

Study on the Repair Effect of Self-Healing Cementitious Material with Urea-Formaldehyde Resin/Epoxy Resin Microcapsule
Abstract
:1. Introduction
2. Materials and Methods
2.1. Raw Material Characteristics
2.1.1. Microcapsule
2.1.2. Cement Mortar
2.2. Preparation Method
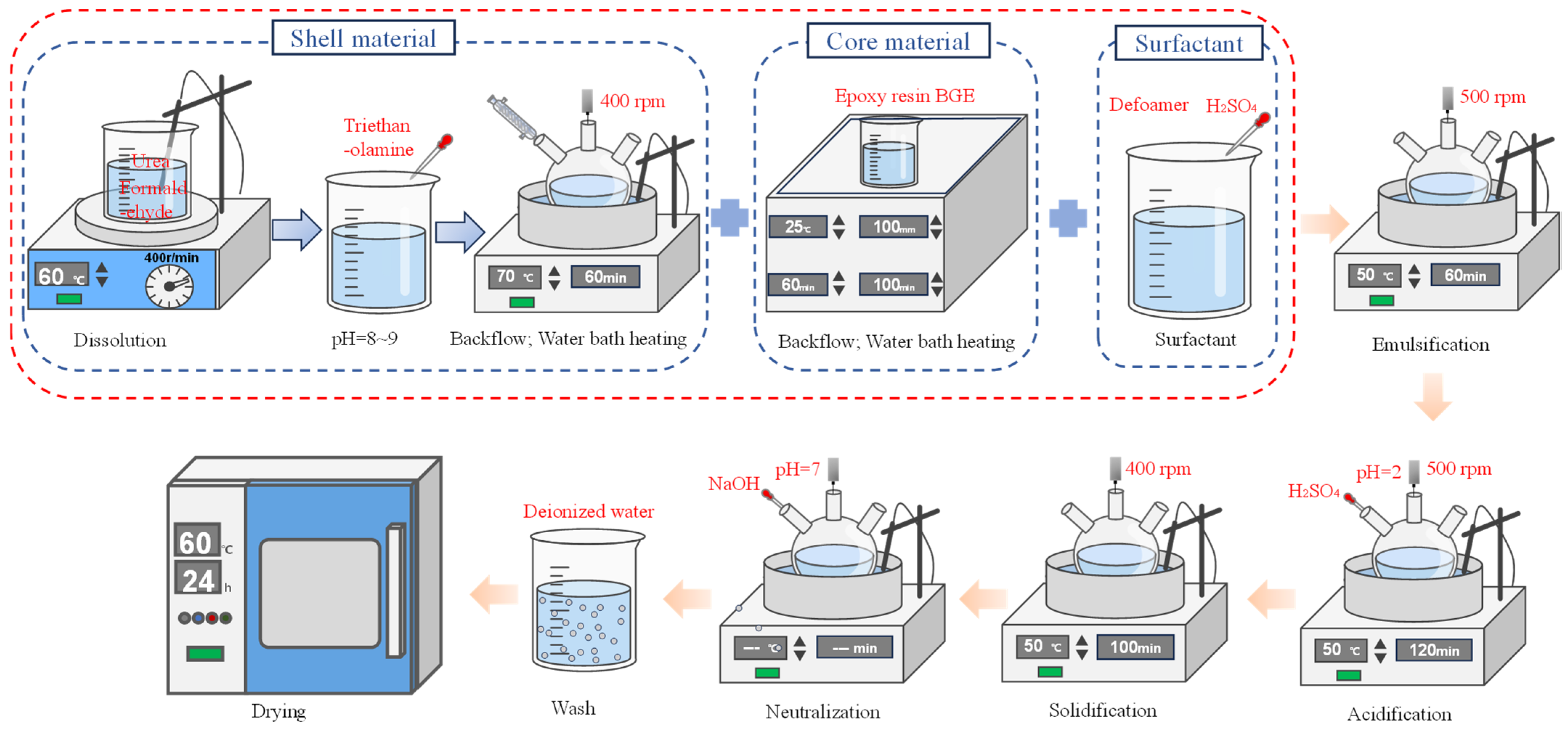
2.2.1. Microcapsule Preparation Process
2.2.2. Cement Mortar Sample Preparation
- (1)
- Mixing ratios
- (2)
- Cement mortar test piece preparation
2.3. Test Methods
2.3.1. Molecular Dynamics Simulation Method
