
Cladosporium species novum Invasive Pulmonary Infection in a Patient with Post-COVID-19 Syndrome and AIDS

 , , , , , and
, , , , , and 
Abstract
1. Introduction
2. Case Report
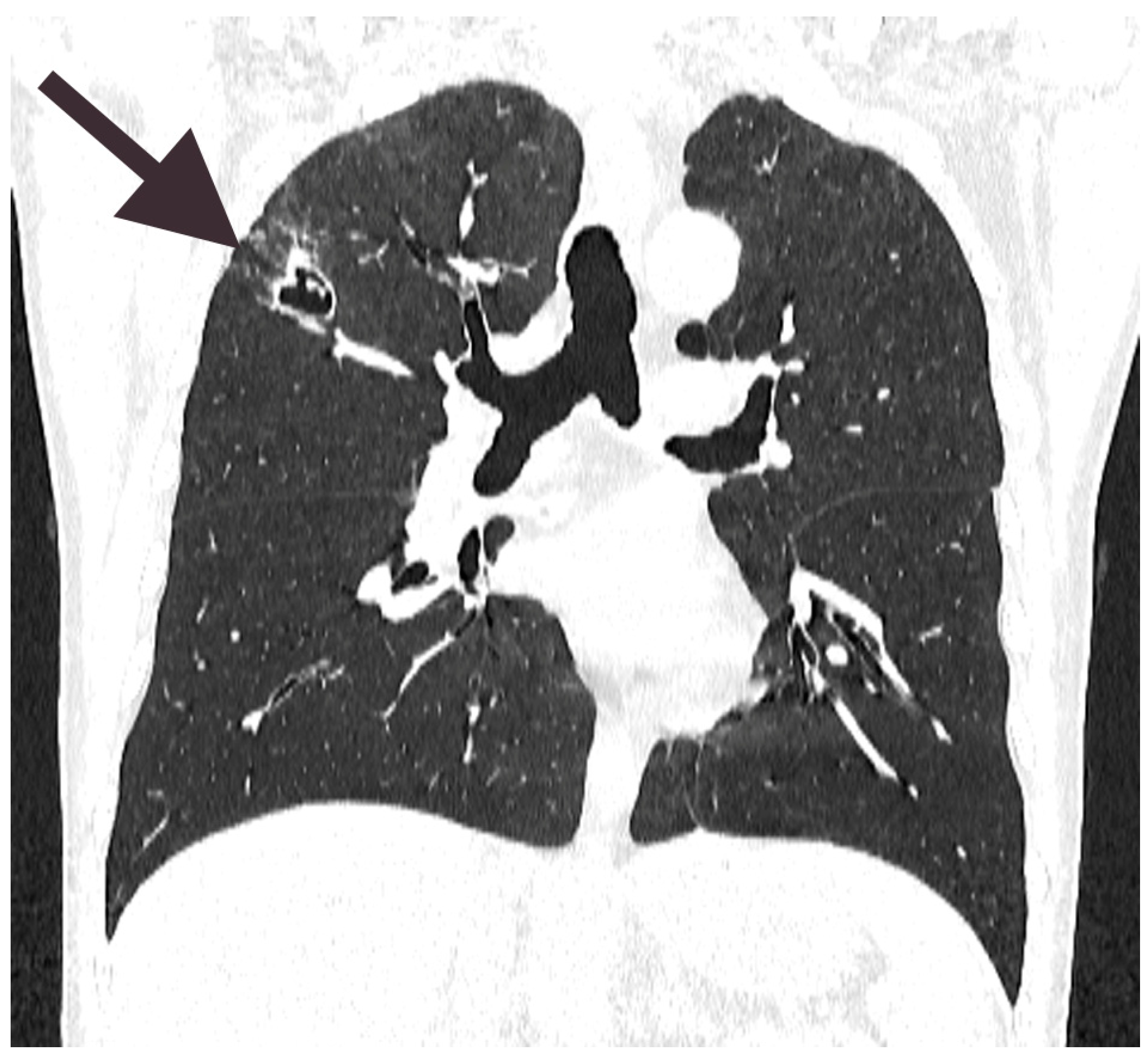
2.1. Patient’s Medical History and Clinical Course of the Disease
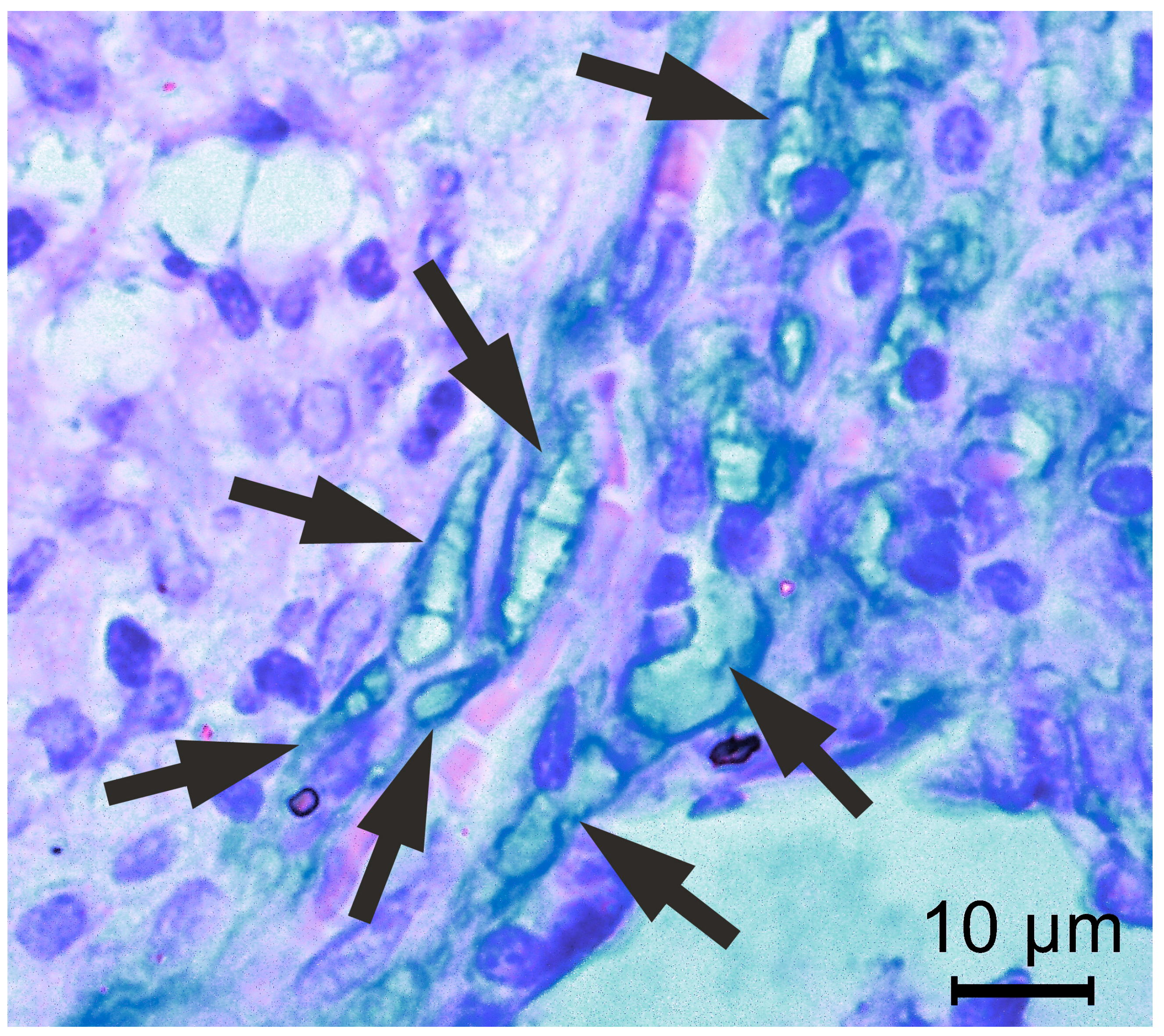
2.2. Histopathology
2.3. Follow-Up with Progression of the Disease and Treatment
2.4. DNA Extraction, PCR Amplification, and Sequencing
2.5. Bioinformatics Approach and Alignments
2.6. Follow-Up
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chan, K.S.; Lai, C.C.; Yu, W.L.; Chao, C.M. COVID-19 Associated with Cryptococcosis: A New Challenge during the Pandemic. JoF 2022, 8, 1111. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, R.; Sehgal, I.S.; Muthu, V.; Denning, D.W.; Chakrabarti, A.; Soundappan, K.; Garg, M.; Rudramurthy, S.M.; Dhooria, S.; Armstrong-James, D.; et al. Revised ISHAM-ABPA working group clinical practice guidelines for diagnosing, classifying and treating allergic bronchopulmonary aspergillosis/mycoses. Eur. Respir. J. 2024, 63, 2400061. [Google Scholar] [CrossRef] [PubMed]
- Chinn, S.; Burney, P.; Sunyer, J.; Jarvis, D.; Luczynska, C.; On Behalf Of The European Community Respiratory Health Survey. Sensitization to individual allergens and bronchial responsiveness in the ECRHS. Eur. Respir. J. 1999, 14, 876. [Google Scholar] [CrossRef]
- Marvisi, M.; Balzarini, L.; Mancini, C.; Mouzakiti, P. A new type of Hypersensitivity Pneumonitis: Salami brusherâ€TMs disease. Monaldi Arch. Chest Dis. 2015, 77, 35–37. Available online: https://www.monaldi-archives.org/index.php/macd/article/view/167 (accessed on 14 March 2025). [CrossRef]
- Xuan, R.; Hong, S.C.; Trinh, T.; Coroneo, M.T.; Petsoglou, C. Case Series of Rare Fungal Keratitides: Experiences from a Quaternary Eye Hospital in Sydney, Australia. JoF 2023, 9, 589. [Google Scholar] [CrossRef]
- Sandoval-Denis, M.; Gené, J.; Sutton, D.A.; Wiederhold, N.P.; Cano-Lira, J.F.; Guarro, J. New species of Cladosporium associated with human and animal infections. Pers.-Int. Mycol. J. 2016, 36, 281–298. [Google Scholar] [CrossRef]
