
A Rare Case of Strongyloides stercoralis Hyperinfection in a Diabetic Patient from Romania—Case Report and Review of the Literature

 ,
,
Abstract
:1. Introduction
2. Case Report
2.1. Presentation and Medical History
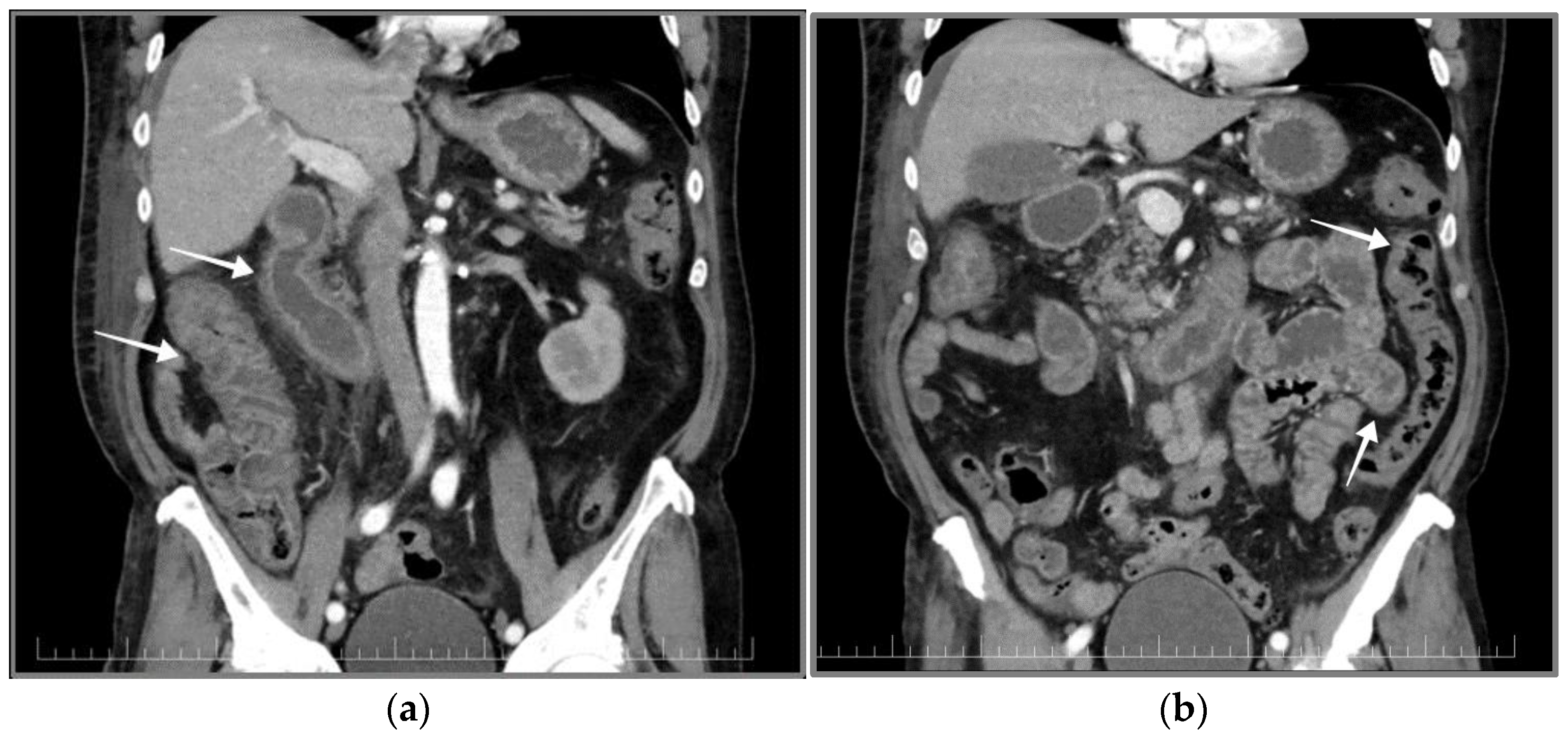
2.2. Physical Examination, Blood Tests, Ultrasound and CT Scan
2.3. Stool Examination
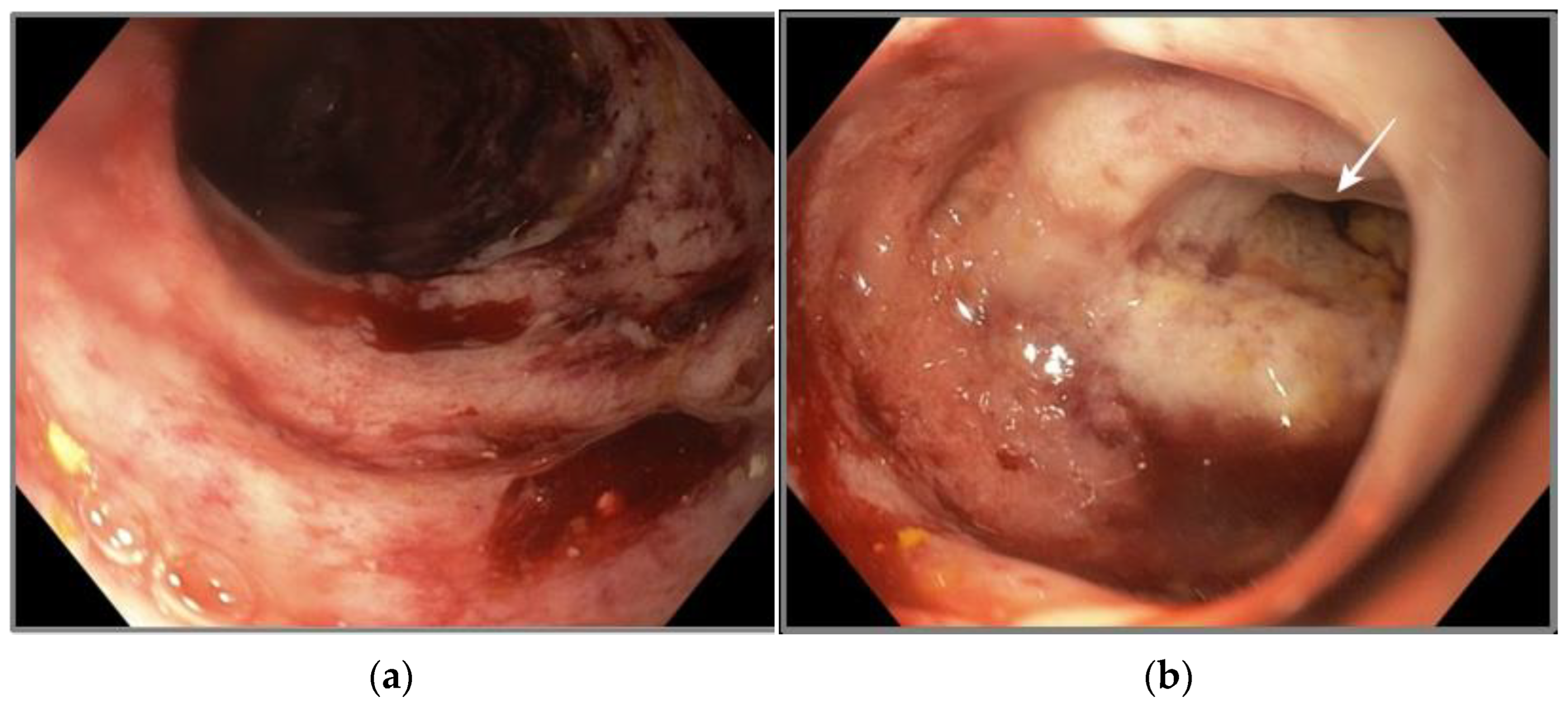
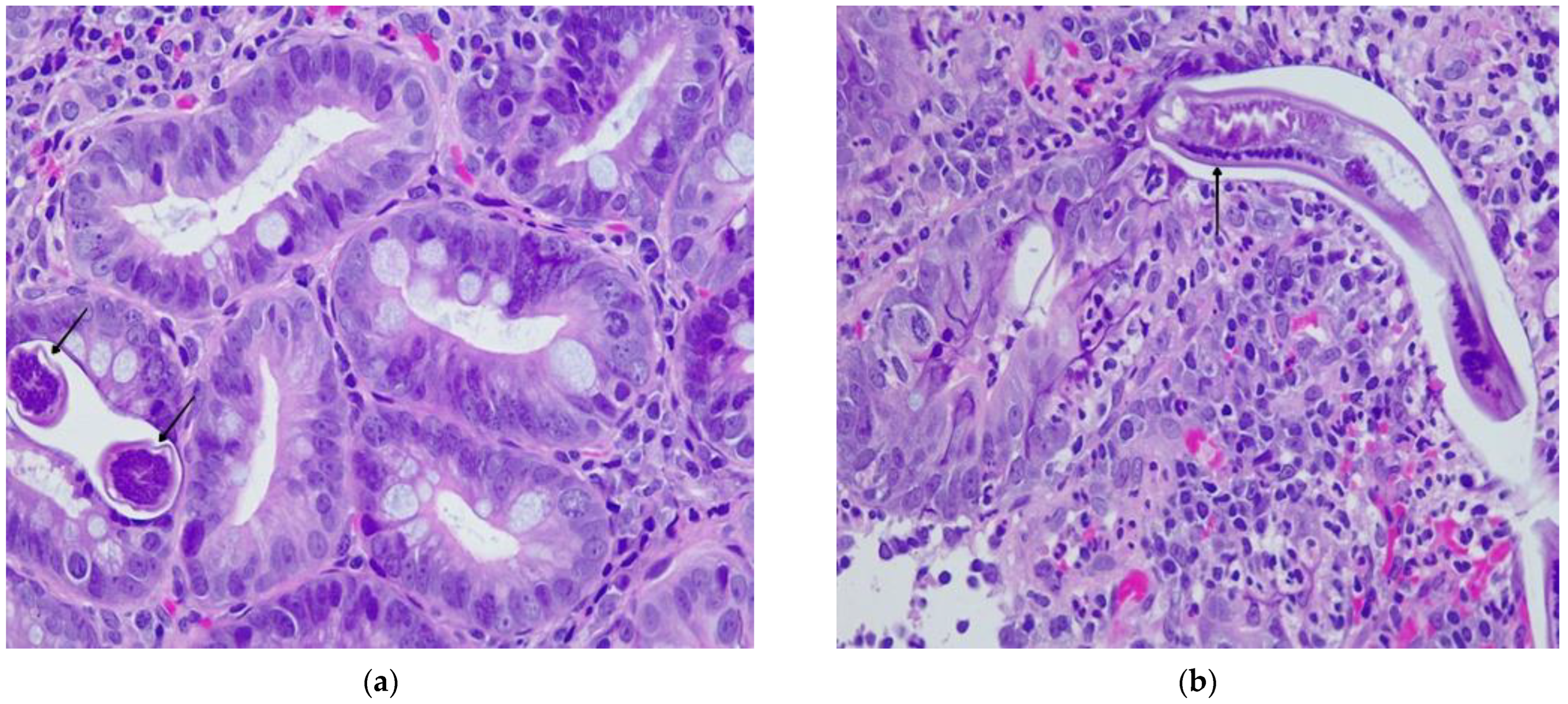
2.4. Gastric and Duodenal Histology
2.5. Diagnosis, Treatment and Additional Examinations
3. Discussion
4. Literature Review
4.1. Review Methodology
4.2. Results
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, C.; Xu, J.; Zhou, X.; Li, J.; Yan, G.; James, A.A.; Chen, X. Strongyloidiasis: An Emerging Infectious Disease in China. Am. J. Trop. Med. Hyg. 2013, 88, 420–425. [Google Scholar] [CrossRef] [PubMed]
