
Study on the Characteristics of Community Elderly Care Service Facilities Usage and Optimization Design Based on Life Cycle Theory



Abstract
1. Introduction
1.1. Background
1.2. Literature Review
1.2.1. The Life Circles Theory
1.2.2. Home-Based or Community Elderly Care
1.2.3. Development of the Elderly Care Service Facilities
1.2.4. Supply of Community Elderly Care Services
1.2.5. Elderly Community Care Needs
2. Method
2.1. Community Elderly Care Service Facility Usage and Demand Characteristics Survey
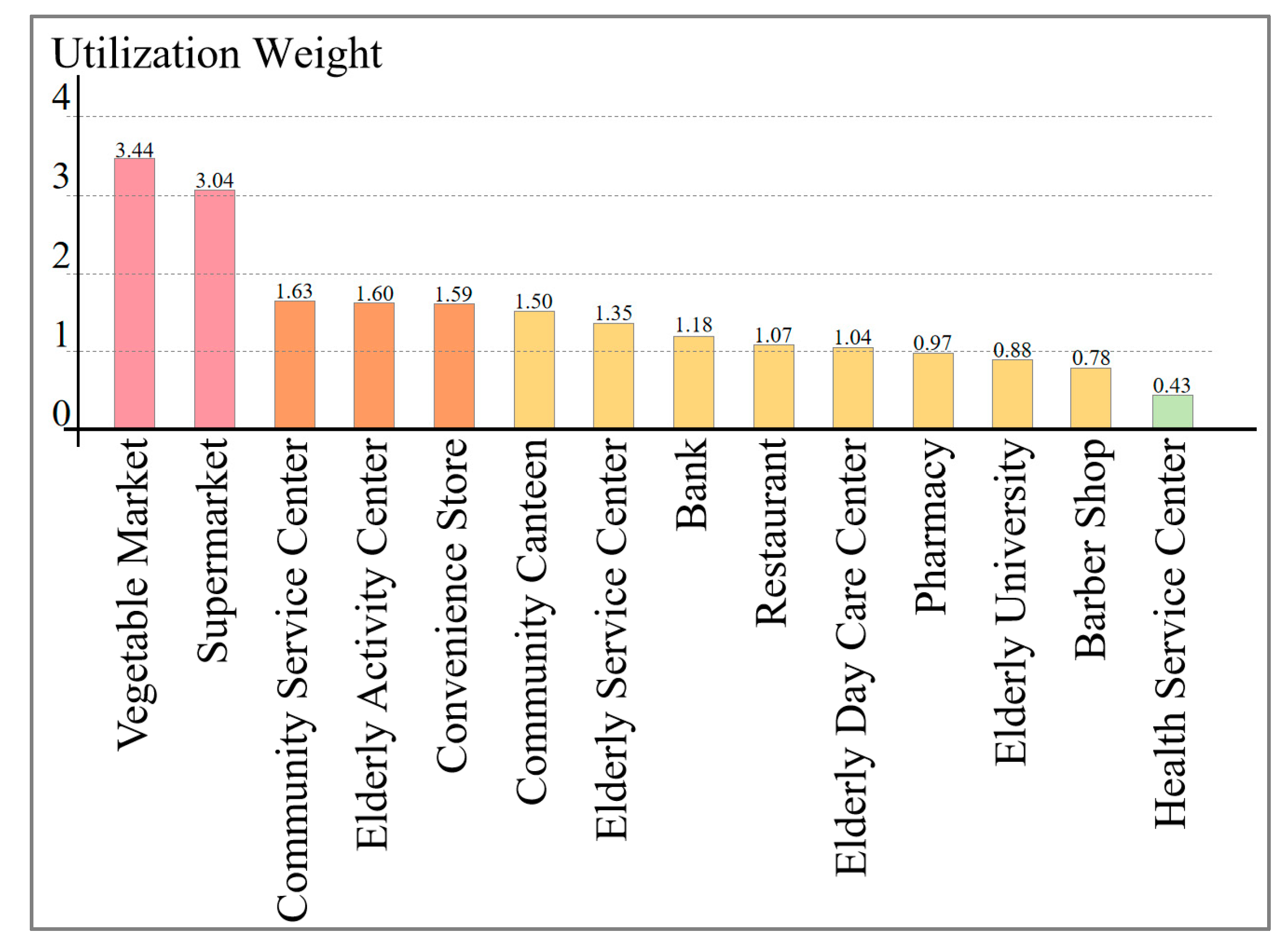
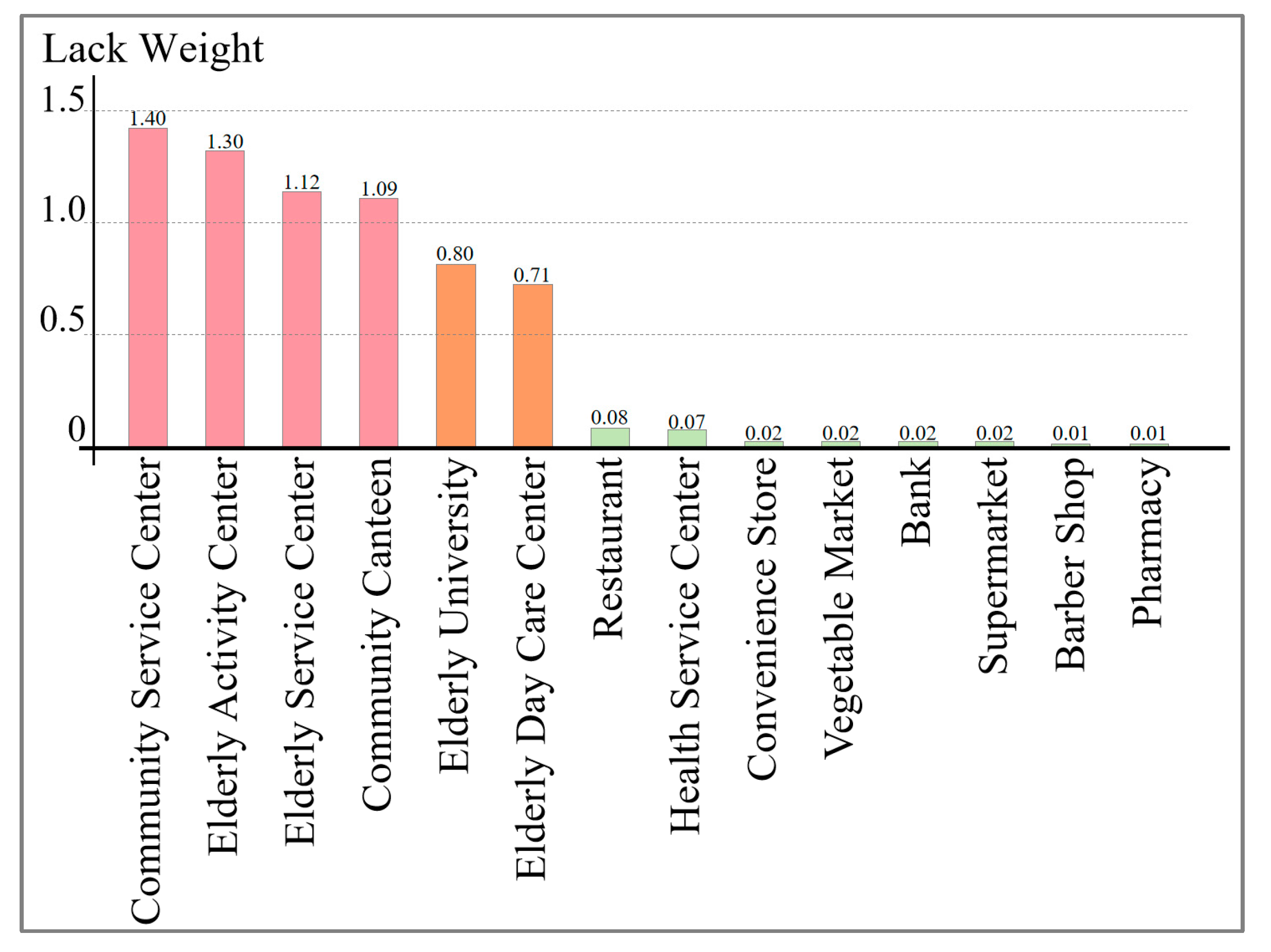
2.2. The Utilization Weight and Lack Weight of Facilities
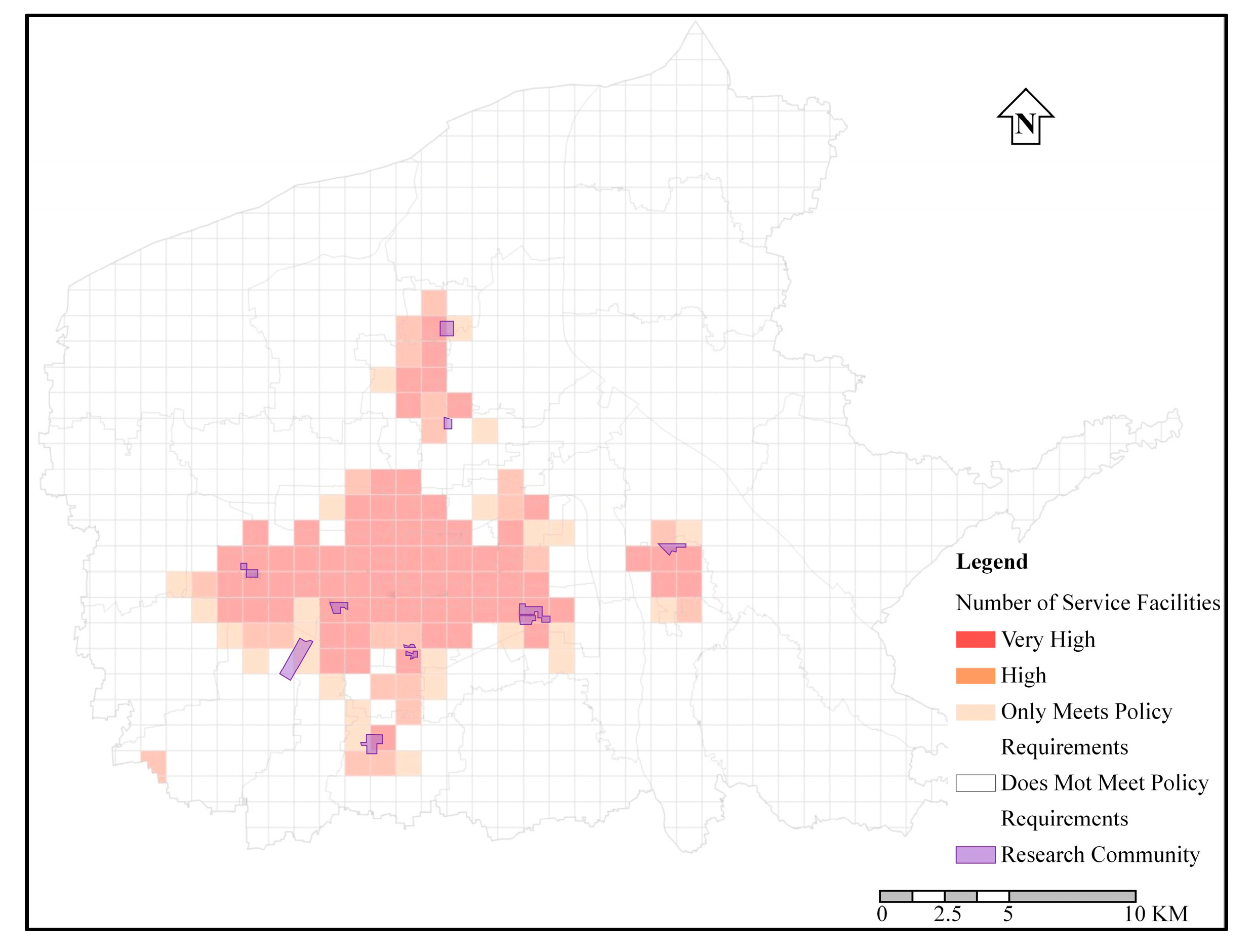