- Tasic, S.; Miladinovic-Tasic, N. Cladosporium spp.—Cause of opportunistic mycoses. Acta Fac. Medicae Naissensis 2007, 24, 15–19. [Google Scholar]
- Castro, A.S.; Oliveira, A.; Lopes, V. Pulmonary phaeohyphomycosis: A challenge to the clinician. Eur. Respir. Rev. 2013, 22, 187–188. [Google Scholar] [CrossRef]
- Kaneda, M.; Nagaoka, K.; Kawasuji, H.; Matsunaga, K.; Inomata, M.; Miyazaki, Y.; Nakashima, A.; Yamamoto, Y. Pulmonary abscess caused by Cladosporium cladosporioides after receiving outpatient chemotherapy. J. Infect. Chemother. 2023, 29, 993–996. [Google Scholar] [CrossRef]
- Vacher, G.; Niculita-Hirzel, H.; Roger, T. Immune responses to airborne fungi and non-invasive airway diseases. Semin. Immunopathol. 2015, 37, 83–96. [Google Scholar] [CrossRef]
- Denning, D.W.; Chakrabarti, A. Pulmonary and sinus fungal diseases in non-immunocompromised patients. Lancet Infect. Dis. 2017, 17, e357–e366. [Google Scholar] [CrossRef] [PubMed]
- Hughes, K.M.; Price, D.; Torriero, A.A.J.; Symonds, M.R.E.; Suphioglu, C. Impact of Fungal Spores on Asthma Prevalence and Hospitalization. Int. J. Mol. Sci. 2022, 23, 4313. [Google Scholar] [CrossRef] [PubMed]
- Nasiri-Jahrodi, A.; Sheikholeslami, F.M.; Barati, M. Cladosporium tenuissimum-induced sinusitis in a woman with immune-deficiency disorder. Braz. J. Microbiol. 2023, 54, 637–643. [Google Scholar] [CrossRef]
- Oliveira, M.; Oliveira, D.; Lisboa, C.; Boechat, J.; Delgado, L. Clinical Manifestations of Human Exposure to Fungi. JoF 2023, 9, 381. [Google Scholar] [CrossRef]
- Xu, X.; Ding, F.; Hu, X.; Yang, F.; Zhang, T.; Dong, J.; Xue, Y.; Liu, T.; Wang, J.; Jin, Q. Upper respiratory tract mycobiome alterations in different kinds of pulmonary disease. Front. Microbiol. 2023, 14, 1117779. [Google Scholar] [CrossRef]
- Denning, D.W.; O’Driscoll, B.R.; Hogaboam, C.M.; Bowyer, P.; Niven, R.M. The link between fungi and severe asthma: A summary of the evidence. Eur. Respir. J. 2006, 27, 615–626. [Google Scholar] [CrossRef]
- Sharpe, R.A.; Bearman, N.; Thornton, C.R.; Husk, K.; Osborne, N.J. Indoor fungal diversity and asthma: A meta-analysis and systematic review of risk factors. J. Allergy Clin. Immunol. 2015, 135, 110–122. [Google Scholar] [CrossRef]
