
Patient Experiences and Perceptions with Infections Due to Multidrug-Resistant Organisms: A Systematic Review
 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection
2.3. Quality Appraisal
2.4. Data Extraction
2.5. Study Outcomes
3. Results
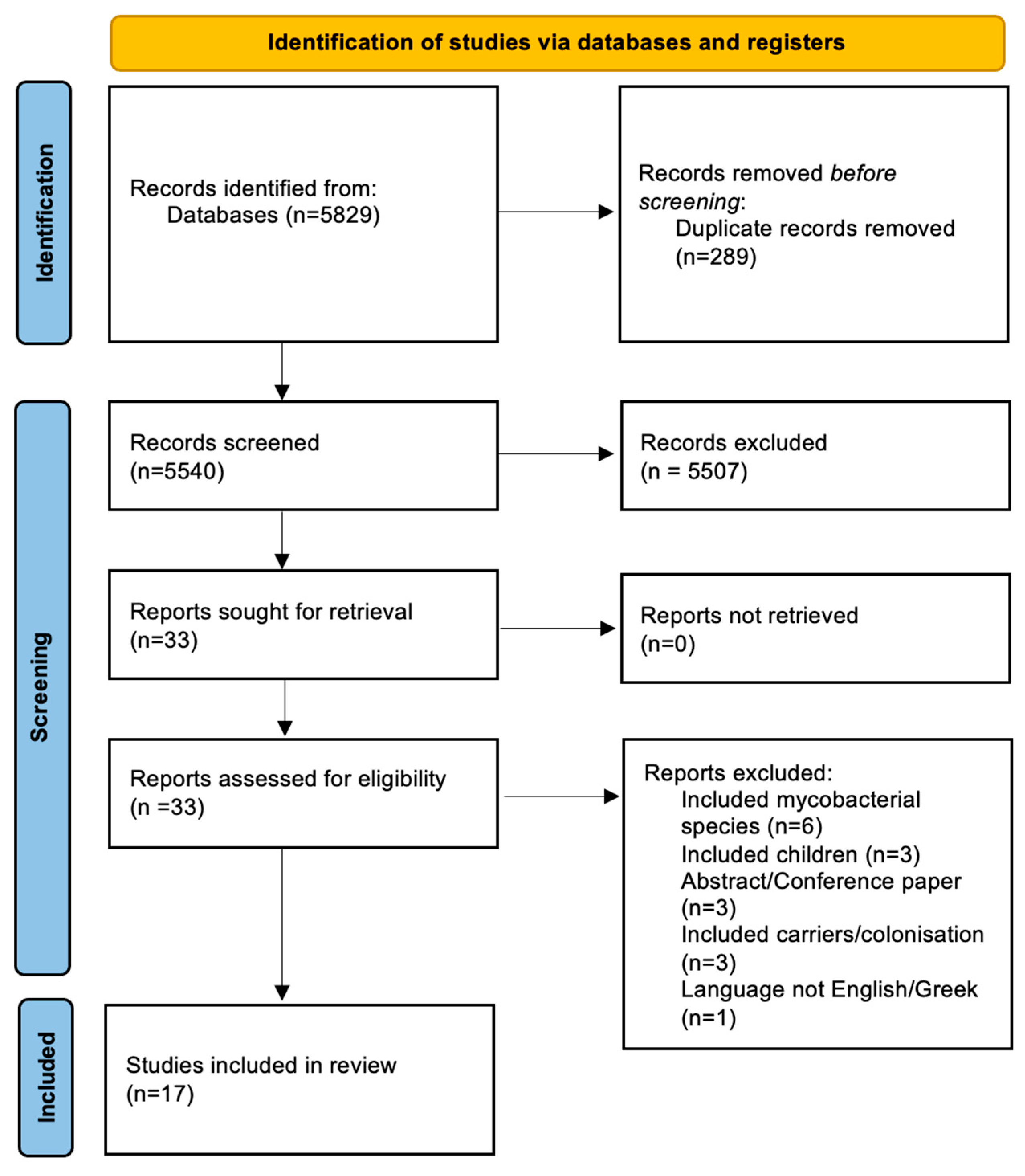
3.1. Literature Search
3.2. Study and Population Characteristics
3.3. Findings from Quantitative Studies
3.3.1. Depression
3.3.2. Anxiety
3.3.3. Other Psychological Aspects
3.4. Findings from Qualitative Studies
3.4.1. Depression and Anxiety
3.4.2. Understanding and Coping
3.4.3. Communication and Information Gaps
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Ibert, F.; Eckstein, M.; Günther, F.; Mutters, N.T. The Relationship between Subjective Perception and the Psychological Effects of Patients in Spatial Isolation. GMS Hyg. Infect. Control 2017, 12, Doc11. [Google Scholar] [CrossRef] [PubMed Central]
- Wiersinga, W.J.; Koopmans, M.P.G.; van Dissel, J.T. Rise and threat of infectious diseases. Ned. Tijdschr. Geneeskd. 2020, 163, D4545. [Google Scholar]
- Yang, X.; Guo, R.; Zhang, B.; Xie, B.; Zhou, S.; Zhang, B.; Lai, Q. Retrospective Analysis of Drug Resistance Characteristics and Infection Related Risk Factors of Multidrug-Resistant Organisms (MDROs) Isolated from the Orthopedics Department of a Tertiary Hospital. Sci. Rep. 2023, 13, 2199. [Google Scholar] [CrossRef]
- Santajit, S.; Indrawattana, N. Mechanisms of Antimicrobial Resistance in ESKAPE Pathogens. BioMed Res. Int. 2016, 2016, 2475067. [Google Scholar] [CrossRef]
- Saleem, M.; de la Bastide, A.; Korzen, M. Antibiotics Overuse and Bacterial Resistance. Ann. Microbiol. Res. 2019, 3, 93–99. [Google Scholar] [CrossRef]
- Mainous, A.G.; Diaz, V.A.; Matheson, E.M.; Gregorie, S.H.; Hueston, W.J. Trends in Hospitalizations with Antibiotic-Resistant Infections: U.S., 1997–2006. Public Health Rep. 2011, 126, 354–360. [Google Scholar] [CrossRef]
- Cassini, A.; Högberg, L.D.; Plachouras, D.; Quattrocchi, A.; Hoxha, A.; Simonsen, G.S.; Colomb-Cotinat, M.; Kretzschmar, M.E.; Devleesschauwer, B.; Cecchini, M.; et al. Attributable Deaths and Disability-Adjusted Life-Years Caused by Infections with Antibiotic-Resistant Bacteria in the EU and the European Economic Area in 2015: A Population-Level Modelling Analysis. Lancet Infect. Dis. 2019, 19, 56–66. [Google Scholar] [CrossRef]