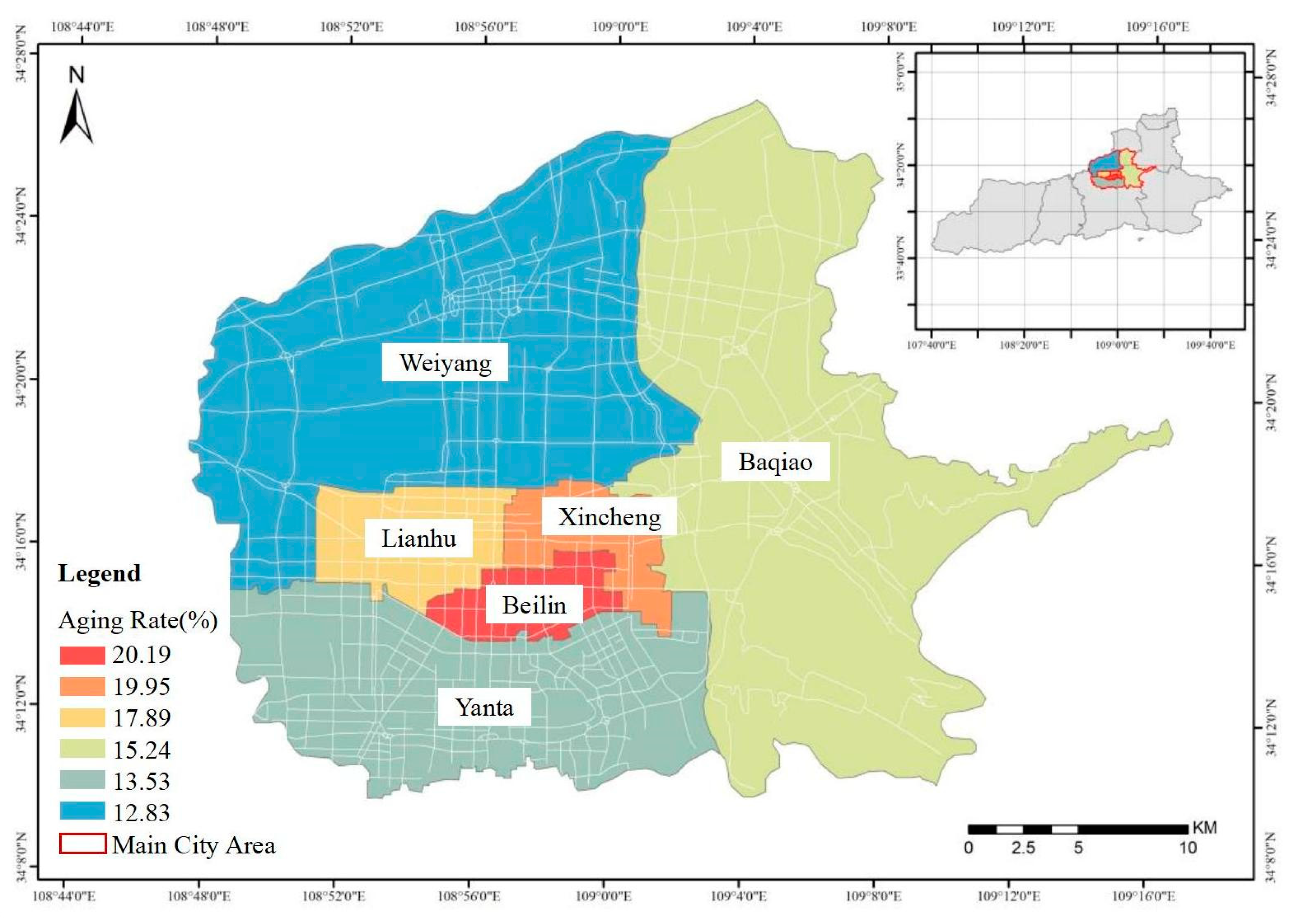
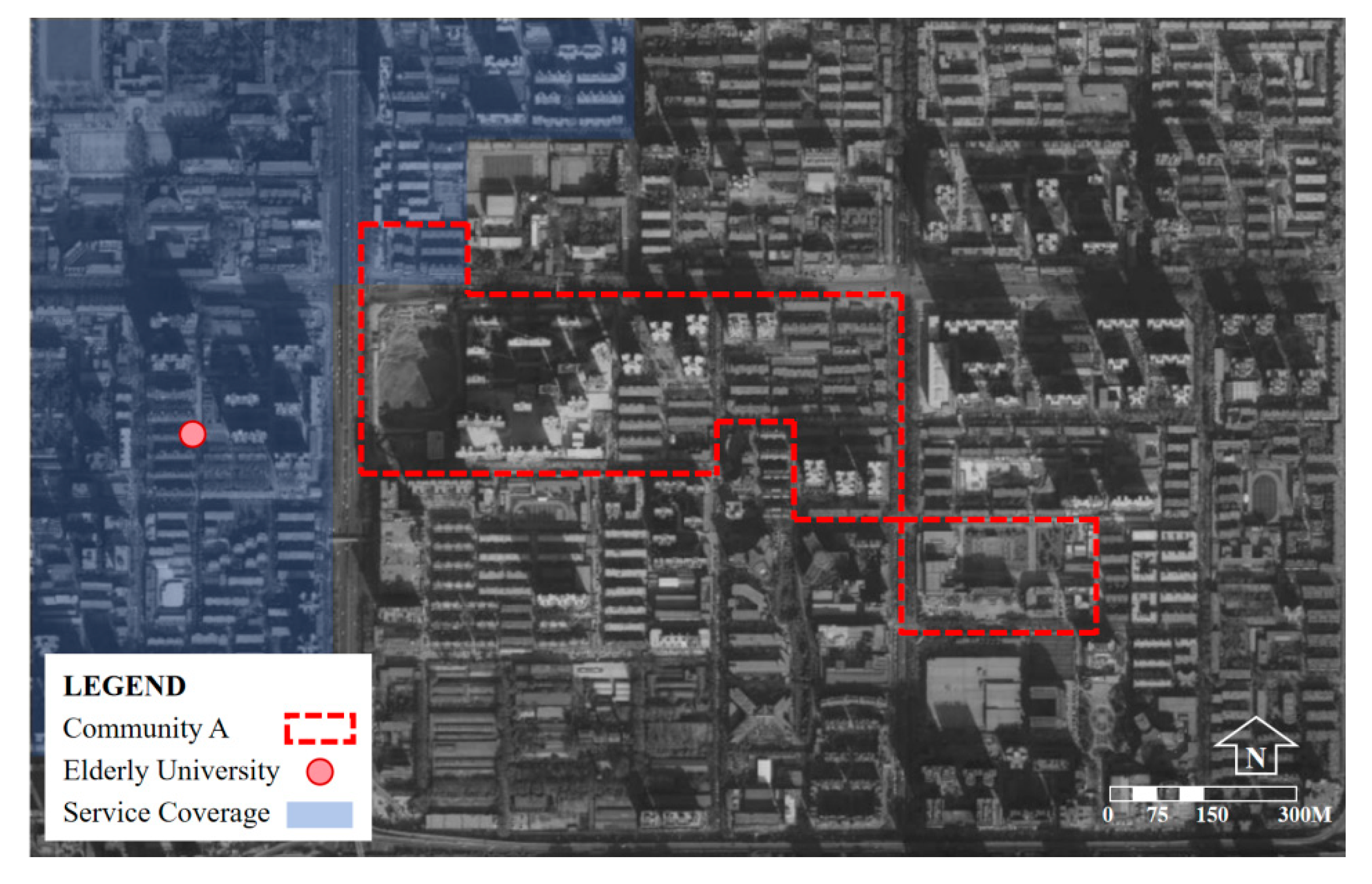
2.3. Research Area
3. Result
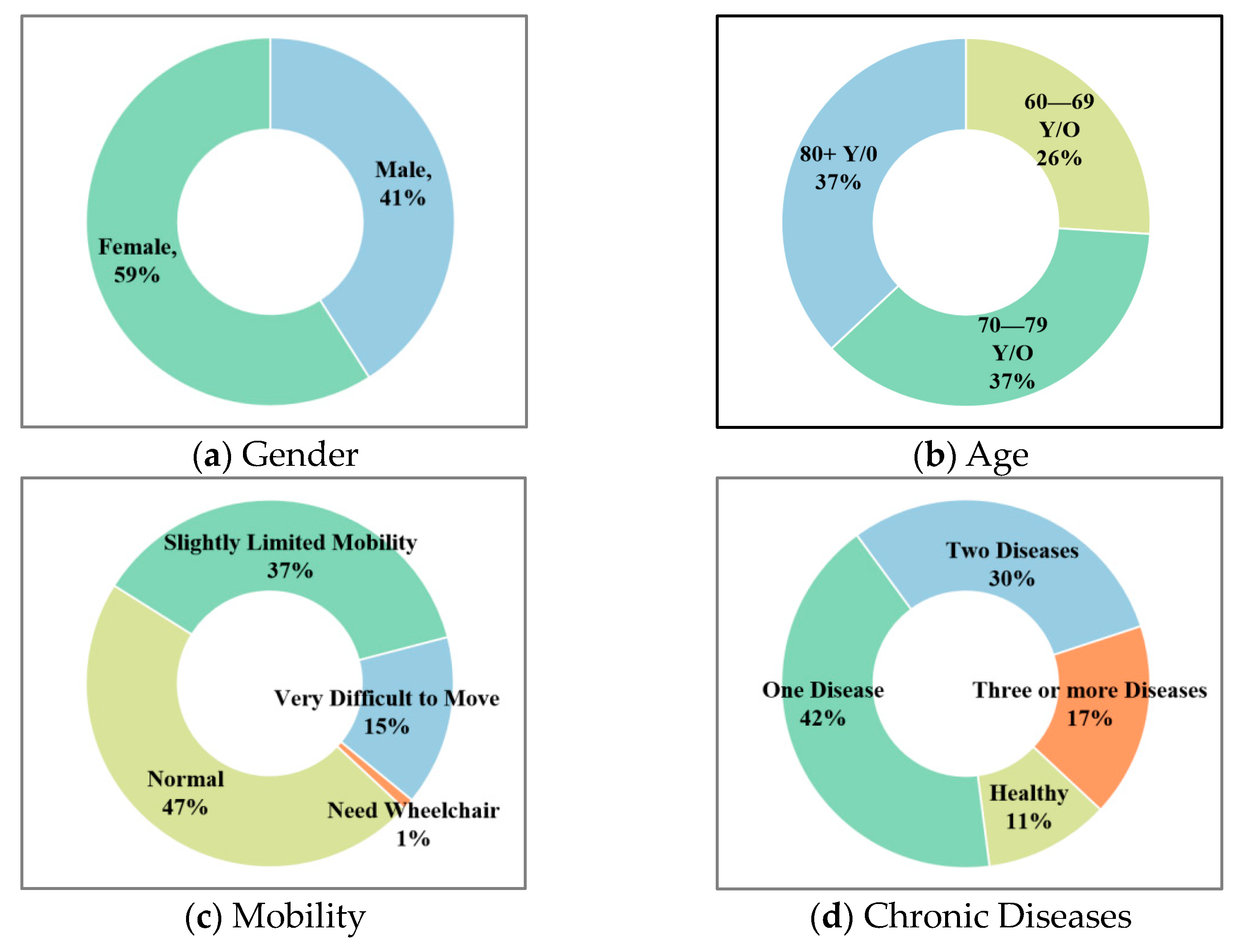
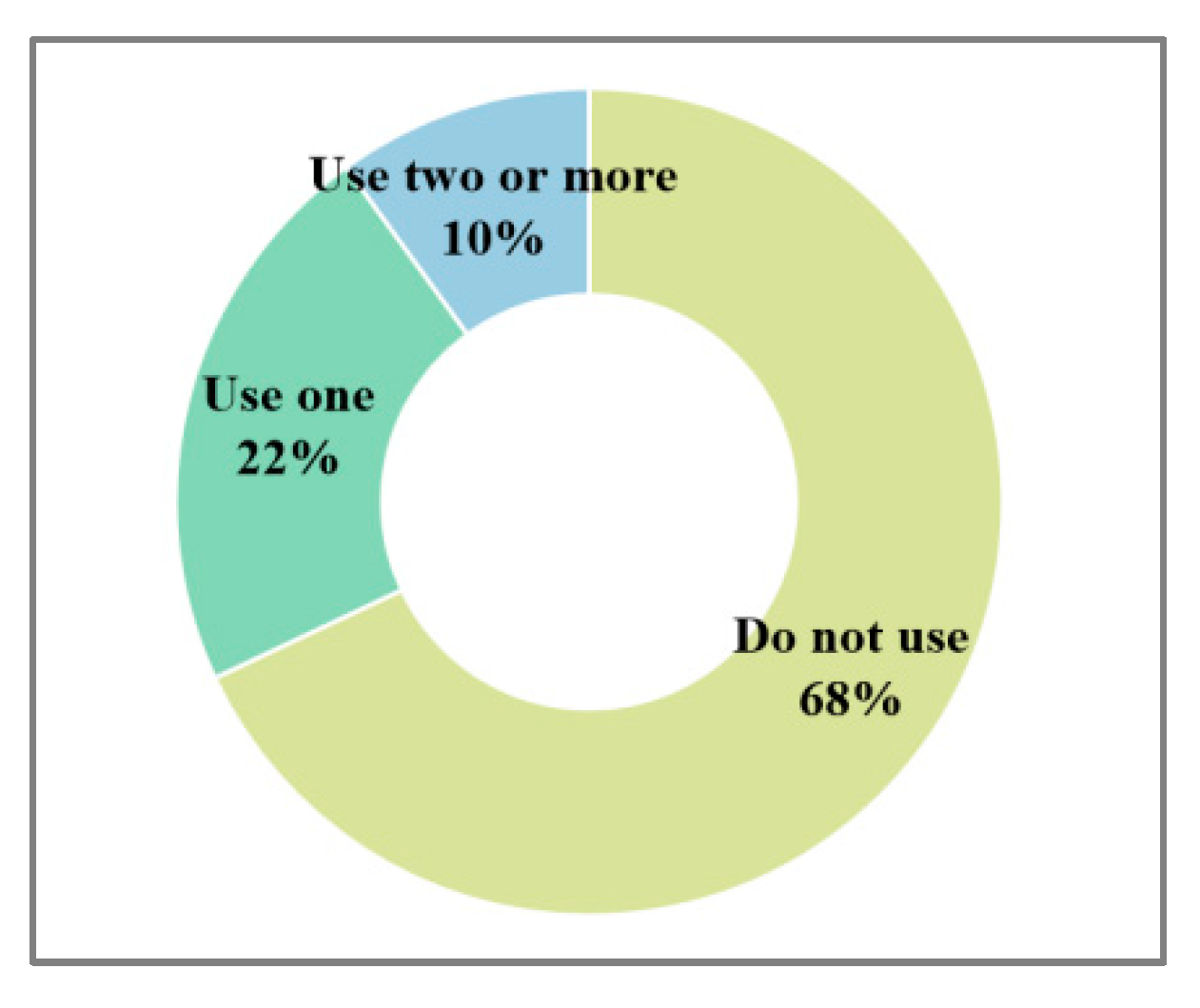
3.1. Basic Information
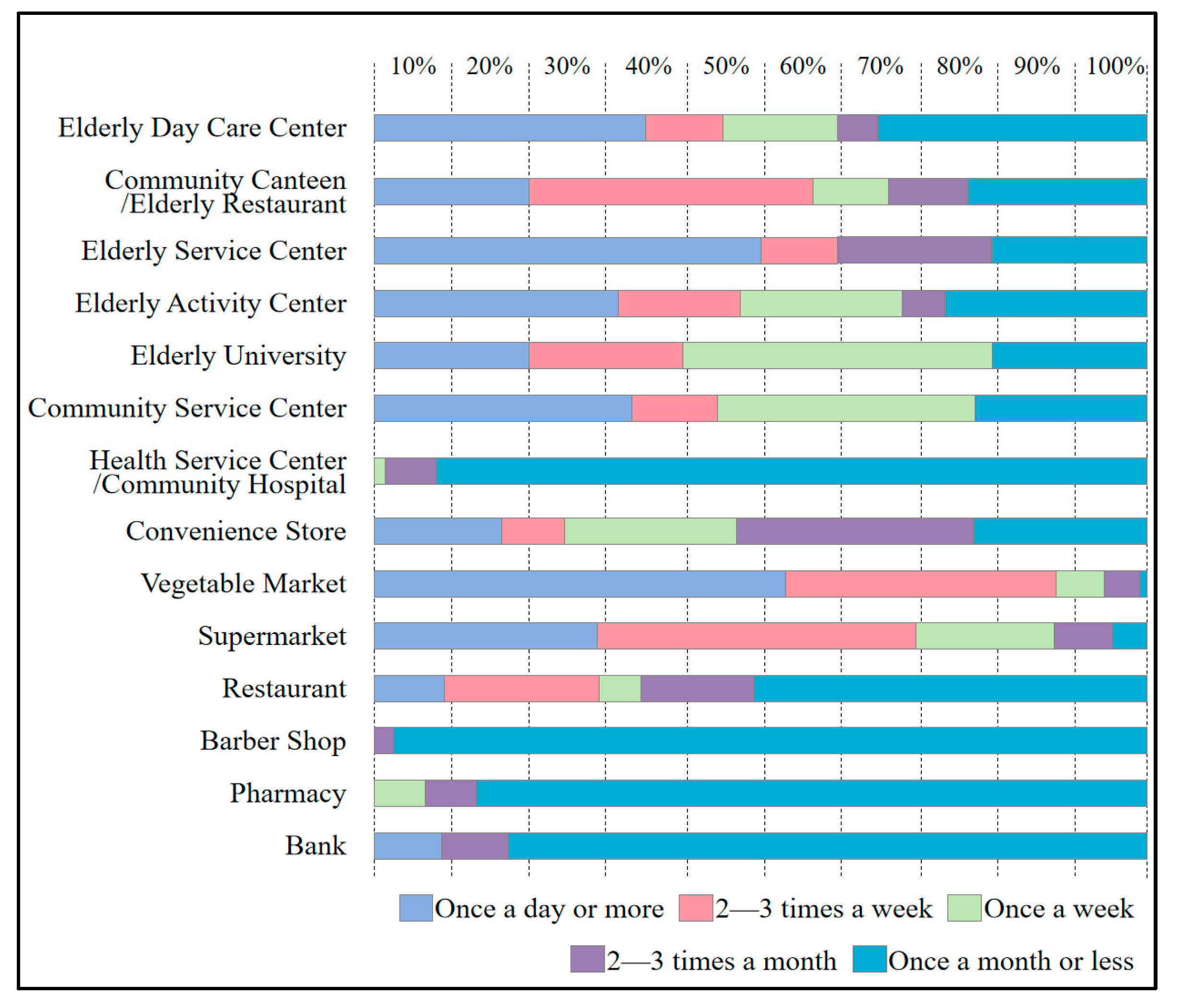
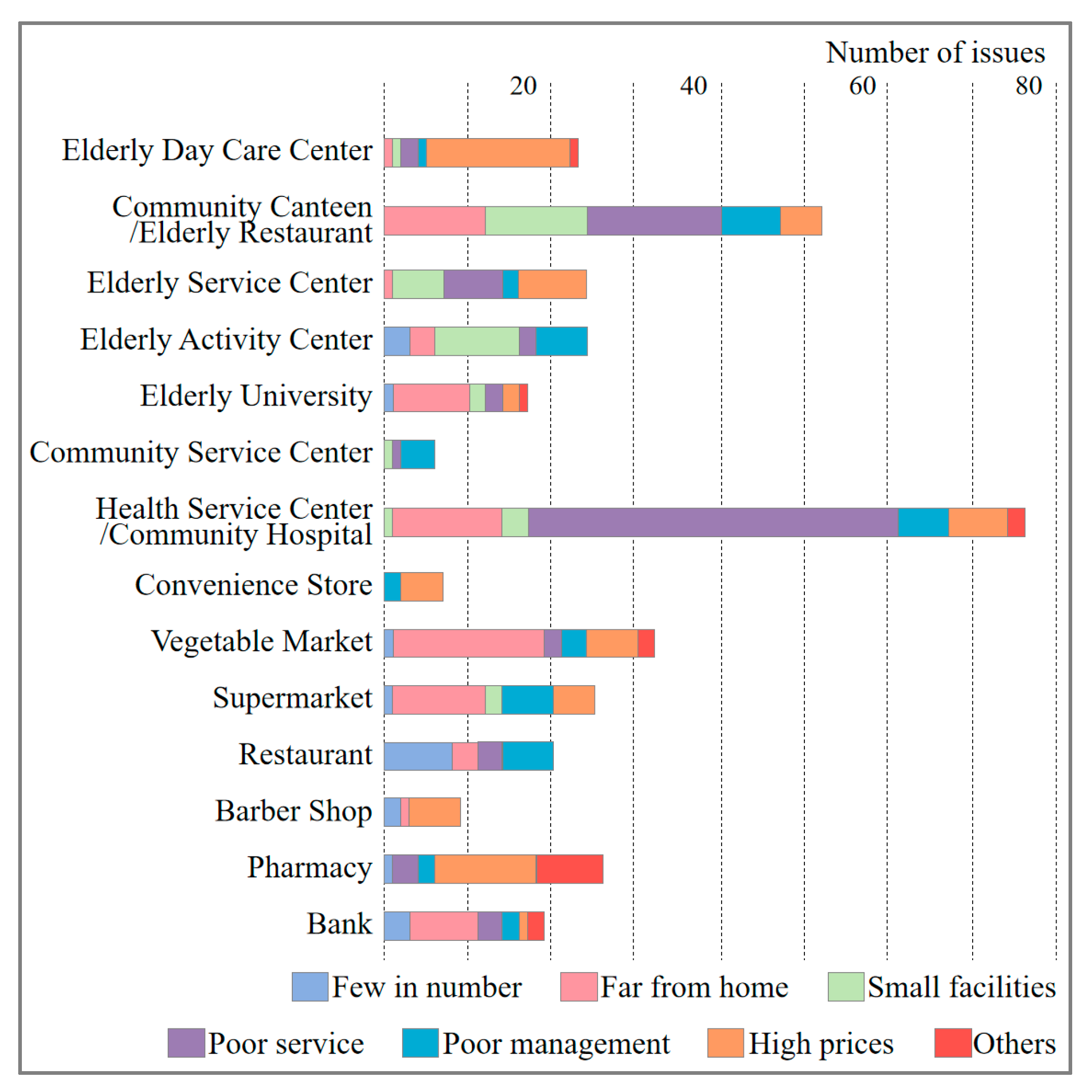
3.2. The Demand Characteristics of Elderly Care Service Facilities
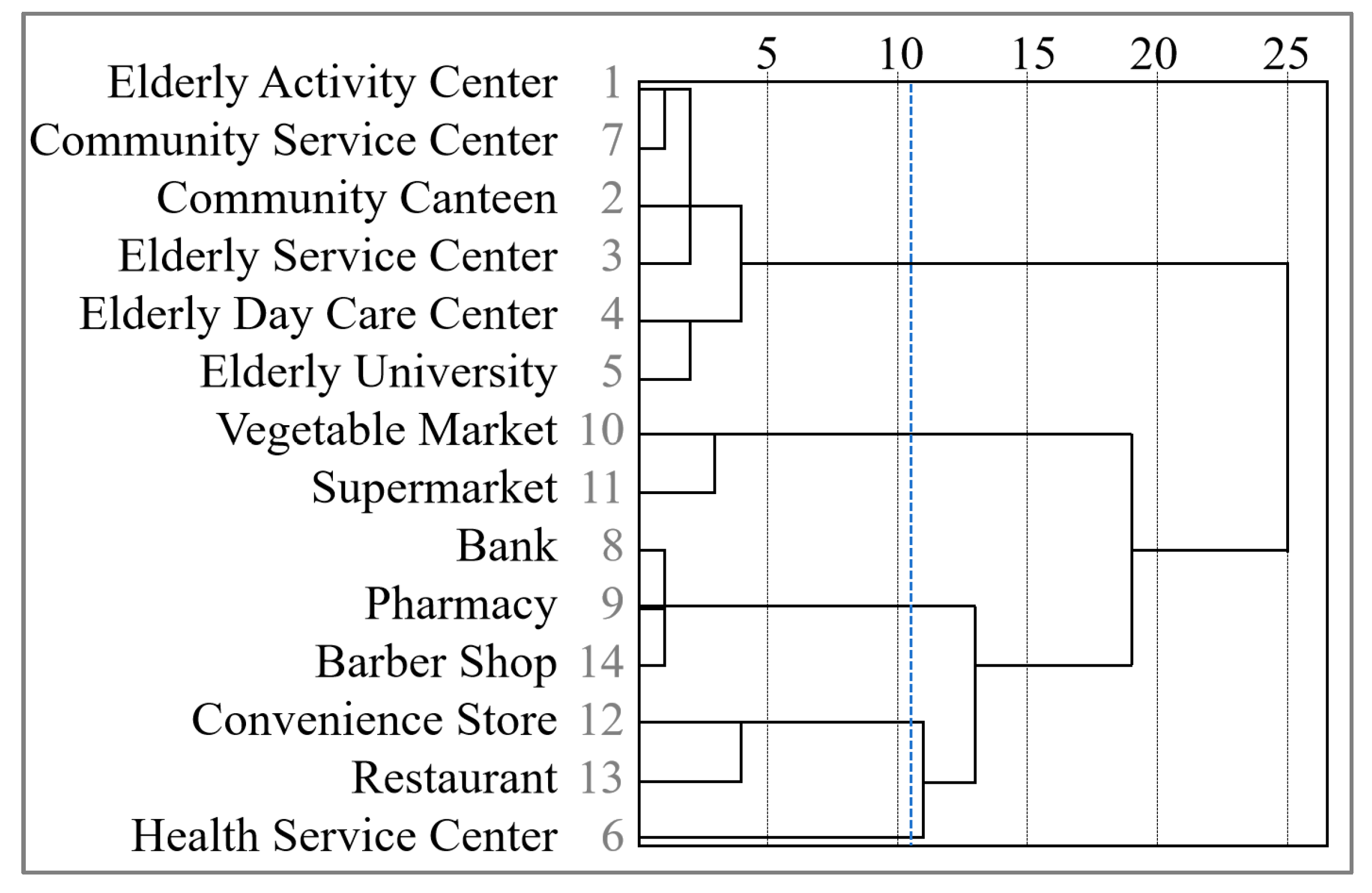
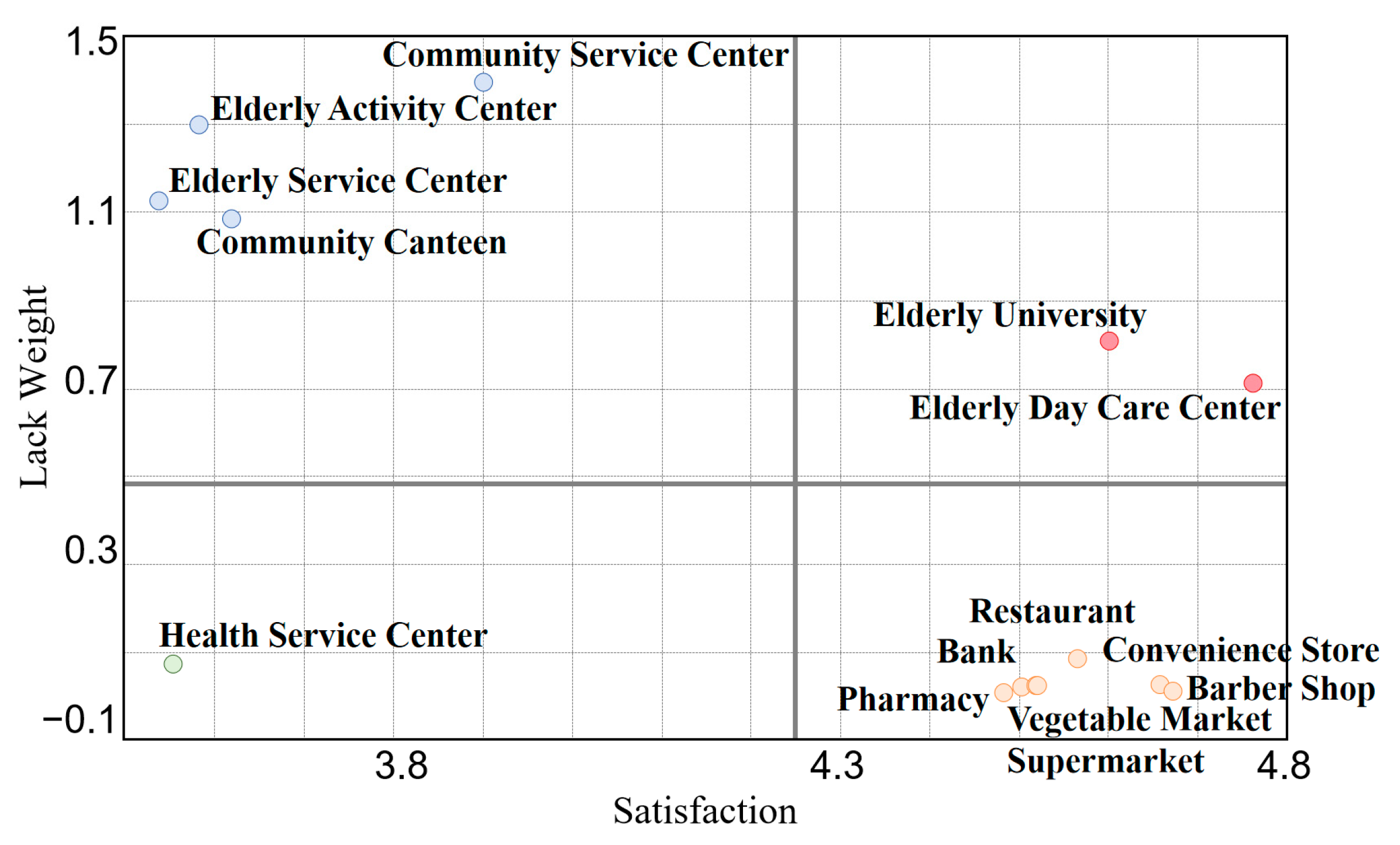
3.3. The Utilization and Lack Weight of Elderly Care Service Facilities
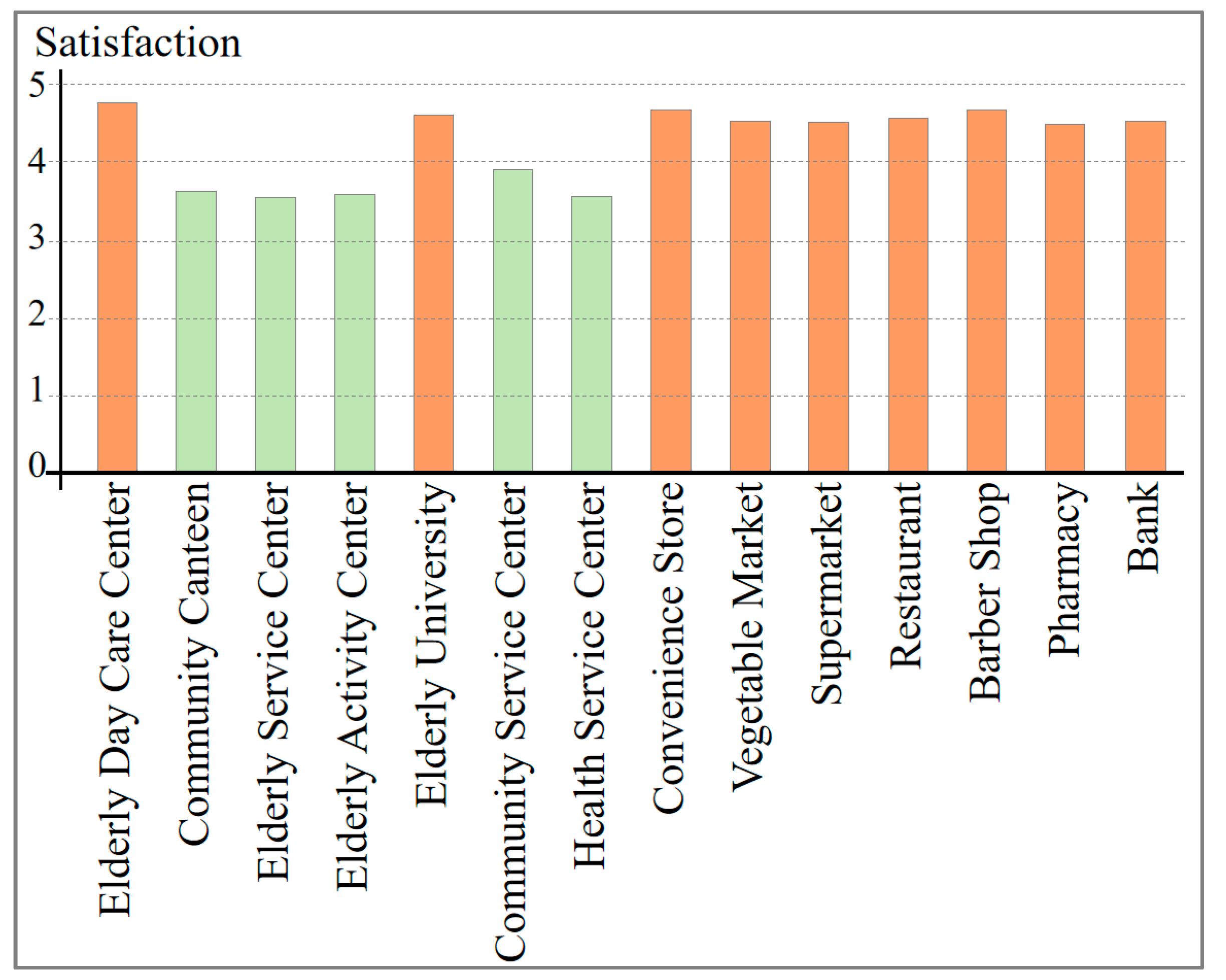
3.4. Satisfaction with the Utilization of Elderly Care Service Facilities
3.5. Demand Characteristics of Facilities among Different Types of Elderly
