
Performance of Fujifilm Dengue NS1 Antigen Rapid Diagnosis Kit Compared to Quantitative Real-Time Polymerase Chain Reaction

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Rapid Diagnostic Tests
2.3. SD Bioline Dengue NS1 Kit
2.4. Fujifilm Dengue NS1 Kit
2.5. Determination of Primary and Secondary Infections
2.6. Viral RNA Extraction and qRT-PCR
2.7. Statistical Analysis
3. Results
3.1. Characteristics and Distribution of DENV Serotypes
3.2. Performance of the Dengue Rapid Diagnostics Test Kits Compared to the Reference Test (qRT-PCR)
3.3. Analysis of Test Sensitivity Based on Days of Fever
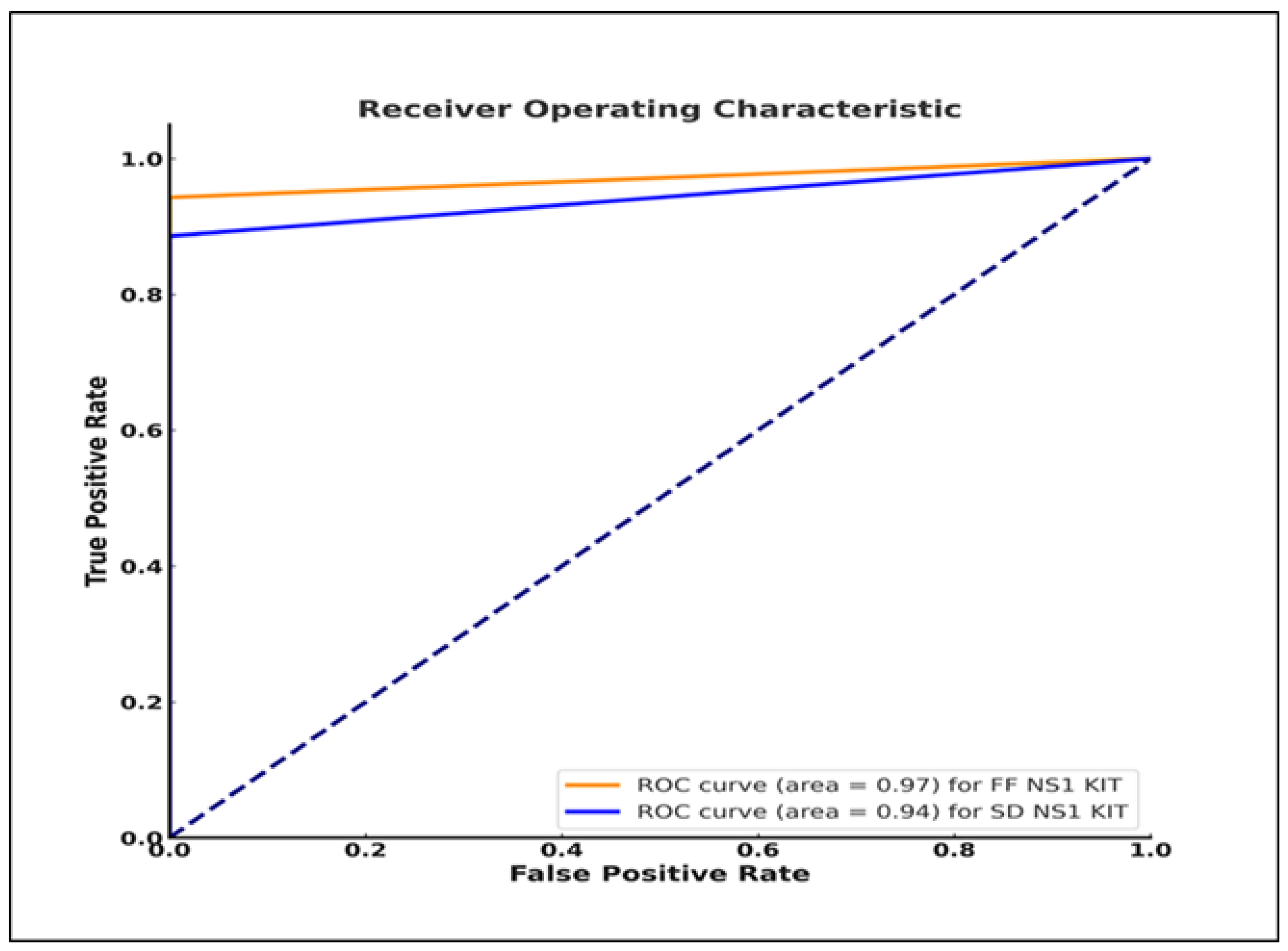
3.4. Evaluation of the Tests’ Diagnostic Ability Compared to the Reference qRT-PCR Results
3.5. Positive Rates of the Two NS1 Kits with Respect to the Type of Dengue Infection
3.6. Comparison between the Two NS1 Kits and Viremia Levels
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Palanichamy Kala, M.; St John, A.L.; Rathore, A.P.S. Dengue: Update on Clinically Relevant Therapeutic Strategies and Vaccines. Curr. Treat. Options Infect. Dis. 2023, 15, 27–52. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, S.; Gething, P.W.; Brady, O.J.; Messina, J.P.; Farlow, A.W.; Moyes, C.L.; Drake, J.M.; Brownstein, J.S.; Hoen, A.G.; Sankoh, O.; et al. The global distribution and burden of dengue. Nature 2013, 496, 504–507. [Google Scholar] [CrossRef] [PubMed]
- Guzman, M.G.; Halstead, S.B.; Artsob, H.; Buchy, P.; Farrar, J.; Gubler, D.J.; Hunsperger, E.; Kroeger, A.; Margolis, H.S.; Martínez, E.; et al. Dengue: A continuing global threat. Nature reviews. Microbiology 2010, 8, S7–S16. [Google Scholar] [CrossRef] [PubMed]
- Vasilakis, N.; Cardosa, J.; Diallo, M.; Sall, A.A.; Holmes, E.C.; Hanley, K.A.; Weaver, S.C.; Mota, J.; Rico-Hesse, R. Sylvatic dengue viruses share the pathogenic potential of urban/endemic dengue viruses. J. Virol. 2010, 84, 3726–3728. [Google Scholar] [CrossRef]
- Gubler, D.J. Dengue, Urbanization and Globalization: The Unholy Trinity of the 21(st) Century. Trop Med. Health 2011, 39 (Suppl. S4), 3–11. [Google Scholar] [CrossRef]
- Cattarino, L.; Rodriguez-Barraquer, I.; Imai, N.; Cummings, D.A.T.; Ferguson, N.M. Mapping global variation in dengue transmission intensity. Sci. Transl. Med. 2020, 12, eaax4144. [Google Scholar] [CrossRef]