- (1)
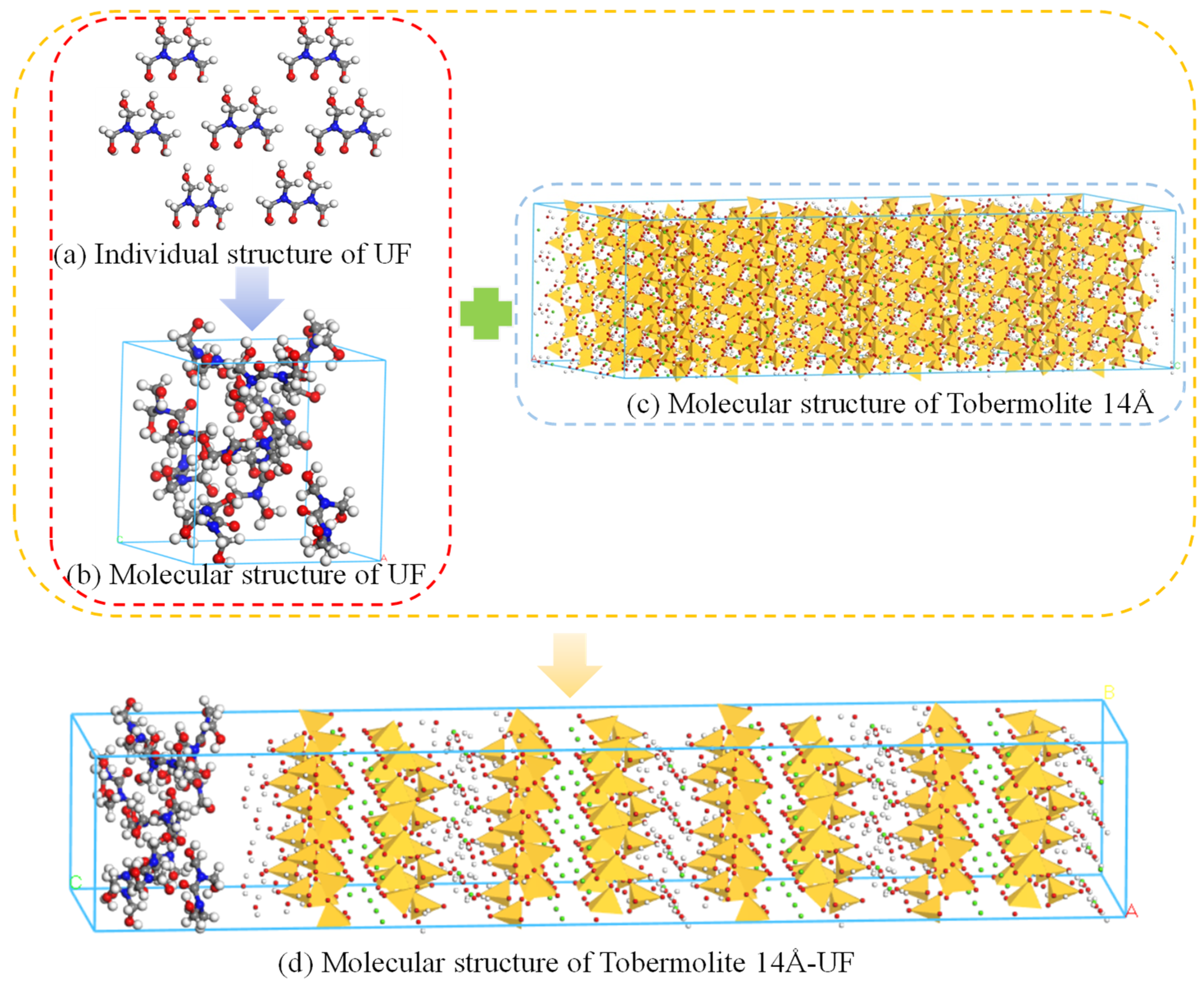
- Cyst wall-cement matrix modelling
- (2)
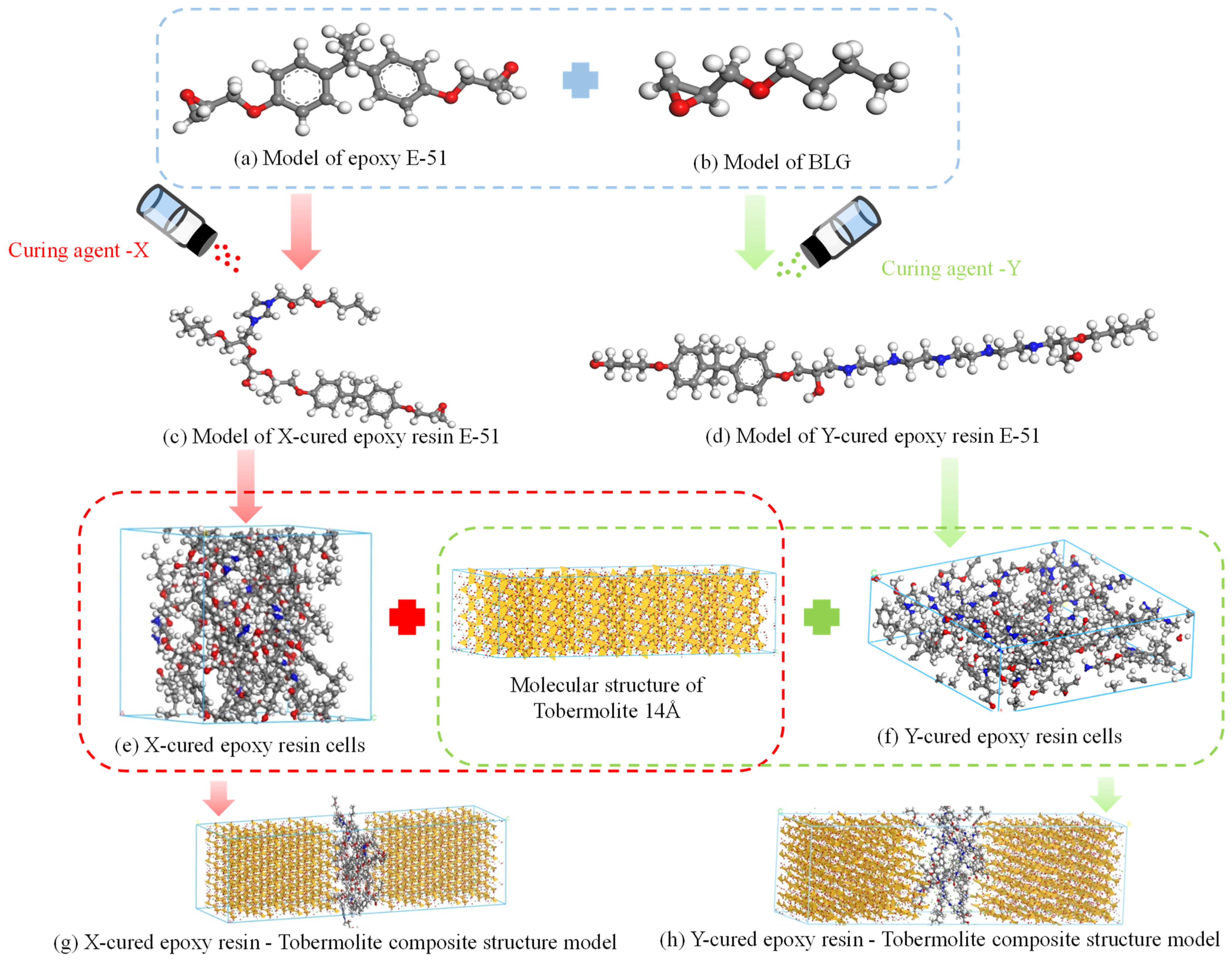
- Sac-core-cement matrix modelling
- (3)
- Indicators for the evaluation of calculation results.
- Bulk and Young’s Moduli: these measure the material’s deformation properties.
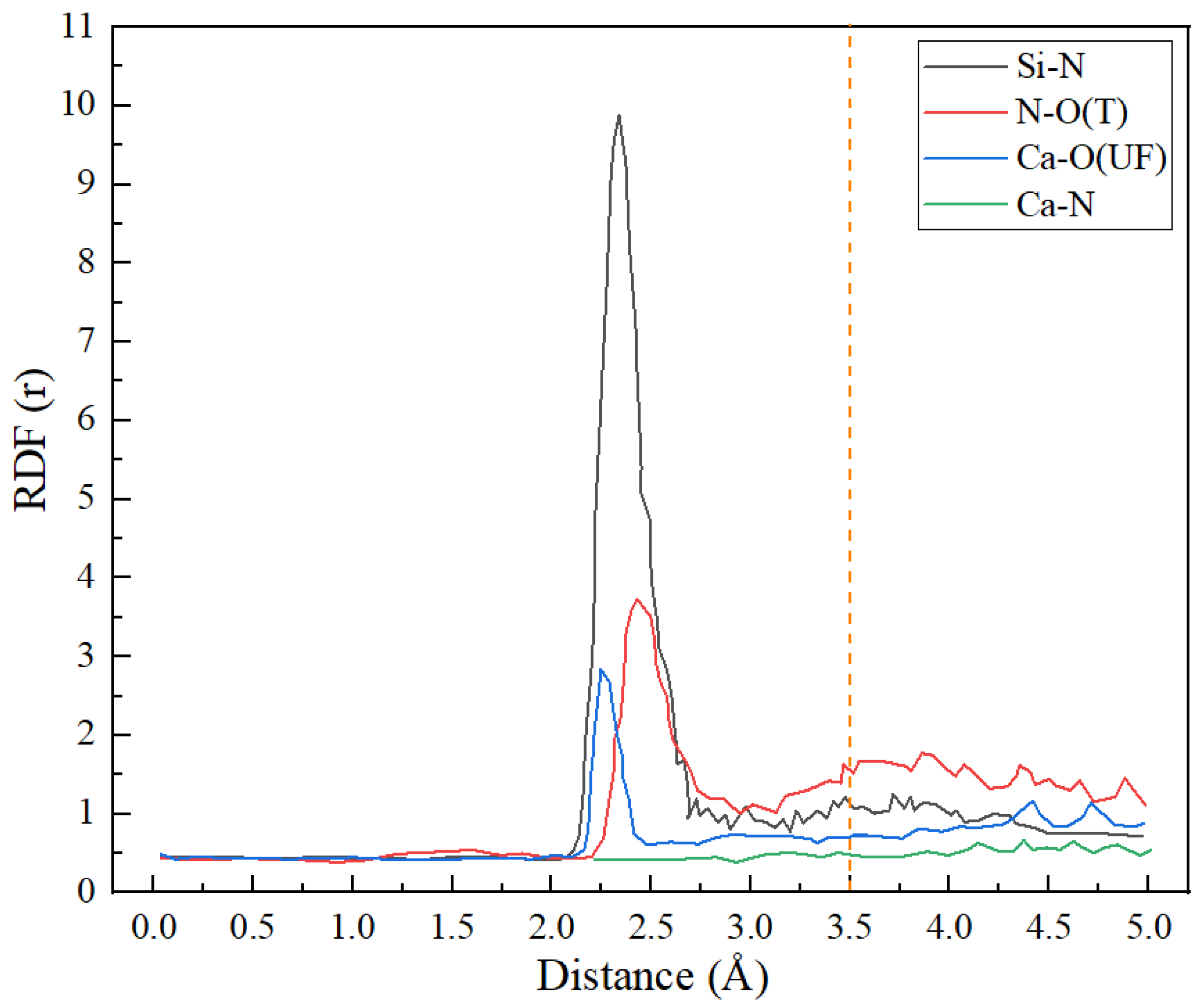
- Radial Distribution Function (RDF): this function indicates the probability density of atomic proximity, providing insights into the potential for bonding at the interface.