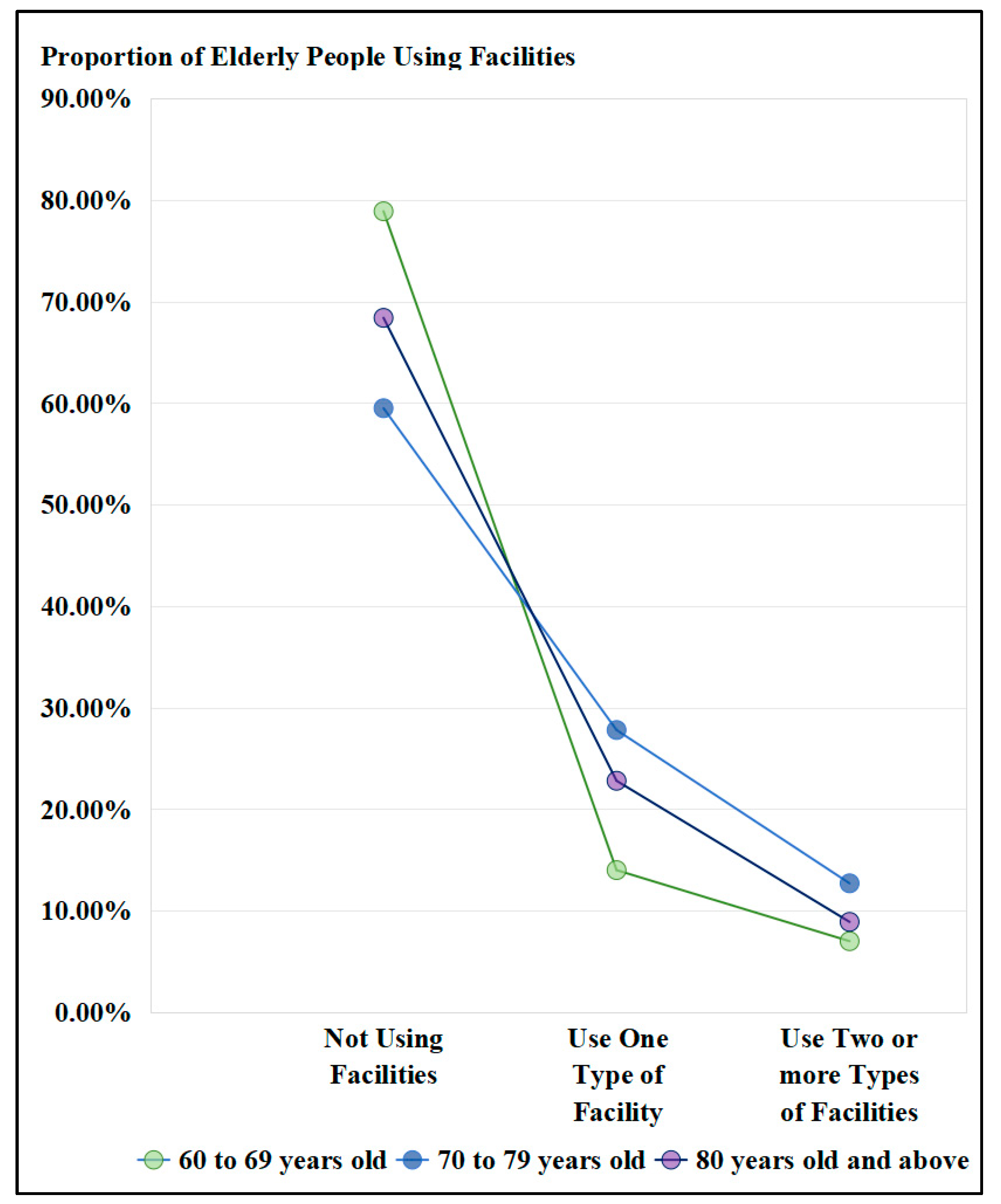
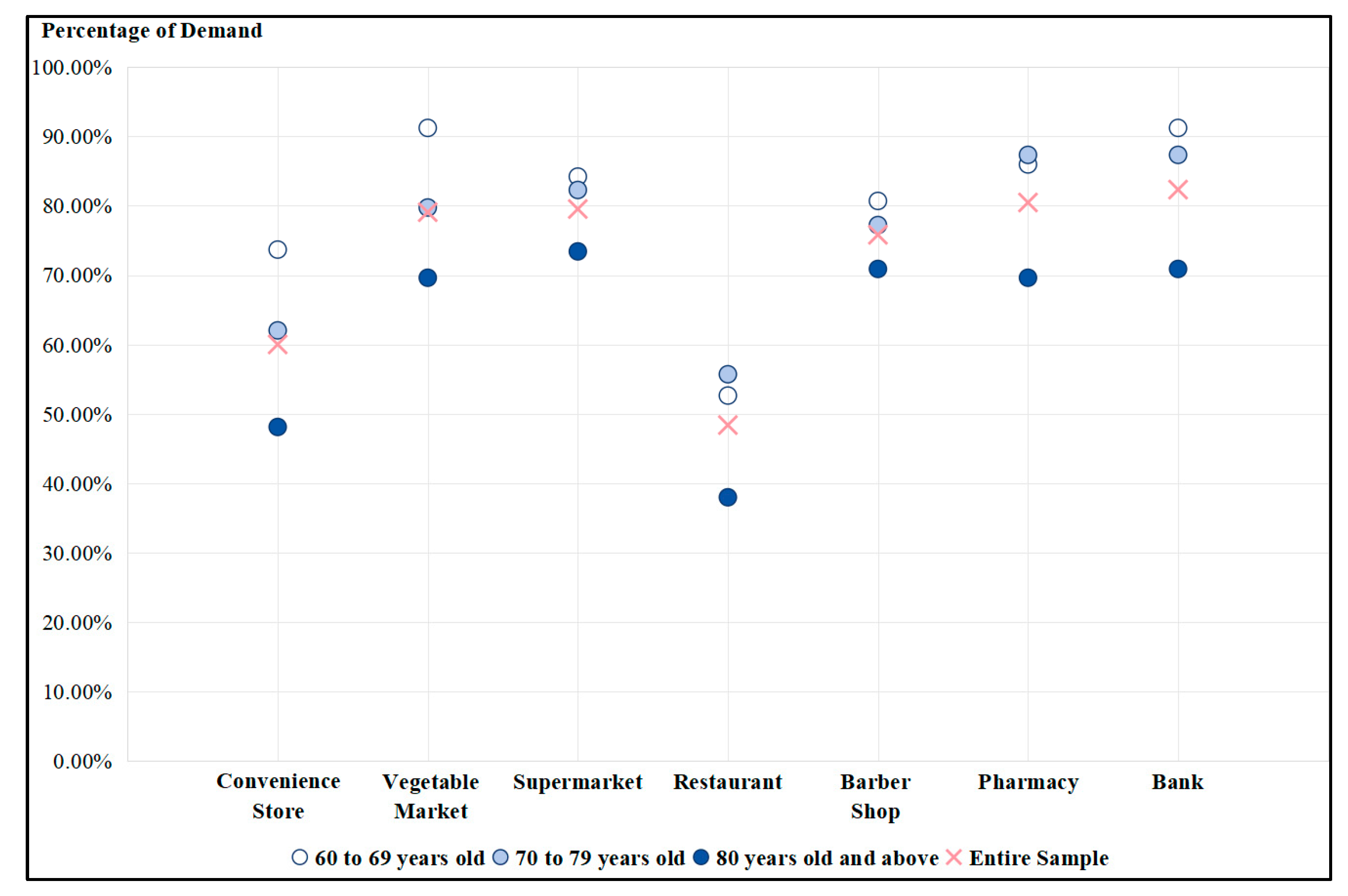
3.5.1. Different Age Groups
3.5.2. Different Activity Capacity
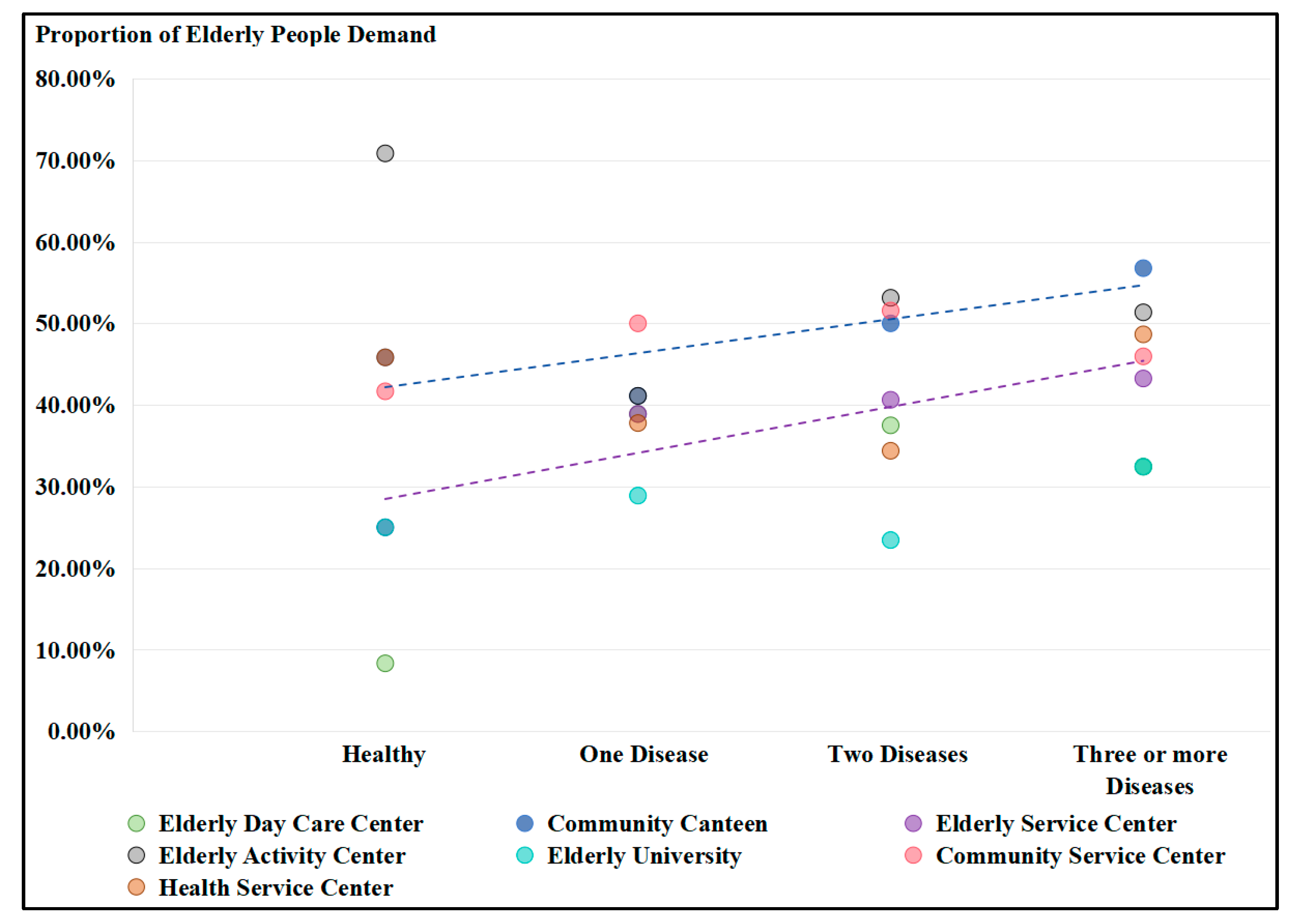
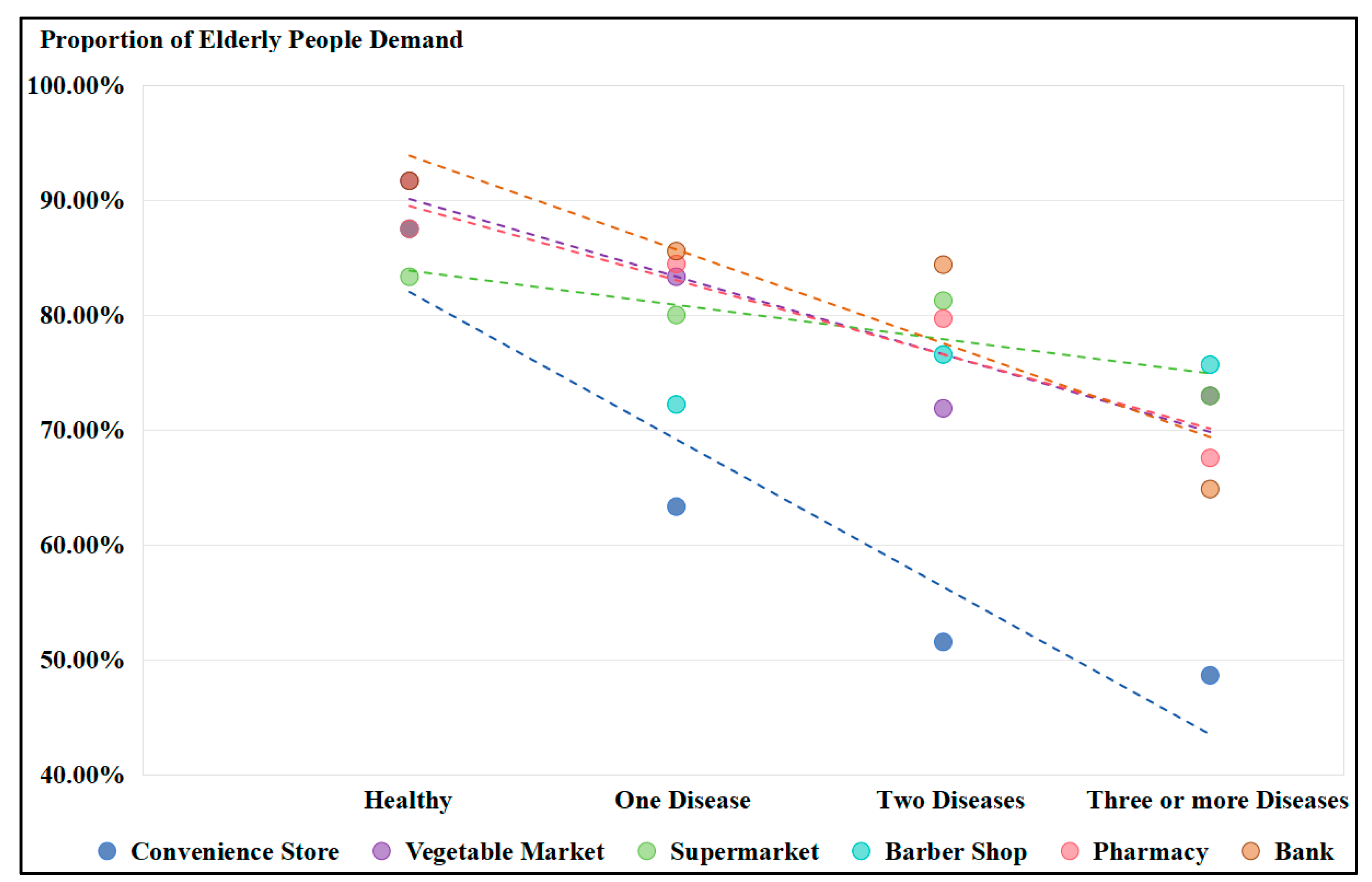
3.5.3. Different Chronic Diseases
4. Discussion
4.1. Characteristics of Elderly Needs Affecting the Planning of Community Service Facilities
4.2. The Impact of Elderly Needs Characteristics on Urban Development
4.2.1. The Facility Needs of the Elderly and Its Impact on Daily Living Behaviors
4.2.2. The Potential for Improved Elderly Needs Satisfaction through the Optimized Design of Service Facilities