- Normand, A. Sur La Maladie Dite Diar-Rh. e de Cochinchine. C.R. Acad. Sci. 1983, 83, 316. [Google Scholar]
- Viney, M. Strongyloides. Parasitology 2017, 144, 259–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Concha, R.; Harrington, W., Jr.; Rogers, A.I. Intestinal Strongyloidiasis: Recognition, Management, and Determinants of Outcome. J. Clin. Gastroenterol. 2005, 39, 203–211. [Google Scholar] [CrossRef]
- Page, W.; Judd, J.A.; Bradbury, R.S. The Unique Life Cycle of Strongyloides Stercoralis and Implications for Public Health Action. Trop. Med. Infect. Dis. 2018, 3, 53. [Google Scholar] [CrossRef] [Green Version]
- Marcos, L.A.; Terashima, A.; Dupont, H.L.; Gotuzzo, E. Strongyloides Hyperinfection Syndrome: An Emerging Global Infectious Disease. Trans. R. Soc. Trop. Med. Hyg. 2008, 102, 314–318. [Google Scholar] [CrossRef]
- Fardet, L.; Généreau, T.; Cabane, J.; Kettaneh, A. Severe Strongyloidiasis in Corticosteroid-Treated Patients. Clin. Microbiol. Infect. 2006, 12, 945–947. [Google Scholar] [CrossRef] [Green Version]
- Grove, D.I. Human Strongyloidiasis. Adv. Parasitol. 1996, 38, 251–309. [Google Scholar] [CrossRef]
- Khieu, V.; Srey, S.; Schär, F.; Muth, S.; Marti, H.; Odermatt, P. Strongyloides Stercoralis Is a Cause of Abdominal Pain, Diarrhea and Urticaria in Rural Cambodia. BMC Res. Notes 2013, 6, 200. [Google Scholar] [CrossRef] [Green Version]
- Nutman, T.B. Human Infection with Strongyloides Stercoralis and Other Related Strongyloides Species. Parasitology 2017, 144, 263–273. [Google Scholar] [CrossRef] [Green Version]
- Gonzales, D.J.; Chakraborty, R.K.; Climaco, A. Strongyloidiasis. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- CDC Parasites-Strongyloides. Available online: https://www.cdc.gov/parasites/strongyloides/health_professionals/ (accessed on 25 January 2023).
