
Probiotic Therapy with Lactobacillus acidophilus and Bifidobacterium animalis subsp. lactis Results in Infarct Size Limitation in Rats with Obesity and Chemically Induced Colitis
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Animals
2.3. Chemicals
2.4. Modelling of Diet-Induced Obesity
2.5. Induction of Colitis
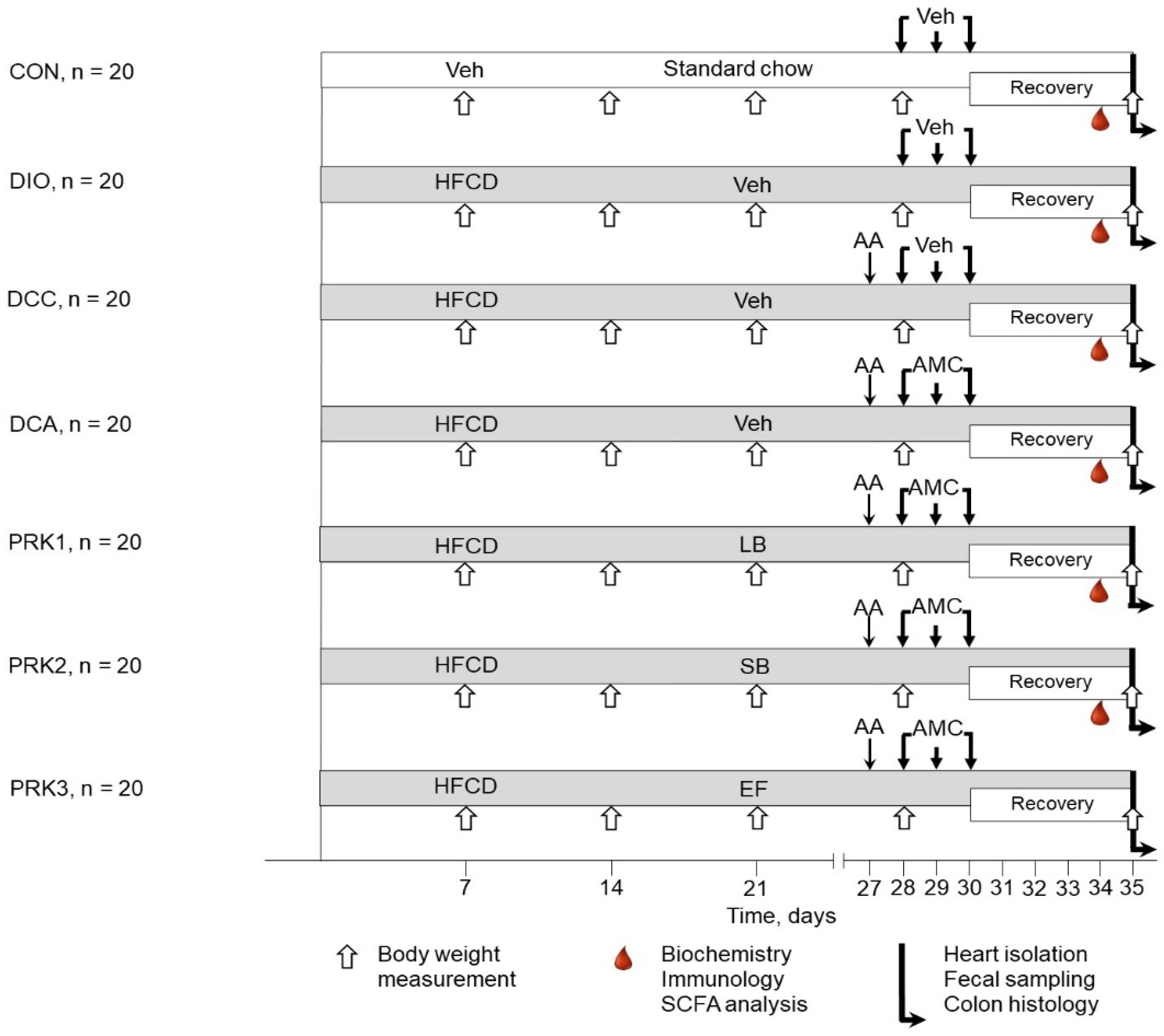
2.6. Experimental Design
2.7. Assessment of Hematological, Biochemical, and Immunological Variables
2.8. Analysis of Gut Microbiota
2.9. Analysis of SCFAs
2.10. Histopathological Studies
2.11. Isolated Heart Perfusion and Infarct Size Measurement
2.12. Statistical Analysis
3. Results
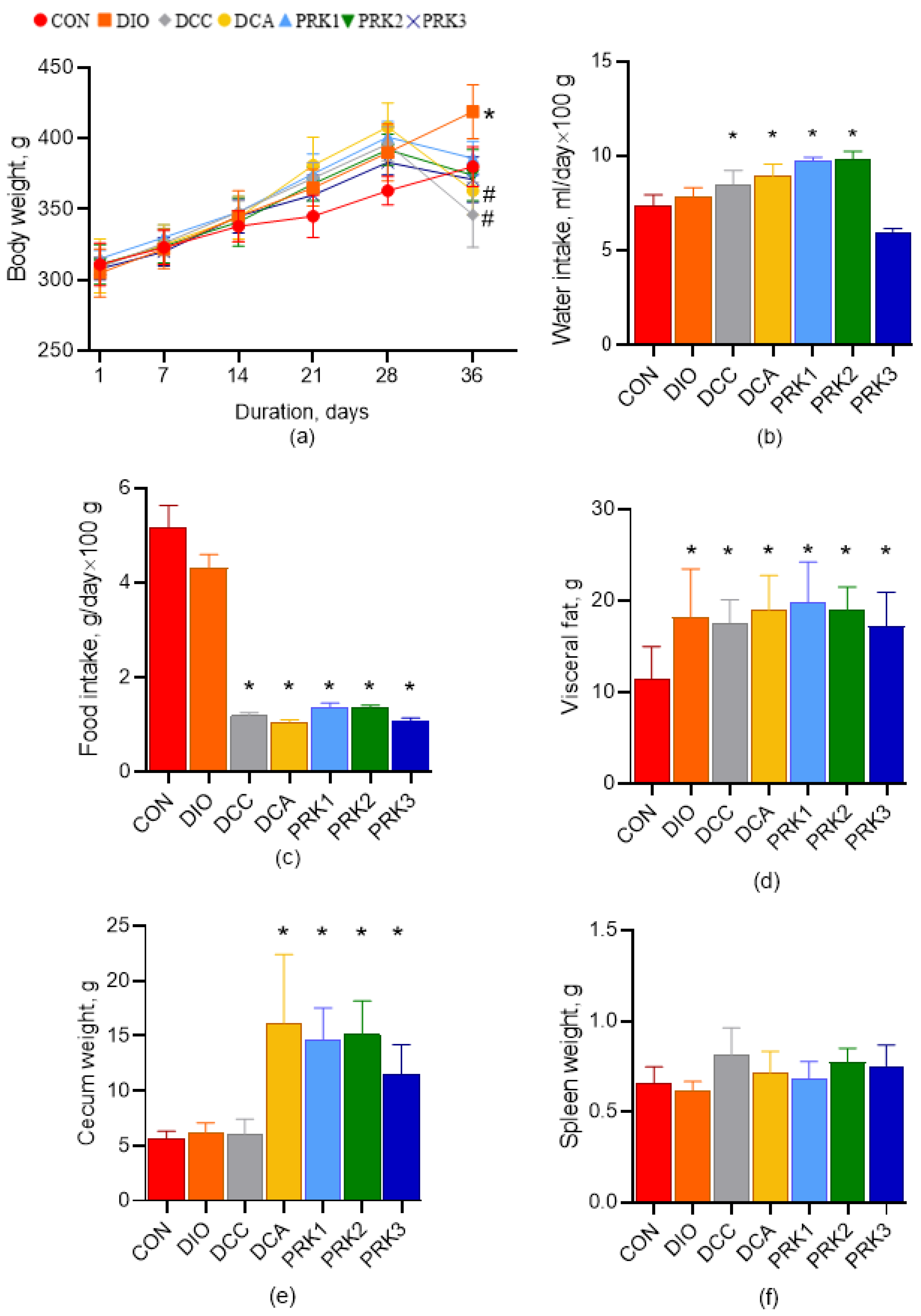
3.1. Animal Body Weight, Consumption of Water and Food, and Organ Weight
3.2. Hematological, Biochemical, and Immunological Parameters
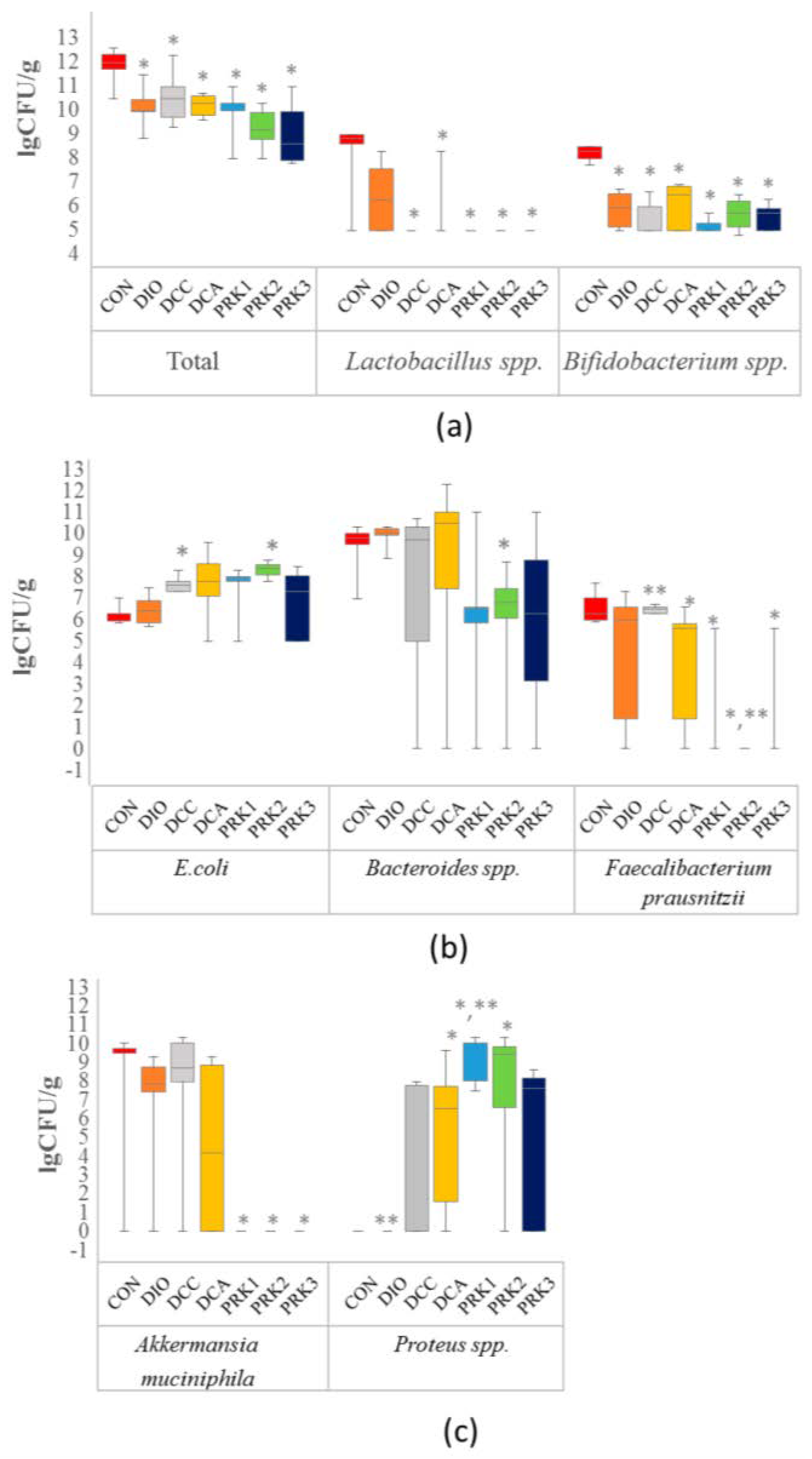
3.3. Alterations in Gut Microbiota
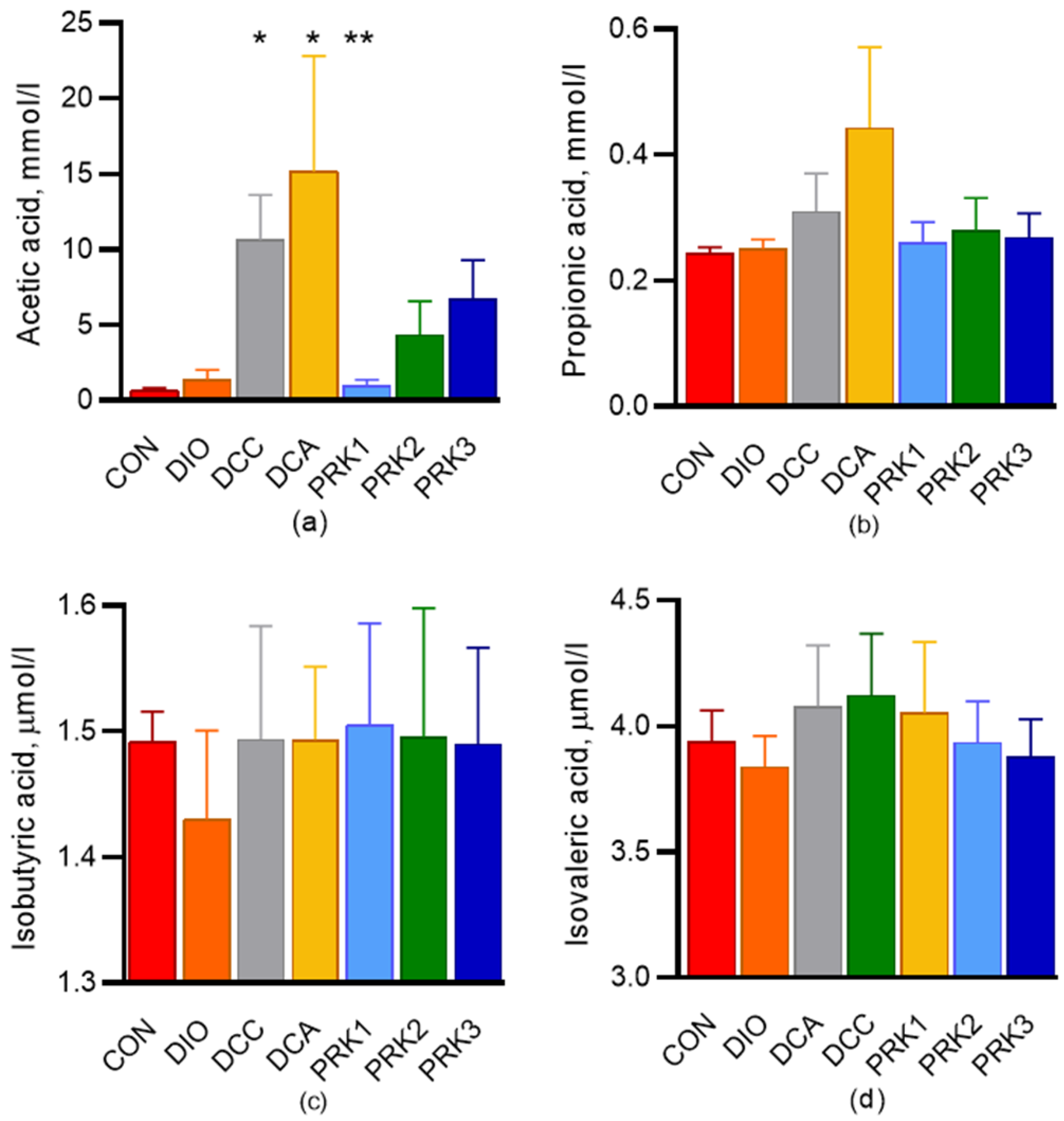
3.4. Short-Chain Fatty Acids
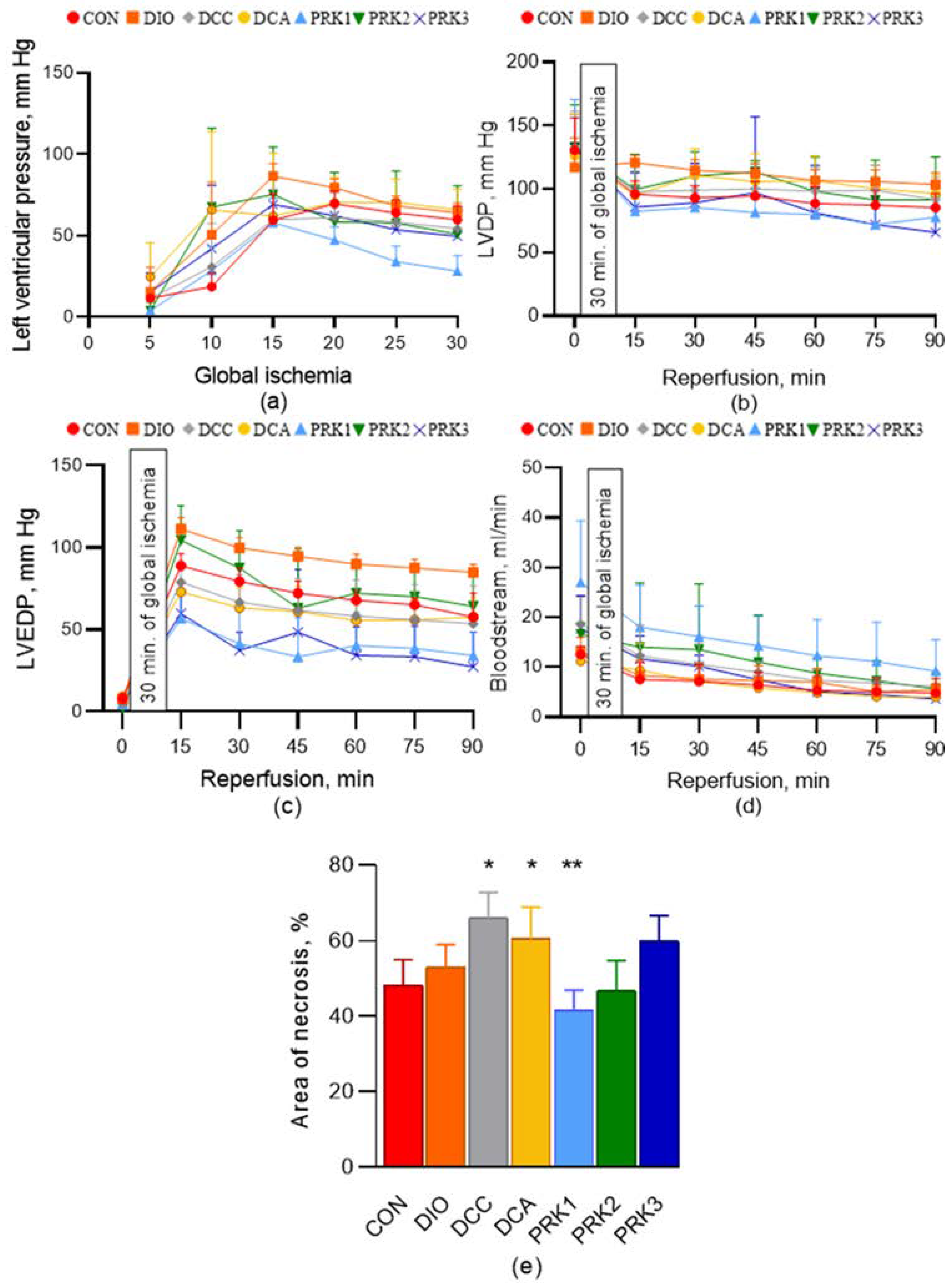
3.5. Hemodynamic Parameters of the Isolated Heart and Myocardial Infarct Size
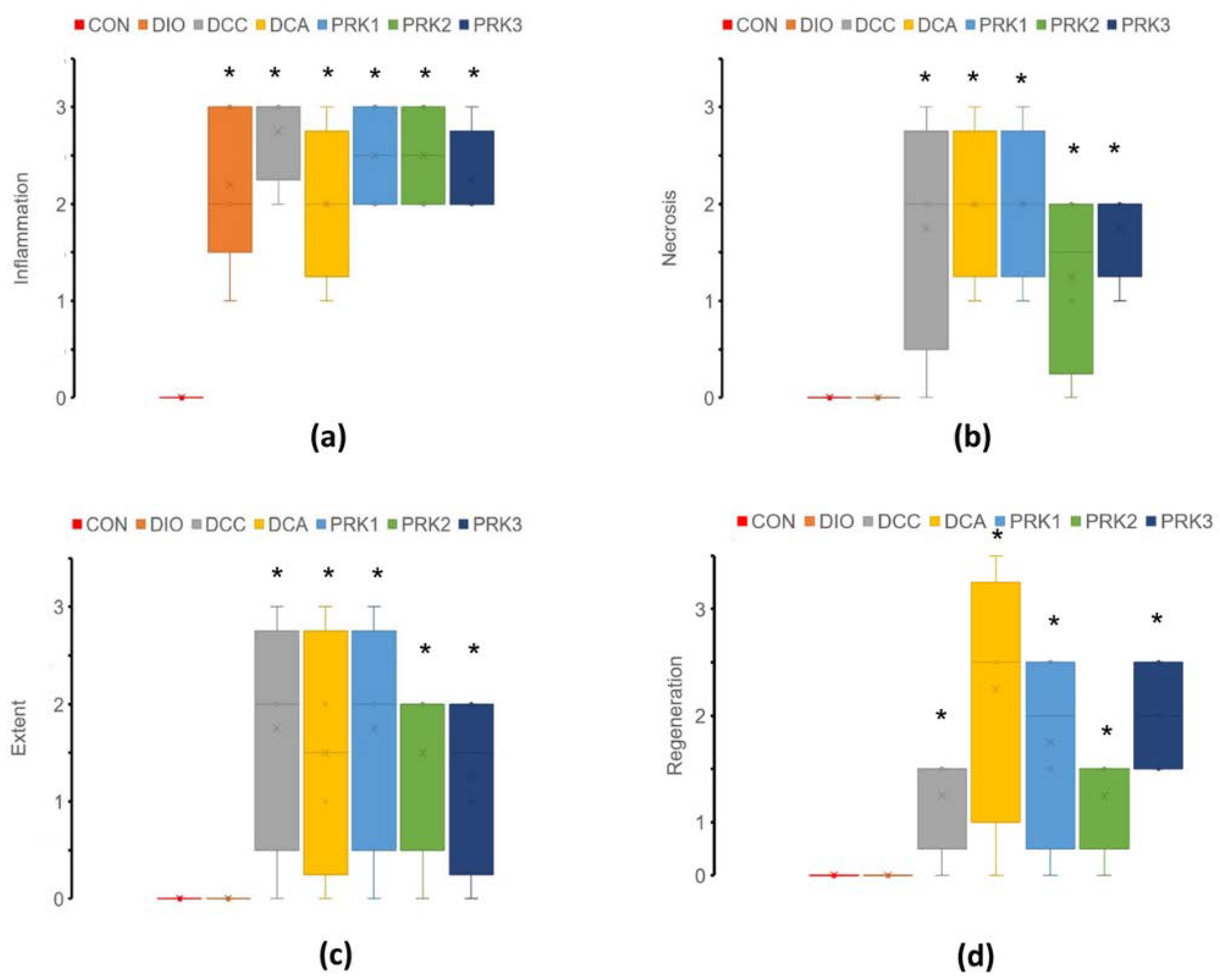
3.6. Histopathological Data
