

Airflow and Pressure Design Review of Modular Negative Pressure Wards


Abstract
:1. Introduction
2. Research Method
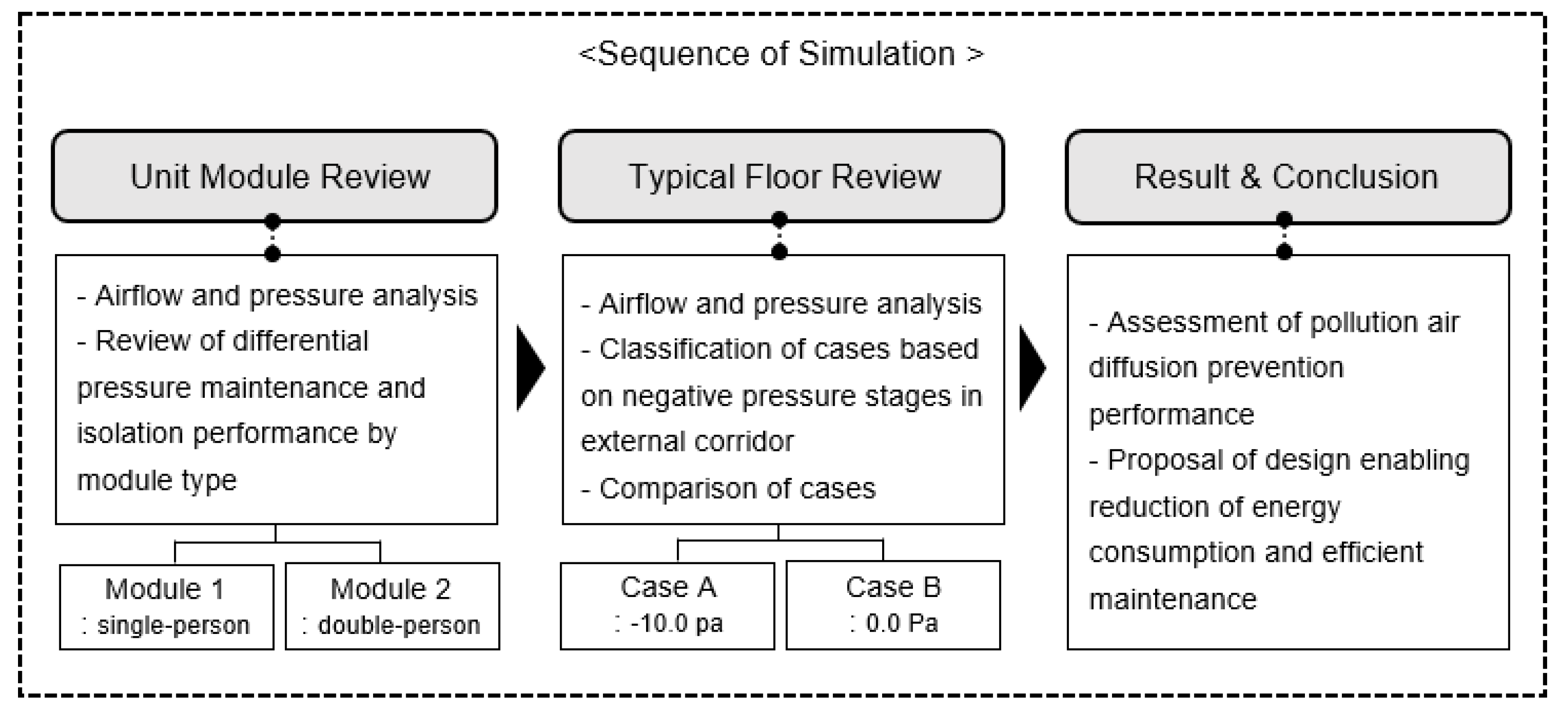
2.1. Study Scope and Process
2.2. Cases of Reviewing a Negative-Pressure Level
2.3. Unit Module Design and Performance Identification
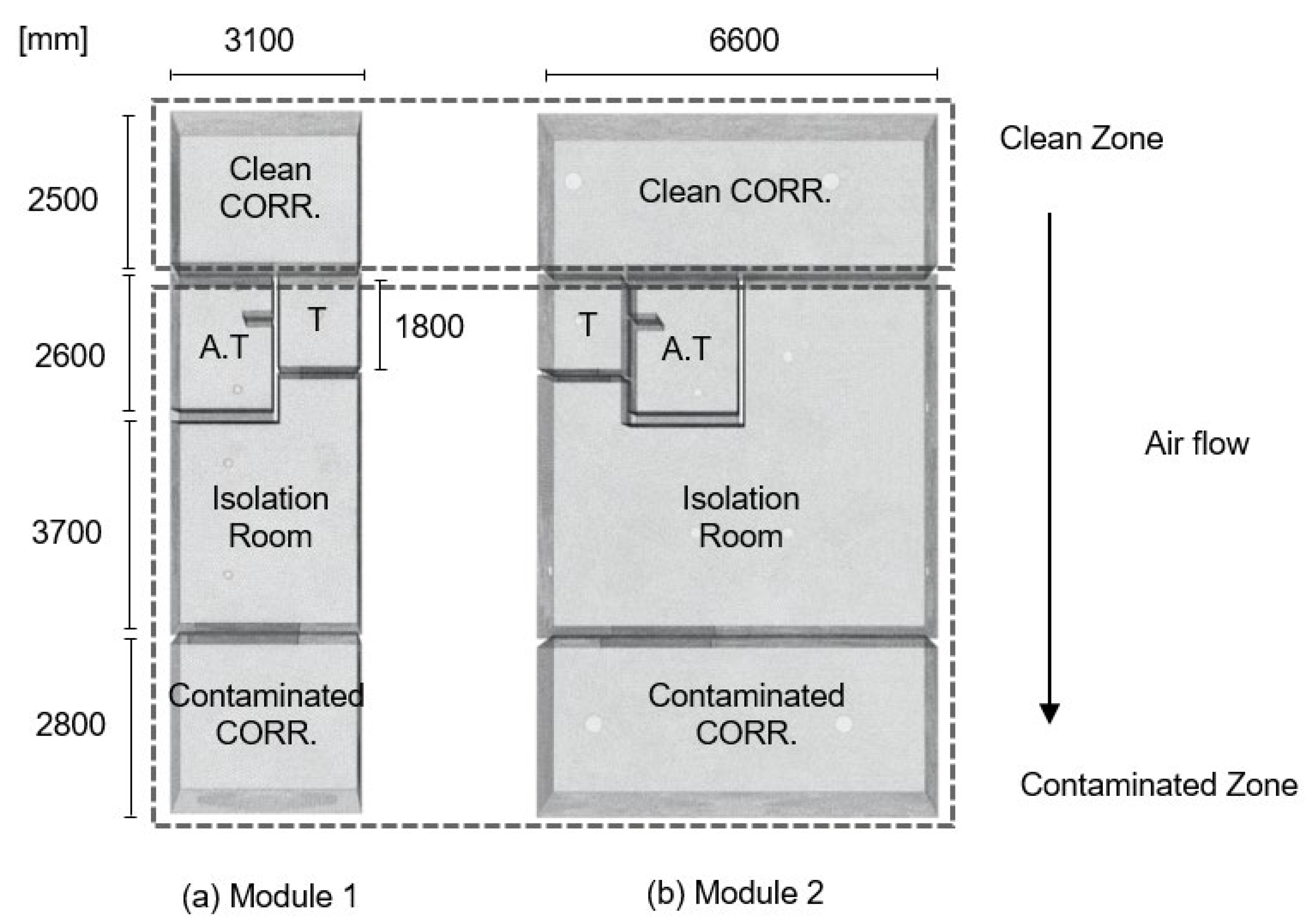