- Jourdan, P.M.; Lamberton, P.H.L.; Fenwick, A.; Addiss, D.G. Soil-Transmitted Helminth Infections. Lancet 2018, 391, 252–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buonfrate, D.; Bisanzio, D.; Giorli, G.; Odermatt, P.; Fürst, T.; Greenaway, C.; French, M.; Reithinger, R.; Gobbi, F.; Montresor, A.; et al. The Global Prevalence of Strongyloides Stercoralis Infection. Pathogens 2020, 9, 468. [Google Scholar] [CrossRef] [PubMed]
- ECDC Public Health Guidance on Screening and Vaccination for Infectious Diseases in Newly Arrived Migrants within the EU/EEA. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/Public%20health%20guidance%20on%20screening%20and%20vaccination%20of%20migrants%20in%20the%20EU%20EEA.pdf (accessed on 1 January 2023).
- Dancescu, P. Investigations on the Intensity of the Infection in a Strongyloidiasis Focus. The Coal Culture Method. Trans. R. Soc. Trop. Med. Hyg. 1968, 62, 490–495. [Google Scholar] [CrossRef]
- Neghina, R.; Neghina, A.M.; Marincu, I.; Iacobiciu, I. Intestinal Nematode Infections in Romania: An Epidemiological Study and Brief Review of Literature. Vector Borne Zoonotic Dis. 2011, 11, 1145–1149. [Google Scholar] [CrossRef]
- Tampa, M.; Benea, V.; Malin Benea, A.; Oancea, C.; Sârbu, I.; Georgescu, S.-R. Acquired Perforating Disorder in a Patient with Strongyloides Stercoralis. BMC Infect. Dis. 2013, 13, 1. [Google Scholar] [CrossRef] [Green Version]
- Drug, V.; Haliga, R.; Akbar, Q.; Mihai, C.; Prelipcean, C.; Stanciu, C. Ascites with Strongyloides Stercoralis in a Patient with Acute Alcoholic Pancreatitis and Liver Cirrhosis. J. Gastrointestin. Liver. Dis. 2009, 18, 367–369. [Google Scholar]
- Gluhovschi, G.; Gluhovschi, C.; Velciov, S.; Ratiu, I.; Bozdog, G.; Taban, S.; Petrica, L. “Surprise” in the Evolution of Chronic Membranoproliferative Glomerulonephritis Associated with Severe Strongyloidiasis under Corticotherapy: “Hygienic Paradox”? Ren. Fail. 2013, 35, 1017–1023. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ottino, L.; Buonfrate, D.; Paradies, P.; Bisoffi, Z.; Antonelli, A.; Rossolini, G.M.; Gabrielli, S.; Bartoloni, A.; Zammarchi, L. Autochthonous Human and Canine Strongyloides Stercoralis Infection in Europe: Report of a Human Case in An Italian Teen and Systematic Review of the Literature. Pathogens 2020, 9, 439. [Google Scholar] [CrossRef]
- Kalantari, N.; Chehrazi, M.; Ghaffari, S.; Gorgani-Firouzjaee, T. Serological Assays for the Diagnosis of Strongyloides Stercoralis Infection: A Systematic Review and Meta-Analysis of Diagnostic Test Accuracy. Trans. R. Soc. Trop. Med. Hyg. 2020, 114, 459–469. [Google Scholar] [CrossRef]
- Buonfrate, D.; Requena-Mendez, A.; Angheben, A.; Cinquini, M.; Cruciani, M.; Fittipaldo, A.; Giorli, G.; Gobbi, F.; Piubelli, C.; Bisoffi, Z. Accuracy of Molecular Biology Techniques for the Diagnosis of Strongyloides Stercoralis Infection-A Systematic Review and Meta-Analysis. PLoS Negl. Trop. Dis. 2018, 12, e0006229. [Google Scholar] [CrossRef] [Green Version]