- Johnston, K.J.; Thorpe, K.E.; Jacob, J.T.; Murphy, D.J. The Incremental Cost of Infections Associated with Multidrug—resistant Organisms in the Inpatient Hospital Setting—A National Estimate. Health Serv. Res. 2019, 54, 782–792. [Google Scholar] [CrossRef]
- Moro, M.; Vigezzi, G.P.; Callari, E.; Biancardi, A.; Nizzero, P.; Cichero, P.; Signorelli, C.; Odone, A. Multidrug-Resistant Organism Infections and Mortality: Estimates from a Large Italian Hospital. Eur. J. Public Health 2020, 30, v166–v167. [Google Scholar] [CrossRef]
- Troiano, G.; Mercurio, I.; Nante, N.; Lancia, M.; Bacci, M. Candida Autovaccination: A New Strategy to Prevent Antifungal Resistance? J. Infect. Prev. 2018, 19, 201–202. [Google Scholar] [CrossRef]
- Troiano, G.; Messina, G.; Nante, N. BACTERIAL LYSATES (OM-85 BV): A Cost-Effective Proposal in Order to Contrast Antibiotic Resistance. J. Prev. Med. Hyg. 2021, 62, E564. [Google Scholar] [CrossRef]
- Baron, R.; Eilers, R.; Haverkate, M.R.; Feenstra, S.G.; Timen, A. A Qualitative Study Examining the Impact of Multidrug-Resistant Organism (MDRO) Carriage on the Daily Lives of Carriers and Parents of Carriers with Experiences of Hospital Precautionary Measures. Antimicrob. Resist. Infect. Control 2022, 11, 103. [Google Scholar] [CrossRef]
- Watson, E.; Tsindos, T.; Peleg, A.Y.; Bass, P.; Stewardson, A.J.; Ayton, D.; Peel, T. Understanding Patient and Healthcare Worker Experiences and Perspectives of Multidrug-Resistant Organisms. JAC-Antimicrob. Resist. 2023, 5, dlad071. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. Br. Med. J. 2021, 372, n71. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A Web and Mobile App for Systematic Reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- JBI Manual for Evidence Synthesis; Aromataris, E., Lockwood, C., Porritt, K., Pilla, B., Jordan, Z., Eds.; JBI: Miami, FL, USA, 2024; ISBN 978-0-648-84882-0. [Google Scholar]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 23 February 2022).
