
Effectiveness and Safety of Transforaminal Spinal Endoscopy: Analysis of 1000 Clinical Cases

 ,
,
Abstract
1. Introduction
2. Material and Method
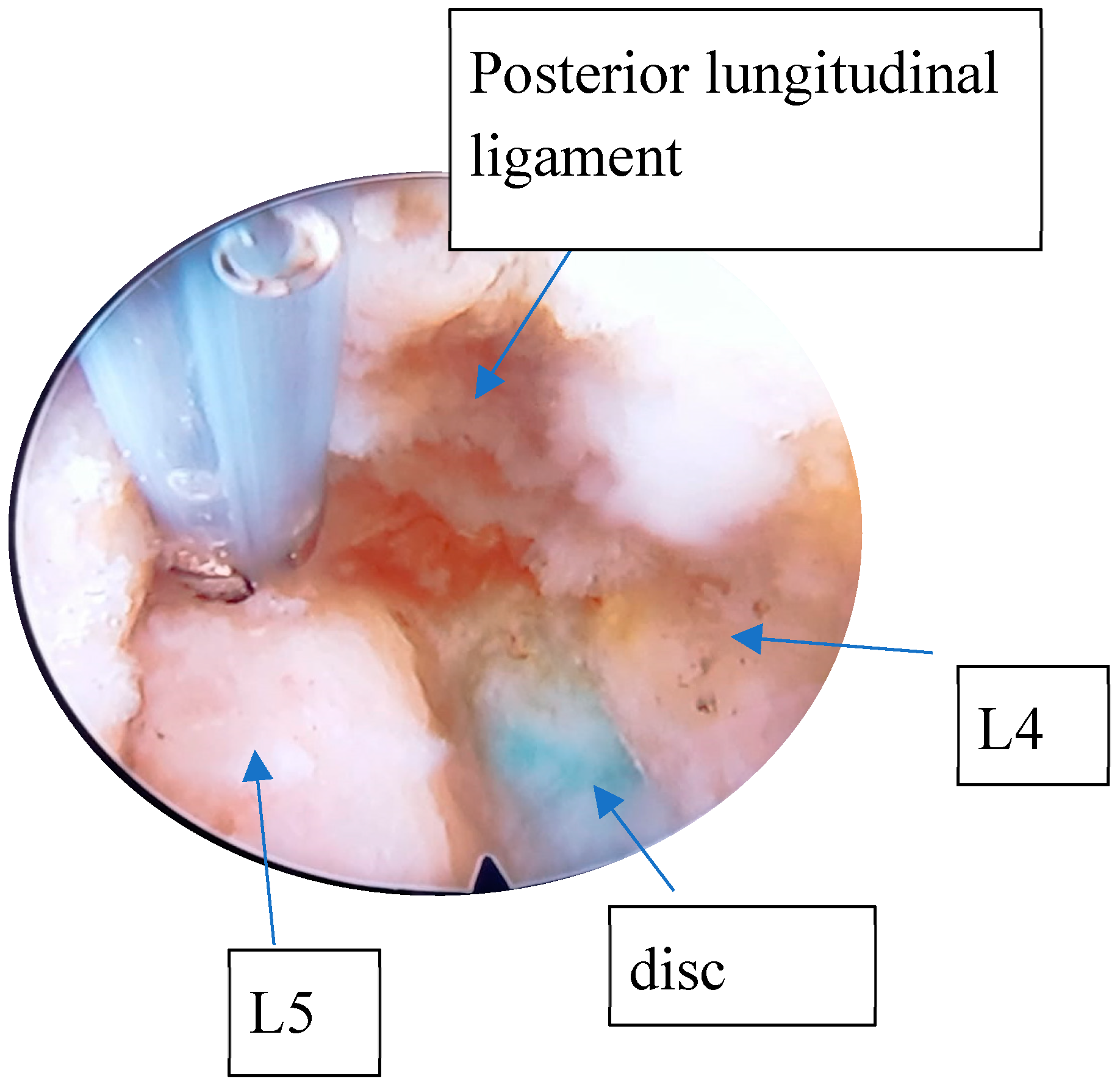
2.1. Surgical Method (L1/L5) for Transforaminal Endoscopic Discectomy
2.2. The Positioning of Patient for L5-S1 Endoscopic Discectomy
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yoon, W.W.; Koch, J. Herniated discs: When is surgery necessary? EFORT Open Rev. 2021, 6, 526–530. [Google Scholar] [CrossRef] [PubMed]
- Amin, R.M.; Andrade, N.S.; Neuman, B.J. Lumbar disc herniation. Curr. Rev. Musculoskelet. Med. 2017, 10, 507–516. [Google Scholar] [CrossRef] [PubMed]
- Weber, H.; Holme, I.; Amlie, E. The natural course of acute sciatica with nerve root symptoms in a double-blind placebo-controlled trial evaluating the effect of piroxicam. Spine 1993, 18, 1433–1438. [Google Scholar] [CrossRef]
- Peul, W.C.; van Houwelingen, H.C.; Hout, W.B.v.D.; Brand, R.; Eekhof, J.A.; Tans, J.T.; Thomeer, R.T.; Koes, B.W. Leiden-The Hague Spine Intervention Prognostic Study Group. Surgery versus prolonged conservative treatment for sciatica. N. Engl. J. Med. 2007, 356, 2245–2256. [Google Scholar] [CrossRef]
- Bailey, C.S.; Rasoulinejad, P.; Taylor, D.; Sequeira, K.; Miller, T.; Watson, J.; Rosedale, R.; Bailey, S.I.; Gurr, K.R.; Siddiqi, F.; et al. Surgery versus Conservative Care for Persistent Sciatica Lasting 4 to 12 Months. N. Engl. J. Med. 2020, 382, 1093–1102. [Google Scholar] [CrossRef]
- Pan, M.; Li, Q.; Li, S.; Mao, H.; Meng, B.; Zhou, F.; Yang, H. Percutaneous endoscopic lumbar discectomy: Indications and complications. Pain Physician 2020, 23, 49–56. [Google Scholar] [CrossRef]
- Jarebi, M.; Awaf, A.; Lefranc, M.; Peltier, J. A matched comparison of outcomes between percutaneous endoscopic lumbar discectomy and open lumbar microdiscectomy for the treatment of lumbar disc herniation: A 2-year retrospective cohort study. Spine J. 2021, 21, 114–121. [Google Scholar] [CrossRef]
- Nie, H.; Zeng, J.; Song, Y.; Chen, G.; Wang, X.; Li, Z.; Jiang, H.; Kong, Q. Percutaneous endoscopic lumbar discectomy for l5–s1 disc herniation via an interlaminar approach versus a transforaminal approach: A prospective randomized controlled study with 2-year follow up. Spine 2016, 41 (Suppl. S19), B30–B37. [Google Scholar] [CrossRef]
- Kambin, P.; Brager, M.D. Percutaneous posterolateral discectomy. Anatomy and mechanism. Clin. Orthop. Relat. Res. 1987, 223, 145–154. [Google Scholar] [CrossRef]