- Kularatne, S.A.; Dalugama, C. Dengue infection: Global importance, immunopathology and management. Clin. Med. 2022, 22, 9–13. [Google Scholar] [CrossRef]
- Garg, A.; Garg, J.; Singh, D.V.; Dhole, T.N. Can rapid dengue diagnostic kits be trusted? A comparative study of commercially available rapid kits for serodiagnosis of dengue fever. J. Lab. Physicians 2019, 11, 63–67. [Google Scholar] [CrossRef]
- Normile, D. Tropical medicine. Surprising new dengue virus throws a spanner in disease control efforts. Science 2013, 342, 415. [Google Scholar] [CrossRef]
- Zaw, W.; Lin, Z.; Ko Ko, J.; Rotejanaprasert, C.; Pantanilla, N.; Ebener, S.; Maude, R.J. Dengue in Myanmar: Spatiotemporal epidemiology, association with climate and short-term prediction. PLoS Negl. Trop Dis. 2023, 17, e0011331. [Google Scholar] [CrossRef]
- Sekaran, S.D.; Wang, S.M. Early diagnosis of Dengue infection using a commercial Dengue Duo rapid test kit for the detection of NS1, IGM, and IGG. Am. J. Trop Med. Hyg. 2010, 83, 690–695. [Google Scholar] [CrossRef]
- Inoue, S.; Alonzo, M.T.; Kurosawa, Y.; Mapua, C.A.; Reyes, J.D.; Dimaano, E.M.; Alera, M.T.; Saito, M.; Oishi, K.; Hasebe, F.; et al. Evaluation of a dengue IgG indirect enzyme-linked immunosorbent assay and a Japanese Encephalitis IgG indirect enzyme-linked immunosorbent assay for diagnosis of secondary dengue virus infection. Vector Borne Zoonotic Dis. 2010, 10, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Ito, M.; Takasaki, T.; Yamada, K.; Nerome, R.; Tajima, S.; Kurane, I. Development and evaluation of fluorogenic TaqMan reverse transcriptase PCR assays for detection of dengue virus types 1 to 4. J. Clin. Microbiol. 2004, 42, 5935–5937. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Li, Y.; Guan, Z.; Yang, Y.; Zhang, J.; Sun, Q.; Li, B.; Qiu, Y.; Liu, K.; Shao, D.; et al. Rapid Differential Detection of Japanese Encephalitis Virus and Getah Virus in Pigs or Mosquitos by a Duplex TaqMan Real-Time RT-PCR Assay. Front. Vet. Sci. 2022, 9, 839443. [Google Scholar] [CrossRef]
- Lanciotti, R.S.; Kosoy, O.L.; Laven, J.J.; Velez, J.O.; Lambert, A.J.; Johnson, A.J.; Stanfield, S.M.; Duffy, M.R. Genetic and serologic properties of Zika virus associated with an epidemic, Yap State, Micronesia, 2007. Emerg. Infect. Dis. 2008, 14, 1232–1239. [Google Scholar] [CrossRef]