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Alonso, A.; Beaton, A.Z.; Bittencourt, M.S.; Boehme, A.K.; Buxton, A.E.; Carson, A.P.; Commodore-Mensah, Y.; et al. Heart Disease and Stroke Statistics-2022 Update: A Report From the American Heart Association. Circulation 2022, 145, e153–e639. [Google Scholar] [CrossRef] [PubMed]
- Miura, T.; Miki, T. Limitation of myocardial infarct size in the clinical setting: Current status and challenges in translating animal experiments into clinical therapy. Basic Res. Cardiol. 2008, 103, 501–513. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.M.; Islam, F.; Rashid, M.H.; Mamun, A.A.; Rahaman, M.S.; Islam, M.M.; Meem, A.F.K.; Sutradhar, P.R.; Mitra, S.; Mimi, A.A.; et al. The Gut Microbiota (Microbiome) in Cardiovascular Disease and Its Therapeutic Regulation. Front. Cell Infect. Microbiol. 2022, 12, 903570. [Google Scholar] [CrossRef] [PubMed]
- Lam, V.; Su, J.; Koprowski, S.; Hsu, A.; Tweddell, J.S.; Rafiee, P.; Gross, G.J.; Salzman, N.H.; Baker, J.E. Intestinal microbiota determine severity of myocardial infarction in rats. FASEB J. 2012, 26, 1727–1735. [Google Scholar] [CrossRef] [PubMed]
- Lam, V.; Su, J.; Hsu, A.; Gross, G.J.; Salzman, N.H.; Baker, J.E. Intestinal Microbial Metabolites Are Linked to Severity of Myocardial Infarction in Rats. PLoS ONE 2016, 11, e0160840. [Google Scholar] [CrossRef]
