
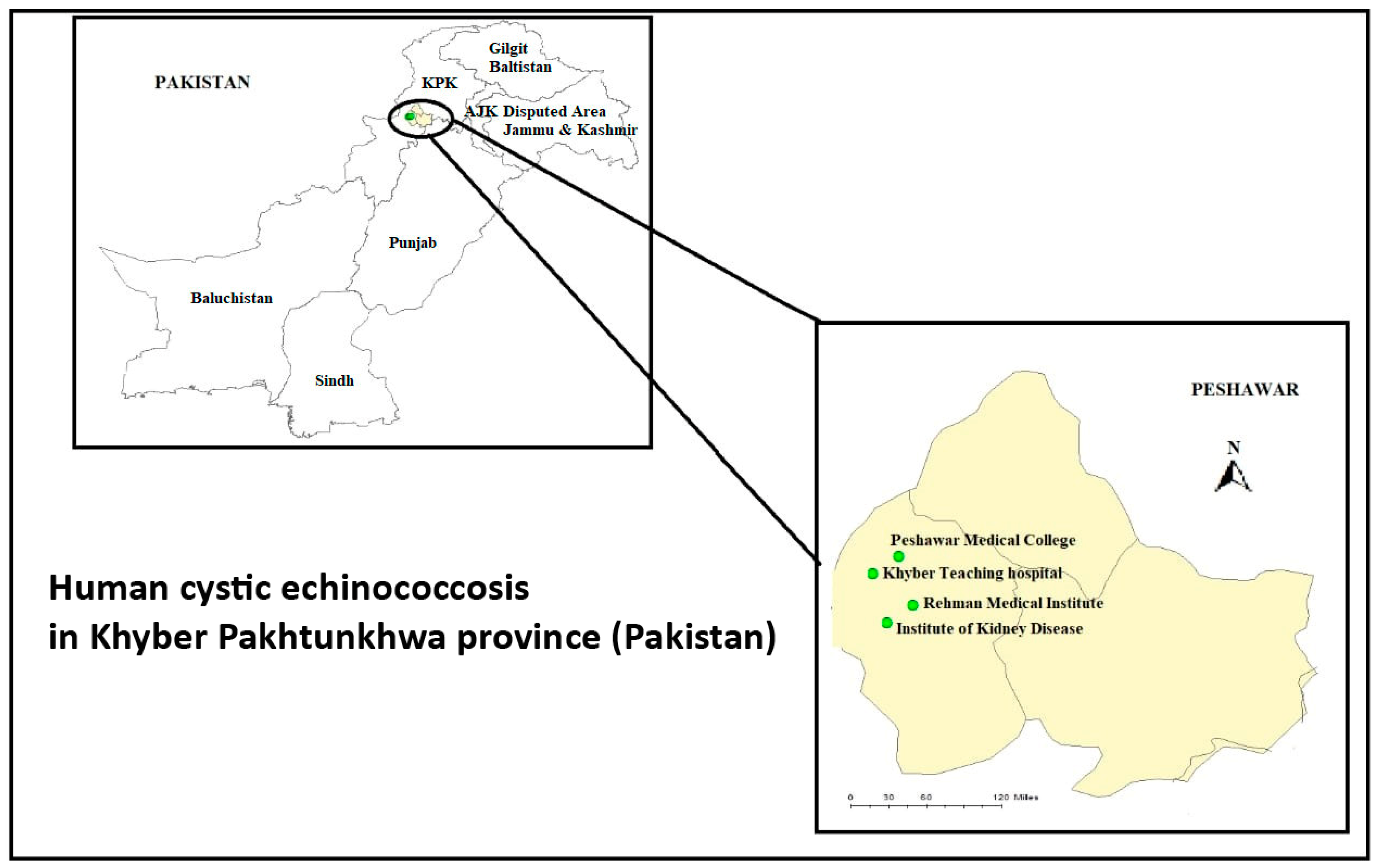
A Retrospective Cohort Study on Human Cystic Echinococcosis in Khyber Pakhtunkhwa Province (Pakistan) Based on 16 Years of Hospital Discharge Records


 ,
,
Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Casulli, A. New global targets for NTDs in the WHO roadmap 2021–2030. PLoS Negl. Trop. Dis. 2021, 5, 13–15. [Google Scholar] [CrossRef]
- Craig, P.S.; McManus, D.P.; Lightowlers, M.W.; Chabalgoity, J.A.; Garcia, H.H.; Gavidia, C.M. Prevention and control of cystic echinococcosis. Lancet Inf. Dis. 2007, 7, 385–394. [Google Scholar] [CrossRef]
- Budke, C.M.; Deplazes, P.; Torgerson, P.R. Global socioeconomic impact of cystic echinococcosis. Emerg. Infect. Dis. 2006, 12, 296–303. [Google Scholar] [CrossRef]
- Agudelo Higuita, N.I.; Brunetti, E.; Mccloskey, C. Cystic echinococcosis. J. Clin. Microbiol. 2006, 54, 518–523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basinger, S.C.; Khan, A.; Ahmed, H.; Afzal, M.S.; Simsek, S.; Budke, C.M. Estimation of the monetary burden of treated human cystic echinococcosis in Pakistan. Acta Trop. 2021, 222, 106026. [Google Scholar] [CrossRef] [PubMed]
- Craig, P.S.; Rogan, M.T.; Campos Ponce, M. Echinococcosis: Disease, detection and transmission. Parasitology 2003, 127, S5–S20. [Google Scholar] [CrossRef] [Green Version]
- Tamarozzi, F.; Deplazes, P.; Casulli, A. Reinventing the wheel of Echinococcus granulosus sensu lato transmission to humans. Trends Parasitol. 2020, 36, 427–434. [Google Scholar] [CrossRef] [PubMed]
- Khan, H.; Zahoor, S.; Afza, M.S.; Khan, A.; Kaleem, I.; Shah, N.A.; Harandi, M.F.; Ahmed, H. Occurrence of massively enlarged multiple hydatid cysts in the lung and liver of a pediatric patient in Pakistan. Iran J. Parasitol. 2021, 16, 339–342. [Google Scholar] [CrossRef]
- Alvarez Rojas, C.A.; Romig, T.; Lightowlers, M.W. Echinococcus granulosus sensu lato genotypes infecting humans—Review of current knowledge. Int. J. Parasitol. 2014, 44, 9–18. [Google Scholar] [CrossRef]
- Ahmed, H.; Ali, S.; Afzal, M.S.; Khan, A.A.; Raza, H.; Shah, Z.H.; Simsek, S. Why more research needs to be done on echinococcosis in Pakistan. Infect. Dis. Poverty 2017, 6, 90. [Google Scholar] [CrossRef]
- Khan, A.; Ahmed, H.; Khan, H.; Simsek, S.; Afzal, M.S.; Kilinic, S.G.; Kesik, H.K.; Yayi, G. A retrospective analysis on the cystic echinococcosis (CE) cases occurred in northeastern Punjab Province, Pakistan. Korean J. Parasitol. 2018, 56, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.; Ahmed, H.; Khan, H.; Saleem, S.; Simsek, S.; Brunetti, E.; Afzal, M.; Manciulli, T.; Budke, C.M. Cystic echinococcosis in Pakistan: A review of reported cases, diagnosis, and management. Acta Trop. 2020, 212, 105709. [Google Scholar] [CrossRef] [PubMed]