- Schubert, M.; Hoogland, T. Endoscopic transforaminal nucleotomy with foraminoplasty for lumbar disk herniation. Oper. Orthop. Traumatol. 2005, 17, 641–661. [Google Scholar] [CrossRef]
- Gadjradj, P.S.; Rubinstein, S.M.; Peul, W.C.; Depauw, P.R.; Vleggeert-Lankamp, C.L.; Seiger, A.; van Susante, J.L.; de Boer, M.R.; van Tulder, M.W.; Harhangi, B.S. Full endoscopic versus open discectomy for sciatica: Randomised controlled non-inferiority trial. BMJ 2022, 376, e065846. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Carlisle, E.; Luna, M.; Tsou, P.M.; Wang, J.C. Percent spinal canal compromise on MRI utilized for predicting the need for surgical treatment in single-level lumbar intervertebral disc herniation. Spine J. 2005, 5, 608–614. [Google Scholar] [CrossRef] [PubMed]
- Boden, S.D.; Davis, D.O.; Dina, T.S.; Patronas, N.J.; Wiesel, S.W. Abnormal magnetic-resonance scans of the lumbar spine in asymptomatic subjects: A prospective investigation. J. Bone Joint Surg. Am. 1990, 72, 403–408. [Google Scholar] [CrossRef] [PubMed]
- Borenstein, D.G.; O’Mara, J.W., Jr.; Boden, S.D.; Lauerman, W.C.; Jacobson, A.; Platenberg, C.; Schellinger, D.; Wiesel, S.W. The value of magnetic resonance imaging of the lumbar spine to predict low-back pain in asymptomatic subjects: A seven-year follow-up study. J. Bone Joint Surg. Am. 2001, 83, 1306–1311. [Google Scholar] [CrossRef]
- Eun, S.S.; Lee, S.-H.; Sabal, L.A. Long-term follow-up results of percutaneous endoscopic lumbar discectomy. Pain Phys. 2016, 19, E1161–E1166. [Google Scholar]
- Choi, K.-C.; Shim, H.-K.; Hwang, J.-S.; Shin, S.H.; Lee, D.C.; Jung, H.H.; Park, H.A.; Park, C.-K. Comparison of surgical invasiveness between microdiscectomy and 3 different endoscopic discectomy techniques for lumbar disc herniation. World Neurosurg. 2018, 116, e750–e758. [Google Scholar] [CrossRef]
- Gadjradj, P.S.; Harhangi, B.S.; Amelink, J.B.; van Susante, J.; Kamper, S.; van Tulder, M.; Peul, W.C.; Vleggeert-Lankamp, C.; Rubinstein, S.M. Percutaneous Transforaminal Endoscopic Discectomy Versus Open Microdiscectomy for Lumbar Disc Herniation: A Systematic Review and Meta-analysis. Spine 2021, 46, 538–549. [Google Scholar] [CrossRef]
- Gibson, J.N.A.; Subramanian, A.S.; Scott, C.E.H. A randomised controlled trial of transforaminal endoscopic discectomy vs microdiscectomy. Eur. Spine J. 2017, 26, 847–856. [Google Scholar] [CrossRef]
- Singh, R.; Zeng Xin, G.; Hirachan, M.P.; Yu Cheng, L. Outcome of percutaneous Transforaminal endoscopic lumbar surgery in >60-year-old patients with low Back pain. Asian Spine J. 2018, 12, 511–517. [Google Scholar] [CrossRef]