- Borshchev, Y.Y.; Minasian, S.M.; Burovenko, I.Y.; Borshchev, V.Y.; Protsak, E.S.; Semenova, N.Y.; Borshcheva, O.V.; Galagudza, M.M. Effects of tetracycline on myocardial infarct size in obese rats with chemically-induced colitis. PLoS ONE 2019, 14, e0225185. [Google Scholar] [CrossRef]
- Gan, X.T.; Ettinger, G.; Huang, C.X.; Burton, J.P.; Haist, J.V.; Rajapurohitam, V.; Sidaway, J.E.; Martin, G.; Gloor, G.B.; Swann, J.R.; et al. Probiotic administration attenuates myocardial hypertrophy and heart failure after myocardial infarction in the rat. Circ. Heart Fail. 2014, 7, 491–499. [Google Scholar] [CrossRef]
- Danilo, C.A.; Constantopoulos, E.; McKee, L.A.; Chen, H.; Regan, J.A.; Lipovka, Y.; Lahtinen, S.; Stenman, L.K.; Nguyen, T.V.V.; Doyle, K.P.; et al. Bifidobacterium animalis subsp. lactis 420 mitigates the pathological impact of myocardial infarction in the mouse. Benef. Microbes 2017, 8, 257–269. [Google Scholar] [CrossRef]
- Sadeghzadeh, J.; Vakili, A.; Sameni, H.R.; Shadnoush, M.; Bandegi, A.R.; Khorasani, M.Z. The Effect of Oral Consumption of Probiotics in Prevention of Heart Injury in a Rat Myocardial Infarction Model: A Histopathological, Hemodynamic and Biochemical Evaluation. Iran Biomed. J. 2017, 21, 174–181. [Google Scholar] [CrossRef]