4.3. Optimization Strategies for Community Elderly Care Service Facilities
4.3.1. The Quantity of Facilities
4.3.2. The Spatial Layout of Facilities
4.3.3. The Quality of Facilities
4.3.4. Service Management
5. Conclusions
6. Limitations
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Appendix A
- Your gender is: ○ male/○ female
- Your age is: _year
- Your community is: _village
- Who do you live with? (Type in the conforming box)
| Grandchildren | Sons and Daughters | Man and Wife | Elder Member of a Family | Be on One’s Own |
- 5.
- Do you suffer from the following diseases?
- ○
- hypertension
- ○
- diabetes mellitus
- ○
- asthma
- ○
- Cardiac and cerebrovascular diseases (coronary heart disease, cerebral infarction, cerebral atrophy, cerebral hemorrhage, etc.)
- ○
- Stomach disease (chronic gastritis, gastric ulcer, etc.)
- ○
- Chronic lung disease (bronchitis, emphysema, etc.)
- ○
- therioma
- ○
- Cataract/glaucoma
- ○
- Reproductive system diseases
- ○
- Ostearthropathy (rheumatism, arthritis, disc disease, etc.)
- ○
- other diseases
- ○
- was free from any disease
- 6.
- How good is your mobility?
- ○
- was perfectly normal
- ○
- The legs and feet are not very flexible
- ○
- Action is very difficult
- ○
- A wheelchair is required to travel
- 7.
- Are there any old service facilities or community pension-related public service facilities around your community? If not, do you need/if so, do you use it, is the reason you do not use it?
| Facility Name | No and No Need | No But Need | Have But Do Not Use | Have and Use | The Reason |
| Senior activity center/station | |||||
| Community canteen/restaurant for the elderly | |||||
| Senior service center/station | |||||
| Day-care centers for the elderly | |||||
| College teaching sites for the elderly | |||||
| Health service center/station/community hospital | |||||
| Community service center/station | |||||
| (Note: Reasons for not using: A person does not need, B facility is far away from home, C facility room is small, D service level is low, E management is not in place, and F price is high). | |||||
- 8.