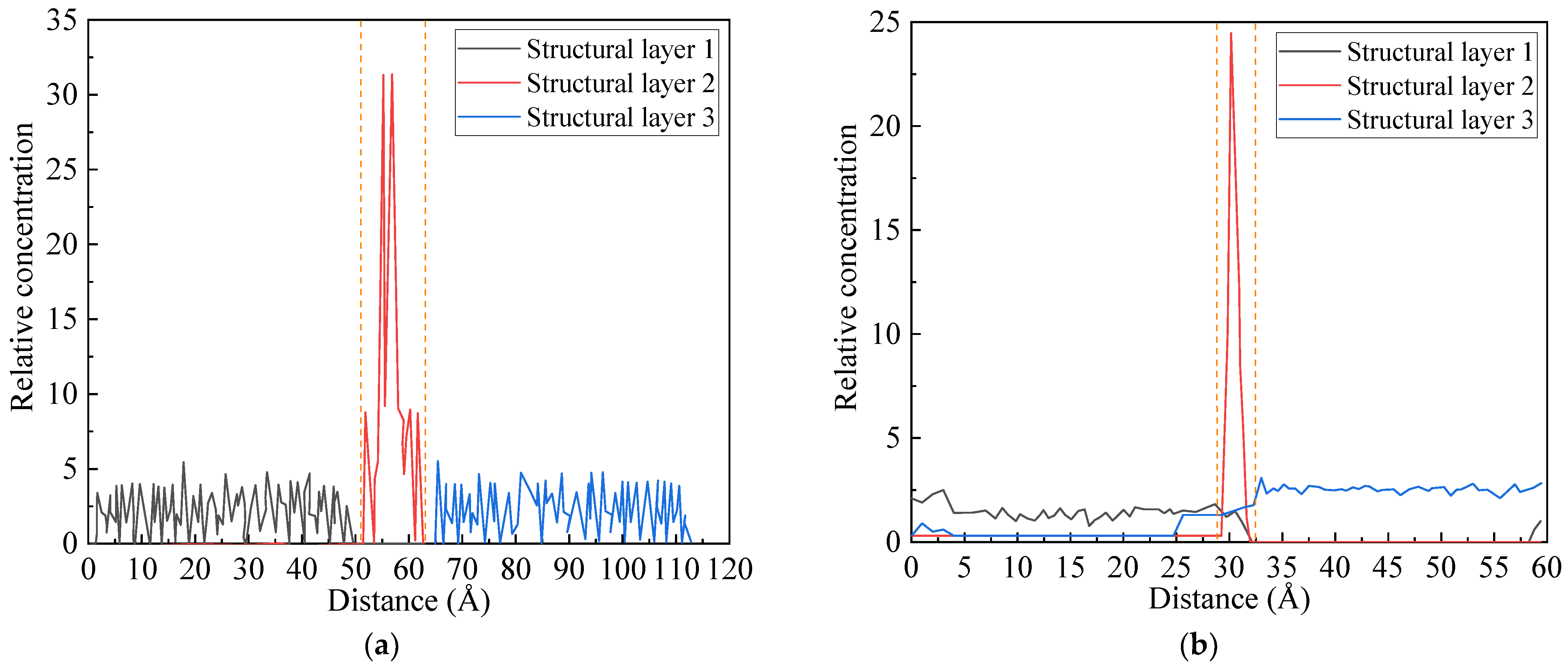
- Relative Concentration: this metric assesses the concentration of each molecular component along an axis, revealing interactions within the layered structure.
- Stress-Strain Curves: these curves demonstrate how the microcapsule repair materials influence the mechanical strength of the cement matrix.
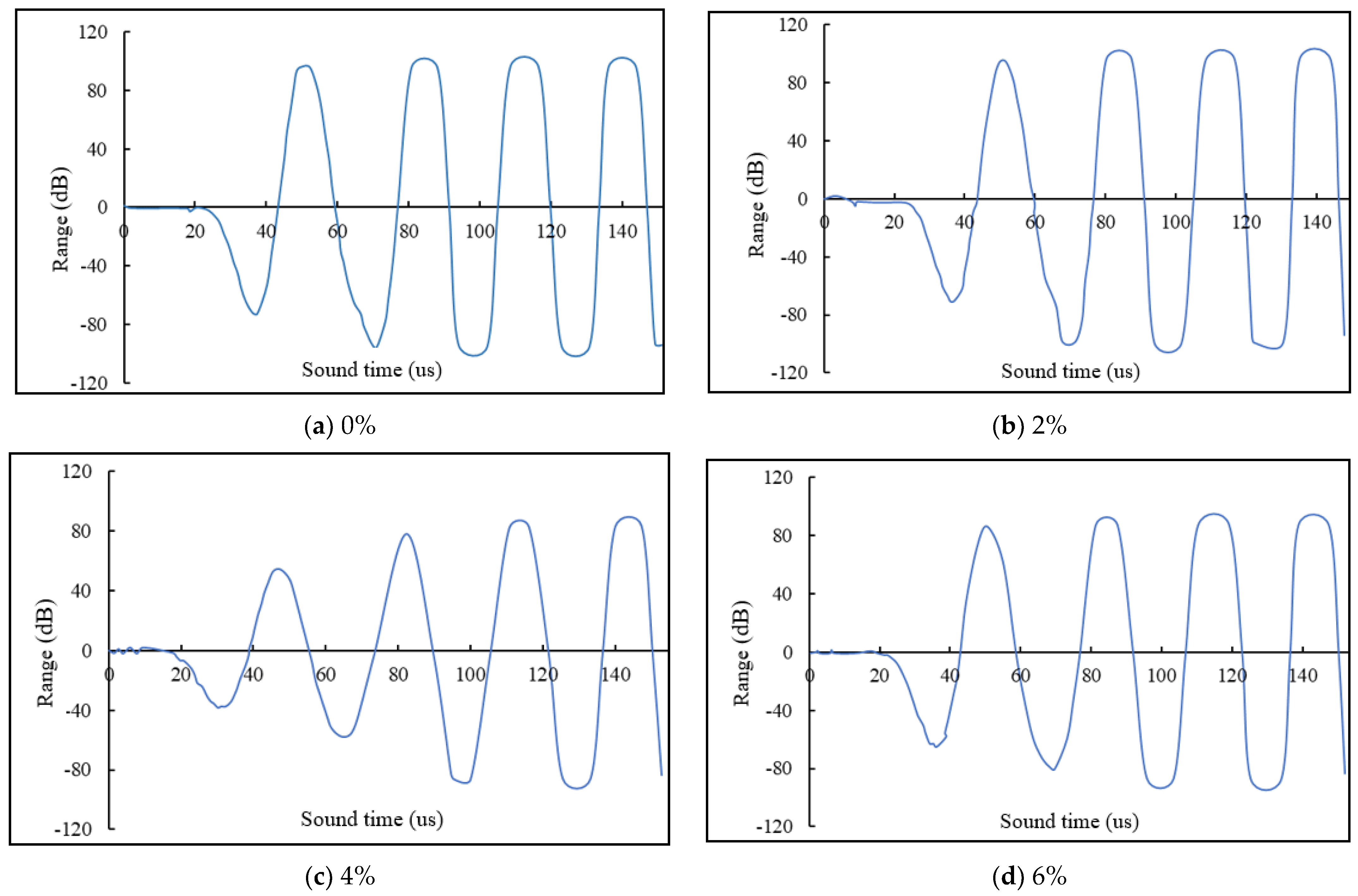
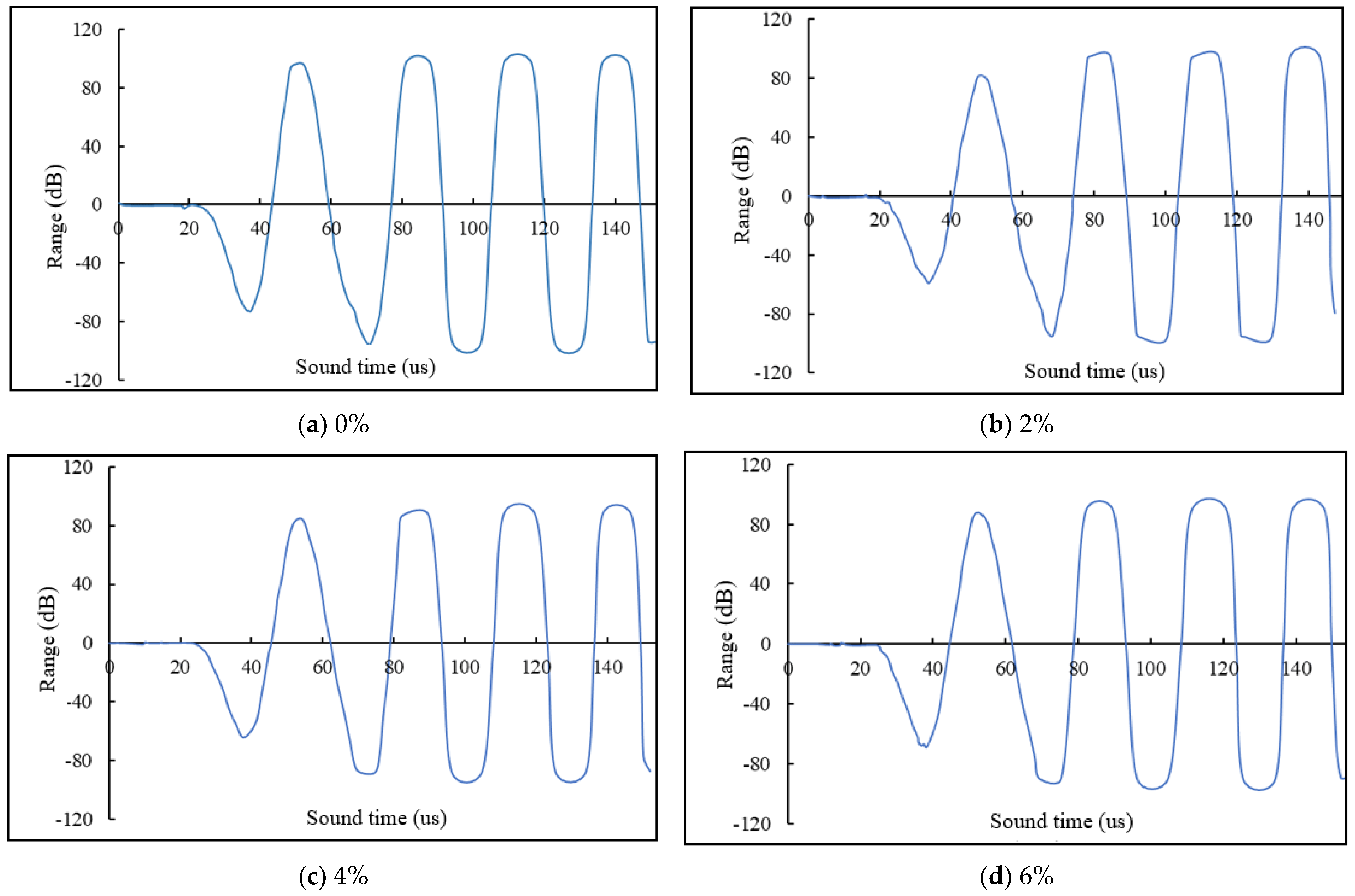