- Finance Division Government of Pakistan. Pakistan Economic Survey 2020–2021; Economic Adviser’s Wing, Finance Division Government of Pakistan: Islamabad, Pakistan, 2021. [Google Scholar]
- Khan, A.; Ahmed, H.; Simsek, S.; Gondal, M.A.; Afzal, M.S.; Irum, S.; Muhammad, I.; Mansur, H.; Fatima, A.; Ali, M.S.; et al. Poverty-associated emerging infection of cystic echinococcosis in population of Northern Pakistan: A hospital based study. Trop. Biomed. 2019, 36, 324–334. [Google Scholar]
- Nur, A.; Abera, B.; Gunse, T. The significance (socio-economic impact) and control of Echinococcosis/Hydatidosis: A review. Eur. J. Biol. Sci. 2017, 9, 58–66. [Google Scholar]
- Torgerson, P.R. The emergence of echinococcosis in central Asia. Parasitology 2013, 140, 1667–1673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, W.; Zhang, Z.; Wu, W.; Shi, B.; Li, J.; Zhou, X.; Wen, H.; McManus, D.P. Epidemiology and control of echinococcosis in central Asia, with particular reference to the People’s Republic of China. Acta Trop. 2015, 141, 235–243. [Google Scholar] [CrossRef] [PubMed]
- Borhani, M.; Fathi, S.; Darabi, E.; Jalousian, F.; Simsek, S.; Ahmed, H.; Kesik, H.K.; Hosseini, S.H.; Romig, T.; Harandi, M.F.; et al. Echinococcoses in Iran, Turkey, and Pakistan: Old diseases in the new millennium. Clin. Microbiol. Rev. 2021, 34, e0029020. [Google Scholar] [CrossRef]
- Harandi, F.M.; Budke, C.M.; Rostami, S. The monetary burden of cystic echinococcosis in Iran. PLoS Negl. Trop. Dis. 2012, 6, e1915. [Google Scholar]
- Altintas, N. Parasitic zoonotic disease in Turkey. Vet. Ital. 2008, 44, 633–646. [Google Scholar]
- Gonlugur, U.; Ozcelik, S.; Gonlugur, T.E.; Arici, S.; Elagoz, S.; Cevit, R. The retrospective annual surgical incidence of cystic echinococcosis in Sivas, Turkey. Zoonoses Public Health 2009, 56, 209–214. [Google Scholar] [CrossRef]
- Tamarozzi, F.; Akhan, O.; Cretu, C.M.; Vutova, K.; Akinci, D.; Chipeva, R.; Ciftci, T.; Constantin, C.M.; Fabiani, M.; Golemanov, B.; et al. Prevalence of abdominal cystic echinococcosis in rural Bulgaria, Romania, and Turkey: A cross-sectional, ultrasound-based, population study from the HERACLES project. Lancet Infect. Dis. 2018, 8, 769–778. [Google Scholar] [CrossRef]
- Wang, L.Y.; Qin, M.; Liu, Z.; Wu, W.P.; Xao, N.; Zhou, X.N.; Manguin, S.; Gavotte, L.; Frutos, R. Prevalence and spatial distribution characteristic of human echinococcosis in China. PLoS Negl. Trop. Dis. 2021, 15, e0009996. [Google Scholar] [CrossRef]