- Liu, Z.; Liu, H.Y.; Zhou, H.; Zhan, Q.; Lai, W.; Zeng, Q.; Ren, H.; Xu, D. Moderate-Intensity Exercise Affects Gut Microbiome Composition and Influences Cardiac Function in Myocardial Infarction Mice. Front. Microbiol. 2017, 8, 1687. [Google Scholar] [CrossRef]
- Deng, F.; Zhang, L.Q.; Wu, H.; Chen, Y.; Yu, W.Q.; Han, R.H.; Han, Y.; Zhang, X.Q.; Sun, Q.S.; Lin, Z.B.; et al. Propionate alleviates myocardial ischemia-reperfusion injury aggravated by Angiotensin II dependent on caveolin-1/ACE2 axis through GPR41. Int. J. Biol. Sci. 2022, 18, 858–872. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Zhang, H.; Xie, R.; Wang, Y.; Ma, Y. Gut microbiota aggravate cardiac ischemia-reperfusion injury via regulating the formation of neutrophils extracellular traps. Life Sci. 2022, 303, 120670. [Google Scholar] [CrossRef] [PubMed]
- Ades, P.A.; Savage, P.D. Obesity in coronary heart disease: An unaddressed behavioral risk factor. Prev. Med. 2017, 104, 117–119. [Google Scholar] [CrossRef] [PubMed]
- Heusch, G. Critical Issues for the Translation of Cardioprotection. Circ. Res. 2017, 120, 1477–1486. [Google Scholar] [CrossRef]
