


Mycobacteriosis in a Pet Ferret (Mustela putorius furo) Caused by Mycobacterium xenopi: A Case Report on Neglected Risk of Zoonotic Transmission
 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. In Vivo Clinical Examination
2.2. Post-Mortem Examination
3. Case Description
3.1. Patient
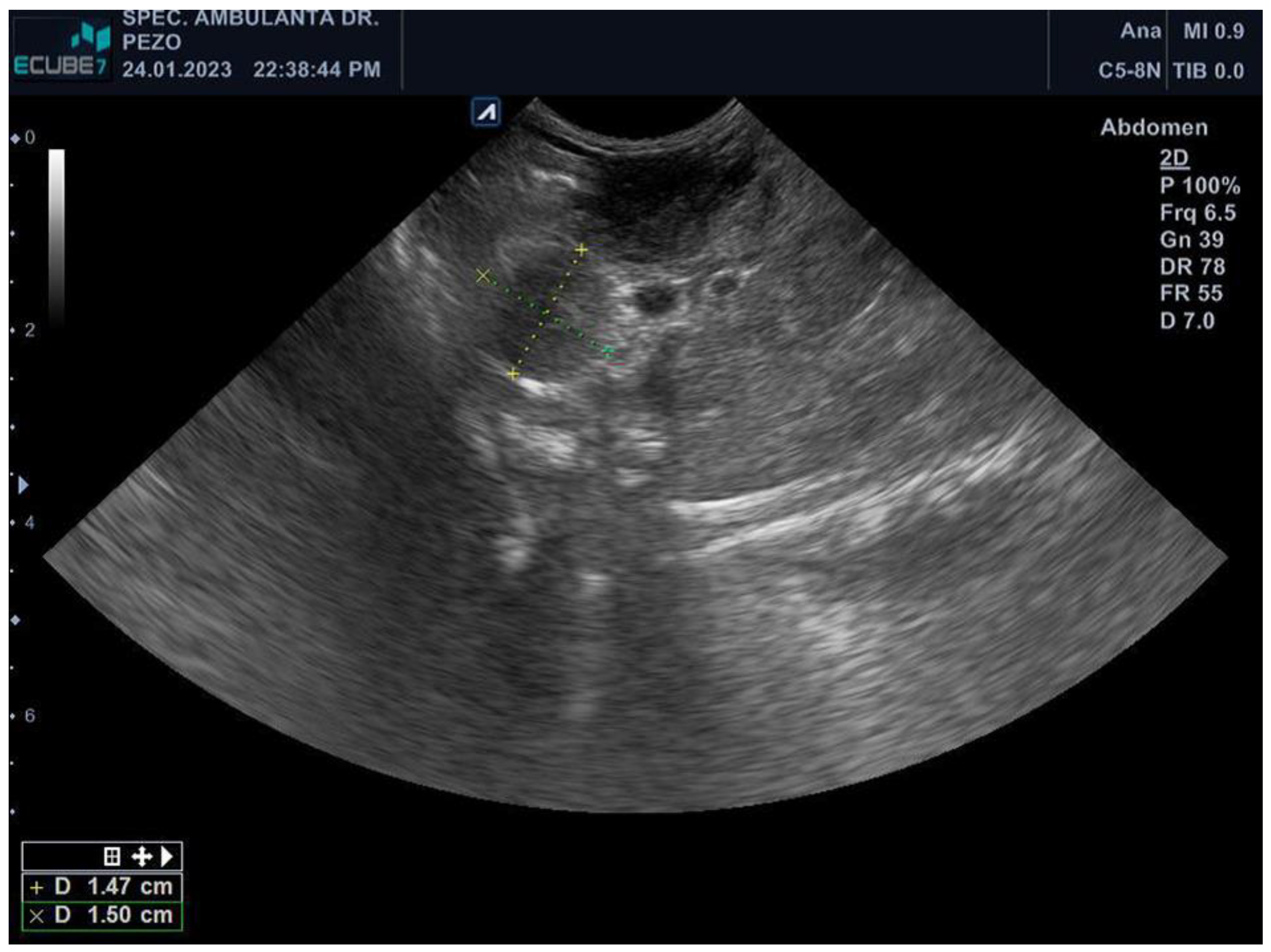
3.2. Diagnostics
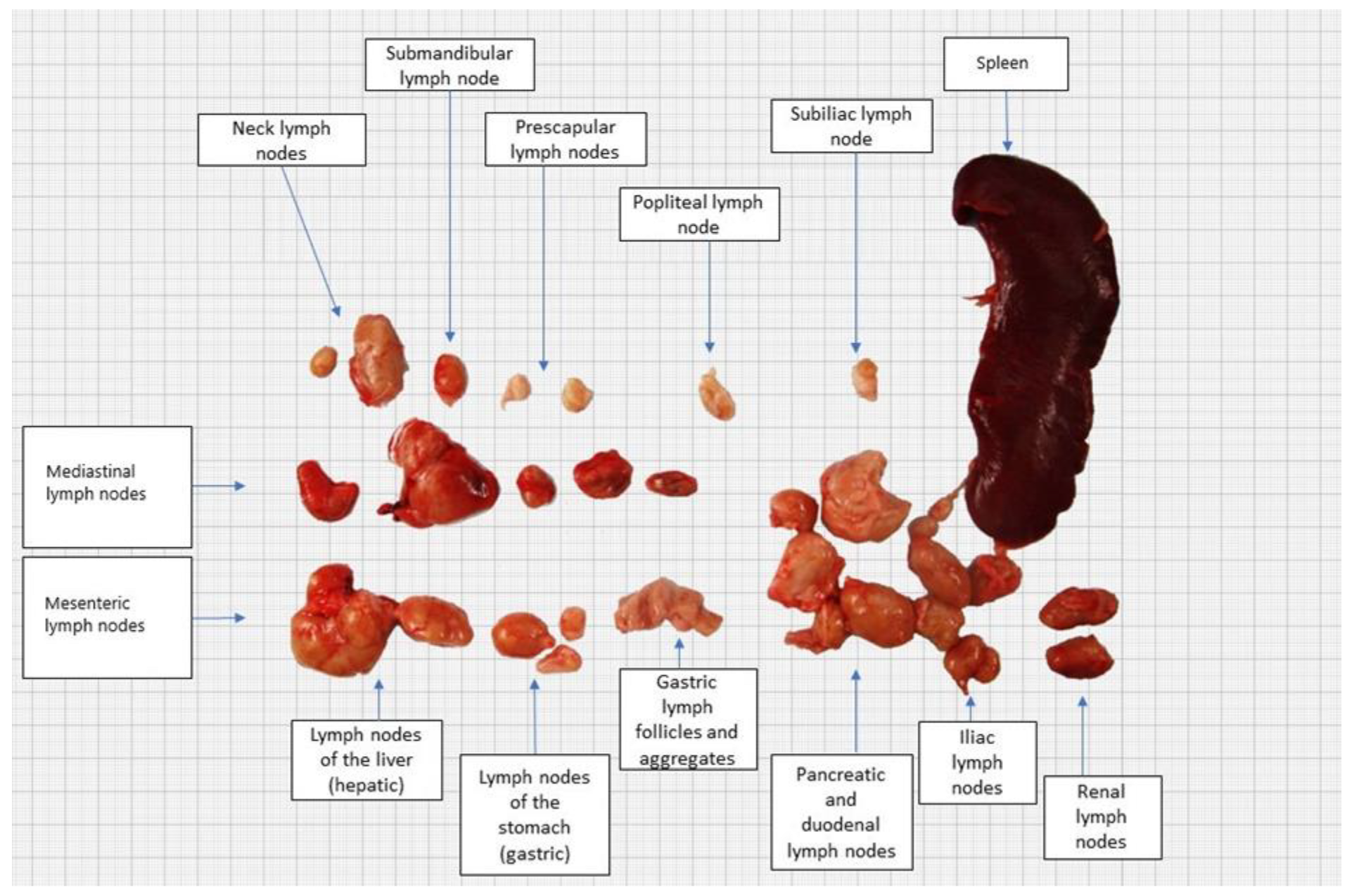
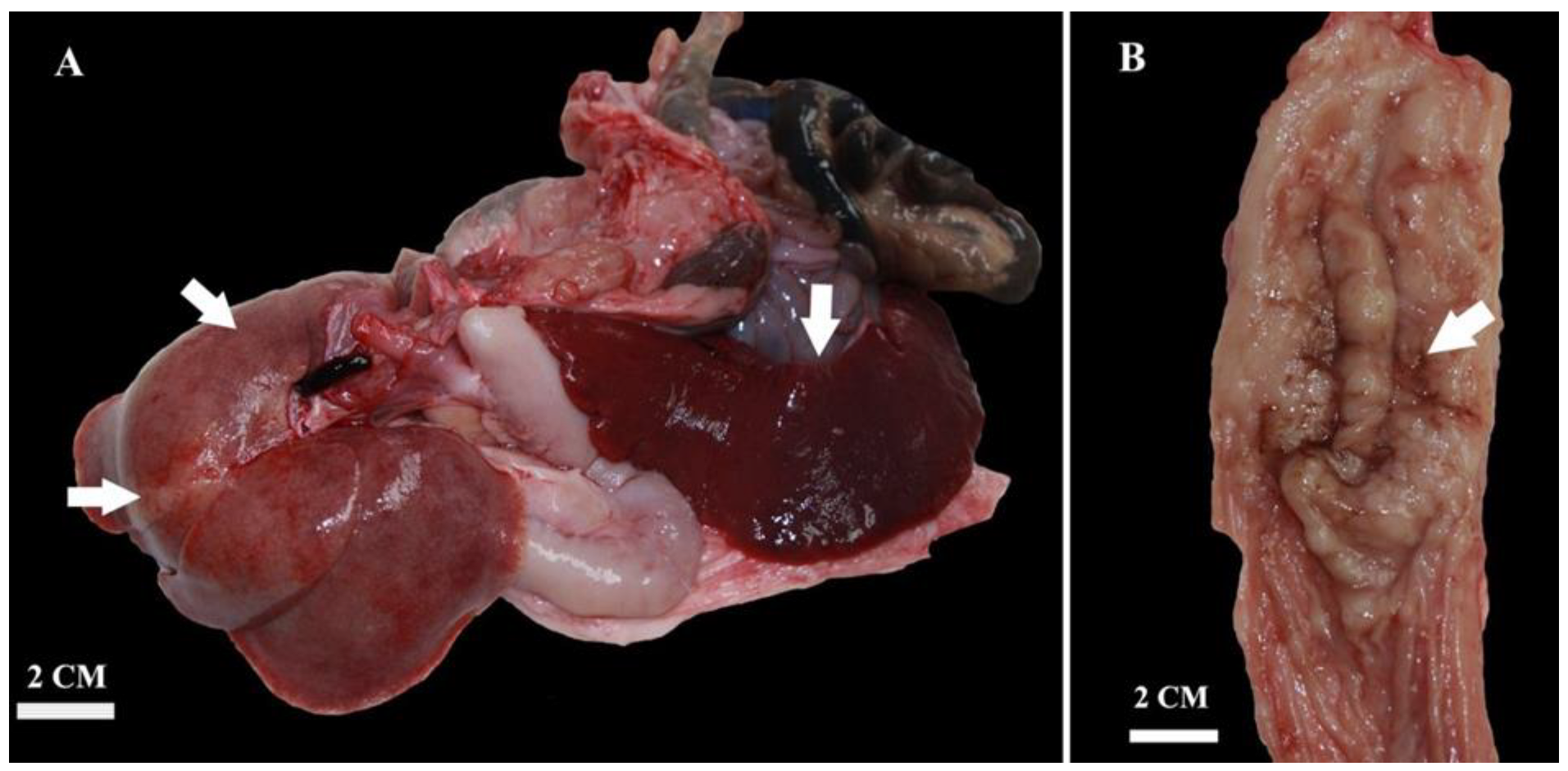
3.3. Necropsy Findings
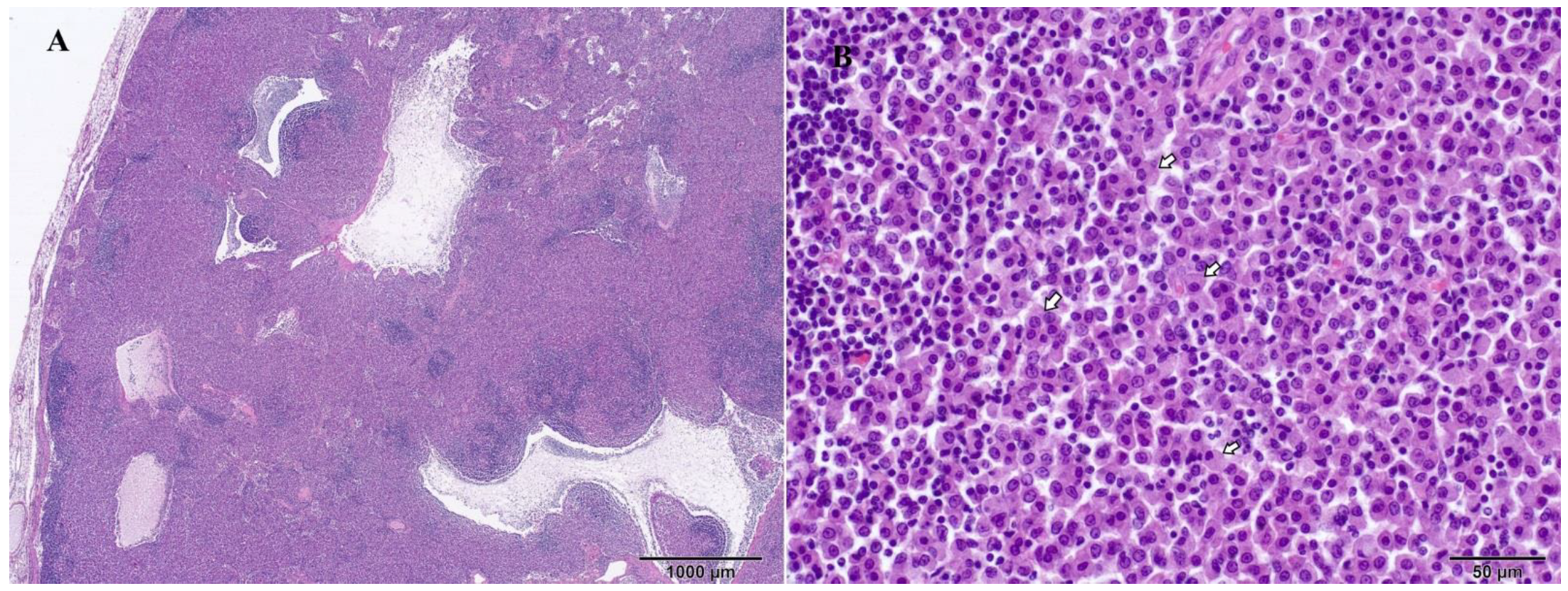
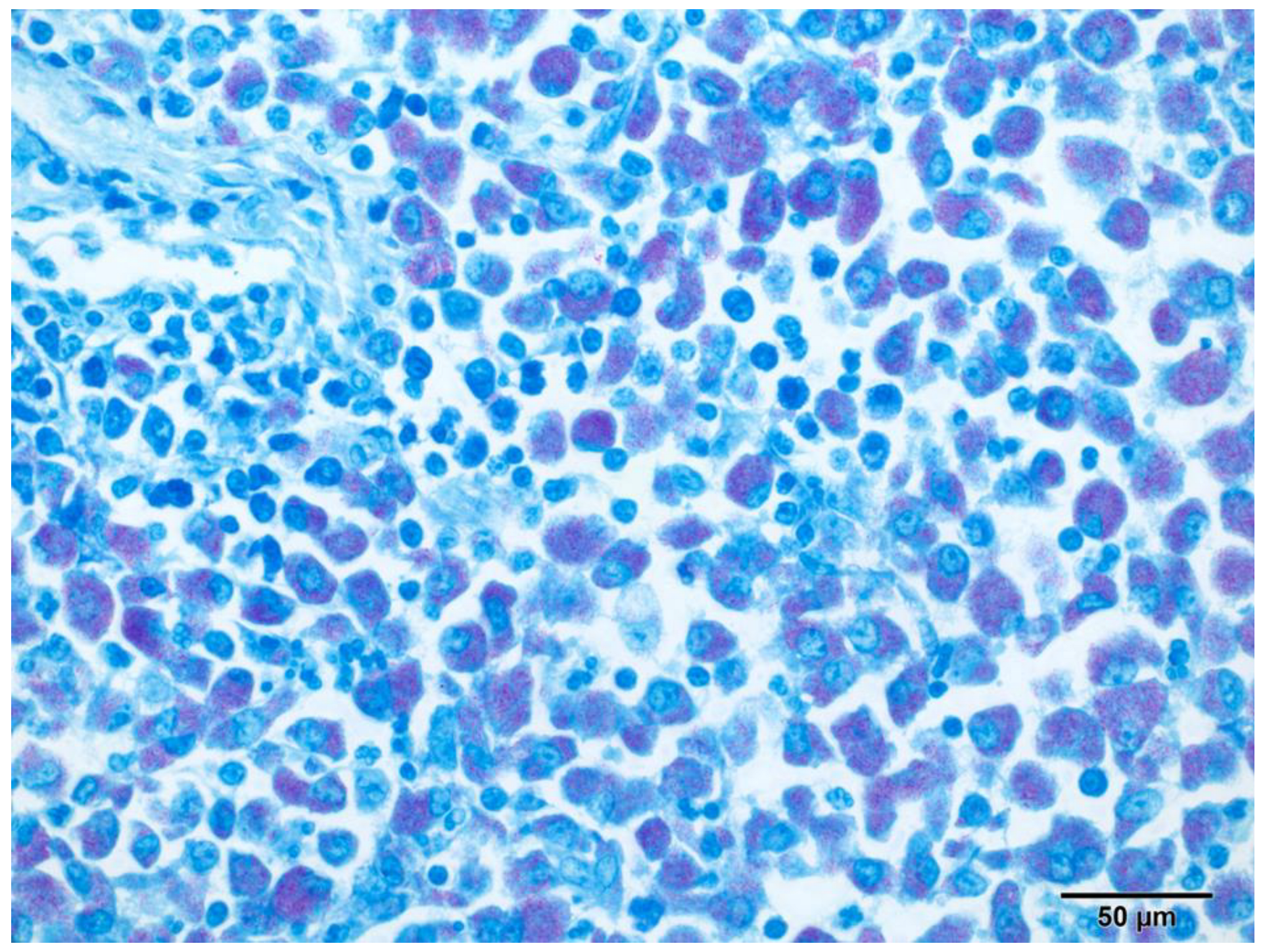
3.4. Histopathological Findings
3.5. Bacterial Examination and Molecular Identification
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Iland, C.N.; Symmers, W.S.; Thomson, A.P. A note on tuberculosis in the ferret (Mustela furo L.). J. Pathol. Bacteriol. 1951, 63, 554–556. [Google Scholar] [PubMed]
- Pollock, C. Mycobacterial infection in the ferret. Vet. Clin. N. Am. Exot. Anim. Pract. 2012, 15, 121–129. [Google Scholar] [CrossRef] [PubMed]
- Davendralingam, N.; Davagnanam, I.; Stidworthy, M.F.; Baldrey, V.; Peters, L.M.; Stapleton, N. Transmission of Mycobacterium xenopi to a pet albino ferret (Mustela putorius furo) from a domestic aquarium. Vet. Rec. 2017, 181, 169. [Google Scholar] [CrossRef]