- Hong, Q.N.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.-P.; Griffiths, F.; Nicolau, B.; O’Cathain, A.; et al. The Mixed Methods Appraisal Tool (MMAT) Version 2018 for Information Professionals and Researchers. Educ. Inf. 2018, 34, 285–291. [Google Scholar] [CrossRef]
- Catalano, G.; Houston, S.H.; Catalano, M.C.; Butera, A.S.; Jennings, S.M.; Hakala, S.M.; Burrows, S.L.; Hickey, M.G.; Duss, C.V.; Skelton, D.N.; et al. Anxiety and Depression in Hospitalized Patients in Resistant Organism Isolation. South. Med. J. 2003, 96, 141–145. [Google Scholar] [CrossRef]
- Day, H.R.; Perencevich, E.N.; Harris, A.D.; Gruber-Baldini, A.L.; Himelhoch, S.S.; Brown, C.H.; Morgan, D.J. Depression, Anxiety, and Moods of Hospitalized Patients under Contact Precautions. Infect. Control Hosp. Epidemiol. 2013, 34, 251–258. [Google Scholar] [CrossRef]
- Evans, H.L.; Shaffer, M.M.; Hughes, M.G.; Smith, R.L.; Chong, T.W.; Raymond, D.P.; Pelletier, S.J.; Pruett, T.L.; Sawyer, R.G. Contact Isolation in Surgical Patients: A Barrier to Care? Surgery 2003, 134, 180–188. [Google Scholar] [CrossRef]
- Findik, U.Y.; Ozbaş, A.; Cavdar, I.; Erkan, T.; Topcu, S.Y. Effects of the Contact Isolation Application on Anxiety and Depression Levels of the Patients. Int. J. Nurs. Pract. 2012, 18, 340–346. [Google Scholar] [CrossRef]
- Gaube, S.; Däumling, S.; Biebl, I.; Rath, A.; Caplunik-Pratsch, A.; Schneider-Brachert, W. Patients with Multi-Drug-Resistant Organisms Feel Inadequately Informed about Their Status: Adverse Effects of Contact Isolation. J. Hosp. Infect. 2023, 133, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, P.; Hamilton, L.R. Psychological Impact of the Management of Methicillin-Resistant Staphylococcus Aureus (MRSA) in Patients with Spinal Cord Injury. Spinal Cord. 1997, 35, 617–619. [Google Scholar] [CrossRef]
- Soon, M.M.L.; Madigan, E.; Jones, K.R.; Salata, R.A. An Exploration of the Psychologic Impact of Contact Isolation on Patients in Singapore. Am. J. Infect. Control 2013, 41, e111–e113. [Google Scholar] [CrossRef] [PubMed]
- Stelfox, H.T. Safety of Patients Isolated for Infection Control. J. Am. Med. Assoc. 2003, 290, 1899. [Google Scholar] [CrossRef] [PubMed]
- Tarzi, S.; Kennedy, P.; Stone, S.; Evans, M. Methicillin-Resistant Staphylococcus Aureus: Psychological Impact of Hospitalization and Isolation in an Older Adult Population. J. Hosp. Infect. 2001, 49, 250–254. [Google Scholar] [CrossRef]
- Barratt, R.; Shaban, R.; Moyle, W. Behind Barriers: Patients’ Perceptions of Source Isolation for Methicillin—Resistant Staphylococcus Aureus (MRSA). Aust. J. Adv. Nurs. 2011, 28, 53–58. [Google Scholar] [CrossRef]
- Day, H.R.; Perencevich, E.N.; Harris, A.D.; Himelhoch, S.S.; Brown, C.H.; Gruber-Baldini, A.L.; Dotter, E.; Morgan, D.J. Do Contact Precautions Cause Depression? A Two-Year Study at a Tertiary Care Medical Centre. J. Hosp. Infect. 2011, 79, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Goldsack, J.C.; DeRitter, C.; Power, M.; Spencer, A.; Taylor, C.L.; Kim, S.F.; Kirk, R.; Drees, M. Clinical, Patient Experience and Cost Impacts of Performing Active Surveillance on Known Methicillin-Resistant Staphylococcus Aureus Positive Patients Admitted to Medical-Surgical Units. Am. J. Infect. Control 2014, 42, 1039–1043. [Google Scholar] [CrossRef]
- Lindberg, M.; Carlsson, M.; Högman, M.; Skytt, B. Suffering from Meticillin-Resistant Staphylococcus Aureus: Experiences and Understandings of Colonisation. J. Hosp. Infect. 2009, 73, 271–277. [Google Scholar] [CrossRef]
- Newton, J.T.; Constable, D.; Senior, V. Patients’ Perceptions of Methicillin-Resistant Staphylococcus Aureus and Source Isolation: A Qualitative Analysis of Source-Isolated Patients. J. Hosp. Infect. 2001, 48, 275–280. [Google Scholar] [CrossRef]
- Skyman, E.; Sjöström, H.T.; Hellström, L. Patients’ Experiences of Being Infected with MRSA at a Hospital and Subsequently Source Isolated. Scand. J. Caring Sci. 2010, 24, 101–107. [Google Scholar] [CrossRef]