- Obeagu, E.I.; Onuoha, E.C. Tuberculosis among HIV patients: A review of Prevalence and Associated Factors. Int. J. Adv. Res. Biol. Sci. 2023, 10, 128–134. [Google Scholar]
- Brown, G.D.; Denning, D.W.; Gow, N.A.R.; Levitz, S.M.; Netea, M.G.; White, T.C. Hidden Killers: Human Fungal Infections. Sci. Transl. Med. 2012, 4, 165rv13. [Google Scholar] [CrossRef]
- Levin, T.P.; Baty, D.E.; Fekete, T.; Truant, A.L.; Suh, B. Cladophialophora bantiana Brain Abscess in a Solid-Organ Transplant Recipient: Case Report and Review of the Literature. J. Clin. Microbiol. 2004, 42, 4374–4378. [Google Scholar] [CrossRef]
- Chakrabarti, A.; Kaur, H.; Rudramurthy, S.M.; Appannanavar, S.B.; Patel, A.; Mukherjee, K.K.; Ghosh, A.; Ray, U. Brain abscess due to Cladophialophora bantiana: A review of 124 cases. Med. Mycol. 2016, 54, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Garzoni, C.; Markham, L.; Bijlenga, P.; Garbino, J. Cladophialophora bantiana: A rare cause of fungal brain abscess. Clinical aspects and new therapeutic options. Med. Mycol. 2008, 46, 481–486. [Google Scholar] [CrossRef] [PubMed]
- Lortholary, O.; Garcia-Hermoso, D.; Sturny-Leclère, A.; Sitbon, K.; Nourrisson, C.; Letscher-Bru, V.; Desbois-Nogard, N.; Bani-Sadr, F.; Bastides, F.; Bienvenu, B.; et al. Reappraising Cladophialophora bantiana phaeohyphomycosis in France: Retrospective nation-based study. Lancet Microbe 2024, 5, 100907. [Google Scholar] [CrossRef] [PubMed]
- The Advisory Committee on Dangerous Pathogens (ACDP). The Approved List of Biological Agents, 5th ed.; Health and Safety Executive (HSE): Bootle, UK, 2023. [Google Scholar]
- Tashiro, M.; Takazono, T.; Izumikawa, K. Overview of Fungi Classified as Risk Group 3 by the Japanese Society for Medical Mycology. Med. Mycol. J. 2024, 65, 99–102. [Google Scholar] [CrossRef]
- Hien, H.T.A.; Thanh, T.T.; Thu, N.T.M.; Nguyen, A.; Thanh, N.T.; Lan, N.P.H.; Simmons, C.; Shikuma, C.; Chau, N.V.V.; Thwaites, G.; et al. Development and evaluation of a real-time polymerase chain reaction assay for the rapid detection of Talaromyces marneffei MP1 gene in human plasma. Mycoses 2016, 59, 773–780. [Google Scholar] [CrossRef]