- Fawcett, T. An introduction to ROC analysis. J. Patrec. 2006, 27, 861–874. [Google Scholar] [CrossRef]
- Parmigiani, G. Receiver Operating Characteristic Curves with an Indeterminacy Zone. J. Patrec. 2020, 136, 94–100. [Google Scholar] [CrossRef]
- Tricou, V.; Vu, H.T.; Quynh, N.V.; Nguyen, C.V.; Tran, H.T.; Farrar, J.; Wills, B.; Simmons, C.P. Comparison of two dengue NS1 rapid tests for sensitivity, specificity and relationship to viraemia and antibody responses. BMC Infect. Dis. 2010, 10, 142. [Google Scholar] [CrossRef]
- Hunsperger, E.A.; Yoksan, S.; Buchy, P.; Nguyen, V.C.; Sekaran, S.D.; Enria, D.A.; Vazquez, S.; Cartozian, E.; Pelegrino, J.L.; Artsob, H.; et al. Evaluation of commercially available diagnostic tests for the detection of dengue virus NS1 antigen and anti-dengue virus IgM antibody. PLoS Negl. Trop Dis. 2014, 8, e3171. [Google Scholar] [CrossRef]
- Teoh, B.T.; Sam, S.S.; Tan, K.K.; Johari, J.; Abd-Jamil, J.; Hooi, P.S.; AbuBakar, S. The Use of NS1 Rapid Diagnostic Test and qRT-PCR to Complement IgM ELISA for Improved Dengue Diagnosis from Single Specimen. Sci. Rep. 2016, 6, 27663. [Google Scholar] [CrossRef]
- Tsai, H.P.; Tsai, Y.Y.; Lin, I.T.; Kuo, P.H.; Chang, K.C.; Chen, J.C.; Ko, W.C.; Wang, J.R. Validation and Application of a Commercial Quantitative Real-Time Reverse Transcriptase-PCR Assay in Investigation of a Large Dengue Virus Outbreak in Southern Taiwan. PLoS Negl. Trop Dis. 2016, 10, e0005036. [Google Scholar] [CrossRef] [PubMed]
- Santoso, M.S.; Yohan, B.; Denis, D.; Hayati, R.F.; Haryanto, S.; Trianty, L.; Noviyanti, R.; Hibberd, M.L.; Sasmono, R.T. Diagnostic accuracy of 5 different brands of dengue virus non-structural protein 1 (NS1) antigen rapid diagnostic tests (RDT) in Indonesia. Diagn. Microbiol. Infect. Dis. 2020, 98, 115116. [Google Scholar] [CrossRef] [PubMed]
- Vickers, I.; Harvey, K.; Nelson, K.; Brown, M.; Bullock-DuCasse, M.; Lindo, J. Evaluation of OneStep Dengue NS1 RapiDip™ InstaTest and OneStep Dengue Fever IgG/IgM RapiCard™ InstaTest during the course of a dengue type 1 epidemic. Diagn. Microbiol. Infect. Dis. 2017, 89, 271–275. [Google Scholar] [CrossRef] [PubMed]
- Simonnet, C.; Okandze, A.; Matheus, S.; Djossou, F.; Nacher, M.; Mahamat, A. Prospective evaluation of the SD BIOLINE Dengue Duo rapid test during a dengue virus epidemic. Eur. J. Clin. Microbiol. Infect. Dis. 2017, 36, 2441–2447. [Google Scholar] [CrossRef] [PubMed]