- Smith, A.; Ray-Barruel, G. Patients’ Perceptions and Knowledge of Source Isolation for Multi-Resistant Organisms in an Australian Metropolitan Hospital: A Bedside Interview with Questionnaire Study. Patient Exp. J. 2022, 9, 126–135. [Google Scholar] [CrossRef]
- Criddle, P.; Potter, J. Exploring Patients’ Views on Colonisation with Meticillin-Resistant Staphylococcus Aureus. Br. J. Infect. Control 2006, 7, 24–28. [Google Scholar] [CrossRef]
- Hays, R.D. Functioning and Well-Being Outcomes of Patients with Depression Compared with Chronic General Medical Illnesses. Arch. Gen. Psychiatry 1995, 52, 11–19. [Google Scholar] [CrossRef]
- Wassenberg, M.W.M.; Severs, D.; Bonten, M.J.M. Psychological Impact of Short-Term Isolation Measures in Hospitalised Patients. J. Hosp. Infect. 2010, 75, 124–127. [Google Scholar] [CrossRef] [PubMed]
- Prina, A.M.; Cosco, T.D.; Dening, T.; Beekman, A.; Brayne, C.; Huisman, M. The Association between Depressive Symptoms in the Community, Non-Psychiatric Hospital Admission and Hospital Outcomes: A Systematic Review. J. Psychosom. Res. 2015, 78, 25–33. [Google Scholar] [CrossRef]
- Elpers, H.; Teismann, H.; Wellmann, J.; Berger, K.; Karch, A.; Rübsamen, N. Major Depressive Disorders Increase the Susceptibility to Self-Reported Infections in Two German Cohort Studies. Soc. Psychiatry Psychiatr. Epidemiol. 2023, 58, 277–286. [Google Scholar] [CrossRef] [PubMed]
- Rona, R.J.; Fear, N.T.; Hull, L.; Greenberg, N.; Earnshaw, M.; Hotopf, M.; Wessely, S. Mental Health Consequences of Overstretch in the UK Armed Forces: First Phase of a Cohort Study. Br. Med. J. 2007, 335, 603. [Google Scholar] [CrossRef]
- Gudnadottir, U.; Fritz, J.; Zerbel, S.; Bernardo, A.; Sethi, A.K.; Safdar, N. Reducing Health Care-Associated Infections: Patients Want to Be Engaged and Learn about Infection Prevention. Am. J. Infect. Control 2013, 41, 955–958. [Google Scholar] [CrossRef]
- Erdek, F.O. The Effect of the Infections Control Prevention and Infection Rates of the Infection Control Prevention Education That Is given to the Inpatients and Their Relatives. North. Clin. Istanb. 2017, 4, 29–35. [Google Scholar] [CrossRef]
- Chen, X.; Du, L.; Wu, R.; Xu, J.; Ji, H.; Zhang, Y.; Zhu, X.; Zhou, L. The Effects of Family, Society and National Policy Support on Treatment Adherence among Newly Diagnosed Tuberculosis Patients: A Cross-Sectional Study. BMC Infect. Dis. 2020, 20, 623. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| PICOS Category | Keywords |
|---|---|
| Population | Young adult [MeSH]; middle age; age 80 and over; age 65 and older; hospitalized; inpatient [MeSH] |
| Intervention/exposure | MDRO, drug resistance; microbial [MeSH], multi drug resistant bacteria; multi drug resistant pathogen |
| Comparator | - |
| Outcome | Patient experience; patient attitude; effect on patients; patient well-being; patient psychology; patient mental being; emotional effect; patient perception; psychological aspects of illness |
| Study Design | Case-control study; observational study |
| Author (Year of Publication) | Methodology | Population Characteristics | Control Characteristics | Main Findings |
|---|---|---|---|---|
| Barratt et al. (2011) [28] | Qualitative design, semi-structured interviews. | 10 adult patients hospitalized with MRSA infection in single rooms for at least 3 days. | N/A | Stigma, contamination, anger, frustration, and guilt were experienced by patients during MRSA isolation. Patients pursued greater insight into infection prevention and MRSA, recognizing the significance of PPE for others’ safety. |
| Catalano et al. (2003) [19] | Matched cohort testing. HAM-A and HAM-D were used to assess anxiety and depression levels. | 27 patients aged 18 or above, infected with MRSA or VRE. | 20 patients with an infectious disease not requiring isolation. | Depression and anxiety scores were both higher in the isolated, infected group compared to controls (p < 0.01) after 1 and 2 weeks. |