- Skiada, A.; Pavleas, I.; Drogari-Apiranthitou, M. Rare fungal infectious agents: A lurking enemy. F1000Research 2017, 6, 1917. [Google Scholar] [CrossRef]
- White, T.J.; Bruns, T.; Lee, S.; Taylor, J. Amplification and Direct Sequencing of Fungal Ribosomal Rna Genes for Phylogenetics. In PCR Protocols: A Guide to Methods and Applications; Sninsky, J., White, T., Eds.; Academic Press: San Diego, CA, USA, 1989; pp. 315–322. [Google Scholar]
- Muñoz-Cadavid, C.; Rudd, S.; Zaki, S.R.; Patel, M.; Moser, S.A.; Brandt, M.E.; Gómez, B.L. Improving Molecular Detection of Fungal DNA in Formalin-Fixed Paraffin-Embedded Tissues: Comparison of Five Tissue DNA Extraction Methods Using Panfungal PCR. J. Clin. Microbiol. 2010, 48, 2147–2153. [Google Scholar] [CrossRef]
- Wang, R.J.; Miller, R.F.; Huang, L. Approach to Fungal Infections in Human Immunodeficiency Virus–Infected Individuals. Clin. Chest Med. 2017, 38, 465–477. [Google Scholar] [CrossRef]
- Brischetto, A.; Kidd, S.; Baird, R. First Reported Australian Case of Cladophilophora arxii: Features Consistent with Possible Primary Pulmonary Chromoblastomycosis. Am. Soc. Trop. Med. Hyg. 2015, 92, 791–793. [Google Scholar] [CrossRef]
- Binford, C.H.; Dooley, J.R. Diseases caused by fungi and actinomycetes-Deep mycoses. In Pathology of Tropical and Extraordinary Diseases; AFIP: Washington, DC, USA, 1976; pp. 587–588. [Google Scholar]
- Suleiman, A.S.; Islam, M.A.; Akter, M.S.; Amin, M.R.; Werkneh, A.A.; Bhattacharya, P. A meta-meta-analysis of co-infection, secondary infections, and antimicrobial resistance in COVID-19 patients. J. Infect. Public Health 2023, 16, 1562–1590. [Google Scholar] [CrossRef]
- Scendoni, R.; Bury, E.; Ribeiro, I.L.A.; Cingolani, M.; Cameriere, R.; De Benedictis, A.; De Micco, F. Leading Pathogens Involved in Co-Infection and Super-Infection with COVID-19: Forensic Medicine Considerations after a Systematic Review and Meta-Analysis. Pathogens 2023, 12, 646. [Google Scholar] [CrossRef] [PubMed]