- Alcon, S.; Talarmin, A.; Debruyne, M.; Falconar, A.; Deubel, V.; Flamand, M. Enzyme-linked immunosorbent assay specific to Dengue virus type 1 nonstructural protein NS1 reveals circulation of the antigen in the blood during the acute phase of disease in patients experiencing primary or secondary infections. J. Clin. Microbiol. 2002, 40, 376–381. [Google Scholar] [CrossRef] [PubMed]
- Anand, A.M.; Sistla, S.; Dhodapkar, R.; Hamide, A.; Biswal, N.; Srinivasan, B. Evaluation of NS1 Antigen Detection for Early Diagnosis of Dengue in a Tertiary Hospital in Southern India. J. Clin. Diagn. Res. 2016, 10, DC01–DC04. [Google Scholar] [CrossRef]
- Yow, K.S.; Aik, J.; Tan, E.Y.; Ng, L.C.; Lai, Y.L. Rapid diagnostic tests for the detection of recent dengue infections: An evaluation of six kits on clinical specimens. PLoS ONE 2021, 16, e0249602. [Google Scholar] [CrossRef]
- Liu, L.T.; Dalipanda, T.; Jagilly, R.; Wang, Y.H.; Lin, P.C.; Tsai, C.Y.; Lai, W.T.; Tsai, J.J. Comparison of two rapid diagnostic tests during a large dengue virus serotype 3 outbreak in the Solomon Islands in 2013. PLoS ONE 2018, 13, e0202304. [Google Scholar] [CrossRef]
- Sánchez-Vargas, L.A.; Sánchez-Marce, E.E.; Vivanco-Cid, H. Evaluation of the SD BIOLINE Dengue Duo rapid test in the course of acute and convalescent dengue infections in a Mexican endemic region. Diagn. Microbiol. Infect. Dis. 2014, 78, 368–372. [Google Scholar] [CrossRef]
- Koraka, P.; Burghoorn-Maas, C.P.; Falconar, A.; Setiati, T.E.; Djamiatun, K.; Groen, J.; Osterhaus, A.D. Detection of immune-complex-dissociated nonstructural-1 antigen in patients with acute dengue virus infections. J. Clin. Microbiol. 2003, 41, 4154–4159. [Google Scholar] [CrossRef]
- Lapphra, K.; Sangcharaswichai, A.; Chokephaibulkit, K.; Tiengrim, S.; Piriyakarnsakul, W.; Chakorn, T.; Yoksan, S.; Wattanamongkolsil, L.; Thamlikitkul, V. Evaluation of an NS1 antigen detection for diagnosis of acute dengue infection in patients with acute febrile illness. Diagn. Microbiol. Infect. Dis. 2008, 60, 387–391. [Google Scholar] [CrossRef]