2.3.1. Unit Module Simulation Configuration
2.3.2. Review of the Isolation Performance of Contaminated Air in the Unit Modules
2.4. Typical Floor Modeling and HVAC Design
3. CFD Calculation Results
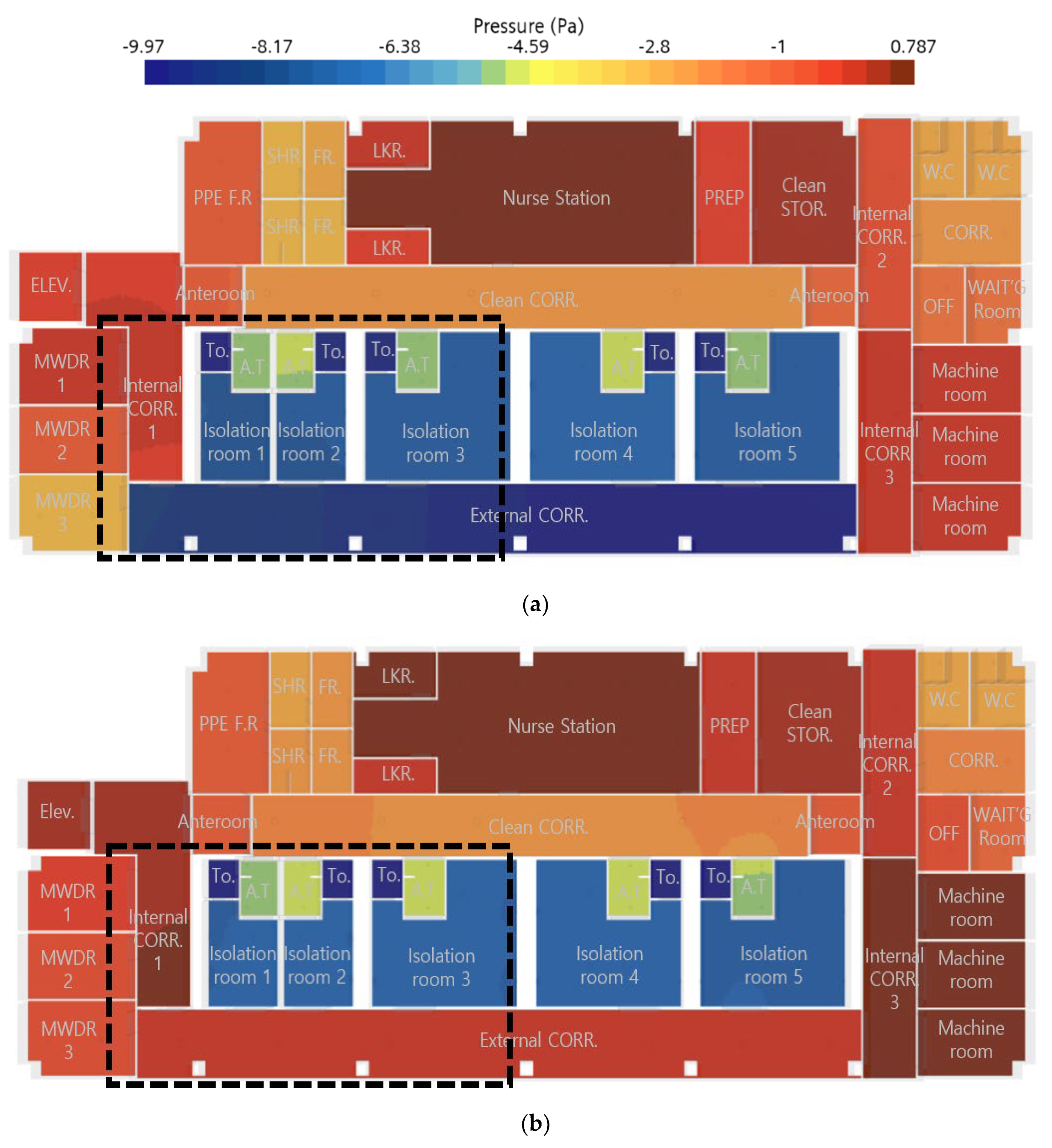
3.1. Evaluating the Actual Pressure Difference and Airflow Blockage Performance Using Pressure Distribution Analysis
3.2. Evaluating the Indoor Airflow Rate and the Spread of Airborne Contaminants
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- ANSI/ASHRAE/ASHE Standard 170-2017; Ventilation of Health Care Facilities. ASHRAE (American Society of Heating, Refrigerating and Air-Conditioning Engineers): Peachtree Corners, GA, USA, 2017.
