
Clinical Impact of Neutrophil Variation on COVID-19 Complications

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics According to Disease Severity
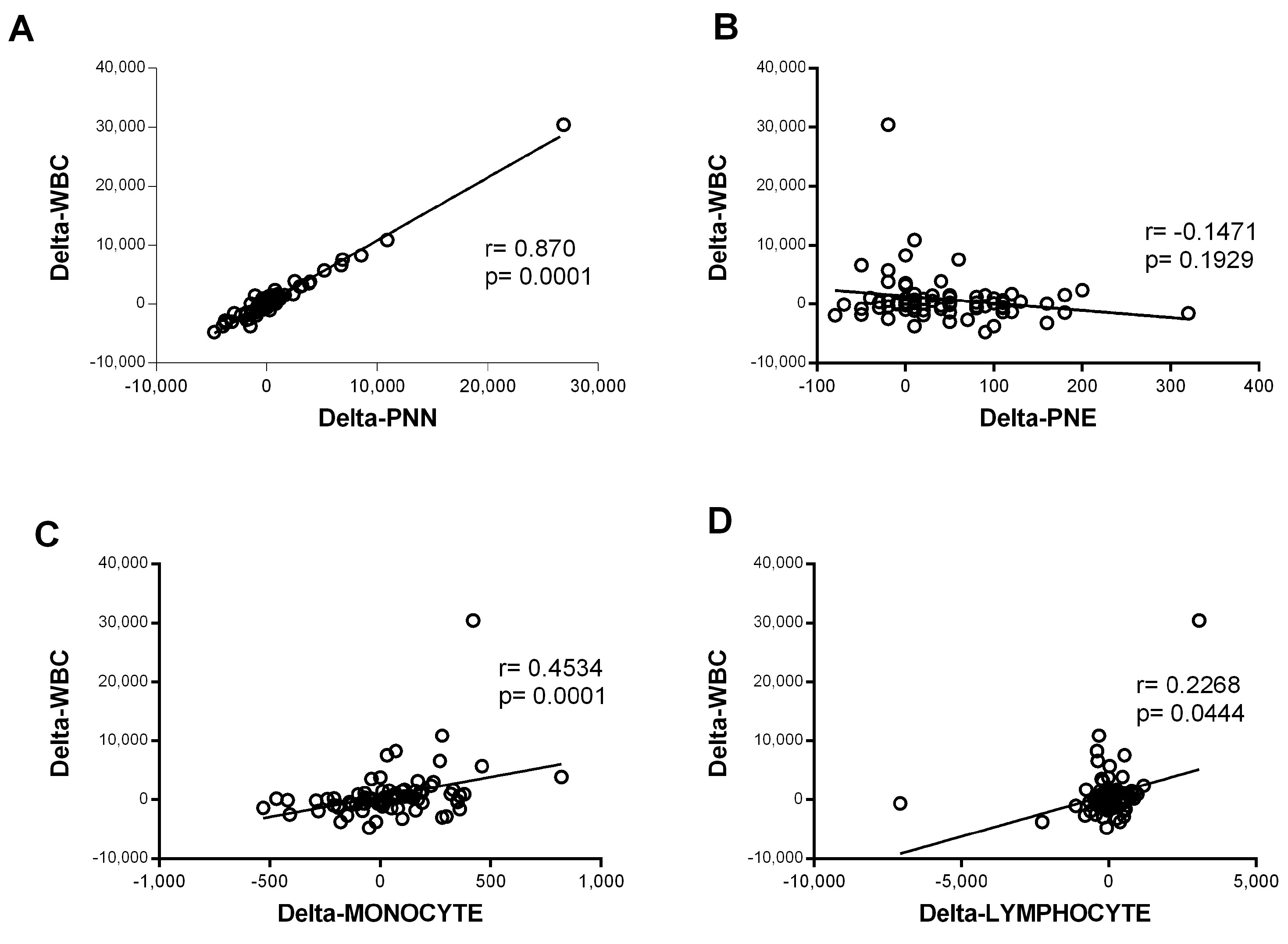
3.2. Immune Blood Cell Involvement in COVID-19
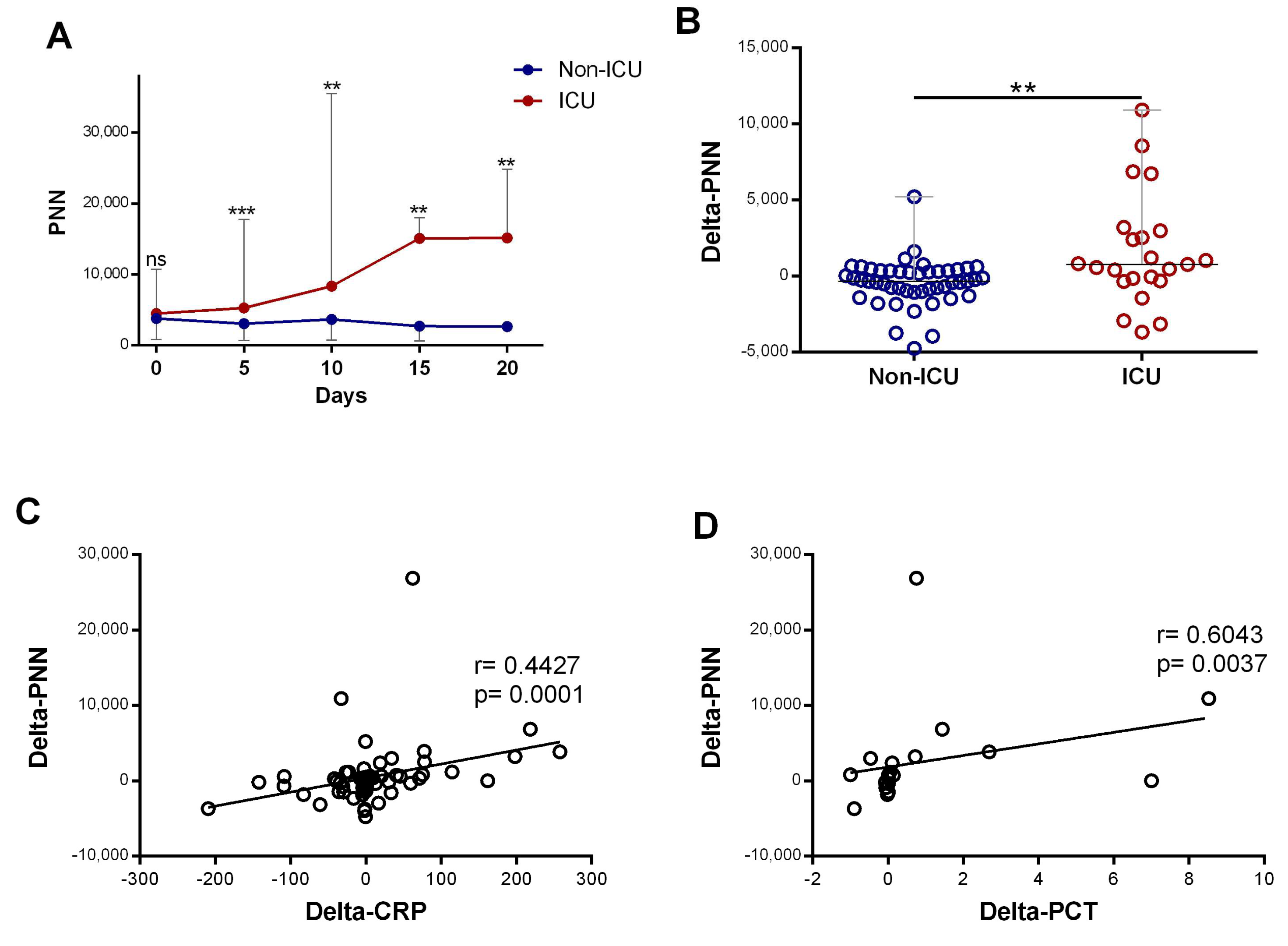
3.3. High Neutrophil Counts Significantly Associated with Disease Severity and Inflammatory Biomarker Levels
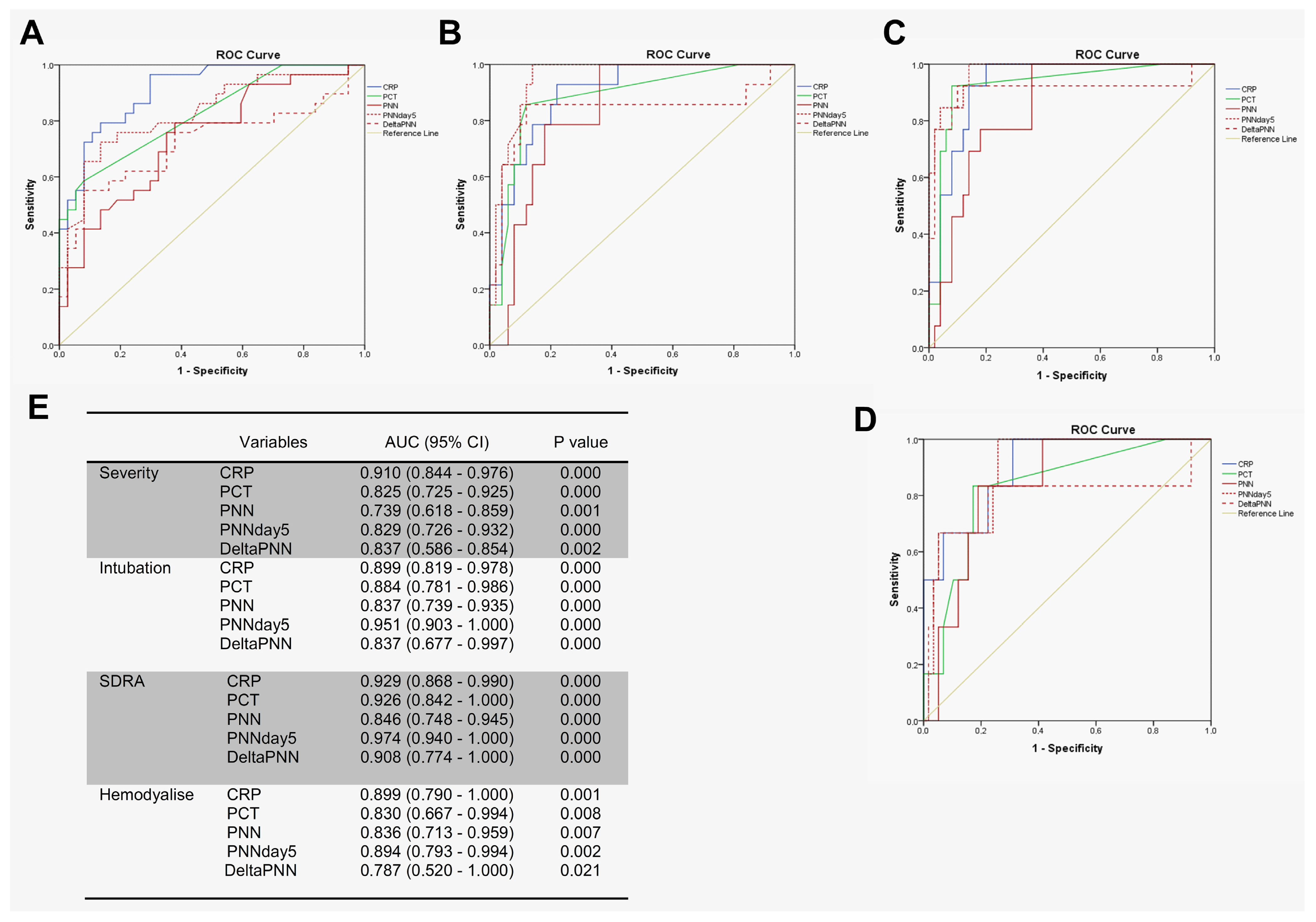
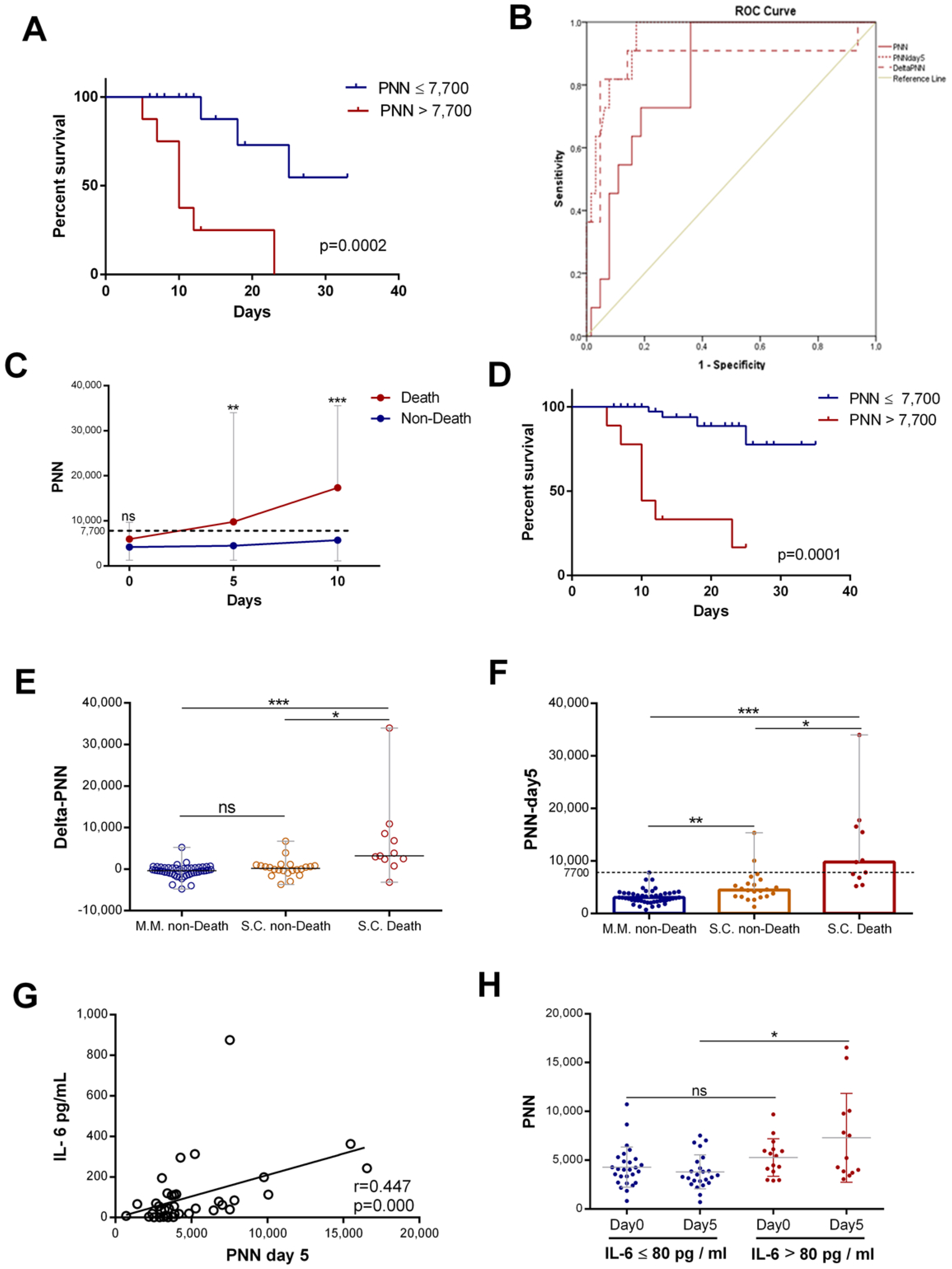
3.4. Neutrophil Counts on Day 5 Appeared to Be Excellent Predictors of Complications During Hospitalization
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ARDS | Acute respiratory distress syndrome |
| AUC | Area under the curve |
| CRP | C-reactive protein |
| CI | Confidence interval |
| COVID-19 | Coronavirus disease 2019 |
| NETs | Extracellular neutrophils traps |
| HB | Hemoglobin |
| ICU | Intensive care unit |
| IL-6 | Interleukin 6 |
| M.M | Mild–moderate |
| PNNs | Neutrophils |
| PNN-day 5 | Neutrophils on day 5 |
| NAR | Neutrophil-to-albumin ratio |
| NLR | Neutrophil-to-lymphocyte ratio |
| OR | Odds ratio |
| PCT | Procalcitonin |
| ROC | Receiver operating characteristic |
| SARS-CoV-2 | Severe Acute Respiratory Syndrome Coronavirus 2 |
| S.C | Severe–critical |
| SE | Standard error |
| WBC | White blood cell |
| WHO | World Health Organization |
References
- Sun, M.; Wu, W.; Liu, Z.; Cong, Y. Microbiota Metabolite Short Chain Fatty Acids, GPCR, and Inflammatory Bowel Diseases. J. Gastroenterol. 2017, 52, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.; Ni, Z.; Hu, Y.; Liang, W.; Ou, C.; He, J.; Liu, L.; Shan, H.; Lei, C.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Lin, S.