS, increased CDS, i-fat | 50 | 100 | 100 | 84 | - | - | CS |
| - | - | |||||||||
| BWT > 3 mm | 33.3 | 65.4 | 10 | 89.5 | - | - | ||||
| LWS | 33.3 | 84.6 | 20 | 91.7 | - | - | ||||
| i-fat | 33.3 | 92.3 | 33.3 | 92.3 | - | - | ||||
| Increased CDS | 33.3 | 92.3 | 33.3 | 92.3 | - | - | ||||
| Goodsall et al. [81] | Prospective | 19 | MUC > 6.3 | 55 | 100 | 100 | 31 | - | - | Histology |
| MUC > 6.3 and FC > 100 μg/g | 88 | 80 | 95 | 57 | - | - | ||||
| Stojkovic et al. [82] | Retrospective | 55 | BWT, CDS, i-fat, LWS, LN | 87.8 | 83.3 | - | - | - | - | CS |
| BWT > 4.75 mm for moderate–severe disease | 82 | 64 | - | - | - | - | ||||
| Takahara et al. [85] | Prospective | 80 | BWT > 2 mm, MES > 0 | 94 | 77 | 93 | 80 | 90 | CS | |
| van Wassenaer et al. [91] | Prospective | 35 | UC-IUS > 1 for MES ≥ 2 | 88–100 | 83–87 | 0.82–0.88 | CS | |||
| Civitelly index > 2 | 6–25 | 93–100 | 0.76–0.84 | |||||||
| Yamada et al. [17] | Prospective | 26 | SWE > 2.2 m/s | 86.4 | 75 | 0.909 | CS |
| Study | Study Design | No. of Patients | Treatment | IUS Frequency of Re-Evaluation | IUS Outcome |
|---|---|---|---|---|---|
| Jin et al. [93] | Prospective | 79 | Mesalazine ± steroids, Infliximab | Baseline, then at 2 and 6 months | Decrease in EUS-UC score at the follow-up visits |
| Smith et al. [97] | Prospective | 10 | Steroids and Infliximab for acute severe UC | First 24 h, then at 3 and 7 days | Lower BWT and significant decrease in responders |
| Helwig et al. [26] | Prospective | 171 | Corticosteroids, AZA/6-MP, anti-TNF, anti-integrin | Baseline and 12 weeks | TR and TH at 12 weeks are associated with better outcomes |
| Goertz et al. [14] | Prospective | 7 | Vedolizumab | Baseline and 14 weeks | A slight decrease in BWT and CDS grade in responders, increase in non-responders a significant decrease in WiR in responders |
| Ilvemark et al. [96] | Prospective | 56 | Corticosteroids for acute severe UC | Before treatment, at 24 ± 24 h and 6 ± 1 days | BWT ≥ 4 mm and BWT reduction ≤ 1 mm or ≤20% in non-responders at 48 h |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mihai, V.-C.; Gheorghe, L.; Rezuș, I.-I.; Jucan, A.E.; Andronic, M.-C.; Gavrilescu, O.; Dranga, M.; Andronic, A.-M.; Prelipcean, C.C.; Rezuș, C.; et al. Novelties and Perspectives of Intestinal Ultrasound in the Personalised Management of Patients with Inflammatory Bowel Diseases—A Systematic Review. Diagnostics 2024, 14, 812. https://doi.org/10.3390/diagnostics14080812
Mihai V-C, Gheorghe L, Rezuș I-I, Jucan AE, Andronic M-C, Gavrilescu O, Dranga M, Andronic A-M, Prelipcean CC, Rezuș C, et al. Novelties and Perspectives of Intestinal Ultrasound in the Personalised Management of Patients with Inflammatory Bowel Diseases—A Systematic Review. Diagnostics. 2024; 14(8):812. https://doi.org/10.3390/diagnostics14080812
Chicago/Turabian StyleMihai, Vasile-Claudiu, Liliana Gheorghe, Ioana-Irina Rezuș, Alina Ecaterina Jucan, Mihaela-Cristiana Andronic, Otilia Gavrilescu, Mihaela Dranga, Andrei-Mihai Andronic, Cristina Cijevschi Prelipcean, Ciprian Rezuș, and et al. 2024. "Novelties and Perspectives of Intestinal Ultrasound in the Personalised Management of Patients with Inflammatory Bowel Diseases—A Systematic Review" Diagnostics 14, no. 8: 812. https://doi.org/10.3390/diagnostics14080812
APA StyleMihai, V.-C., Gheorghe, L., Rezuș, I.-I., Jucan, A. E., Andronic, M.-C., Gavrilescu, O., Dranga, M., Andronic, A.-M., Prelipcean, C. C., Rezuș, C., & Mihai, C. (2024). Novelties and Perspectives of Intestinal Ultrasound in the Personalised Management of Patients with Inflammatory Bowel Diseases—A Systematic Review. Diagnostics, 14(8), 812. https://doi.org/10.3390/diagnostics14080812