- Martínez-Cuellar, C.; Lovera, D.; Galeano, F.; Gatti, L.; Arbo, A. Non-structural protein 1 (NS1) of dengue virus detection correlates with severity in primary but not in secondary dengue infection. J. Clin. Virol. Off. Publ. Pan Am. Soc. Clin. Virol. 2020, 124, 104259. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Test Kit | Sensitivity% (95% CI) | Specificity% (95% CI) | PPV% (95% CI) | NPV% (95% CI) | PLR (95% CI) | NLR (95% CI) | Test Accuracy (95% CI) * | Test Concordance (k) | p-Value (Comparing Sensitivities) |
|---|---|---|---|---|---|---|---|---|---|
| FF NS1 Kit | 94.3% (86.2–97.8) | 100% (94.8–100) | 100% (94.5–100) | 94.6% (86.9–97.9) | ∞ | 0.057 (0.02–0.14) | 97.1 (92.9–99.2) | 0.94, p < 0.001 | 0.125 |
| SD NS1 Kit | 88.6% (79.0–94.1) | 100% (94.8–100) | 100% (94.2–100) | 89.8% (81.0–94.7) | ∞ | 0.114 (0.06–0.21) | 94.3 (89.1–97.5) | 0.89, p < 0.001 |
| Sample ID | Sex | Age (Years) | Diagnosis | Dengue Serotype | Days of Fever | Viral RNA Copies/Reaction | FF NS1 Kit | SD NS1 Kit | Primary (P) or Secondary (S) Infection |
|---|---|---|---|---|---|---|---|---|---|
| 1 | M | 7.0 | DWoWS | DENV-1 | 3 | 1.8 × 105 | + | + | P |
| 2 | F | 8.0 | DWWS | DENV-1 | 3 | 7.1 × 105 | + | + | P |
| 3 | F | 11.0 | SD | DENV-1 | 4 | 3.5 × 104 | + | + | P |
| 4 | M | 2.0 | DWWS | DENV-1 | 5 | 4.2 × 104 | + | + | P |
| 5 | F | 7.3 | SD | DENV-1 | 4 | 1.1 × 105 | + | + | S |
| 6 | M | 14.0 | DWWS | DENV-1 | 4 | 6.2 × 104 | + | + | P |
| 7 | F | 11.1 | DWWS | DENV-1 | 4 | 5.6 × 104 | + | + | S |
| 8 | F | 15.0 | DWoWS | DENV-1 | 5 | 7.7 × 105 | + | + | S |
| 9 | F | 13.0 | DWoWS | DENV-1 | 2 | 5.2 × 104 | + | + | P |
| 10 | M | 9.0 | DWoWS | DENV-1 | 4 | 1.2 × 104 | + | + | P |
| 11 | F | 9.0 | DWoWS | DENV-1 | 4 | 3.8 × 106 | + | + | P |
| 12 | F | 2.5 | DWoWS | DENV-1 | 3 | 3.5 × 105 | + | + | P |
| 13 | F | 9.0 | DWoWS | DENV-1 | 4 | 2.3 × 107 | + | + | P |
| 14 | M | 30.0 | DWoWS | DENV-1 | 4 | 3.7 × 104 | + | + | P |
| 15 | M | 18.0 | DWoWS | DENV-1 | 2 | 8.8 × 105 | + | + | P |
| 16 | M | 20.0 | DWoWS | DENV-1 | 3 | 1.1 × 106 | + | + | P |
| 17 | M | 22.0 | DWoWS | DENV-1 | 2 | 2.3 × 107 | + | + | P |
| 18 | M | 9.0 | DWWS | DENV-1 | 4 | 5.7 × 106 | + | + | P |
| 19 | F | 12.0 | SD | DENV-1 | 3 | 6.0 × 106 | + | + | P |
| 20 | F | 7.5 | DWoWS | DENV-1 | 5 | 1.9 × 104 | + | + | P |
| 21 | F | 9.0 | DWWS | DENV-1 | 4 | 1.2 × 107 | + | + | P |
| 22 | M | 11.0 | DWWS | DENV-1 | 4 | 2.2 × 104 | + | + | P |
| 23 | M | 5.0 | DWoWS | DENV-1 | 4 | 1.6 × 104 | − | − | P |