- Khan, A.; Ahmed, H.; Simsek, S.; Liu, H.; Yin, J.; Wang, Y.; Shen, Y.; Cao, J. Molecular characterization of human Echinococcus isolates and the first report of E. canadensis (G6/G7) and E. multilocularis from the Punjab Province of Pakistan using sequence analysis. BMC Infect. Dis. 2020, 20, 262. [Google Scholar] [CrossRef]
- Muqaddas, H.; Arshad, M.; Ahmed, H.; Mehmood, N.; Khan, A.; Simsek, S. Retrospective study of cystic echinococcosis (CE) based on hospital record from five major metropolitan cities of Pakistan. Acta Parasitol. 2019, 64, 866–872. [Google Scholar] [CrossRef]
- Khan, A.; Ahmed, H.; Khan, H.; Simsek, S.; Kilinc, S.G.; Kesik, H.K.; Yayi, G.; Celik, F.; Afzal, M.A. First report of Echinococcus canadensis (G6/G7) by sequence analysis from the Khyber Pakhtunkhwa province of Pakistan. Acta Trop. 2020, 209, 105559. [Google Scholar] [CrossRef]
- Ali, S.A.; Akhtar, T.; Zaki, M.A.; Safi, W.A. Echinococcosis is an emerging public health problem in Pakistan. Int. J. Med. 2013, 3, 39–48. [Google Scholar]
- Kebede, N.; Mitiku, A.; Tilahun, G. Retrospective survey of human hydatidosis in Bahir Dar, northwestern Ethiopia. East. Med. Health J. 2010, 16, 937–941. [Google Scholar] [CrossRef]
- Ghartimagar, D.; Ghosh, A.; Shrestha, M.K.; Talwar, O.P.; Sathian, B. A 14 years hospital based study on clinical and morphological spectrum of hydatid disease. J. Nepal Med. Assoc. 2013, 52, 349–353. [Google Scholar]
- Abdul Hameed, M.F.; Habib, I.; Al-Azizz, S.A.; Robertson, I. A retrospective study of human cystic echinococcosis in Basrah province, Iraq. Acta Trop. 2017, 178, 130–133. [Google Scholar] [CrossRef] [Green Version]
- Hajipirloo, H.M.; Bozorgomid, A.; Alinia, T.; Tappeh, K.H.; Mahmodlou, R. Human cystic echinococcosis in West Azerbaijan, Northwest Iran: A retrospective hospital-based survey from 2000 to 2009. Iran J. Parasitol. 2013, 8, 323–326. [Google Scholar] [PubMed]
- Zhang, T.; Zhao, W.; Yang, D.; Piao, D.; Huang, S.; Mi, Y. Human cystic echinococcosis in Heilongjiang Province, China: A retrospective study. BMC Gastroenterol. 2015, 15, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abebe, E.; Kassa, T.; Bekele, M.; Tsehay, A. Intra-abdominal hydatid cyst: Sociodemographic, clinical profiles, and outcomes of patients operated on at a tertiary hospital in Addis Ababa, Ethiopia. J. Parasitol. 2017, 2017, 4837234. [Google Scholar] [CrossRef] [Green Version]
- Sharma, M.; Sehgal, R.; Fomda, B.A.; Malhotra, A.; Malla, N. Molecular characterization of Echinococcus granulosus cysts in north Indian patients: Identification of G1, G3, G5 and G6 genotypes. PLoS Negl. Trop. Dis. 2013, 7, e2262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Possenti, A.; Manzano-Román, R.; Sánchez-Ovejero, C.; Boufana, B.; La Torre, G.; Siles-Lucas, M.; Casulli, A. Potential risk factors associated with human cystic