- Boulware, D.R.; Stauffer, W.M.; Hendel-Paterson, B.R.; Rocha, J.L.L.; Seet, R.C.-S.; Summer, A.P.; Nield, L.S.; Supparatpinyo, K.; Chaiwarith, R.; Walker, P.F. Maltreatment of Strongyloides Infection: Case Series and Worldwide Physicians-in-Training Survey. Am. J. Med. 2007, 120, 545.e1–545.e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koga, K.; Kasuya, S.; Khamboonruang, C.; Sukavat, K.; Nakamura, Y.; Tani, S.; Ieda, M.; Tomita, K.; Tomita, S.; Hattan, N. An Evaluation of the Agar Plate Method for the Detection of Strongyloides Stercoralis in Northern Thailand. J. Trop. Med. Hyg. 1990, 93, 183–188. [Google Scholar] [PubMed]
- Sudarshi, S.; Stümpfle, R.; Armstrong, M.; Ellman, T.; Parton, S.; Krishnan, P.; Chiodini, P.L.; Whitty, C.J.M. Clinical Presentation and Diagnostic Sensitivity of Laboratory Tests for Strongyloides Stercoralis in Travellers Compared with Immigrants in a Non-Endemic Country. Trop. Med. Int. Health 2003, 8, 728–732. [Google Scholar] [CrossRef] [Green Version]
- Speare, R.; Durrheim, D.N. Strongyloides Serology--Useful for Diagnosis and Management of Strongyloidiasis in Rural Indigenous Populations, but Important Gaps in Knowledge Remain. Rural Remote Health 2004, 4, 264. [Google Scholar] [CrossRef] [PubMed]
- Uparanukraw, P.; Phongsri, S.; Morakote, N. Fluctuations of Larval Excretion in Strongyloides Stercoralis Infection. Am. J. Trop. Med. Hyg. 1999, 60, 967–973. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Requena-Méndez, A.; Chiodini, P.; Bisoffi, Z.; Buonfrate, D.; Gotuzzo, E.; Muñoz, J. The Laboratory Diagnosis and Follow up of Strongyloidiasis: A Systematic Review. PLoS Negl. Trop. Dis. 2013, 7, e2002. [Google Scholar] [CrossRef]
- Buonfrate, D.; Requena-Mendez, A.; Angheben, A.; Muñoz, J.; Gobbi, F.; Van Den Ende, J.; Bisoffi, Z. Severe Strongyloidiasis: A Systematic Review of Case Reports. BMC Infect. Dis. 2013, 13, 78. [Google Scholar] [CrossRef] [Green Version]
- Lam, C.S.; Tong, M.K.H.; Chan, K.M.; Siu, Y.P. Disseminated Strongyloidiasis: A Retrospective Study of Clinical Course and Outcome. Eur. J. Clin. Microbiol. Infect. Dis. 2006, 25, 14–18. [Google Scholar] [CrossRef]
- Geri, G.; Rabbat, A.; Mayaux, J.; Zafrani, L.; Chalumeau-Lemoine, L.; Guidet, B.; Azoulay, E.; Pène, F. Strongyloides Stercoralis Hyperinfection Syndrome: A Case Series and a Review of the Literature. Infection 2015, 43, 691–698. [Google Scholar] [CrossRef]
- Cruz, R.J., Jr.; Vincenzi, R.; Ketzer, B.M. Duodenal Obstruction–an Unusual Presentation of Strongyloides Stercoralis Enteritis: A Case Report. World J. Emerg. Surg. 2010, 5, 23. [Google Scholar] [CrossRef] [Green Version]
- Pecorella, I.; Okello, T.R.; Ciardi, G.; Ogwang, D.M. Is Gastric Involvement by Strongyloides Stercoralis in an Immunocompetent Patient a Common Finding? A Case Report and Review of the Literature. Acta Parasitol. 2022, 67, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (CDC) Transmission of Strongyloides Stercoralis through Transplantation of Solid Organs—Pennsylvania, 2012. MMWR Morb. Mortal. Wkly. Rep. 2013, 62, 264–266.