- Dequeant, B.; Pascal, Q.; Bilbault, H.; Dagher, E.; Boschiroli, M.L.; Cordonnier, N.; Reyes-Gomez, E. Identification of Mycobacterium genavense natural infection in a domestic ferret. J. Vet. Diagn. Investig. 2019, 31, 133–136. [Google Scholar] [CrossRef] [PubMed]
- Valheim, M.; Djonne, B.; Heiene, R.; Caugant, D.A. Disseminated Mycobacterium celatum (Type 3) infection in a domestic ferret (Mustela putorius furo). Vet. Pathol. 2001, 38, 460–463. [Google Scholar] [CrossRef] [PubMed]
- Barth, S.A.; Menge, C.; Hillemann, D.; Lauda, A.; Pfleghaar, S. Tuberculosis in a pet ferret (Mustela putorius furo). Tierärztliche Prax. Ausg. K Kleintiere Heimtiere 2020, 48, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Lugton, I.W.; Wobeser, G.; Morris, R.S.; Caley, P. Epidemiology of Mycobacterium bovis infection in feral ferrets (Mustela furo) in New Zealand: II. Routes of infection and excretion. N. Z. Vet. J. 1997, 45, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Ragg, J.R.; Waldrup, K.A.; Moller, H. The distribution of gross lesions of tuberculosis caused by Mycobacterium bovis in feral ferrets (Mustela furo) from Otago, New Zealand. N. Z. Vet. J. 1995, 43, 338–341. [Google Scholar] [CrossRef] [PubMed]
- Lugton, I.W.; Wobeser, G.; Morris, R.S.; Caley, P. Epidemiology of Mycobacterium bovis infection in feral ferrets (Mustela furo) in New Zealand: I. Pathology and diagnosis. N. Z. Vet. J. 1997, 45, 140–150. [Google Scholar] [CrossRef]