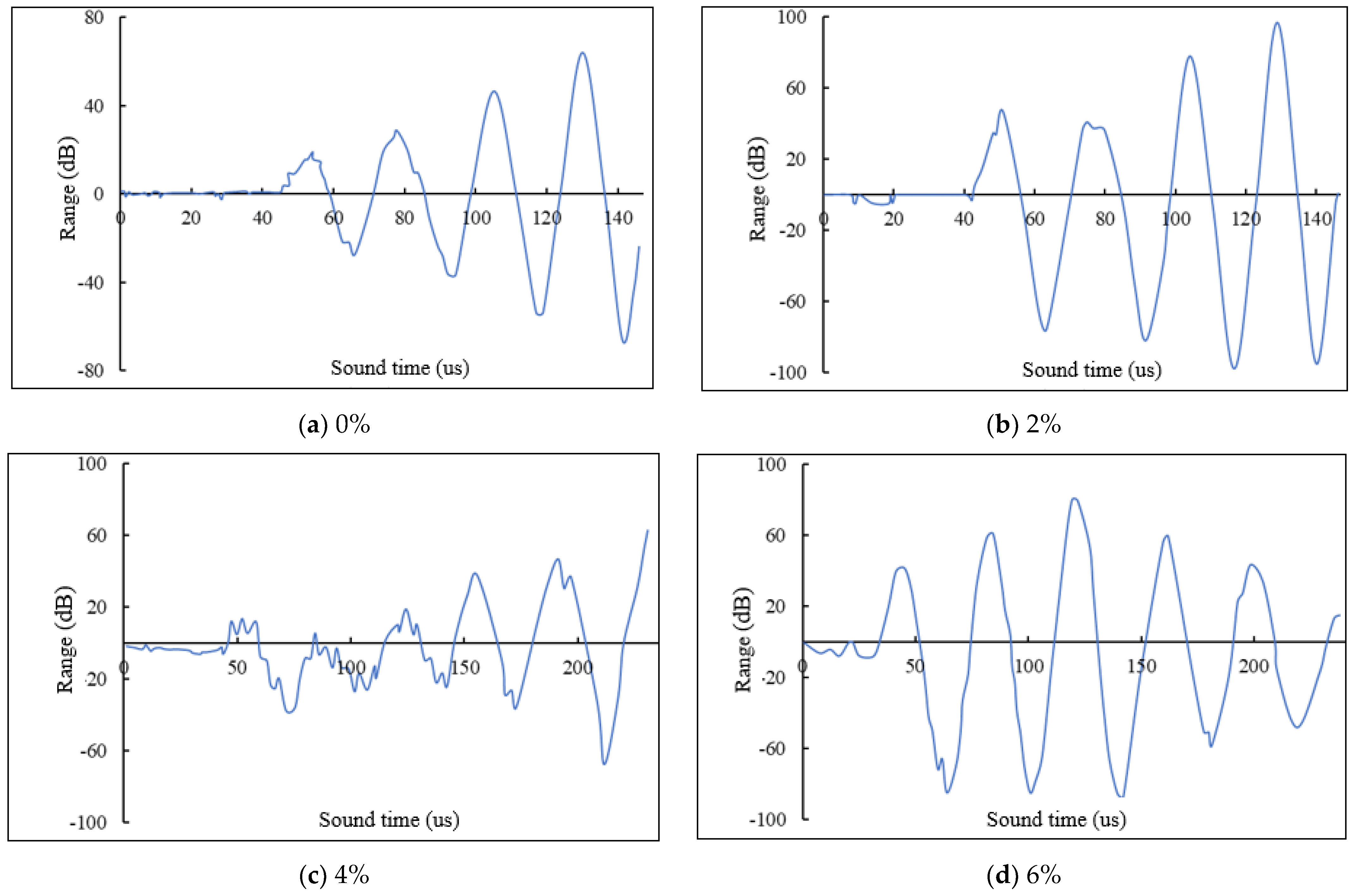
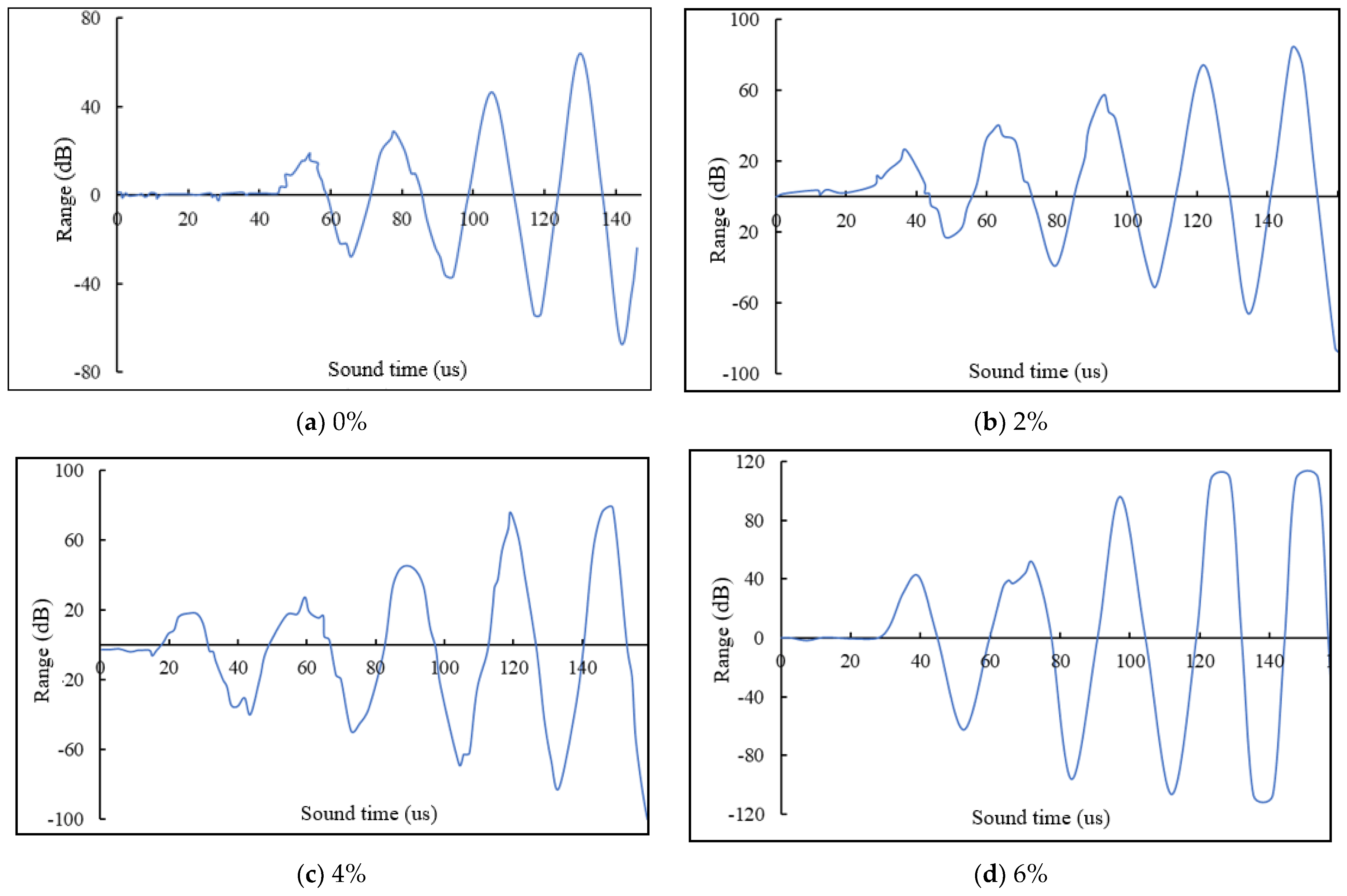
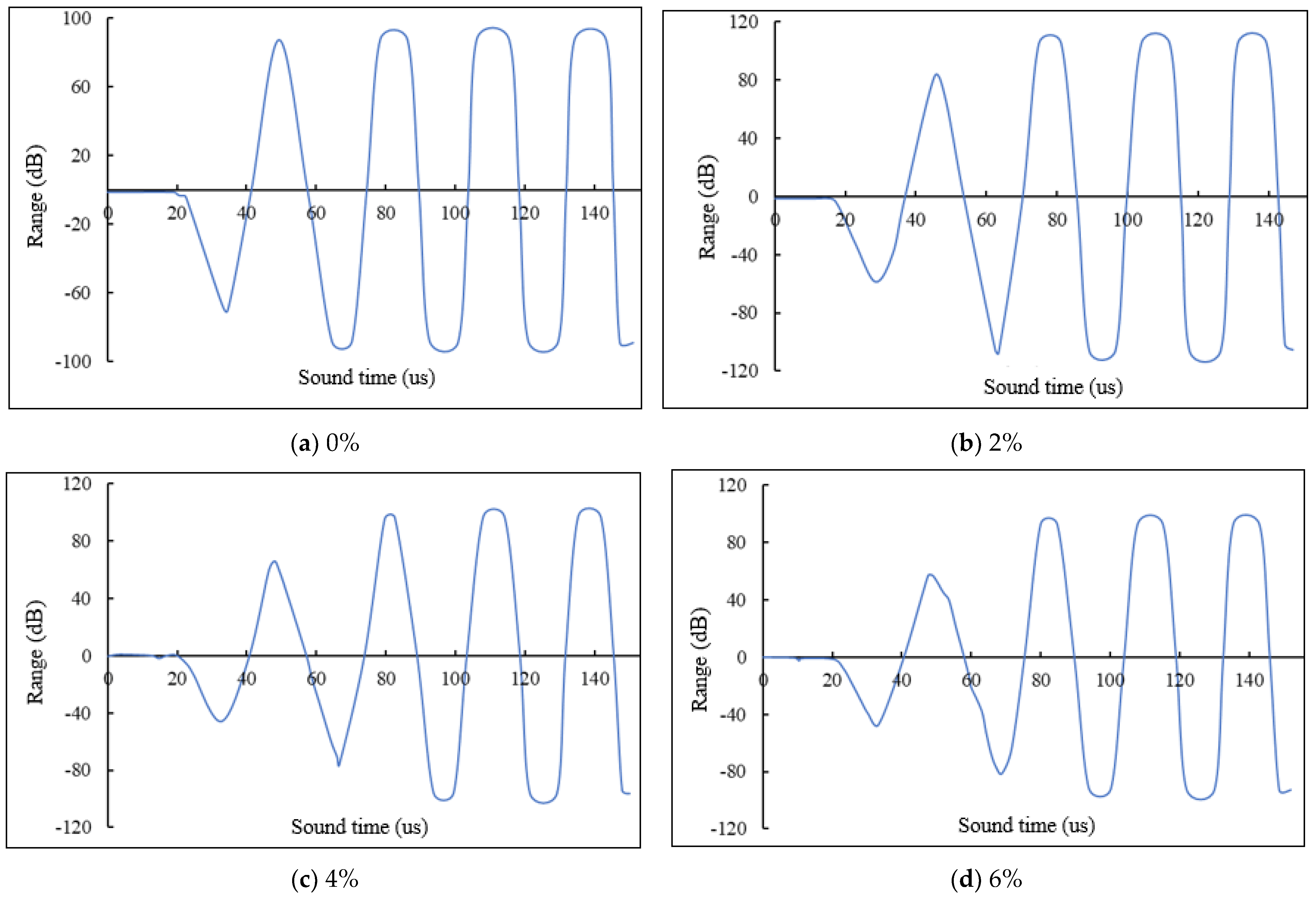
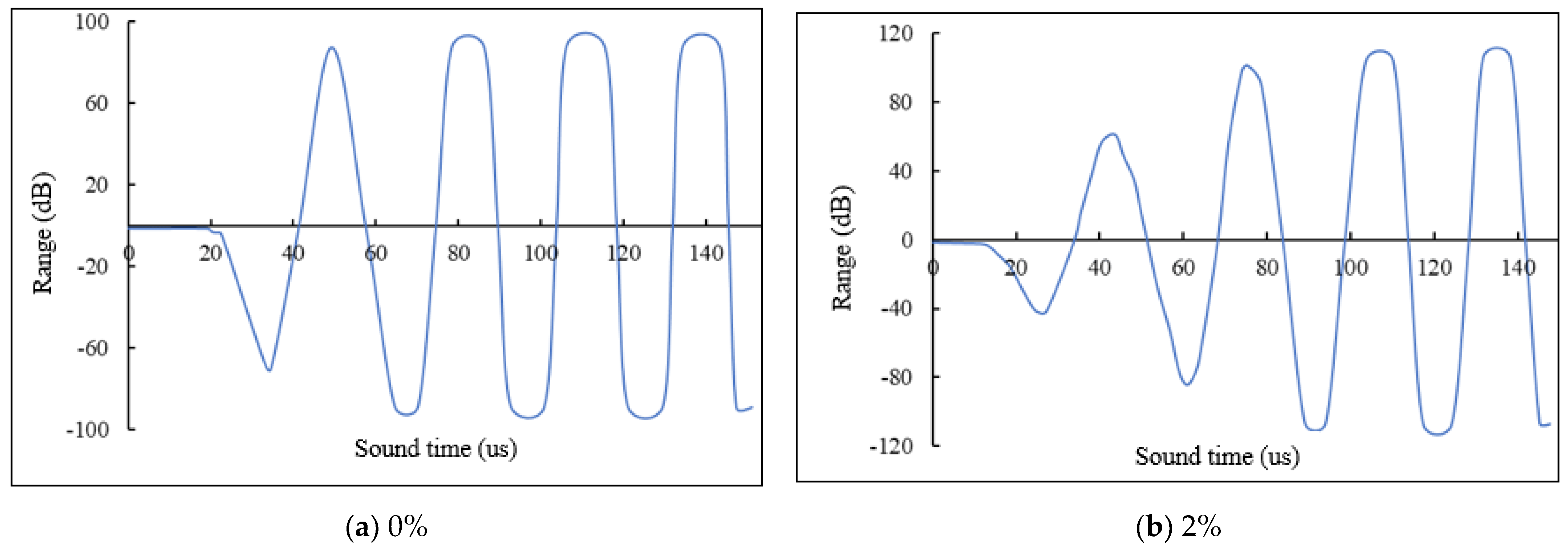
2.3.2. Self-Healing Function Detection
2.3.3. Test Programme for the Effectiveness of the Repair
2.3.4. Pore Size Distribution Test Method
2.3.5. Rapid Chloride Diffusion Method
3. Results and Discussion
3.1. Interfacial Contact Properties and Microscopic Remediation
3.1.1. Cyst Wall-Cement Matrix