-H.; Zhao, Y.-S.; Zhou, D.-X.; Zhou, F.-C.; Xu, F. Coronavirus Disease 2019 (COVID-19): Cytokine Storms, Hyper-Inflammatory Phenotypes, and Acute Respiratory Distress Syndrome. Genes Dis. 2020, 7, 520–527. [Google Scholar] [CrossRef] [PubMed]
- Feng, Z.; Yu, Q.; Yao, S.; Luo, L.; Zhou, W.; Mao, X.; Li, J.; Duan, J.; Yan, Z.; Yang, M.; et al. Early Prediction of Disease Progression in COVID-19 Pneumonia Patients with Chest CT and Clinical Characteristics. Nat. Commun. 2020, 11, 4968. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical Features of Patients Infected with 2019 Novel Coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Miyazawa, M. Immunopathogenesis of SARS-CoV-2-Induced Pneumonia: Lessons from Influenza Virus Infection. Inflamm. Regen. 2020, 40, 39. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; Shi, L.; Wang, Y.; Zhang, J.; Huang, L.; Zhang, C.; Liu, S.; Zhao, P.; Liu, H.; Zhu, L.; et al. Pathological Findings of COVID-19 Associated with Acute Respiratory Distress Syndrome. Lancet Respir. Med. 2020, 8, 420–422. [Google Scholar] [CrossRef] [PubMed]
- Sun, S.; Cai, X.; Wang, H.; He, G.; Lin, Y.; Lu, B.; Chen, C.; Pan, Y.; Hu, X. Abnormalities of Peripheral Blood System in Patients with COVID-19 in Wenzhou, China. Clin. Chim. Acta 2020, 507, 174–180. [Google Scholar] [CrossRef] [PubMed]
- Sun, D.; Zhang, D.; Tian, R.; Li, Y.; Wang, Y.; Cao, J.; Tang, Y.; Zhang, N.; Zan, T.; Gao, L.; et al. The Underlying Changes and Predicting Role of Peripheral Blood Inflammatory Cells in Severe COVID-19 Patients: A Sentinel? Clin. Chim. Acta 2020, 508, 122–129. [Google Scholar] [CrossRef]