- Mentre, V.; Bulliot, C. A Retrospective Study of 17 Cases of Mycobacteriosis in Domestic Ferrets (Mustela Putorius furo) between 2005 and 2013. J. Exot. Pet. Med. 2015, 24, 340–349. [Google Scholar] [CrossRef]
- Schultheiss, P.C.; Dolginow, S.Z. Granulomatous enteritis caused by Mycobacterium avium in a ferret. J. Am. Vet. Med. Assoc. 1994, 204, 1217–1218. [Google Scholar] [CrossRef]
- Hance, A.J.; Grandchamp, B.; Lévi-Frébault, V.; Lecossier, D.; Rauzier, J.; Bocart, D.; Gicquel, B. Detection and identification of mycobacteria by amplification of mycobacterial DNA. Mol. Microbiol. 1989, 3, 843–849. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.H.; Sheu, M.M.; Lin, S.R. Rapid identification of mycobacteria to the species level by polymerase chain reaction and restriction enzyme analysis—A case report of corneal ulcer. Kaohsiung J. Med. Sci. 1997, 13, 583–588. [Google Scholar]
- Kent, P.T.; Kubica, G.P. Public Health Mycobacteriology: A Guide for the Level III; U.S. Department of Health and Human Services, Centers for Disease Control: Atlanta, GA, USA, 1985.
- Ringuet, H.; Akoua-Koffi, C.; Honore, S.; Varnerot, A.; Vincent, V.; Berche, P.; Gaillard, J.L.; Pierre-Audigier, C. hsp65 sequencing for identification of rapidly growing mycobacteria. J. Clin. Microbiol. 1999, 37, 852–857. [Google Scholar] [CrossRef]