| Day et al. (2011) [29] | Retrospective cohort study. | 4782 patients on contact precaution due to MDRO infection. | N/A | Contact precautions were associated with depression (odds ratio (OR) 1.4, 95% confidence interval (CI) 1.2–1.5) but not with anxiety (OR 0.8, 95% CI 0.7–1.1) in the non-ICU population. |
| Day et al. (2013) [20] | Prospective frequency-matched cohort study. | 238 patients infected with Clostridioides difficile or other MDRO were placed in contact precautions. | 290 patients with Clostridioides difficile or other MDRO not placed in contact precaution. | Three days following contact precautions, isolated patients showed no increase in depression levels. Contact precautions were also unrelated to happiness, sadness, worry, or anger as reflected by a VAMS score of 10%. |
| Evans et al. (2003) [21] | Matched cohort observation, questionnaire using Likert scale, retrospective review incidence. | 485 isolated patients, of which 58% were infected with MRSA, VRE, Clostridioides difficile, multidrug-resistant Acinetobacter spp., or multidrug-resistant S. maltophilia. | 1002 non-isolated patients in ICU setting. | Patients in isolation were seen less by healthcare professionals compared to non-isolated patients (p < 0.01). |
| Findik et al. (2012) [22] | Non-randomized quasi-experimental study. Data acquired (HADS-A (anxiety) and HADS-D (depression)) and patient information form. | 60 patients with an MDRO * infection were isolated in a single room for 5 days. | 57 non-isolated patients with a hospital infection diagnosis. | No statistically significant difference in anxiety and depression was found between isolated and non-isolated patients. However, females and those with lower income levels in the isolated group had higher levels of depression. |
| Gaube et al. (2023) [23] | Matched case-control study. | 118 patients with contact isolation due to VRE, MRSA, or multidrug-resistant gram-negative bacteria infections | 149 matched controls who were non-isolated (matched by hospital ward, sex, condition severity, age, and length of stay). | Patients under contact isolation reported greater dissatisfaction than non-isolated patients, particularly due to a lack of information provision regarding their MDRO diagnosis. |
| Goldsack et al. (2014) [30] | Mixed methods retrospective evaluation of patients diagnosed with MRSA infection. | 211 patients in contact isolation due to MRSA infection, with 32 patients being selected for the questionnaire. Mean age: 61. | N/A | 41% of patients reported contact isolation impacted their hospital stay, citing concerns about transmission, fewer visitors, feelings of anger, and contamination. Additionally, 28% experienced distress from isolation, feeling stigmatized, neglected, and having limited rights and privileges. |
| Kennedy and Hamilton (1997) [24] | Cross-sectional matched control study | 16 patients infected with MRSA, aged 18–65. | MRSA-negative matched controls (matched for age, sex, level of injury, and time since admission or injury). | 50% of the participants felt contact isolation worsened their mood, while 30% found it helpful in coping with their illness. Despite overall psychological well-being remaining mostly unchanged, isolated patients reported a significant rise in anger. |
| Lindberg et al. (2009) [31] | Qualitative design. | 14 interviews of patients infected with MRSA. | N/A | Patients encountered fears and daily limitations due to MRSA colonization and felt a responsibility to prevent infection spread. Patient experiences with healthcare workers varied. |
| Newton et al. (2001) [32] | Qualitative, semi-structured interviews. | 19 patients infected with MRSA hospitalized and placed in source isolation. | N/A | Patients had limited knowledge of MRSA’s impact, however, half deemed it “serious”. Most were uncertain about its origin and the purpose of isolation, despite seeing its pros and cons. Isolation did not appear to affect them psychologically. |