- Li, X.; Liu, C.; Mao, Z.; Xiao, M.; Wang, L.; Qi, S.; Zhou, F. Predictive Values of Neutrophil-to-Lymphocyte Ratio on Disease Severity and Mortality in COVID-19 Patients: A Systematic Review and Meta-Analysis. Crit. Care 2020, 24, 647. [Google Scholar] [CrossRef]
- Terpos, E.; Ntanasis-Stathopoulos, I.; Elalamy, I.; Kastritis, E.; Sergentanis, T.N.; Politou, M.; Psaltopoulou, T.; Gerotziafas, G.; Dimopoulos, M.A. Hematological Findings and Complications of COVID-19. Am. J. Hematol. 2020, 95, 834–847. [Google Scholar] [CrossRef] [PubMed]
- Qin, C.; Zhou, L.; Hu, Z.; Zhang, S.; Yang, S.; Tao, Y.; Xie, C.; Ma, K.; Shang, K.; Wang, W.; et al. Dysregulation of Immune Response in Patients With Coronavirus 2019 (COVID-19) in Wuhan, China. Clin. Infect. Dis. 2020, 71, 762–768. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Li, Q.; Yin, Y.; Zhang, Y.; Cao, Y.; Lin, X.; Huang, L.; Hoffmann, D.; Lu, M.; Qiu, Y. Excessive Neutrophils and Neutrophil Extracellular Traps in COVID-19. Front. Immunol. 2020, 11, 2063. [Google Scholar] [CrossRef]
- Zheng, Y.; Zhang, Y.; Chi, H.; Chen, S.; Peng, M.; Luo, L.; Chen, L.; Li, J.; Shen, B.; Wang, D. The Hemocyte Counts as a Potential Biomarker for Predicting Disease Progression in COVID-19: A Retrospective Study. Clin. Chem. Lab. Med. (CCLM) 2020, 58, 1106–1115. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus–Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061. [Google Scholar] [CrossRef] [PubMed]
- Soehnlein, O.; Steffens, S.; Hidalgo, A.; Weber, C. Neutrophils as Protagonists and Targets in Chronic Inflammation. Nat. Rev. Immunol. 2017, 17, 248–261. [Google Scholar] [CrossRef] [PubMed]