- DeBoer, M.D. Obesity, systemic inflammation, and increased risk for cardiovascular disease and diabetes among adolescents: A need for screening tools to target interventions. Nutrition 2013, 29, 379–386. [Google Scholar] [CrossRef]
- Chen, Z.W.; Qian, J.Y.; Ma, J.Y.; Chang, S.F.; Yun, H.; Jin, H.; Sun, A.J.; Zou, Y.Z.; Ge, J.B. TNF-α-induced cardiomyocyte apoptosis contributes to cardiac dysfunction after coronary microembolization in mini-pigs. J. Cell Mol. Med. 2014, 18, 1953–1963. [Google Scholar] [CrossRef]
- Collins, K.H.; Hart, D.A.; Seerattan, R.A.; Reimer, R.A.; Herzog, W. High-fat/high-sucrose diet-induced obesity results in joint-specific development of osteoarthritis-like degeneration in a rat model. Bone Jt. Res. 2018, 7, 274–281. [Google Scholar] [CrossRef]
- El-Akabawy, G.; El-Sherif, N.M. Zeaxanthin exerts protective effects on acetic acid-induced colitis in rats via modulation of pro-inflammatory cytokines and oxidative stress. Biomed. Pharmacother. 2019, 111, 841–851. [Google Scholar] [CrossRef]
- Dieleman, L.A.; Palmen, M.J.; Akol, H.; Bloemena, E.; Peña, A.S.; Meuwissen, S.G.; Van Rees, E.P. Chronic experimental colitis induced by dextran sulphate sodium (DSS) is characterized by Th1 and Th2 cytokines. Clin. Exp. Immunol. 1998, 114, 385–391. [Google Scholar] [CrossRef]