- Henriquez-Camacho, C.; Gotuzzo, E.; Echevarria, J.; Clinton White, A., Jr.; Terashima, A.; Samalvides, F.; Pérez-Molina, J.A.; Plana, M.N. Ivermectin versus Albendazole or Thiabendazole for Strongyloides Stercoralis Infection. Cochrane Database Syst. Rev. 2016, 2016, CD007745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Requena-Méndez, A.; Buonfrate, D.; Gomez-Junyent, J.; Zammarchi, L.; Bisoffi, Z.; Muñoz, J. Evidence-Based Guidelines for Screening and Management of Strongyloidiasis in Non-Endemic Countries. Am. J. Trop. Med. Hyg. 2017, 97, 645–652. [Google Scholar] [CrossRef] [PubMed]
- Vasquez-Rios, G.; Pineda-Reyes, R.; Pineda-Reyes, J.; Marin, R.; Ruiz, E.F.; Terashima, A. Strongyloides Stercoralis Hyperinfection Syndrome: A Deeper Understanding of a Neglected Disease. J. Parasit. Dis. 2019, 43, 167–175. [Google Scholar] [CrossRef]
- Mejia, R.; Nutman, T.B. Screening, Prevention, and Treatment for Hyperinfection Syndrome and Disseminated Infections Caused by Strongyloides Stercoralis. Curr. Opin. Infect. Dis. 2012, 25, 458–463. [Google Scholar] [CrossRef] [Green Version]
- Keiser, P.B.; Nutman, T.B. Strongyloides Stercoralis in the Immunocompromised Population. Clin. Microbiol. Rev. 2004, 17, 208–217. [Google Scholar] [CrossRef] [Green Version]
- Almugadam, B.S.; Ibrahim, M.K.; Liu, Y.; Chen, S.-M.; Wang, C.-H.; Shao, C.-Y.; Ren, B.-W.; Tang, L. Association of Urogenital and Intestinal Parasitic Infections with Type 2 Diabetes Individuals: A Comparative Study. BMC Infect. Dis. 2021, 21, 20. [Google Scholar] [CrossRef]
- Sisu, A.; Abugri, J.; Ephraim, R.K.D.; Dadzie, I.; Essien-Baidoo, S.; Kyei-Mensah, J.; Storph, R.P.; Toboh, E. Intestinal Parasite Infections in Diabetes Mellitus Patients; A Cross-Sectional Study of the Bolgatanga Municipality, Ghana. Sci. Afr. 2021, 11, e00680. [Google Scholar] [CrossRef]
- Neculicioiu, V.S.; Colosi, I.A.; Toc, D.A.; Lesan, A.; Costache, C. When a Ciliate Meets a Flagellate: A Rare Case of Colpoda Spp. and Colpodella Spp. Isolated from the Urine of a Human Patient. Case Report and Brief Review of Literature. Biology 2021, 10, 476. [Google Scholar] [CrossRef]
- McGuire, E.; Welch, C.; Melzer, M. Is Strongyloides Seropositivity Associated with Diabetes Mellitus? A Retrospective Case-Control Study in an East London NHS Trust. Trans. R. Soc. Trop. Med. Hyg. 2019, 113, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Mendonça, S.C.L.; Gonçalves-Pires, M.d.R.F.; Rodrigues, R.M.; Ferreira, A., Jr.; Costa-Cruz, J.M. Is There an Association between Positive Strongyloides Stercoralis Serology and Diabetes Mellitus? Acta Trop. 2006, 99, 102–105. [Google Scholar] [CrossRef] [PubMed]
- Munisankar, S.; Rajamanickam, A.; Balasubramanian, S.; Muthusamy, S.; Dolla, C.K.; Menon, P.A.; Chinnayan, P.; Whalen, C.; Gumne, P.; Kaur, I.; et al. Seroprevalence of Strongyloides Stercoralis Infection in a South Indian Adult Population. PLoS Negl. Trop. Dis. 2022, 16, e0010561. [Google Scholar] [CrossRef] [PubMed]
- Hays, R.; Esterman, A.; Giacomin, P.; Loukas, A.; McDermott, R. Does Strongyloides Stercoralis Infection Protect against Type 2 Diabetes in Humans? Evidence from Australian Aboriginal Adults. Diabetes Res. Clin. Pract. 2015, 107, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Hays, R.; Esterman, A.; McDermott, R. Type 2 Diabetes Mellitus Is Associated with Strongyloides Stercoralis Treatment Failure in Australian Aboriginals. PLoS Negl. Trop. Dis. 2015, 9, e0003976. [Google Scholar] [CrossRef] [PubMed]
- Kishimoto, K.; Hokama, A.; Hirata, T.; Ihama, Y.; Nakamoto, M.; Kinjo, N.; Kinjo, F.; Fujita, J. Endoscopic and Histopathological Study on the Duodenum of Strongyloides Stercoralis Hyperinfection. World J. Gastroenterol. 2008, 14, 1768–1773. [Google Scholar] [CrossRef]
- Chan, F.L.Y.; Kennedy, B.; Nelson, R. Fatal Strongyloides Hyperinfection Syndrome in an Immunocompetent Adult with Review of the Literature. Intern. Med. J. 2018, 48, 872–875. [Google Scholar] [CrossRef]