- Galani, I.E.; Andreakos, E. Neutrophils in Viral Infections: Current Concepts and Caveats. J. Leukoc. Biol. 2015, 98, 557–564. [Google Scholar] [CrossRef] [PubMed]
- Naumenko, V.; Turk, M.; Jenne, C.N.; Kim, S.-J. Neutrophils in Viral Infection. Cell Tissue Res. 2018, 371, 505–516. [Google Scholar] [CrossRef]
- Papayannopoulos, V. Neutrophil Extracellular Traps in Immunity and Disease. Nat. Rev. Immunol. 2018, 18, 134–147. [Google Scholar] [CrossRef] [PubMed]
- Middleton, E.A.; He, X.-Y.; Denorme, F.; Campbell, R.A.; Ng, D.; Salvatore, S.P.; Mostyka, M.; Baxter-Stoltzfus, A.; Borczuk, A.C.; Loda, M.; et al. Neutrophil Extracellular Traps Contribute to Immunothrombosis in COVID-19 Acute Respiratory Distress Syndrome. Blood 2020, 136, 1169–1179. [Google Scholar] [CrossRef]
- Veras, F.P.; Pontelli, M.C.; Silva, C.M.; Toller-Kawahisa, J.E.; De Lima, M.; Nascimento, D.C.; Schneider, A.H.; Caetité, D.; Tavares, L.A.; Paiva, I.M.; et al. SARS-CoV-2–Triggered Neutrophil Extracellular Traps Mediate COVID-19 Pathology. J. Exp. Med. 2020, 217, e20201129. [Google Scholar] [CrossRef]
- Zuo, Y.; Yalavarthi, S.; Shi, H.; Gockman, K.; Zuo, M.; Madison, J.A.; Blair, C.N.; Weber, A.; Barnes, B.J.; Egeblad, M.; et al. Neutrophil Extracellular Traps in COVID-19. JCI Insight 2020, 5, e138999. [Google Scholar] [CrossRef]
- Abraham, E. Neutrophils and Acute Lung Injury. Crit. Care Med. 2003, 31, S195–S199. [Google Scholar] [CrossRef] [PubMed]
- Camp, J.V.; Jonsson, C.B. A Role for Neutrophils in Viral Respiratory Disease. Front. Immunol. 2017, 8, 550. [Google Scholar] [CrossRef] [PubMed]