- Minasian, S.M.; Galagudza, M.M.; Dmitriev, Y.V.; Kurapeev, D.I.; Vlasov, T.D. Myocardial protection against global ischemia with Krebs-Henseleit buffer-based cardioplegic solution. J. Cardiothorac. Surg. 2013, 8, 60. [Google Scholar] [CrossRef]
- Polyakova, E.A.; Mikhaylov, E.N.; Galagudza, M.M.; Shlyakhto, E.V. Hyperleptinemia results in systemic inflammation and the exacerbation of ischemia-reperfusion myocardial injury. Heliyon 2021, 7, e08491. [Google Scholar] [CrossRef] [PubMed]
- Sack, M.N.; Murphy, E. The role of comorbidities in cardioprotection. J. Cardiovasc. Pharmacol. Ther. 2011, 16, 267–272. [Google Scholar] [CrossRef] [PubMed]
- Hausenloy, D.J.; Garcia-Dorado, D.; Bøtker, H.E.; Davidson, S.M.; Downey, J.; Engel, F.B.; Jennings, R.; Lecour, S.; Leor, J.; Madonna, R.; et al. Novel targets and future strategies for acute cardioprotection: Position Paper of the European Society of Cardiology Working Group on Cellular Biology of the Heart. Cardiovasc. Res. 2017, 113, 564–585. [Google Scholar] [CrossRef] [PubMed]
- Meng, F.; Li, D.; Song, B.; Li, L. Impaired Myocardial MIF/AMPK Activation Aggravates Myocardial Ischemia Reperfusion Injury in High-Fat Diet-Induced Obesity. Endocr. Metab. Immune Disord. Drug Targets 2019, 19, 1046–1054. [Google Scholar] [CrossRef]