| 24 | F | 9.0 | DWWS | DENV-1 | 4 | 1.0 × 106 | + | + | S |
| 25 | M | 11.0 | DWWS | DENV-1 | 2 | 8.1 × 104 | − | − | S |
| 26 | F | 12.0 | DWWS | DENV-2 | 3 | 1.4 × 104 | + | + | S |
| 27 | M | 3.0 | DWWS | DENV-2 | 5 | 1.3 × 104 | − | − | S |
| 28 | M | 16.0 | DWWS | DENV-2 | 4 | 2.1 × 104 | + | + | S |
| 29 | M | 8.0 | DWWS | DENV-2 | 3 | 1.6 × 104 | − | − | S |
| 30 | M | 5.3 | DWoWS | DENV-2 | 4 | 2.6 × 104 | + | − | S |
| 31 | M | 11.0 | DWoWS | DENV-2 | 1 | 4.4 × 105 | + | − | P |
| 32 | M | 3.0 | DWWS | DENV-2 | 4 | 9.7 × 104 | + | + | P |
| 33 | F | 6.0 | DWWS | DENV-2 | 3 | 2.5 × 104 | + | + | P |
| 34 | M | 4.0 | DWoWS | DENV-3 | 3 | 2.2 × 104 | + | + | P |
| 35 | F | 8.0 | DWWS | DENV-3 | 3 | 2.2 × 105 | + | + | P |
| 36 | M | 16.0 | DWoWS | DENV-3 | 3 | 5.6 × 104 | + | + | P |
| 37 | M | 7.0 | DWoWS | DENV-3 | 4 | 5.0 × 105 | + | + | P |
| 38 | M | 8.0 | DWWS | DENV-3 | 3 | 1.3 × 105 | + | + | S |
| 39 | M | 11.0 | DWoWS | DENV-3 | 4 | 3.4 × 104 | + | + | P |
| 40 | M | 10.0 | DWWS | DENV-3 | 3 | 2.7 × 104 | + | + | P |
| 41 | F | 15.0 | DWWS | DENV-3 | 4 | 1.5 × 105 | + | + | P |
| 42 | M | 15.0 | DWWS | DENV-3 | 4 | 1.0 × 104 | + | + | S |
| 43 | M | 23.0 | DWoWS | DENV-3 | 2 | 6.6 × 104 | + | + | P |
| 44 | M | 15.0 | DWoWS | DENV-3 | 6 | 2.8 × 104 | + | + | P |
| 45 | M | 17.0 | DWWS | DENV-3 | 3 | 2.2 × 104 | + | + | P |
| 46 | M | 8.0 | DWWS | DENV-3 | 3 | 4.3 × 105 | + | + | P |
| 47 | M | 11.0 | DWWS | DENV-3 | 7 | 5.2 × 104 | + | + | P |
| 48 | M | 5.5 | DWoWS | DENV-3 | 5 | 5.9 × 104 | + | + | P |
| 49 | F | 8.0 | SD | DENV-4 | 4 | 3.7 × 106 | + | + | S |
| 50 | M | 15.0 | DWoWS | DENV-4 | 4 | 3.0 × 105 | + | + | S |
| 51 | M | 17.0 | DWoWS | DENV-4 | 2 | 1.5 × 105 | + | + | S |
| 52 | F | 9.0 | DWWS | DENV-4 | 7 | 1.2 × 104 | + | + | S |
| 53 | F | 6.5 | SD | DENV-4 | 4 | 7.1 × 104 | + | − | S |
| 54 | M | 10.0 | DWWS | DENV-4 | 5 | 3.6 × 105 | + | + | S |
| 55 | F | 27.0 | DWoWS | DENV-4 | 2 | 1.9 × 106 | + | + | S |
| 56 | M | 14.0 | DWWS | DENV-4 | 4 | 2.9 × 105 | + | + | S |
| 57 | M | 14.0 | DWoWS | DENV-4 | 3 | 9.0 × 105 | + | + | S |
| 58 | M | 13.0 | DWWS | DENV-4 | 4 | 2.2 × 106 | + | + | S |
| 59 | M | 9.0 | DWoWS | DENV-4 | 6 | 1.6 × 105 | + | + | S |
| 60 | F | 6.7 | DWoWS | DENV-4 | 3 | 6.3 × 105 | + | + | S |