- Liu, X.; Yuan, S.; Tian, Y.; Wang, L.; Gong, L.; Zheng, Y.; Li, J. Comparison of percutaneous endoscopic transforaminal discectomy, microendoscopic discectomy, and microdiscectomy for symptomatic lumbar disc herniation: Minimum 2-year follow-up results. J. Neurosurg. Spine 2018, 28, 317–325. [Google Scholar] [CrossRef]
- Ahn, S.S.; Kim, S.H.; Kim, D.W. Learning curve of percutaneous endoscopic lumbar discectomy based on the period (early vs. late) and technique (in-and-out vs. in-and-out-and-in): A retrospective comparative study. J. Korean Neurosurg. Soc. 2015, 58, 539–546. [Google Scholar] [CrossRef] [PubMed]
- Xie, P.; Feng, F.; Chen, Z.; He, L.; Yang, B.; Chen, R.; Wu, W.; Liu, B.; Dong, J.; Shu, T.; et al. Percutaneous transforaminal full endoscopic decompression for the treatment of lumbar spinal stenosis. BMC Musculoskelet. Disord. 2020, 21, 546. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| neurogenic intermittent claudication | potential mental illness |
| radicular irritation with or without sensory loss | multilevel lumbar spinal stenosis |
| concordant imaging diagnosis of lumbar stenosis or spinal disc herniation | severe scoliosis |
| failure of conservative treatment for at least 3 months | patient with spinal/vertebral tumour or vertebral tumor |
| age between 30 and 60 | active neoplastic systemic pathologies |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tornatore, I.; Basile, A.; Aureli, A.; Tarantino, A.; Orlando, G.; Buharaja, R. Effectiveness and Safety of Transforaminal Spinal Endoscopy: Analysis of 1000 Clinical Cases. Diagnostics 2025, 15, 1021. https://doi.org/10.3390/diagnostics15081021
Tornatore I, Basile A, Aureli A, Tarantino A, Orlando G, Buharaja R. Effectiveness and Safety of Transforaminal Spinal Endoscopy: Analysis of 1000 Clinical Cases. Diagnostics. 2025; 15(8):1021. https://doi.org/10.3390/diagnostics15081021
Chicago/Turabian StyleTornatore, Ignazio, Attilio Basile, Alessandro Aureli, Alessio Tarantino, Giuseppe Orlando, and Rodrigo Buharaja. 2025. "Effectiveness and Safety of Transforaminal Spinal Endoscopy: Analysis of 1000 Clinical Cases" Diagnostics 15, no. 8: 1021. https://doi.org/10.3390/diagnostics15081021
APA StyleTornatore, I., Basile, A., Aureli, A., Tarantino, A., Orlando, G., & Buharaja, R. (2025). Effectiveness and Safety of Transforaminal Spinal Endoscopy: Analysis of 1000 Clinical Cases. Diagnostics, 15(8), 1021. https://doi.org/10.3390/diagnostics15081021