- Clinical and Laboratory Standards Institute. Susceptibility Testing of Mycobacteria, Nocardia spp., and Other Aerobic Actinomycetes (M24), 3rd ed.; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2018; pp. 37–44. [Google Scholar]
- Clinical and Laboratory Standards Institute. Performance Standards for Susceptibility Testing of Mycobacteria, Nocardia spp., and Other Aerobic Actinomycetes (M62), 1st ed.; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2018; pp. 4–11. [Google Scholar]
- Hein, J.; Spreyer, F.; Sauter-Louis, C.; Hartmann, K. Reference ranges for laboratory parameters in ferrets. Vet. Rec. 2012, 171, 218. [Google Scholar] [CrossRef] [PubMed]
- Reference Ranges for Serum Biochemical Values in Ferrets. Merck & Co., Inc., Rahway, NJ, USA. Available online: https://www.msdvetmanual.com/multimedia/table/reference-ranges-for-serum-biochemical-values-in-ferrets (accessed on 6 September 2023).
- Lucas, J.; Lucas, A.; Furber, H.; James, G.; Hughes, M.S.; Martin, P.; Chen, S.C.; Mitchell, D.H.; Love, D.N.; Malik, R. Mycobacterium genavense infection in two aged ferrets with conjunctival lesions. Aust. Vet. J. 2000, 78, 685–689. [Google Scholar] [CrossRef]
- Gupta, A.; McBride, A.M.; Holder, K.A.; Heggem, B.; Royal, A.B.; Wakamatsu, N. Pathology in Practice. J. Am. Vet. Med. Assoc. 2012, 240, 1427–1429. [Google Scholar] [CrossRef]