echinococcosis: Systematic review and meta-analysis. PLoS Negl. Trop. Dis. 2016, 10, e0005114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tamarozzi, F.; Akhan, O.; Cretu, C.M.; Vutova, K.; Fabiani, M.; Orsten, S.; Pezzotti, P.; Popa, G.L.; Velev, V.; Siles-Lucas, M.; et al. Epidemiological factors associated with human cystic echinococcosis: A semi-structured questionnaire from a large population-based ultrasound cross-sectional study in eastern Europe and Turkey. Parasit. Vectors 2019, 12, 371. [Google Scholar] [CrossRef] [Green Version]
- Kern, S. The Infectious Disease Epidemiology Annual Report. 2017. Available online: https://www.gatestoneinstitute.org/10676/germany-migrants-Infectious (accessed on 12 July 2021).
- Rasib, Q.; Khan, A.; Ahmed, H.; Nizamuddin, S.; Asif, F.; Afzal, M.S.; Simsek, S.; Khurshid, F.; Irum, S.; Hussain, N.; et al. Demographics of cystic echinococcosis patients treated surgically in Lahore, Pakistan: A single centre study from 2007–2018. Helminthologia 2021, 58, 162–172. [Google Scholar] [CrossRef]
- Khan, A.; Zahoor, S.; Ahmed, H.; Malik, U.; Butt, R.A.; Muzam, M.S.; Kilinc, S.G.; Noor, N.; Zahoor, S.; Afzal, M.S.; et al. A retrospective analysis on the cystic echinococcosis cases occured in Northeastern Punjab Province, Pakistan. Korean J. Parasitol. 2018, 56, 385–390. [Google Scholar] [CrossRef]
- Ahmadi, N.A.; Badi, F. Human hydatidosis in Tehran, Iran: A retrospective epidemiological study of surgical cases between 1999 and 2009 at two university medical centers. Trop. Biomed. 2011, 28, 450–456. [Google Scholar]
- Brundu, D.; Piseddu, T.; Stegel, G.; Masu, G.; Ledda, S.; Masala, G. Retrospective study of human cystic echinococcosis in Italy based on the analysis of hospital discharge records between 2001 and 2012. Acta Trop. 2014, 140, 91–96. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Ethnicity | Number of Cases | Percentages |
|---|---|---|
| Afghani | 43 | 17.13% |
| Pakistani | 16 | 6.37% |
| Not available | 192 | 76.49% |
| Total | 251 | |
| Body organ | ||
| Liver | 103 | 41.0% |
| Liver and Omentum | 1 | 0.40% |
| Liver/spleen/pelvis | 2 | 0.80% |
| Lung | 12 | 4.78% |
| Lung and liver | 3 | 1.19% |
| Spleen | 9 | 3.58% |
| Abdomen | 7 | 2.78% |
| Gall bladder | 3 | 1.19% |
| Neck | 1 | 0.40% |
| Omentum | 3 | 1.19% |
| Ovary | 1 | 0.40% |
| Right flank | 3 | 1.19% |
| Right paraspinal cyst | 1 | 0.40% |
| Shoulder | 1 | 0.40% |
| Spleen and liver | 2 | 0.80% |
| Thyroid | 2 | 0.80% |
| Vertebrae | 2 | 0.80% |
| Others | 23 | 9.16% |
| Site not mentioned | 72 | 28.60% |
| Total | 251 |
| Number | Size (cm) | Number of Cysts | ||||
|---|---|---|---|---|---|---|
| Single | Multiple | Multiple/Single | Not Available | Total | ||