- Emad, A. Exudative Eosinophilic Pleural Effusion Due to Strongyloides Stercoralis in a Diabetic Man. South. Med. J. 1999, 92, 58–60. [Google Scholar] [CrossRef]
- Myint, A.; Chapman, C.; Almira-Suarez, I.; Mehta, N. Strongyloides Hyperinfection Syndrome in an Immunocompetent Host Resulting in Bandemia and Death. BMJ Case Rep. 2017, 2017, bcr2016217911. [Google Scholar] [CrossRef]
- Murali, A.; Rajendiran, G.; Ranganathan, K.; Shanthakumari, S. Disseminated Infection with Strongyloides Stercoralis in a Diabetic Patient. Indian J. Med. Microbiol. 2010, 28, 407–408. [Google Scholar] [CrossRef]
- St Cyr, S.; Nagpal, A.; Sohail, M.R. Shiga Toxin Producing E Coli Bloodstream Infection Secondary to Strongyloides Penetration through Intestinal Mucosa. BMJ Case Rep. 2013, 2013, bcr2013200728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sridhara, S.; Simon, N.; Raghuraman, U.; Crowson, N.; Aggarwal, V. Strongyloides Stercoralis Pancolitis in an Immunocompetent Patient. Gastrointest. Endosc. 2008, 68, 196–199. [Google Scholar] [CrossRef] [PubMed]
- Tiwari, S.; Rautaraya, B.; Tripathy, K.P. Hyperinfection of Strongyloides Stercoralis in an Immunocompetent Patient. Trop. Parasitol. 2012, 2, 135–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, R.; Finn, T.; Babushkin, F.; Shapiro, M.; Uda, M.; Grossman, T. Streptococcus Pyogenes Bacteremia and Toxic Shock Syndrome Related to Strongyloides Stercoralis Hyperinfection: A Case Report. J. Med. Case Rep. 2018, 12, 346. [Google Scholar] [CrossRef] [Green Version]
- Reyes, F.; Singh, N.; Anjuman-Khurram, N.; Lee, J.; Chow, L. Strongyloides Hyperinfection Syndrome Causing Fatal Meningitis and Septicemia by Citrobacter Koseri. IDCases 2017, 10, 102–104. [Google Scholar] [CrossRef] [PubMed]
- Poveda, J.; El-Sharkawy, F.; Arosemena, L.R.; Garcia-Buitrago, M.T.; Rojas, C.P. Strongyloides Colitis as a Harmful Mimicker of Inflammatory Bowel Disease. Case Rep. Pathol. 2017, 2017, 2560719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.-F.; Xu, L.; Luo, S.-Q.; Xie, H.; Chen, W.; Wu, Z.-D.; Sun, X. Diagnosis of Strongyloides Stercoralis by Morphological Characteristics Combine with Molecular Biological Methods. Parasitol. Res. 2017, 116, 1159–1163. [Google Scholar] [CrossRef]
- Miranda, C.J.; Al Sabbagh, R.; Sarquiz, A.M.; Piliguian, M.; Reber, D.; Makdissi, R. S3431 Intestinal Strongyloidiasis and Hyperinfection Syndrome in an Immunocompetent Patient. Off. J. Am. Coll. Gastroenterol. 2022, 117, e2165. [Google Scholar] [CrossRef]
- Román-Vélez, J.M.; Martínez-Camacho, R.N.; Alayón-Laguer, D.; Fernández-González, R.; Reyes-Sosa, R.; Santos-Llanos, G.; Colón-Pérez, M.; Ferrer, D. An Unusual Presentation of Alveolar Hemorrhage. Prim. Care Respir. J. 2009, 18, 337–339. [Google Scholar] [CrossRef]
- Pedersen, A.A.; Hartmeyer, G.N.; Stensvold, C.R.; Martin-Iguacel, R. Strongyloides Stercoralis Hyperinfection Syndrome with Cerebral Involvement. BMJ Case Rep. 2022, 15, e247032. [Google Scholar] [CrossRef]
- Choudhry, U.; Choudhry, R.; Romeo, D.P.; Cammerer, R.C.; Gopalswamy, N. Strongyloidiasis: New Endoscopic Findings. Gastrointest. Endosc. 1995, 42, 170–173. [Google Scholar] [CrossRef]
- Rets, A.; Gupta, R.; Haseeb, M.A. Determinants of Reactivation of Inapparent Strongyloides Stercoralis Infection in Patients Hospitalized for Unrelated Admitting Diagnosis. Eur. J. Gastroenterol. Hepatol. 2013, 25, 1279–1285. [Google Scholar] [CrossRef]
- Ersöz, Ş.; Turgutalp, H.; Akdoğan, R.; Çobanoğlu, Ü.; Saygın, İ.; Mungan, S.; Özgür, O. Gastric Strongyloidiasis in a Diabetic Patient. Turk. J. Pathol. 2010, 26, 71–73. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Patient Data | Country of Origin/Recent Trips or Immigration | Eosinophilia | Comorbidities | Severe Strongyloidiasis | Diagnosis | Treatment | Complications | Outcome |
|---|---|---|---|---|---|---|---|---|---|