- Zaheen, A.; Hirama, T.; Mehrabi, M.; Brode, S.K.; Marras, T.K. Clinical outcomes in Mycobacterium xenopi versus Mycobacterium avium complex pulmonary disease: A retrospective matched cohort study. Respir. Med. 2020, 167, 105967. [Google Scholar] [CrossRef]
- Jiva, T.M.; Jacoby, H.M.; Weymouth, L.A.; Kaminski, D.A.; Portmore, A.C. Mycobacterium xenopi: Innocent bystander or emerging pathogen? Clin. Infect. Dis. 1997, 24, 226–232. [Google Scholar] [CrossRef]
- Brown-Elliott, B.A.; Nash, K.A.; Wallace, R.J., Jr. Antimicrobial susceptibility testing, drug resistance mechanisms, and therapy of infections with nontuberculous mycobacteria. Clin. Microbiol. Rev. 2012, 25, 545–582. [Google Scholar] [CrossRef]
- Andréjak, C.; Lescure, F.X.; Pukenyte, E.; Douadi, Y.; Yazdanpanah, Y.; Laurans, G.; Schmit, J.L.; Jounieaux, V.; Xenopi Group. Mycobacterium xenopi pulmonary infections: A multicentric retrospective study of 136 cases in north-east France. Thorax 2009, 64, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Salmon, J.H.; Direz, G.; Ziza, J.M.; Desplaces, N.; Brochot, P.; Eschard, J.P. Discitis and sacroiliitis diagnosed 15years after iatrogenic Mycobacterium xenopi inoculation. Jt. Bone Spine 2012, 79, 409–411. [Google Scholar] [CrossRef] [PubMed]