- Selvan, P.T.; Abhiram, K.; Raghava, C.A.; Sai, V.N. CFD analysis of the fluid motion in the isolation rooms. IOP Conf. Ser. Earth Environ. Sci. 2021, 850, 012025. [Google Scholar] [CrossRef]
- Noh, S.; Park, M.; Sim, W.; Choi, C.; Ha, M. Application of virtual product design to the development of HVAC solution for Incheon International Airport Modular COVID-19 testing center. Case Stud. Chem. Environ. Eng. 2022, 6, 100257. [Google Scholar] [CrossRef] [PubMed]
- Lind, M.C.; Koskela, H.; Venås, B.; Vikan, A.W.; Kalliomäki, P.; Harsem, T.T. Designing Simplified Airborne Infection Isolation Rooms to Reduce Infection Rate in Future Pandemics. ASHRAE Trans. 2019, 125, 280–287. [Google Scholar]
- Cho, J.; Woo, K.; Kang, H. Experimental Study of an AIIR Ventilation System for Effective Removal of Airborne Contamination in Hospitals. J. Archit. Inst. Korea Struct. Constr. 2017, 33, 85–90. [Google Scholar] [CrossRef]
- Cho, J.; Kim, J. Evaluation of Ventilation Performance of a Mobile Negative Pressure Isolation Room for Infectious Disease Response to Prevent Infection. Korean J. Air-Cond. Refrig. Eng. 2023; 35, 253–264. [Google Scholar]
- Bang, J.; Sung, M. Study on the Prevention of the Spread of Airborne Pathogen with CFD Simulation and Experiments of Tracer Gas in Outpatient Departments of Medical Facility. J. Archit. Inst. Korea 2023, 39, 187–194. [Google Scholar]
- Le, T.-L.; Nguyen, T.T.; Kieu, T.T. A CFD Study on the Design Optimization of Airborne Infection Isolation Room. Math. Probl. Eng. 2022, 2022, e5419671. [Google Scholar] [CrossRef]
- Kong, X.; Guo, C.; Lin, Z.; Duan, S.; He, J.; Ren, Y.; Ren, J. Experimental study on the control effect of different ventilation systems on fine particles in a simulated hospital ward. Sustain. Cities Soc. 2021, 73, 103102. [Google Scholar] [CrossRef]
- Lee, J. Insulation and Airtight Plan of the Modular Construction System. Rev. Archit. Build. Sci. 2014, 58, 28–31. [Google Scholar]
- Tanyer, A.M.; Tavukcuoglu, A.; Bekboliev, M. Assessing the airtightness performance of container houses in relation to its effect on energy efficiency. Build. Environ. 2018, 134, 59–73. [Google Scholar] [CrossRef]
- Chung, J.; Lim, S.; Seol, W.; Lee, K. Improvement Plan of Airtight Performance in PC Modular House according to Passive House Standard. J. Korean Inst. Archit. Sustain. Environ. Build. Syst. 2023, 17, 1–14. [Google Scholar]
- Chung, J.; Lim, S.; Seol, W.; Yang, H.; Lee, K. Research on Improvement Measures based on Experimental Results of Airtightness Performance of Modular Negative-pressure wards. J. Korean Inst. Archit. Sustain. Environ. Build. Syst. 2023, 17, 422–433. [Google Scholar]
- Park, H.; Song, Y. A Study on the Isolation Performance of Modular Negative Pressure Room by Air Flow Analysis. J. Korean Inst. Archit. Sustain. Environ. Build. Syst. 2023, 17, 284–295. [Google Scholar]
- Choi, K.; Yun, H. A Study on Implications and Planning Directions for the Development of a Modular Airborne Infection Isolation Ward. J. Korea Inst. Healthc. Archit. 2022, 28, 7–16. [Google Scholar]