| Kishimoto et al., 2008 [49] | 82, M | Japan | N/A | - | H/D | Microscopy (stool, sputum) | ivermectin | Small bowel obstruction, meningitis, pneumonia | Died |
| Chan et al., 2018 [50] | 72, M | Australia/Southeast Asia | No | Peripheral vascular disease, dyslipidemia, hypertension, gastro-esophageal reflux, asthma, recent laparotomy for inguinal hernia | H | Microscopy (mesenteric biopsy, tracheal aspirate) | ivermectin, 200 mcg/kg daily | Multi-organ failure | Died |
| Current case | 71, M | Romania | No | Hypertension, benign prostatic hyperplasia, colonic diverticular uncomplicated disease | H | Microscopy (stool, duodenal biopsy) | albendazole, 400 mg twice daily for 10 days ivermectin, 200 mcg/kg for 3 days | Partial duodenal obstruction | Survived |
| Emad et al., 1999 [51] | 61, M | Iran | Yes | - | H/D | Microscopy (bronchial washing) | thiabendazole, 1.5 g twice/day for 21 days | Eosinophilic pleural effusion | Survived |
| Myint et al., 2017 [52] | 60, M | USA/El Salvador | No Peripheral bandemia | Hypertension, obesity, alcohol consumption (stopped 8 months prior) | H | Microscopy (stool) | ivermectin | Duodenitis, small bowel obstruction, pulmonary hemorrhage and oedema, cardiac arrest | Died |
| Murali et al., 2010 [53] | 58, M | India | No | Total laryngectomy due to carcinoma (4 years prior) | D | Microscopy (pericardial fluid) | ivermectin, 12 mg for 2 days | Pericardial effusion | Survived |
| Lam et al., 2006 [31] | 57, M | Hong Kong | No | - | D | Microscopy (gastric biopsy) | mebendazole, 100 mg two times a day thiabendazole | Multiple organ involvement, diabetic ketoacidosis | Died |
| St. Cyr et al., 2013 [54] | 51, F | USA/Laos | No | Hypertension, hyperlipidemia, gastroesophageal reflux disease | H | Microscopy (stool) | ivermectin, 200 mcg/kg for 2 days | Bloodstream infection due to Shiga toxin producing E. coli | Survived |
| Sridhara et al., 2008 [55] | 45, M | USA/Ghana | Yes | Colon polyps, lactose intolerance, internal hemorrhoids | H | Microscopy (colon biopsy) | ivermectin, 15 mg/day for 5 days | Pancolitis | Survived |
| Tiwari et al., 2012 [56] | 31, M | India | No | - * | H | Microscopy (stool) | albendazole, 10 mg/kg/day for 7 days | - | Survived |
| Immune Status | Immunocompetent | Diabetes | Immunosuppressed | |
|---|---|---|---|---|
| Reference | Chan et al. [50] | Current review | Geri et al. [32] | Buonfrate et al. [30] |
| Sample size | n = 9 | n = 10 | n = 133 | n = 244 |
| Male gender | 88.9% | 90% | 72.2% | N/A |
| Mortality | 22.2% | 40% | 60.3% | 62.7% |
| Eosinophilia | 66.7% | 20% | 34.3% | 22.5% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costache, C.; Colosi, I.A.; Neculicioiu, V.S.; Florian, D.I.; Petrushev, B.; Vasvari, A.; Seicean, A. A Rare Case of Strongyloides stercoralis Hyperinfection in a Diabetic Patient from Romania—Case Report and Review of the Literature. Pathogens 2023, 12, 530. https://doi.org/10.3390/pathogens12040530
Costache C, Colosi IA, Neculicioiu VS, Florian DI, Petrushev B, Vasvari A, Seicean A. A Rare Case of Strongyloides stercoralis Hyperinfection in a Diabetic Patient from Romania—Case Report and Review of the Literature. Pathogens. 2023; 12(4):530. https://doi.org/10.3390/pathogens12040530
Chicago/Turabian StyleCostache, Carmen, Ioana Alina Colosi, Vlad Sever Neculicioiu, Diana Ioana Florian, Bobe Petrushev, Alexandra Vasvari, and Andrada Seicean. 2023. "A Rare Case of Strongyloides stercoralis Hyperinfection in a Diabetic Patient from Romania—Case Report and Review of the Literature" Pathogens 12, no. 4: 530. https://doi.org/10.3390/pathogens12040530
APA StyleCostache, C., Colosi, I. A., Neculicioiu, V. S., Florian, D. I., Petrushev, B., Vasvari, A., & Seicean, A. (2023). A Rare Case of Strongyloides stercoralis Hyperinfection in a Diabetic Patient from Romania—Case Report and Review of the Literature. Pathogens, 12(4), 530. https://doi.org/10.3390/pathogens12040530