- Adjemian, J.; Olivier, K.N.; Seitz, A.E.; Holland, S.M.; Prevots, D.R. Prevalence of nontuberculous mycobacterial lung disease in U.S. Medicare beneficiaries. Am. J. Respir. Crit. Care Med. 2012, 185, 881–886. [Google Scholar] [CrossRef] [PubMed]
- Weathered, C.; Wei, N.; Pienaar, E. Reduced macrophage killing of M. avium drives infection risk in post-menopausal patients. Tuberculosis 2023, 139, 102304. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Antimicrobial | MIC (µg/mL) Criteria | MIC Results | Interpretation | ||
|---|---|---|---|---|---|
| S | I | R | |||
| Amikacin | ≤16 | 32 | ≥64 | 4 | S |
| Ciprofloxacin | ≤1 | 2 | ≥4 | 1 | S |
| Clarithromycin | ≤8 | 16 | ≥32 | ≤0.6 | S |
| Doxycycline | ≤1 | 2–4 | ≥8 | 8 | R |
| Ethambutol | No interpretations available | 8 | / | ||
| Ethionamide | No interpretations available | 5 | / | ||
| Isoniazid | No interpretations available | 2 | S | ||
| Linezolid | ≤8 | 16 | ≥32 | 4 | S |
| Moxifloxacin | ≤1 | 2 | ≥4 | 0.25 | S |
| Rifabutin | ≤2 | - | ≥4 | ≤0.25 | S |
| Rifampin | ≤1 | - | ≥2 | 1 | S |
| Streptomicin | No interpretations available | 8 | / | ||
| Trimethoprim/sulfamethoxazole | ≤2/38 | - | ≥4/76 | 0.25/4.75 | S |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mihaljević, Ž.; Reil, I.; Habuš, J.; Štritof, Z.; Naletilić, Š.; Jurkić Krsteska, G.; Kovač, T.; Zdelar-Tuk, M.; Duvnjak, S.; Špičić, S. Mycobacteriosis