- For the following old service facilities and public service facilities related to community pension, what is your use and satisfaction? What do you think is the current problem of the facilities?
| Installation | Senior Activity Center/Station | Community Canteen/Restaurant for the Elderly | Senior Service Center/Station | Day-Care Centers for the Elderly | College Teaching Sites for the Elderly | Health Service Center/Station/Community Hospital | Community Service Center/Station |
| satisfaction | |||||||
| The status of the problem | |||||||
| walking time | |||||||
| Walking experience | |||||||
| operating frequency | |||||||
| service time | |||||||
| Room size | |||||||
| (Note: Satisfaction; A is very dissatisfied, B is relatively dissatisfied, C is general, D is relatively satisfied, E is very satisfied; Current problems: the number of A facilities is small, B facilities is far away from home, C facilities room is small, D service level is low, E management is not in place, F price is high; walking time: A. Within 5 min, the B. For 5–10 min, and for C. For 10–15 min, and for D. For 15–30 min, and for E. More than 30 min. Walking experience: A. Too long a time is unbearable, B. Long time is tolerable, C. The right time is more convenient; Frequency of use: A. Once or more daily, and B. Two and three times a week, and C. Once a week, and D. 2 times and 3 times per month, E. Once a month or less; Usage time: A. Within 5 min, the B. For 5–15 min, and for C. For 15–30 min, and for D. 30 min–1 h, and E. More than 1 h; Room size: A. Is more crowded, and B. size to fit, C. More empty). | |||||||
- 9.
- Do you use the following community pension related life service facilities, do you use them or do them for your children? What is your satisfaction? Do you think of the current problem of the facilities? What other personalized facilities do you need/often use (TCM clinic/health massage/)?
| Respect | Bank | Pharmacy/Pharmaceutical Sales | Vegetable market | Supermarket | Convenient Store | Catering 2. Food & Beverage | Beauty Hair | |
| Whether to use | ||||||||
| Satisfaction score | ||||||||
| operating frequency | ||||||||
| service time | ||||||||
| The status of the problem | ||||||||
| (Note: whether to use: A has no and do not need, B has no but need, C has but do not use, D has and use, E children for the wo). | ||||||||
References
- National Bureau of Statistics. The Seventh National Population Census Bulletin, Population Age Structure. Available online: http://www.stats.gov.cn/sj/tjgb/rkpcgb/qgrkpcgb/202302/t20230206_1902005.html (accessed on 11 May 2021).
- State Council. Notice of the State Council on Issuing the “14th Five-Year Plan” for the Development of Aging Affairs and the Elderly Care Service System. Available online: http://www.gov.cn/zhengce/content/2022-02/21/content_5674844.htm (accessed on 21 February 2022).
- Xu, M.; Zhao, Y.; You, J.; Wang, B.Y.; Li, Z. Preference and Influencing Factors of Community Home-based Elderly Care in Community-living Elderly People in Nanning. Chin. Gen. Pract. 2020, 23, 2328–2334. (In Chinese) [Google Scholar] [CrossRef]
- GB 50180—2018; Urban Residential Area Planning and Design Standard. Architecture & Building Press: Beijing, China, 2018. Available online: https://www.chinesestandard.net/PDF/English.aspx/GB50180-2018 (accessed on 19 September 2024).
- Huang, J.; Zhang, R.; Hu, G. Research on the Daily Life Circle of the Elderly Based on Spatiotemporal Behavior—Spatial Identification and Feature Analysis. Urban Plan. Forum 2019, 87–95. (In Chinese) [Google Scholar] [CrossRef]
- Department of Circulation Development. Notice of the General Office of the Ministry of Commerce and 11 Other Departments on Issuing the “Urban 15-Minute Convenience Life Circle Construction Guide”. Available online: http://www.mofcom.gov.cn/article/h/redht/202107/20210703179512.shtml (accessed on 20 July 2021).
- Ministry of Natural Resources of the People’s Republic of China. Technical Guidelines for Community Life Circle Planning: TD/T 1062-2021. 2021. Available online: http://www.nrsis.org.cn/portal/stdDetail/240432 (accessed on 19 September 2024).
- Office of the Ministry of Housing and Urban-Rural Development. Notice of the Office of the Ministry of Housing and Urban-Rural Development on Issuing the Guide for the Construction of Complete Residential Communities. Available online: https://www.gov.cn/zhengce/zhengceku/2022-01/12/content_5667815.htm (accessed on 17 December 2021).
- Liu, Q.; Qian, Z.; Huang, D.; Zhou, X. Spatial pattern evolution characteristics and trends of 15 min9ute living circle. J. Urban Plan. 2020, 6, 94–101. (In Chinese) [Google Scholar]
- Xiao, Z.; Chai, Y.; Zhang, Y. Review of the Progress in Research and Practice of Life Circle Planning at Home and Abroad. Planner 2014, 30, 89–95. (In Chinese) [Google Scholar]
- Li, Y.; Chai, Y.; Ta, N. From Disaster Prevention Life Circle to Safe Life Circle: Japanese Experience and Chinese Reflection. Int. Urban Plan. 2022, 37, 113–120. (In Chinese) [Google Scholar] [CrossRef]
- Xiao, Z.; Han, L.; Chai, Y. Reflections on Integrating Life Circle Planning into National Spatial Planning. Planner 2022, 38, 145–151. (In Chinese) [Google Scholar]
- Da Silva, D.C.; King, D.A.; Lemar, S. Accessibility in Practice: 20-Minute City as a Sustainability Planning Goal. Sustainability 2019, 12, 129. [Google Scholar] [CrossRef]
- Moreno, C.; Allam, Z.; Chabaud, D.; Gall, C.; Pratlong, F. Introducing the “15-Minute City”: Sustainability, Resilience and Place Identity in Future Post-Pandemic Cities. Smart Cities 2021, 4, 93–111. [Google Scholar] [CrossRef]
- United Nations, Department of Economic and Social Affairs. World Population Ageing. 2017. Available online: https://www.un.org/development/desa/pd/content/world-population-ageing-2017 (accessed on 1 October 2017).
- Tang, X.; Zhou, Y. Community Renewal Strategy for Implementing on site Elderly Care: A Study of Naturally Formed Retirement Communities (NORC) in the United States. J. Archit. 2018, 2, 80–84. (In Chinese) [Google Scholar]
- Peng, Y.; Zhou, S.; Wen, P. German Multi Generational Mutual Aid Community Elderly Care Model and Its Implications. Shanghai Urban Plan 2021, 103–108. Available online: https://www.shplanning.com.cn/archive/detail/id/980.html (accessed on 4 August 2024). (In Chinese).
- Zhu, W.; Lin, Y. Construction of the “Medical Elderly Integration” Community Elderly Care Model in Japan and Its Implications for China: Based on the Perspective of Institutional Analysis. Southwest Financ. 2022, 1, 76–87. (In Chinese) [Google Scholar]
- Wiles, J.L.; Leibing, A.; Guberman, N.; Reeve, J.; Allen, R.E. The Meaning of “Aging in Place” to Older People. Gerontologist 2012, 52, 357–366. [Google Scholar] [CrossRef] [PubMed]
- Oswald, F.; Jopp, D.; Rott, C.; Wahl, H.W. Is Aging in Place a Resource for or Risk to Life Satisfaction? Gerontologist 2011, 51, 238–250. [Google Scholar] [CrossRef] [PubMed]
- Kerr, J.; Rosenberg, D.; Frank, L. The Role of the Built Environment in Healthy Aging. J. Plan. Lit. 2012, 27, 43–60. [Google Scholar] [CrossRef]
- Rosso, A.L.; Grubesic, T.H.; Auchincloss, A.H.; Tabb, L.P.; Michael, Y.L. Neighborhood Amenities and Mobility in Older Adults. Am. J. Epidemiol. 2013, 178, 761–769. [Google Scholar] [CrossRef]
- Curl, A.; Mason, P. Neighbourhood Perceptions and Older Adults’ Wellbeing: Does Walking Explain the Relationship in Deprived Urban Communities? Transp. Res. Part. A Policy Pract. 2019, 123, 119–129. [Google Scholar] [CrossRef]
- Apparicio, P.; Abdelmajid, M.; Riva, M.; Shearmur, R. Comparing Alternative Approaches to Measuring the Geographical Accessibility of Urban Health Services: Distance Types and Aggregation-error Issues. Int. J. Health Geogr. 2008, 7, 7. [Google Scholar] [CrossRef]
- Bauer, J.; Groneberg, D.A. Measuring Spatial Accessibility of Health Care Providers—Introduction of a Variable Distance Decay Function within the Floating Catchment Area (FCA) Method. PLoS ONE 2016, 11, e0159148. [Google Scholar] [CrossRef]
- Benevenuto, R.; Caulfield, B. Measuring Access to Urban Centres in Rural Northeast Brazil: A Spatial Accessibility Poverty Index. J. Transp. Geogr. 2020, 82, 102553. [Google Scholar] [CrossRef]
- Dadashpoor, H.; Rostami, F.; Alizadeh, B. Is Inequality in the Distribution of Urban Facilities Inequitable? Exploring a Method for Identifying Spatial Inequity in an Iranian City. Cities 2016, 52, 159–172. [Google Scholar] [CrossRef]
- Jang, S.; An, Y.; Yi, C.; Lee, S. Assessing the Spatial Equity of Seoul’s Public Transportation Using the Gini Coefficient Based on Its Accessibility. Int. J. Urban Sci. 2016, 21, 91–107. [Google Scholar] [CrossRef]
- Sharma, G.; Patil, G.R. Public Transit Accessibility Approach to Understand the Equity for Public Healthcare Services: A Case Study of Greater Mumbai. J. Transp. Geogr. 2021, 94, 103–123. [Google Scholar] [CrossRef]
- Lee, S. Spatial and Socioeconomic Inequalities in Accessibility to Healthcare Services in South Korea. Healthcare 2022, 10, 2049. [Google Scholar] [CrossRef] [PubMed]
- AHiggins, J. Comparative social policy. Q. J. Soc. Aff. 1986, 3, 90–91. [Google Scholar]
- Pinker, R. Making Sense of the Mixed Economy of Welfare. Soc. Policy Adm. 1992, 4, 273–284. [Google Scholar] [CrossRef]
- Shaw, W.S.; Patterson, T.L.; Semple, S.J.; Halpain, M.C.; Koch, W.L.; Harris, M.J.; Grant, I.; Jeste, D.V. Use of community support services by middle-aged and older patients with psychotic disorders. Psychiatr. Serv. 2000, 51, 506–512. [Google Scholar] [CrossRef]
- Sumini, S.; Sukamdi, E.; Pangaribowo, E.H.; Keban, Y.T.; Darwin, M.; Grosset, J.F. Elderly Care: A Study on Community Care Services in Sleman, DIY, Indonesia. J. Aging Res. 2020, 7, 3983290. [Google Scholar] [CrossRef]
- Wang, Y.H.; Hsu, N.W.; Huang, H.Y.; Tsai, C.C.; Pan, P.J. Effectiveness of a machine-assisted healthy physical fitness promotion program for community elderly. J. Chin. Med. Assoc. JCMA 2020, 83, 779–783. [Google Scholar] [CrossRef]
- Lin, H.R.; Otsubo, T.; Imanaka, Y. Survival analysis of increases in care needs associated with dementia and living alone among older long-term care service users in Japan. BMC Geriatr. 2017, 17, 182. [Google Scholar] [CrossRef]
- Hajek, A.; Lehnert, T.; Wegener, A.; Riedel-Heller, S.G.; König, H.H. Factors associated with preferences for long-term care settings in old age: Evidence from a population-based survey in Germany. BMC Health Serv. Res. 2017, 17, 156. [Google Scholar] [CrossRef]
- Madeira, T.; Peixoto-Plácido, C.; Sousa-Santos, N.; Santos, O.; Alarcão, V.; Nicola, P.J.; Lopes, C.; Gorjão, C.J. Geriatric Assessment of the Portuguese Population Aged 65 and Over Living in the Community: The PEN-3S Study. Acta Medica Port. 2020, 33, 475–482. [Google Scholar] [CrossRef]
- Joyce, S.; Berry, H.; Jorgensen, M.; Brett, L.; Georgiou, A.; McClean, T.; Westbrook, J. Social Participation Among Older Adults Receiving Community Care Services. J. Appl. Gerontol. Off. J. South. Gerontol. Soc. 2020, 40, 997–1007. [Google Scholar]
- Hee, J.K.; Park, J.; Ryu, S.Y. The effects of mental health on recurrent falls among elderly adults, based on Korean Community Health Survey data. Epidemiol. Health 2020, 42, e2020005. [Google Scholar]
- Doughty, K.; Williams, G. New models of assessment and prescription of smart assisted living technologies for personalised support of older and disabled people. J. Assist. Technol. 2016, 10, 39–50. [Google Scholar] [CrossRef]
- Ministry of Housing and Urban-Rural Development of the People’s Republic of China. Code for Design of Elderly Care Facilities: JGJ 450-2018. 2018. Available online: https://www.soujianzhu.cn/NormAndRules/NormContent.aspx?id=324 (accessed on 19 September 2024).