- (1)
- Moduli of the composite structure
- (2)
- Radial Distribution Function (RDF)
- (3)
- Stress-strain behavior
3.1.2. Core-Cement Matrix
- (1)
- Relative concentration
- (2)
- Stress-strain curve
- (3)
- Radial Distribution Function
3.2. Structural Damage Repair Effect
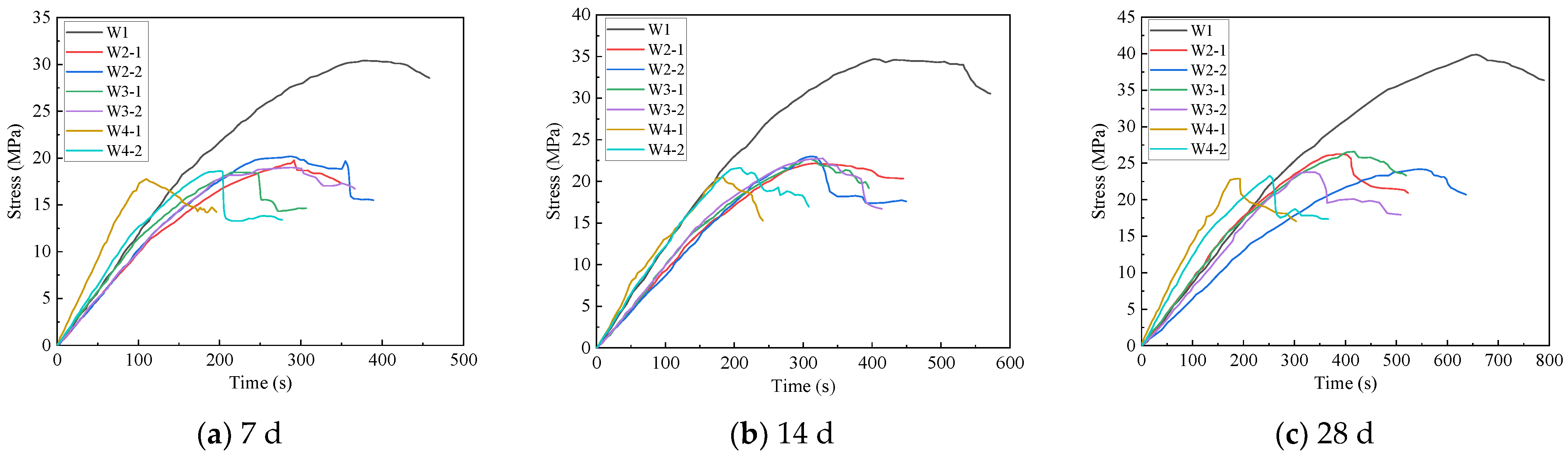
3.3. Effect of Initial Strength of Cement Mortar
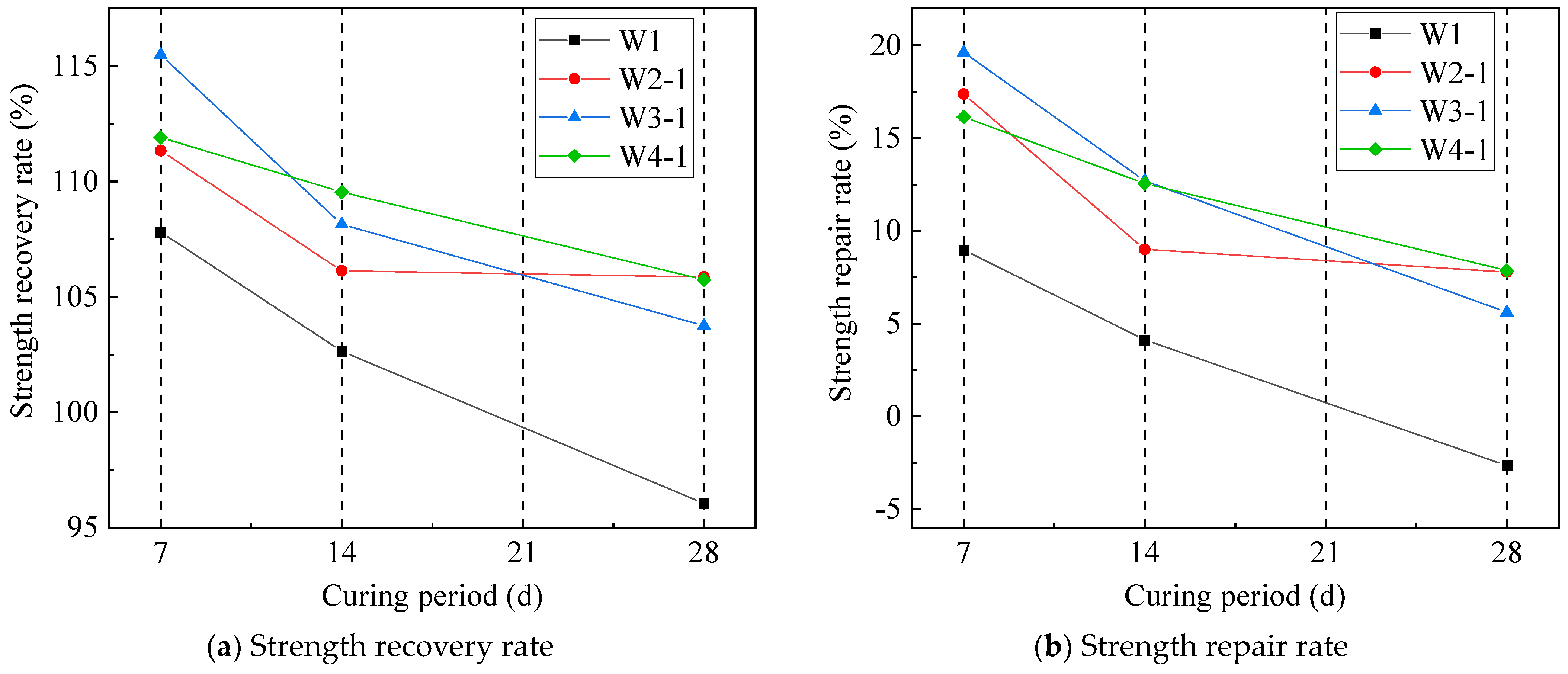
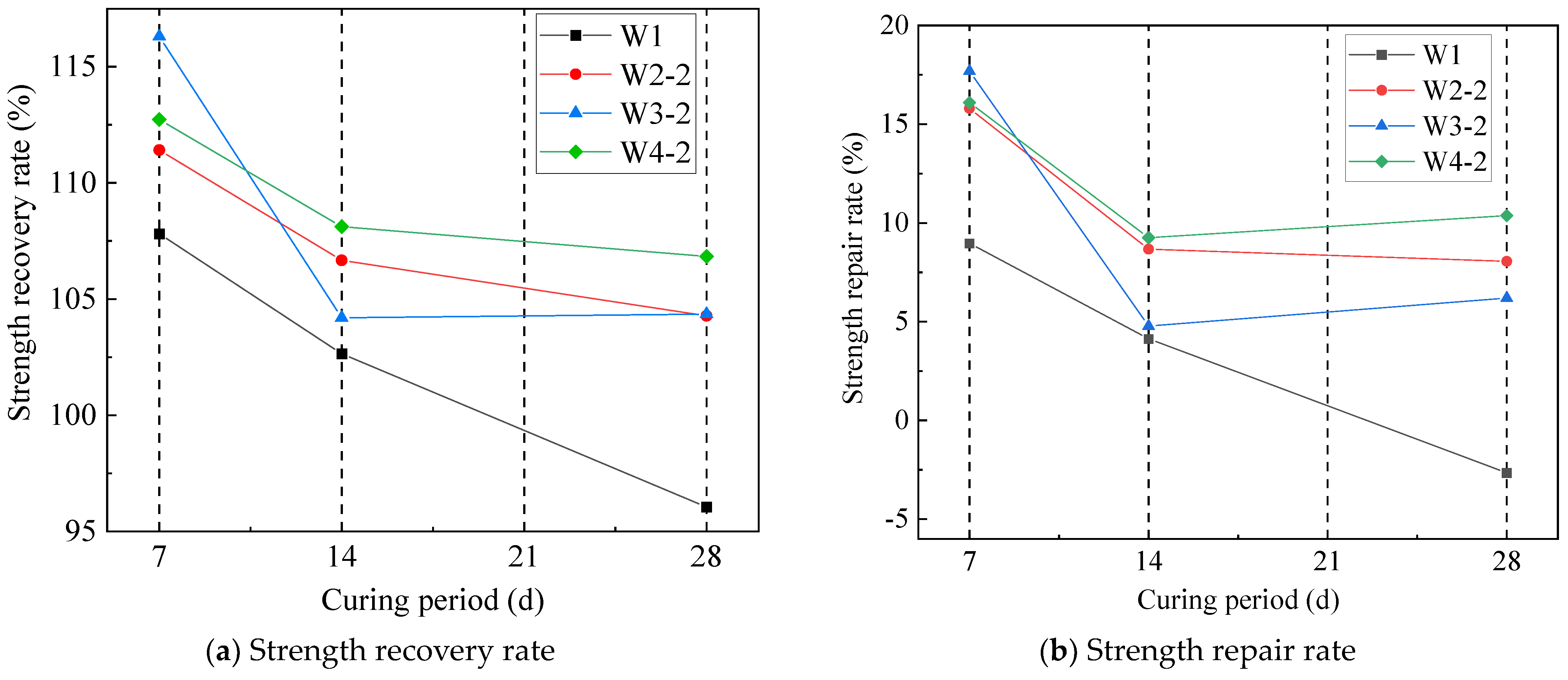