- Ulloque-Badaracco, J.R.; Copaja-Corzo, C.; Hernandez-Bustamante, E.A.; Cabrera-Guzmán, J.C.; Huayta-Cortez, M.A.; Carballo-Tello, X.L.; Seminario-Amez, R.A.; Hueda-Zavaleta, M.; Benites-Zapata, V.A. Fungal infections in patients after recovering from COVID-19: A systematic review. Ther. Adv. Infect. 2024, 11, 20499361241242963. [Google Scholar] [CrossRef] [PubMed]
- De León-Borrás, R.; DelPilar-Morales, E.; Rivera-Pérez, N.; Pallens-Feliciano, M.; Tirado-Gómez, M.; González-Sepúlveda, L.; Bertrán-Pasarell, J. Factors Associated to Invasive Fungal Infection in Hispanic Patients with Hematological Malignancies. Bol. Asoc. Med. P. R. 2017, 109, 43–48. [Google Scholar]
- Ren, P.; Sridhar, S.; Chaturvedi, V. Use of Paraffin-Embedded Tissue for Identification of Saccharomyces cerevisiae in a Baker’s Lung Nodule by Fungal PCR and Nucleotide Sequencing. J. Clin. Microbiol. 2004, 42, 2840–2842. [Google Scholar] [CrossRef] [PubMed]
- Guarner, J.; Brandt, M.E. Histopathologic Diagnosis of Fungal Infections in the 21st Century. Clin. Microbiol. Rev. 2011, 24, 247–280. [Google Scholar] [CrossRef]
- Batra, N.; Kaur, H.; Mohindra, S.; Singh, S.; Shamanth, A.S.; Rudramurthy, S.M. Cladosporium sphaerospermum causing brain abscess, a saprophyte turning pathogen: Case and review of published reports. J. Mycol. Méd. 2019, 29, 180–184. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Before 1st Surgery | Before 2nd Surgery | Reference Range |
|---|---|---|---|
| RBC | 4.65 × 1012/L | 4.24 × 1012/L | 3.8–5.63 × 1012/L |
| Hgb | 134 g/L | 126 g/L | 125–175 g/L |
| Hct | 0.408 1/L | 0.380 1/L | 0.367–0.53 1/L |
| MCV | 88 fL | 90 fL | 80–100 fL |
| MCH | 28.7 pg | 29.7 pg | 27.4–33.9 pg |
| MCHC | 328 g/L | 332 g/L | 320–360 g/L |
| WBC | 4.2 × 109/L | 2.8 × 109/L | 4–11 × 109/L |
| Neu % | 51% | 75% | 44–75% |
| Neu # | 2.11 × 109/L | 2.14 × 109/L | 2.0–7.6 × 109/L |
| Lym % | 34% | 12% | 20–46% |
| Lym # | 1.4 × 109/L | 0.35 × 109/L | 1.0–4.5 × 109/L |
| Mon % | 12% | 12% | 2–12% |
| Mon # | 0.48 × 109/L | 0.33 × 109/L | 0.2–0.8 × 109/L |
| Eos % | 3.4% | 0.3% | 0.1–7% |
| Eos # | 0.14 × 109/L | 0.01 × 109/L | 0.1–0.6 × 109/L |
| Bas % | 0.6% | 0.4% | 0.2–2% |