- Ministry of Housing and Urban-Rural Development of the People’s Republic of China. Urban Planning Standards for the Elderly Facilities: GB 50437-2007. 2018. Available online: https://www.soujianzhu.cn/NormAndRules/NormContent.aspx?id=376 (accessed on 19 September 2024).
- Xi’an Municipal Bureau of Statistics. Main Data Bulletin of the Seventh National Population Census in Xi’an. Available online: http://tjj.xa.gov.cn/rdzt/xapc/60b47af8f8fd1c0bdc2d59c0.html (accessed on 31 May 2021).
- General Office of Xi’an Municipal People’s Government. Notice on Issuing the Layout Plan of Elderly Care Service Facilities in Xi’an (2018–2030). Available online: https://www.xa.gov.cn/gk/zcfg/szbf/5d495b2765cbd87465b11025.html (accessed on 7 January 2019).
- Survey Center of Xi’an Municipal Bureau of Statistics. Survey Report on the Living Conditions and Elderly Care Status of Elderly People in Xi’an City. Available online: http://tjj.xa.gov.cn/tjsj/tjxx/619e21e3f8fd1c0bdc6da63f.html (accessed on 24 November 2021).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Research Content | Method | Evaluation Indicators |
|---|---|---|
| Demand Characteristics of Elderly Care Service Facilities | Questionnaire | |
| Utilization and Lack Weight of Elderly Care Service Facilities | Questionnaire Cluster Analysis | The Utilization Weight and Lack Weight of Facilities |
| Satisfaction with the Utilization of Elderly Care Service Facilities | Satisfaction Rating | |
| Demand Characteristics of Facilities among Different Types of Elderly | Proportion of Need and Usage. |
| Age Group | Elderly Day Care Center | Community Canteen | Elderly Service Center | Elderly Activity Center | Elderly University | Community Service Center | Health Service Center |
|---|---|---|---|---|---|---|---|
| 60 to 69 years old | 24.56% | 36.84% | 35.09% | 47.37% | 33.33% | 52.63% | 43.86% |
| 70 to 79 years old | 43.04% | 55.70% | 44.30% | 50.63% | 35.44% | 51.90% | 40.51% |
| 80 years old and above | 31.65% | 45.57% | 35.44% | 50.63% | 15.19% | 43.04% | 35.44% |
| Age Group | Not Using Facilities | Using One Type of Facility | Use Two or More Types of Facilities | Total |
|---|---|---|---|---|
| 60 to 69 years old | 45 (78.90%) | 8 (14.00%) | 4 (7.00%) | 57 (100.00%) |
| 70 to 79 years old | 47 (59.50%) | 22 (27.80%) | 10 (12.70%) | 79 (100.00%) |
| 80 years old and above | 54 (68.40%) | 18 (22.80%) | 7 (8.90%) | 79 (100.00%) |
| Entire Sample | 146 (67.90%) | 48 (22.30%) | 21 (9.80%) | 215 (100.00%) |
| Age Group | Convenience Store | Vegetable Market | Supermarket | Restaurant | Barber Shop | Pharmacy | Bank |
|---|---|---|---|---|---|---|---|
| 60 to 69 years old | 73.68% | 91.23% | 84.21% | 52.63% | 80.70% | 85.96% | 91.23% |
| 70 to 79 years old | 62.03% | 79.75% | 82.28% | 55.70% | 77.22% | 87.34% | 87.34% |
| 80 years old and above | 48.10% | 69.62% | 73.42% | 37.97% | 70.89% | 69.62% | 70.89% |
| Entire Sample | 60.00% | 79.07% | 79.53% | 48.37% | 75.81% | 80.47% | 82.33% |
| Activity Capacity | Elderly Day Care Center | Community Canteen | Elderly Service Center | Elderly Activity Center | Elderly University | Community Service Center | Health Service Center |
|---|---|---|---|---|---|---|---|
| Normal | 25.49% | 41.18% | 31.37% | 50.00% | 29.41% | 46.08% | 39.22% |
| Slightly Limited Mobility | 42.50% | 53.75% | 43.75% | 47.50% | 26.25% | 51.25% | 35.00% |
| Very Limited Mobility | 40.63% | 50.00% | 50.00% | 56.25% | 25.00% | 53.13% | 53.13% |
| Entire Sample | 33.95% | 46.98% | 38.60% | 49.77% | 27.44% | 48.84% | 39.53% |
| Activity Capacity | Not Using Facilities | Using One Type of Facility | Use Two or More Types of Facilities | Total |
|---|---|---|---|---|
| Normal | 74 (72.50%) | 19 (18.60%) | 9 (8.80%) | 102 (100.00%) |
| Slightly Limited Mobility | 52 (65.00%) | 19 (23.80%) | 9 (11.30%) | 80 (100.00%) |
| Very Limited Mobility | 19 (59.40%) | 10 (31.30%) | 3 (9.40%) | 32 (100.00%) |
| Entire Sample | 146 (67.90%) | 48 (22.30%) | 21 (9.80%) | 214 (100.00%) |
| Activity Capacity | Convenience Store | Vegetable Market | Supermarket | Restaurant | Barber Shop | Pharmacy | Bank |
|---|---|---|---|---|---|---|---|
| Normal | 59.80% | 87.25% | 82.35% | 51.96% | 77.45% | 85.29% | 90.20% |
| Slightly Limited Mobility | 70.00% | 78.75% | 85.00% | 47.50% | 76.25% | 85.00% | 85.00% |
| Very Limited Mobility | 37.50% | 56.25% | 59.38% | 40.63% | 68.75% | 56.25% | 53.13% |
| Entire Sample | 60.00% | 79.07% | 79.53% | 48.37% | 75.81% | 80.47% | 82.33% |
| Chronic Diseases | Elderly Day Care Center | Community Canteen | Elderly Service Center | Elderly Activity Center | Elderly University | Community Service Center | Health Service Center |
|---|---|---|---|---|---|---|---|
| Healthy | 8.33% | 45.83% | 25.00% | 70.83% | 25.00% | 41.67% | 45.83% |
| One Disease | 38.89% | 41.11% | 38.89% | 41.11% | 28.89% | 50.00% | 37.78% |
| Two Diseases | 37.50% | 50.00% | 40.63% | 53.13% | 23.44% | 51.56% | 34.38% |
| Three or More Diseases | 32.43% | 56.76% | 43.24% | 51.35% | 32.43% | 45.95% | 48.65% |
| Entire Sample | 33.95% | 46.98% | 38.60% | 49.77% | 27.44% | 48.84% | 39.53% |
| Chronic Diseases | Not Using Facilities | Using One Type of Facility | Use Two or More Types of Facilities | Total |
|---|---|---|---|---|
| Healthy | 17 (70.80%) | 7 (29.20%) | 0 (0.00%) | 24 (100.00%) |
| One Disease | 63 (70.00%) | 18 (20.00%) | 9 (10.00%) | 90 (100.00%) |
| Two Diseases | 40 (62.50%) | 16 (25.00%) | 8 (12.50%) | 64 (100.00%) |
| Three or More Diseases | 26 (70.30%) | 7 (18.90%) | 4 (10.80%) | 37 (100.00%) |
| Entire Sample | 146 (67.90%) | 48 (22.30%) | 21 (9.80%) | 215 (100.00%) |
| Chronic Diseases | Convenience Store | Vegetable Market | Supermarket | Barber Shop | Pharmacy | Bank |
|---|---|---|---|---|---|---|
| Healthy | 87.50% | 91.67% | 83.33% | 87.50% | 87.50% | 91.67% |
| One Disease | 63.33% | 83.33% | 80.00% | 72.22% | 84.44% | 85.56% |
| Two Diseases | 51.56% | 71.88% | 81.25% | 76.56% | 79.69% | 84.38% |
| Three or More Diseases | 48.65% | 72.97% | 72.97% | 75.68% | 67.57% | 64.86% |
| Entire Sample | 60.00% | 79.07% | 79.53% | 75.81% | 80.47% | 82.33% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, Y.; Li, C.; Zhou, D. Study on the Characteristics of Community Elderly Care Service Facilities Usage and Optimization Design Based on Life Cycle Theory. Buildings 2024, 14, 3003. https://doi.org/10.3390/buildings14093003
Yang Y, Li C, Zhou D. Study on the Characteristics of Community Elderly Care Service Facilities Usage and Optimization Design Based on Life Cycle Theory. Buildings. 2024; 14(9):3003. https://doi.org/10.3390/buildings14093003
Chicago/Turabian StyleYang, Yujun, Chenxi Li, and Dian Zhou. 2024. "Study on the Characteristics of Community Elderly Care Service Facilities Usage and Optimization Design Based on Life Cycle Theory" Buildings 14, no. 9: 3003. https://doi.org/10.3390/buildings14093003
APA StyleYang, Y., Li, C., & Zhou, D. (2024). Study on the Characteristics of Community Elderly Care Service Facilities Usage and Optimization Design Based on Life Cycle Theory. Buildings, 14(9), 3003. https://doi.org/10.3390/buildings14093003