- Inserte, J.; Aluja, D.; Barba, I.; Ruiz-Meana, M.; Miró, E.; Poncelas, M.; Vilardosa, Ú.; Castellano, J.; Garcia-Dorado, D. High-fat diet improves tolerance to myocardial ischemia by delaying normalization of intracellular PH at reperfusion. J. Mol. Cell Cardiol. 2019, 133, 164–173. [Google Scholar] [CrossRef]
- Hanna, A.; Frangogiannis, N.G. Inflammatory Cytokines and Chemokines as Therapeutic Targets in Heart Failure. Cardiovasc. Drugs Ther. 2020, 34, 849–863. [Google Scholar] [CrossRef]
- Lin, J.; Li, Q.; Jin, T.; Wang, J.; Gong, Y.; Lv, Q.; Wang, M.; Chen, J.; Shang, M.; Zhao, Y.; et al. Cardiomyocyte IL-1R2 protects heart from ischemia/reperfusion injury by attenuating IL-17RA-mediated cardiomyocyte apoptosis. Cell Death Dis. 2022, 13, 90. [Google Scholar] [CrossRef]
- Belosjorow, S.; Bolle, I.; Duschin, A.; Heusch, G.; Schulz, R. TNF-alpha antibodies are as effective as ischemic preconditioning in reducing infarct size in rabbits. Am. J. Physiol. Heart Circ. Physiol. 2003, 284, H927–H930. [Google Scholar] [CrossRef]
- Carbone, A.M.; Borges, J.I.; Suster, M.S.; Sizova, A.; Cora, N.; Desimine, V.L.; Lymperopoulos, A. Regulator of G-Protein Signaling-4 Attenuates Cardiac Adverse Remodeling and Neuronal Norepinephrine Release-Promoting Free Fatty Acid Receptor FFAR3 Signaling. Int. J. Mol. Sci. 2022, 23, 5803. [Google Scholar] [CrossRef]