| 1 | ≤ 4 | 10 (9.7%) | 39 (37.9%) | - | 54 (52.4%) | 103 (41.0%) |
| 2 | 5–6 | 10 (24.3%) | 23 (56.0%) | 1 (2.4%) | 7 (17.0%) | 41(16.3%) |
| 3 | 7–8 | 8 (18.1%) | 28 (63.6%) | - | 8(18.1%) | 44 (17.5%) |
| 4 | 9–10 | 5 (18.5%) | 16 (59.2%) | - | 6 (20.7%) | 27 (10.7%) |
| 5 | 11–12 | 4 (25%) | 10 (62.5%) | - | 2(12.5%) | 16 (6.37%) |
| 6 | 13–14 | 1 (16.6%) | 4 (66.6%) | - | 1 (16.6%) | 6 (2.39%) |
| 7 | 15–16 | - | 4 (66.6%) | - | 2 (33.3%) | 6 (2.39%) |
| 8 | 17–18 | 1 (50%) | 1 (50%) | - | - | 2 (0.79%) |
| 9 | 19–20 | 1 (33.3%) | 2 (66.6%) | - | - | 3 (1.19%) |
| 10 | 21–22 | - | 1 (50.0%) | - | 1 (50.0%) | 2 (0.79%) |
| 11 | ≥23 | - | 1 (100.0%) | - | - | 1 (0.39%) |
| 251 | ||||||
| Year | Number of Reported Cases | Total Population * | Incidence Per 100,000 |
|---|---|---|---|
| 2006 | 1 | 18,575,729 a | 0.005 |
| 2007 | 4 | 18,575,729 a | 0.021 |
| 2008 | 13 | 18,575,729 a | 0.070 |
| 2009 | 21 | 18,575,729 a | 0.113 |
| 2010 | 15 | 18,575,729 a | 0.080 |
| 2011 | 23 | 26,000,000 a | 0.090 |
| 2012 | 42 | 26,000,000 a | 0.161 |
| 2013 | 11 | 26,000,000 a | 0.042 |
| 2014 | 14 | 26,000,000 a | 0.053 |
| 2015 | 14 | 26,000,000 a | 0.053 |
| 2016 | 11 | 26,000,000 a | 0.042 |
| 2017 | 18 | 35,525,047 b | 0.050 |
| 2018 | 21 | 35,525,047 b | 0.060 |
| 2019 | 30 | 35,525,047 b | 0.084 |
| 2020 | 12 | 35,525,047 b | 0.034 |
| 2021 | 1 | 35,525,047 b | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khan, H.; Casulli, A.; Harandi, M.F.; Afzal, M.S.; Saqib, M.A.N.; Ahmed, H. A Retrospective Cohort Study on Human Cystic Echinococcosis in Khyber Pakhtunkhwa Province (Pakistan) Based on 16 Years of Hospital Discharge Records. Pathogens 2022, 11, 194. https://doi.org/10.3390/pathogens11020194
Khan H, Casulli A, Harandi MF, Afzal MS, Saqib MAN, Ahmed H. A Retrospective Cohort Study on Human Cystic Echinococcosis in Khyber Pakhtunkhwa Province (Pakistan) Based on 16 Years of Hospital Discharge Records. Pathogens. 2022; 11(2):194. https://doi.org/10.3390/pathogens11020194
Chicago/Turabian StyleKhan, Huma, Adriano Casulli, Majid Fasihi Harandi, Muhammad Sohail Afzal, Muhammad Arif Nadeem Saqib, and Haroon Ahmed. 2022. "A Retrospective Cohort Study on Human Cystic Echinococcosis in Khyber Pakhtunkhwa Province (Pakistan) Based on 16 Years of Hospital Discharge Records" Pathogens 11, no. 2: 194. https://doi.org/10.3390/pathogens11020194
APA StyleKhan, H., Casulli, A., Harandi, M. F., Afzal, M. S., Saqib, M. A. N., & Ahmed, H. (2022). A Retrospective Cohort Study on Human Cystic Echinococcosis in Khyber Pakhtunkhwa Province (Pakistan) Based on 16 Years of Hospital Discharge Records. Pathogens, 11(2), 194. https://doi.org/10.3390/pathogens11020194