- Ye, Q.; Wang, B.; Mao, J. The Pathogenesis and Treatment of the ‘Cytokine Storm’ in COVID-19. J. Infect. 2020, 80, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Guan, J.; Wei, X.; Qin, S.; Liu, X.; Jiang, Y.; Chen, Y.; Chen, Y.; Lu, H.; Qian, J.; Wang, Z.; et al. Continuous Tracking of COVID-19 Patients’ Immune Status. Int. Immunopharmacol. 2020, 89, 107034. [Google Scholar] [CrossRef]
- Singh, K.; Mittal, S.; Gollapudi, S.; Butzmann, A.; Kumar, J.; Ohgami, R.S. A Meta-analysis of SARS-CoV-2 Patients Identifies the Combinatorial Significance of D-dimer, C-reactive Protein, Lymphocyte, and Neutrophil Values as a Predictor of Disease Severity. Int. J. Lab. Hematol. 2021, 43, 324–328. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Jiang, M.; Chen, X.; Montaner, L.J. Cytokine Storm and Leukocyte Changes in Mild versus Severe SARS-CoV-2 Infection: Review of 3939 COVID-19 Patients in China and Emerging Pathogenesis and Therapy Concepts. J. Leukoc. Biol. 2020, 108, 17–41. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Zhang, Y.; Mo, P.; Liu, J.; Wang, H.; Wang, F.; Zhao, Q. Neutrophil to CD4+ Lymphocyte Ratio as a Potential Biomarker in Predicting Virus Negative Conversion Time in COVID-19. Int. Immunopharmacol. 2020, 85, 106683. [Google Scholar] [CrossRef]
- Fu, J.; Kong, J.; Wang, W.; Wu, M.; Yao, L.; Wang, Z.; Jin, J.; Wu, D.; Yu, X. The Clinical Implication of Dynamic Neutrophil to Lymphocyte Ratio and D-Dimer in COVID-19: A Retrospective Study in Suzhou China. Thromb. Res. 2020, 192, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Liu, Y.; Xiang, P.; Pu, L.; Xiong, H.; Li, C.; Zhang, M.; Tan, J.; Xu, Y.; Song, R.; et al. Neutrophil-to-Lymphocyte Ratio Predicts Critical Illness Patients with 2019 Coronavirus Disease in the Early Stage. J Transl. Med 2020, 18, 206. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.; Sun, N.-N.; Gao, H.-N.; Chen, Z.-Y.; Yang, Y.; Ju, B.; Tang, L.-L. Risk Factors Analysis of COVID-19 Patients with ARDS and Prediction Based on Machine Learning. Sci. Rep. 2021, 11, 2933. [Google Scholar] [CrossRef]