- Bhattacharyya, S.; Dey, K.; Paul, A.R.; Biswas, R. A novel CFD analysis to minimize the spread of COVID-19 virus in a hospital isolation room. Chaos Solitons Fractals 2020, 139, 110294. [Google Scholar] [CrossRef] [PubMed]
- WHO. Roadmap to Improve and Ensure Good Indoor Ventilation in the Context of COVID-19; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Ninomura, P.; Rousseau, C.; Bartley, J. Updated guidelines for the design and construction of hospitals and healthcare facilities. Ashrae J. 2006, 48, H33. [Google Scholar]
- CDC. Guidelines for Environmental Infection Control in Health-Care Facilities. Morb. Mortal. Wkly. Rep. Recomm. Rep. RR 2003, 52, 1–42. [Google Scholar]
- Jo, S.; Kim, G.; Sung, M. Analysis on contaminant Migration from Negative Pressure Isolation Ward during Door Opening and Human Movement using CFD Simulation. J. Archit. Inst. Korea Struct. Constr. 2017, 33, 61–68. [Google Scholar]
- Available online: https://docs.sw.siemens.com/en-US/doc/226870983/PL20220729105072148.starccmp_userguide_html (accessed on 30 March 2024).
- Cho, J. A Reference Model and HVAC Design Criteria of Mobile Negative Pressure Isolation Room for Responding to Infectious Disease Outbreaks. J. Archit. Inst. Korea 2022, 38, 195–205. [Google Scholar]
- Cho, J.; Jang, S.; Song, J. Onsite measurement and dilution-based infection risk assessment for a new mobile negative pressure isolation (MNPIR) as a solution to minimize cross-infection. Sustain. Cities Soc. 2023, 95, 104583. [Google Scholar] [CrossRef]
- Zahed, F.; Pardakhti, A.; Motlagh, M.S.; Kari, B.M.; Tavakoli, A. The effect of airtightness required in building energy conservation regulations on indoor and outdoor originated pollutants. Heliyon 2023, 9, e20378. [Google Scholar] [CrossRef]
- Lee, J.H.; Shim, J.W.; Lim, M.H.; Baek, C.; Jeon, B.; Cho, M.; Park, S.; Choi, D.H.; Kim, B.S.; Yoon, D.; et al. Towards optimal design of patient isolation units in emergency rooms to prevent airborne virus transmission: From computational fluid dynamics to data-driven modeling. Comput. Biol. Med. 2024, 173, 108309. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| (m3/h) | Module 1 | Module 2 | ||
|---|---|---|---|---|
| Supply | Exhaust | Supply | Exhaust | |
| Clean corridor | - | - | 300 | 360 |
| Anteroom | 100 | 150 | 100 | 150 |
| Isolation room | 320 | 480 | 690 | 1020 |
| Toilet | - | 40 | - | 40 |
| Contaminated corridor | - | - | 375 | 450 |
| Module 1 | Module 2 | |
|---|---|---|
| Clean corridor | - | −2.3931 |
| Anteroom | −4.937 | −4.6609 |
| Isolation room | −7.4866 | −7.4829 |
| Toilet | −9.721 | −10.1279 |
| Contaminated corridor | - | −9.4684 |
| Pressure (pa) | Zone | CMH (m3/h) | Remark | |
|---|---|---|---|---|
| Supply | Exhaust | |||
| 0 | Nurse station | 2500 | Clean zone | |
| Medical staff’s prep room | 100 | |||
| Medical staff’s storage room | 150 | |||
| Internal corridor 1 | 350 | |||
| Internal corridor 2 | 100 | |||
| Internal corridor 3 | 200 | |||