| Skyman et al. (2010) [33] | Qualitative, semi-structured interviews. | 6 adult patients hospitalized in single rooms due to MRSA infection. All patients have been isolated for at least one week. | N/A | Contact isolation caused participants to feel confined, stigmatized, ashamed, and isolated. Patients criticized staff for not washing their hands regularly. Patients complained about being misinformed and confused regarding their MRSA diagnosis. |
| Smith and Ray-Barruel (2022) [34] | Bedside interviews with structured questionnaires. | 30 patients with MRSA, VRE, or ESBL with a median age of 67 years | N/A | 70% of patients were unaware of their infection and 23.3% were unsure of its duration. There was a clear preference for face-to-face education (96.7%) and brochures (86.7%) over phone calls (33.3%) and videos (0%). Communication and knowledge gaps exacerbated detrimental psychological effects, including fear and loneliness. |
| Soon et al. (2013) [25] | Cross-sectional matched control. HADS, MSPSS, PSS, and Euroqol Questionnaire tests were used. | 20 patients in isolation due to MDRO * infection were compared to 20 non-isolated controls. | 20 infected patients not in contact isolation. | A statistically significant increase in depression (t = 3.731, p < 0.01) and anxiety (t = 4.841, p < 0.001) was reported in patients in contact isolation compared with the controls. |
| Stelfox et al. (2003) [26] | Two matched cohorts | 78 patients isolated due to MRSA infection. | 156 non-isolated patients with other infectious disorders. | Patients in contact isolation were more likely to have their vital signs incompletely recorded or have days with no vital sign recordings at all (p = 0.08). |
| Tarzi et al. (2001) [27] | Cross-sectional matched control. The Abbreviated Mental Score, The Barthel Index, The Geriatric Depression Scale, and The Profile of Mood State tests were used. | 22 MRSA-infected patients. Patients older than 65 in isolation. | 20 non-isolated, MRSA-negative patients. | Independent sample t-tests showed higher levels of anxiety (t = 2.98, p < 0.01) and depression (t = 3, p < 0.01) in the isolated group compared to the non-isolated group. No difference in anger levels was reported (t = 0.06, not significant). |
| Watson et al. (2023) [13] | A sequential exploratory mixed-methods study, with semi-structured, face-to-face interviews. | 76 patients approached, of which 20 patients conducted the interviews. The majority were males, older than 52 years. Patients had documented CPE or VRE infection. | N/A | Just 35% of staff reported that they would know exactly what to do if a patient was CPE-positive. Patients were confused by staff practices and inconsistent isolation protocols. Several individuals were not adequately aware of their MDRO diagnosis due to insufficient information. Written materials or verbal discussions with healthcare professionals were suggested as better information sources. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
AlRawashdeh, M.M.; Ishak, A.; Al-Bunnia, A.; Agouridis, A.P.; Lytras, T.; Spernovasilis, N.; Tsioutis, C. Patient Experiences and Perceptions with Infections Due to Multidrug-Resistant Organisms: A Systematic Review. Pathogens 2024, 13, 817. https://doi.org/10.3390/pathogens13090817
AlRawashdeh MM, Ishak A, Al-Bunnia A, Agouridis AP, Lytras T, Spernovasilis N, Tsioutis C. Patient Experiences and Perceptions with Infections Due to Multidrug-Resistant Organisms: A Systematic Review. Pathogens. 2024; 13(9):817. https://doi.org/10.3390/pathogens13090817
Chicago/Turabian StyleAlRawashdeh, Mousa M., Angela Ishak, Ahmed Al-Bunnia, Aris P. Agouridis, Theodore Lytras, Nikolaos Spernovasilis, and Constantinos Tsioutis. 2024. "Patient Experiences and Perceptions with Infections Due to Multidrug-Resistant Organisms: A Systematic Review" Pathogens 13, no. 9: 817. https://doi.org/10.3390/pathogens13090817
APA StyleAlRawashdeh, M. M., Ishak, A., Al-Bunnia, A., Agouridis, A. P., Lytras, T., Spernovasilis, N., & Tsioutis, C. (2024). Patient Experiences and Perceptions with Infections Due to Multidrug-Resistant Organisms: A Systematic Review. Pathogens, 13(9), 817. https://doi.org/10.3390/pathogens13090817