- Ma, A.; Cheng, J.; Yang, J.; Dong, M.; Liao, X.; Kang, Y. Neutrophil-to-Lymphocyte Ratio as a Predictive Biomarker for Moderate-Severe ARDS in Severe COVID-19 Patients. Crit. Care 2020, 24, 288. [Google Scholar] [CrossRef] [PubMed]
- Varim, C.; Yaylaci, S.; Demirci, T.; Kaya, T.; Nalbant, A.; Dheir, H.; Senocak, D.; Kurt, R.; Cengiz, H.; Karacaer, C. Neutrophil Count to Albumin Ratio as a New Predictor of Mortality in Patients with COVID-19 Infection. Rev. Assoc. Med. Bras. 2020, 66, 77–81. [Google Scholar] [CrossRef] [PubMed]
- Mei, Q.; Wang, A.Y.; Bryant, A.; Yang, Y.; Li, M.; Wang, F.; Zhao, J.W.; Ma, K.; Wu, L.; Chen, H.; et al. Development and Validation of Prognostic Model for Predicting Mortality of COVID-19 Patients in Wuhan, China. Sci. Rep. 2020, 10, 22451. [Google Scholar] [CrossRef] [PubMed]
- Simadibrata, D.M.; Calvin, J.; Wijaya, A.D.; Ibrahim, N.A.A. Neutrophil-to-Lymphocyte Ratio on Admission to Predict the Severity and Mortality of COVID-19 Patients: A Meta-Analysis. Am. J. Emerg. Med. 2021, 42, 60–69. [Google Scholar] [CrossRef]
- Zeng, Z.-Y.; Feng, S.-D.; Chen, G.-P.; Wu, J.-N. Predictive Value of the Neutrophil to Lymphocyte Ratio for Disease Deterioration and Serious Adverse Outcomes in Patients with COVID-19: A Prospective Cohort Study. BMC Infect. Dis. 2021, 21, 80. [Google Scholar] [CrossRef] [PubMed]
- Hashizume, M.; Higuchi, Y.; Uchiyama, Y.; Mihara, M. IL-6 Plays an Essential Role in Neutrophilia under Inflammation. Cytokine 2011, 54, 92–99. [Google Scholar] [CrossRef]