| −1.0 | Internal corridor anteroom × 2 | 190 | 230 | |
| Office and waiting room | 200 | 400 | ||
| −2.5 | Clean corridor | 900 | 1080 | |
| PPE changing room * | 250 | 300 | Contaminated zone | |
| Shower room × 2 * | - | 100 | ||
| Changing room × 2 * | - | 100 | ||
| Locker × 2 | 100 | 100 | ||
| Public toilet × 2* | - | 100 | ||
| Office corridor * | 200 | 400 | ||
| MWDR 1 * | 300 | 600 | ||
| MWDR 2 * | 200 | 500 | ||
| MWDR 3 * | 200 | 400 | ||
| −5.0 | Anteroom of an isolation room × 5 | 500 | 1900 | |
| −7.5 | Isolation room 1 and 2 | 640 | 960 | |
| Isolation room 3–5 | 2070 | 3060 | ||
| −10.0 | Attached toilet × 5 | - | 200 | |
| External corridor | 1500 | 1800 | ||
| Total | 10,650 | 12,230 | ||
| Zone | Case A | Case B | |
|---|---|---|---|
| Nurse station | 1.31 | 0.86 | |
| Medical staff’s prep room | 0.19 | 0.02 | |
| Medical staff’s storage room | 0.35 | 0.04 | |
| Internal corridor 1 | 0.59 | 0.47 | |
| Internal corridor 2 | 0.11 | 0.08 | |
| Internal corridor 3 | 0.59 | 0.57 | |
| Internal corridor anteroom L | −1.13 | −0.99 | |
| Internal corridor anteroom R | −1.07 | −10.9 | |
| Office and waiting room | −1.57 | −1.59 | |
| Clean corridor | −2.36 | −2.35 | |
| PPE changing room | −1.88 | −1.89 | |
| Shower room | −2.63 | −2.69 | |
| Changing room | −2.50 | −2.53 | |
| Locker | 0.09 | 0.06 | |
| Public toilet | −2.46 | −2.85 | |
| Office corridor | −2.10 | −2.12 | |
| MWDR 1 | −0.78 | −0.43 | |
| MWDR 2 | −1.86 | −0.69 | |
| MWDR 3 | −2.45 | −0.68 | |
| Anteroom of an isolation room | 1 | −5.11 | −4.96 |
| 2 | −4.89 | −4.87 | |
| 3 | −5.01 | −4.91 | |
| 4 | −5.00 | −4.92 | |
| 5 | −5.23 | −5.13 | |
| Isolation room | 1 | −7.66 | −7.49 |
| 2 | −7.64 | −7.47 | |
| 3 | −7.60 | −7.53 | |
| 4 | −7.61 | −7.52 | |
| 5 | −7.63 | −7.56 | |
| Attached toilet 1~5 | −10.1 | −10.00 | |
| External corridor | −9.52 | 0.45 | |
| Case A | Case B | |
|---|---|---|
| Clean corridor | 0.1602 | 0.5862 |
| Anteroom 1 and 2 | 0.6391 | 0.3675 |
| Isolation room 1 and 2 | 0.1795 | 0.1406 |
| Toilet 1 and 2 | 0.1620 | 0.4030 |
| Anteroom 3 | 0.3917 | 0.3846 |
| Isolation room 3 | 0.1971 | 0.2839 |
| Toilet 3 | 0.1553 | 0.3825 |
| Internal corridor | 0.1872 | 0.2728 |
| External corridor | 0.6495 | 0.5908 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, H.-E.; Go, S.; Song, Y.-H. Airflow and Pressure Design Review of Modular Negative Pressure Wards. Buildings 2024, 14, 1623. https://doi.org/10.3390/buildings14061623
Park H-E, Go S, Song Y-H. Airflow and Pressure Design Review of Modular Negative Pressure Wards. Buildings. 2024; 14(6):1623. https://doi.org/10.3390/buildings14061623
Chicago/Turabian StylePark, Hyung-Eun, Sumin Go, and Young-Hak Song. 2024. "Airflow and Pressure Design Review of Modular Negative Pressure Wards" Buildings 14, no. 6: 1623. https://doi.org/10.3390/buildings14061623
APA StylePark, H. -E., Go, S., & Song, Y. -H. (2024). Airflow and Pressure Design Review of Modular Negative Pressure Wards. Buildings, 14(6), 1623. https://doi.org/10.3390/buildings14061623