| Bas # | 0.02 × 109/L | 0.01 × 109/L | 0.0–0.20 × 109/L |
| Plt | 239 × 109/L | 190 × 109/L | 150–450 × 109/L |
| Sequence ID | Organism | Host | Isolation Source | Location | Accession Number |
|---|---|---|---|---|---|
| C1 | Cladosporium spp. | Homo sapiens | Lungs | Serbia | PQ067362 |
| No | Organism | Query Cover | E-Value | Percentage Identity | No |
|---|---|---|---|---|---|
| 1. | Cladosporium herbarum, isolate ZS9–10 | 100% | 1 × 10−147 | 98.68% | OR884130.1 |
| 2. | Cladosporium tenuissimum, isolate TJU_JAN24 | 100% | 1 × 10−147 | 98.68% | OM237137.1 |
| 3. | Cladosporium tenuissimum, isolate TJU_JAN7 | 100% | 1 × 10−147 | 98.68% | OM237120.1 |
| 4. | Cladosporium cladosporioides, isolate TJU_JAN44 | 99% | 5 × 10−147 | 98.68% | OM237156.1 |
| 5. | Cladosporium oryzae, isolate TJU_JAN21 | 99% | 5 × 10−147 | 98.68% | OM237134.1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bijelović, M.; Gardić, N.; Lovrenski, A.; Petrović, D.; Kozoderović, G.; Lalošević, V.; Vračar, V.; Lalošević, D. Cladosporium species novum Invasive Pulmonary Infection in a Patient with Post-COVID-19 Syndrome and AIDS. Diagnostics 2025, 15, 781. https://doi.org/10.3390/diagnostics15060781
Bijelović M, Gardić N, Lovrenski A, Petrović D, Kozoderović G, Lalošević V, Vračar V, Lalošević D. Cladosporium species novum Invasive Pulmonary Infection in a Patient with Post-COVID-19 Syndrome and AIDS. Diagnostics. 2025; 15(6):781. https://doi.org/10.3390/diagnostics15060781
Chicago/Turabian StyleBijelović, Milorad, Nikola Gardić, Aleksandra Lovrenski, Danijela Petrović, Gordana Kozoderović, Vesna Lalošević, Vuk Vračar, and Dušan Lalošević. 2025. "Cladosporium species novum Invasive Pulmonary Infection in a Patient with Post-COVID-19 Syndrome and AIDS" Diagnostics 15, no. 6: 781. https://doi.org/10.3390/diagnostics15060781
APA StyleBijelović, M., Gardić, N., Lovrenski, A., Petrović, D., Kozoderović, G., Lalošević, V., Vračar, V., & Lalošević, D. (2025). Cladosporium species novum Invasive Pulmonary Infection in a Patient with Post-COVID-19 Syndrome and AIDS. Diagnostics, 15(6), 781. https://doi.org/10.3390/diagnostics15060781