- Mateer, S.W.; Mathe, A.; Bruce, J.; Liu, G.; Maltby, S.; Fricker, M.; Goggins, B.J.; Tay, H.L.; Marks, E.; Burns, G.; et al. IL-6 Drives Neutrophil-Mediated Pulmonary Inflammation Associated with Bacteremia in Murine Models of Colitis. Am. J. Pathol. 2018, 188, 1625–1639. [Google Scholar] [CrossRef] [PubMed]
- Herold, T.; Jurinovic, V.; Arnreich, C.; Lipworth, B.J.; Hellmuth, J.C.; Von Bergwelt-Baildon, M.; Klein, M.; Weinberger, T. Elevated Levels of IL-6 and CRP Predict the Need for Mechanical Ventilation in COVID-19. J. Allergy Clin. Immunol. 2020, 146, 128–136.e4. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Variables | Mild–Moderate (n = 83) | Severe–Critical (n = 36) | p-Value |
|---|---|---|---|
| Age, mean (SD), y | 44 (16) | 66 (11) | 0.003 |
| Male, no. (%) | 37 (44.6) | 29 (80.6) | 0.000 |
| Clinical symptoms, no. (%) | |||
| Asthenia | 2 (2.4) | 20 (55.6) | 0.000 |
| Fever | 30 (36.1) | 22 (68.8) | 0.002 |
| Headache | 13 (15.7) | 5 (15.6) | 0.996 |
| Gough | 34 (41) | 17 (53.1) | 0.239 |
| Dyspnea | 15 (18.1) | 22 (66.7) | 0.000 |
| Vomiting | 16 (19.5) | 6 (18.2) | 0.87 |
| Diarrhea | 17 (20.5) | 10 (31.2) | 0.22 |
| Ageusia | 16 (19.5) | 5 (15.6) | 0.63 |
| Past medical history, no. (%) | |||
| Asthma | 5 (6) | 5 (13.9) | 0.155 |
| Cardiac disease | 3 (3.6) | 11 (30.6) | 0.000 |
| Diabetes | 7 (8.4) | 10 (27.8) | 0.006 |
| Renal failure | 0 | 2 (5.6) | 0.03 |
| Autoimmune disease | 3 (3.6) | 3 (8.3) | 0.28 |
| Smoking | 4 (4.8) | 2 (5.6) | 0.866 |
| Complications | |||
| ARDS | 0 | 13 (40.6) | 0.000 |
| Arterial hypertension | 0 | 7 (23.3) | 0.000 |
| Hemodialysis | 0 | 8 (24.2) | 0.000 |