in a Pet Ferret (Mustela putorius furo) Caused by Mycobacterium xenopi: A Case Report on Neglected Risk of Zoonotic Transmission. Pathogens 2024, 13, 328. https://doi.org/10.3390/pathogens13040328
Mihaljević Ž, Reil I, Habuš J, Štritof Z, Naletilić Š, Jurkić Krsteska G, Kovač T, Zdelar-Tuk M, Duvnjak S, Špičić S. Mycobacteriosis in a Pet Ferret (Mustela putorius furo) Caused by Mycobacterium xenopi: A Case Report on Neglected Risk of Zoonotic Transmission. Pathogens. 2024; 13(4):328. https://doi.org/10.3390/pathogens13040328
Chicago/Turabian StyleMihaljević, Željko, Irena Reil, Josipa Habuš, Zrinka Štritof, Šimun Naletilić, Gabrijela Jurkić Krsteska, Tajna Kovač, Maja Zdelar-Tuk, Sanja Duvnjak, and Silvio Špičić. 2024. "Mycobacteriosis in a Pet Ferret (Mustela putorius furo) Caused by Mycobacterium xenopi: A Case Report on Neglected Risk of Zoonotic Transmission" Pathogens 13, no. 4: 328. https://doi.org/10.3390/pathogens13040328
APA StyleMihaljević, Ž., Reil, I., Habuš, J., Štritof, Z., Naletilić, Š., Jurkić Krsteska, G., Kovač, T., Zdelar-Tuk, M., Duvnjak, S., & Špičić, S. (2024). Mycobacteriosis in a Pet Ferret (Mustela putorius furo) Caused by Mycobacterium xenopi: A Case Report on Neglected Risk of Zoonotic Transmission. Pathogens, 13(4), 328. https://doi.org/10.3390/pathogens13040328