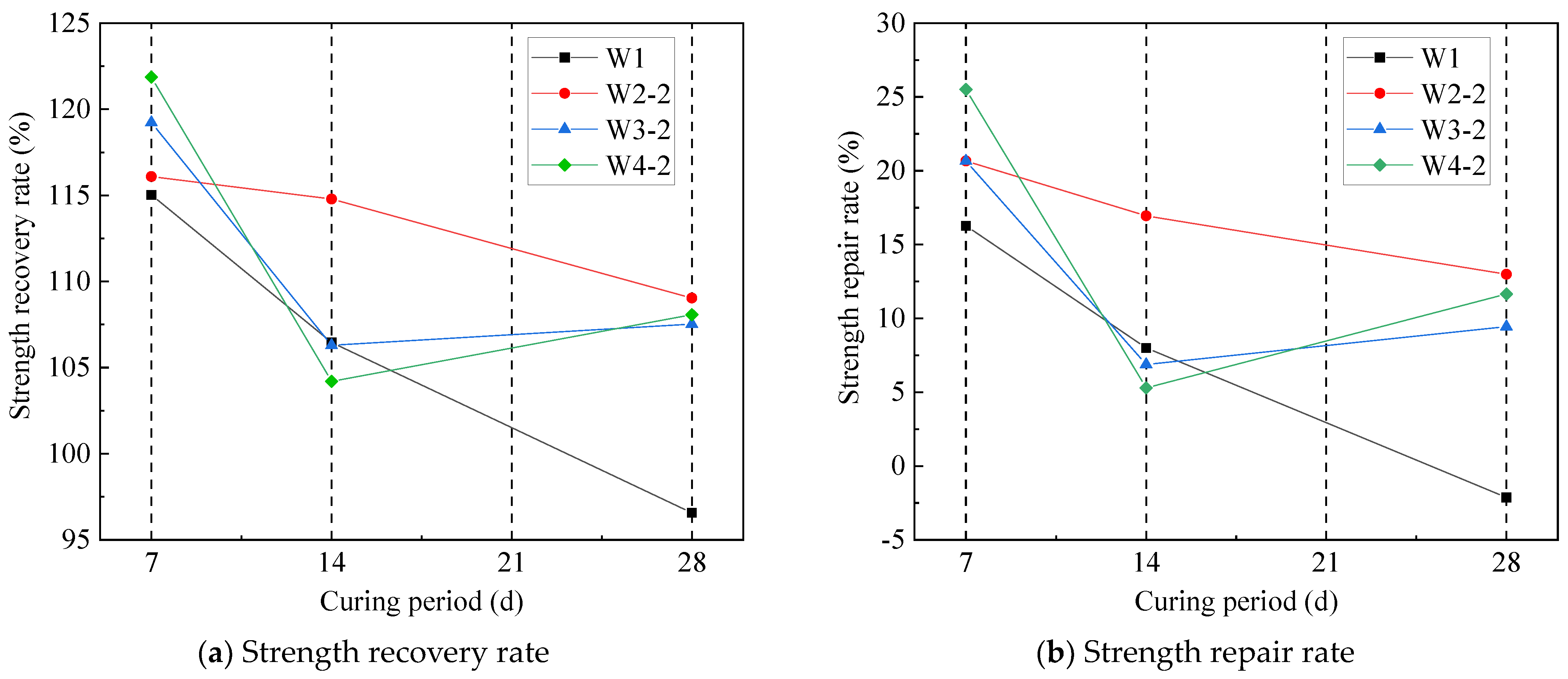
3.4. Influence of Cement Mortar Strength on the Effectiveness of Repair
3.4.1. Experimental Group without Microcapsule Incorporation
3.4.2. Test Group with Microencapsulation
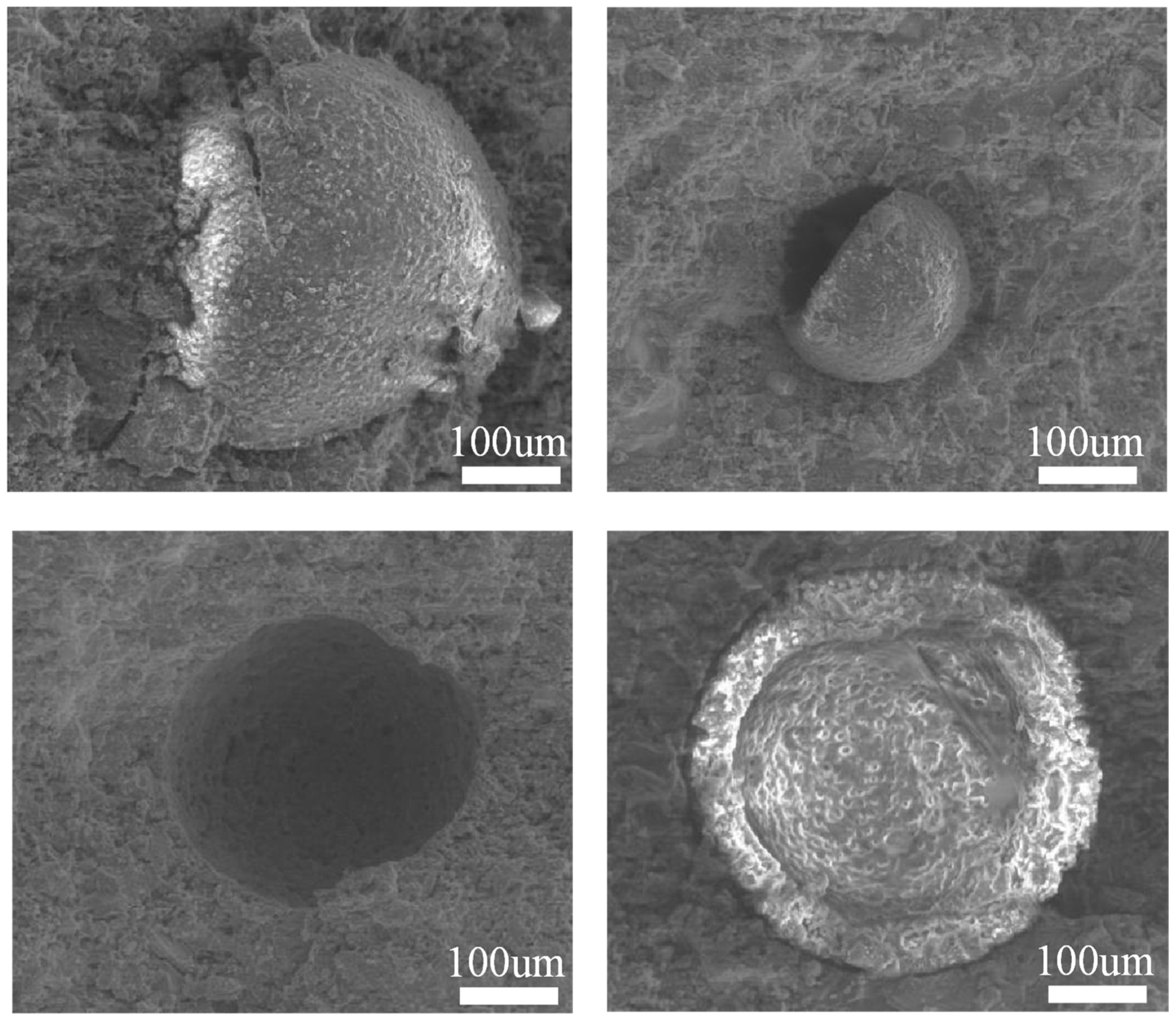
3.5. Microscopic Morphology of Cement Mortar Containing Microcapsules
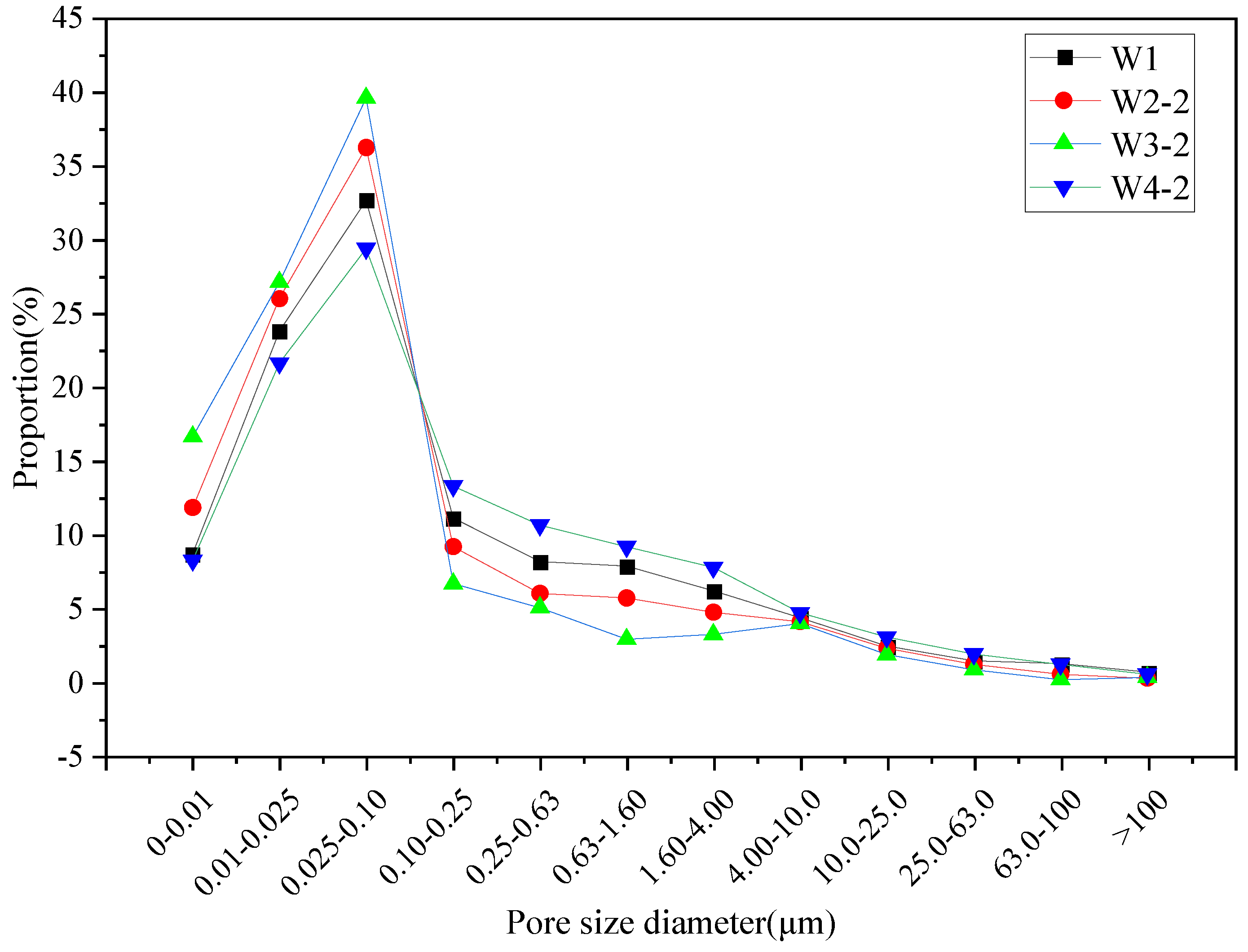
3.6. Effect of Microcapsules on the Pore Structure of Cement Mortar
3.7. Effect of Microcapsules on the Impermeability of Cement Mortar
4. Conclusions
- (1)
- Urea-formaldehyde resin/epoxy resin E-51 microcapsules were successfully synthesized via in-situ polymerization with optimal conditions identified for particle size, morphology, and encapsulation rate. The microcapsules made under the optimal conditions had a dense and smooth morphology, with an encapsulation rate of 55.59% at an average particle size of 495.56 μm.