| Mortality | 0 | 13 (39.4) | 0.000 |
| Mortality | ||
|---|---|---|
| OR (95% CI) | p-Value | |
| Neutrophils on day 5 | 1.001 (1.00–1.001) | 0.020 |
| Neutrophils | 0.999 (0.998–1.001) | 0.360 |
| NLR | 0.998 (0.992–1.004) | 0.525 |
| CRP | 1.010 (0.985–1.036) | 0.432 |
| PCT | 4.655 (0.044–367.372) | 0.519 |
| HB | 1.707 (0.650–4.481) | 0.278 |
| Creatinine | 0.958 (0.671–1.366) | 0.811 |
| Age | 1.021 (0.944–1.104) | 0.609 |
| Variable | Parameter | B | SE | p | OR (95% CI) |
|---|---|---|---|---|---|
| Mortality | PNN-day 5 | 3.572 | 0.862 | 0.000 | 35.583 (6.573–192.644) |
| ARDS | PNN-day 5 | 3.854 | 0.918 | 0.000 | 47.200 (7.814–285.092) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
El Azhary, K.; Ghazi, B.; Kouhen, F.; El Bakkouri, J.; Chamlal, H.; El Ghanmi, A.; Badou, A. Clinical Impact of Neutrophil Variation on COVID-19 Complications. Diagnostics 2025, 15, 457. https://doi.org/10.3390/diagnostics15040457
El Azhary K, Ghazi B, Kouhen F, El Bakkouri J, Chamlal H, El Ghanmi A, Badou A. Clinical Impact of Neutrophil Variation on COVID-19 Complications. Diagnostics. 2025; 15(4):457. https://doi.org/10.3390/diagnostics15040457
Chicago/Turabian StyleEl Azhary, Khadija, Bouchra Ghazi, Fadila Kouhen, Jalila El Bakkouri, Hasna Chamlal, Adil El Ghanmi, and Abdallah Badou. 2025. "Clinical Impact of Neutrophil Variation on COVID-19 Complications" Diagnostics 15, no. 4: 457. https://doi.org/10.3390/diagnostics15040457
APA StyleEl Azhary, K., Ghazi, B., Kouhen, F., El Bakkouri, J., Chamlal, H., El Ghanmi, A., & Badou, A. (2025). Clinical Impact of Neutrophil Variation on COVID-19 Complications. Diagnostics, 15(4), 457. https://doi.org/10.3390/diagnostics15040457