| 61 | F | 2.8 | DWoWS | DENV-4 | 3 | 4.0 × 106 | + | + | S |
| 62 | F | 23.0 | DWoWS | DENV-4 | 2 | 1.5 × 107 | + | + | S |
| 63 | F | 14.0 | DWWS | DENV-4 | 4 | 5.7 × 106 | + | + | S |
| 64 | M | 7.0 | SD | DENV-4 | 3 | 3.0 × 107 | + | + | P |
| 65 | M | 8.0 | DWWS | DENV-4 | 4 | 3.0 × 106 | + | + | P |
| 66 | F | 12.0 | DWoWS | DENV-4 | 3 | 2.1 × 106 | + | + | P |
| 67 | M | 25.0 | DWoWS | DENV-4 | 4 | 1.2 × 104 | + | + | S |
| 68 | F | 22.0 | DWoWS | DENV-4 | 5 | 9.3 × 104 | + | + | S |
| 69 | M | 11.0 | DWoWS | DENV-4 | 3 | 1.2 × 104 | + | + | P |
| 70 | F | 13.0 | SD | DENV-4 | 5 | 1.8 × 104 | + | − | S |
| Type of Infection | Number of Patients | Number of Patients with Infection Status (%, 95% CI) | |
|---|---|---|---|
| FF NS1 Kit | SD NS1 Kit | ||
| Primary | 40 | 39 (97.5%, 92.7–100%) | 38 (95%, 88.2–100%) |
| Secondary | 30 | 27 (90%, 79.3–100%) | 24 (80%, 65.7–94.3%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ngwe Tun, M.M.; Kapandji, M.; Wada, A.; Yamamoto, K.; Dumre, S.P.; Nwe, K.M.; Lin, H.; Takamatsu, Y.; Thant, K.Z.; Thu, H.M.; et al. Performance of Fujifilm Dengue NS1 Antigen Rapid Diagnosis Kit Compared to Quantitative Real-Time Polymerase Chain Reaction. Pathogens 2024, 13, 818. https://doi.org/10.3390/pathogens13090818
Ngwe Tun MM, Kapandji M, Wada A, Yamamoto K, Dumre SP, Nwe KM, Lin H, Takamatsu Y, Thant KZ, Thu HM, et al. Performance of Fujifilm Dengue NS1 Antigen Rapid Diagnosis Kit Compared to Quantitative Real-Time Polymerase Chain Reaction. Pathogens. 2024; 13(9):818. https://doi.org/10.3390/pathogens13090818
Chicago/Turabian StyleNgwe Tun, Mya Myat, Merveille Kapandji, Atsuhiko Wada, Ko Yamamoto, Shyam Prakash Dumre, Khine Mya Nwe, Htin Lin, Yuki Takamatsu, Kyaw Zin Thant, Hlaing Myat Thu, and et al. 2024. "Performance of Fujifilm Dengue NS1 Antigen Rapid Diagnosis Kit Compared to Quantitative Real-Time Polymerase Chain Reaction" Pathogens 13, no. 9: 818. https://doi.org/10.3390/pathogens13090818
APA StyleNgwe Tun, M. M., Kapandji, M., Wada, A., Yamamoto, K., Dumre, S. P., Nwe, K. M., Lin, H., Takamatsu, Y., Thant, K. Z., Thu, H. M., Urano, T., Pandey, B. D., & Morita, K. (2024). Performance of Fujifilm Dengue NS1 Antigen Rapid Diagnosis Kit Compared to Quantitative Real-Time Polymerase Chain Reaction. Pathogens, 13(9), 818. https://doi.org/10.3390/pathogens13090818