- (2)
- The microcapsule wall and the cured core material exhibit strong interfacial contact with the cementitious material, enhancing ductility and providing significant strength support, whereas the uncured core material diminishes mechanical properties.
- (3)
- Microcapsule-enhanced cement mortar demonstrates a superior self-repair capability compared to ordinary cement mortar, although its initial strength is reduced with higher microcapsule dosages.
- (4)
- The repair effectiveness of microencapsulated self-healing cement mortar diminishes over time due to the ongoing hydration of cement particles and the release of the repair material from the capsule core. However, the self-healing effect remains stable over a longer period compared to ordinary cement mortar, which shows a nearly linear decline in repair capability.
- (5)
- The incorporation of microcapsules will have a significant effect on the flexural strength and compressive strength of the mortar. The effect on the compressive strength is greater the larger the dosage, the initial strength value of the cement mortar decreases more; the loss of strength of the cement mortar when using the Y curing agent is less than that of the use of the X curing agent, and the strength of the cement mortar with the use of the Y curing agent is more recovered.
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Jonkers, H.M. Self Healing Concrete: A Biological Approach; Springer Series in Materials Science; Springer: Dordrecht, The Netherlands, 2007; Volume 100, pp. 195–204. [Google Scholar]
- Wedding, P.A.; Cady, P.D.; Weyers, R.E. Chloride Penetration and the Deterioration of Concrete Bridge Decks. Concr. Aggreg. 1983, 5, 81–87. [Google Scholar]
- Marsavina, L.; Audenaert, K.; De Schutter, G.; Faur, N.; Marsavina, D. Experimental and Numerical Determination of the Chloride Penetration in Cracked Concrete. Constr. Build. Mater. 2009, 23, 264–274. [Google Scholar] [CrossRef]
- Chahal, N.; Siddique, R.; Rajor, A. Influence of bacteria on the compressive strength, water absorption and rapid chloride permeability of fly ash concrete. Constr. Build. Mater. 2012, 28, 351–356. [Google Scholar] [CrossRef]
- BS EN 1504; Products and Systems for the Protection and Repair of Concrete Structures-Definitions, Requirements, Quality Control and Evaluation of Conformity Concrete Injection. BSI Standards: Hong Kong, China, 2013.
- ACI 562-16; Code Requirements for Assessment, Repair, and Rehabilitation of Existing Concrete Structures and Commentary (Metric). ACI: Farmington Hills, MI, USA, 2016.
- ACI 546R-14; Guide to Concrete Repair. ACI: Farmington Hills, MI, USA, 2014.
- Nishiwaki, T.; Mihashi, H.; Jang, B.-K.; Miuea, K. Development of self-healing system for concrete with selective heating around crack. J. Adv. Concr. Technol. 2006, 4, 267–275. [Google Scholar] [CrossRef]
- Fengbin, Y.; Juanru, J.; Xuejun, C. Preferred design methods for reinforcement of concrete structures. Constr. Technol. 2016, 45, 22–24. [Google Scholar]
- Lubelli, B.; Nijland, T.G.; Van Hees, R.P.J. Self-healing of lime based mortars: Microscopy observations on case studies. Heron 2011, 56, 81–97. [Google Scholar]
- Yuhong, Q.; Guoliang, Z.; Jinfeng, C. Research progress of anticorrosive coatings for concrete. Coat. Ind. 2018, 48, 63–71. [Google Scholar]
- Concrete Repairs. Performance in Service and Current Practice (EP 79); Building Research Establishment: Garston, UK, 2007. [Google Scholar]
- Taylor, H.F.W. Proposed Structure For Calcium Silicate Hydrate Gel. J. Am. Ceram. Soc. 1986, 69, 464–467. [Google Scholar] [CrossRef]
- Pacheco-Torgal, F.; Labrincha, J.A.; Leonelli, C.; Palomo, A.; Chindaprasirt, P. Handbook of Alkali-Activated Cements, Mortars and Concretes; Woodhead Publishing: Delhi, India, 2015. [Google Scholar]
- Bureau of Transport and Communications Economics. The Cost of Maintaining the Australian National Highway System; Australian Government Publishing Service: Canberra, Australia, 1992.
- ISO 679:2009-05; Cement—Test Methods—Determination of Strength. ISO: Geneva, Switzerland, 2009.



















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Water Consumption for Standard Consistency (%) | Flexural Strength (MPa) | Compressive Strength (MPa) | ||
|---|---|---|---|---|
| 3 d | 28 d | 3 d | 28 d | |
| 28 | ≥3.5 | ≥6.5 | ≥17 | ≥42.5 |
| Performance Indicators | Density (g/cm3) | 80 μm Sieve Residue (%) | Content of CaO (%) | Content of SiO2 (%) | Content of Al2O3 (%) | MgO in Clinker (%) | Fineness (%) | Stability | Condensation Time (min) | |
|---|---|---|---|---|---|---|---|---|---|---|
| Condensation | Congeal | |||||||||
| standardised requirements | - | - | - | - | - | - | ≤10.0 | eligible (voter etc.) | ≥180 | ≤600 |
| experimental | 3.15 | 0.3 | 62.4 | 21.7 | 6.6 | 2.24 | 3.5 | eligible (voter etc.) | 210 | 250 |
| Characterisation | Apparent Density (kg/m3) | Bulk Density (kg/m3) | Voids (%) | Moisture Content (%) | Mud Content (%) |
|---|---|---|---|---|---|
| request | >2500 | >1350 | <47 | 4%~6% | ≤2.0 |
| measured value | 2614 | 1761 | 35.5 | 4.35% | 0.4 |
| Groups | Water/g | Cement/g | Sand/g | Microencapsulation/g | X/g | Y/g |
|---|---|---|---|---|---|---|
| W1 | 225 | 450 | 1350 | 0 | 0 | 0 |
| W2-1 | 225 | 450 | 1350 | 9 | 4.5 | 0 |
| W2-2 | 225 | 450 | 1350 | 9 | 0 | 4.5 |
| W3-1 | 225 | 450 | 1350 | 18 | 9 | 0 |
| W3-2 | 225 | 450 | 1350 | 18 | 0 | 9 |
| W4-1 | 225 | 450 | 1350 | 27 | 13.5 | 0 |
| W4-2 | 225 | 450 | 1350 | 27 | 0 | 13.5 |
| Modelling | Bulk Modulus (GPa) | Shear Modulus (GPa) | Modulus of Elasticity (GPa) | ||
|---|---|---|---|---|---|
| x | y | z | |||
| T14Å-urea formaldehyde ester | 26.8332 | 9.0122 | 24.6834 | 37.5336 | 20.878 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mao, H.; Cao, X.; Guo, M.; Jiang, C.; Chen, D. Study on the Repair Effect of Self-Healing Cementitious Material with Urea-Formaldehyde Resin/Epoxy Resin Microcapsule. Buildings 2024, 14, 2201. https://doi.org/10.3390/buildings14072201
Mao H, Cao X, Guo M, Jiang C, Chen D. Study on the Repair Effect of Self-Healing Cementitious Material with Urea-Formaldehyde Resin/Epoxy Resin Microcapsule. Buildings. 2024; 14(7):2201. https://doi.org/10.3390/buildings14072201
Chicago/Turabian StyleMao, Hanqing, Xuemei Cao, Minru Guo, Chaozhe Jiang, and De Chen. 2024. "Study on the Repair Effect of Self-Healing Cementitious Material with Urea-Formaldehyde Resin/Epoxy Resin Microcapsule" Buildings 14, no. 7: 2201. https://doi.org/10.3390/buildings14072201