- Wang, J.; Zhang, J.; Lin, X.; Wang, Y.; Wu, X.; Yang, F.; Gao, W.; Zhang, Y.; Sun, J.; Jiang, C.; et al. DCA-TGR5 signaling activation alleviates inflammatory response and improves cardiac function in myocardial infarction. J. Mol. Cell Cardiol. 2021, 151, 3–14. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CON | DIO | DCC | DCA | PRK1 | PRK2 | PRK3 | |
|---|---|---|---|---|---|---|---|
| WBC (×109/L) | 5.1 ± 0.7 | 5.5 ± 0.4 | 6.8 ± 1.3 | 7.1 ± 2.2 * | 5.2 ± 0.9 ** | 5.9 ± 1.9 | 8.8 ± 1.6 * |
| RBC (×1012/L) | 7.4 ± 0.5 | 7.1 ± 0.4 | 7.3 ± 0.6 | 7.5 ± 0.3 | 7.3 ± 0.3 | 7.1 ± 1.2 | 7.2 ± 1.1 |
| PLT (×109/L) | 475 ± 52 | 505 ± 66 | 598 ± 130 | 548 ± 212 | 557 ± 99 | 651 ± 95 * | 618 ± 108 * |
| CON | DIO | DCC | DCA | PRK1 | PRK2 | PRK3 | |
|---|---|---|---|---|---|---|---|
| Protein (g/L) | 64 ± 3 | 62 ± 6 | 61 ± 4 | 63 ± 2 | 64 ± 3 | 65 ± 3 | 63 ± 3 |
| TG (mg/dL) | 74 ± 31 | 79 ± 38 | 72 ± 35 | 76 ± 41 | 91 ± 37 | 84 ± 35 | 97 ± 45 |
| CHOL (mg/dL) | 71 ± 36 | 76 ± 49 | 71 ± 35 | 74 ± 38 | 76 ± 41 | 69 ± 39 | 72 ± 37 |
| BA (μM/L) | 12.1 ± 4.4 | 10.8 ± 3.9 | 1.6 ± 1.5 * | 1.8 ± 1.2 * | 10.9 ± 3.2 ** | 4.3 ± 3.5 * | 0.7 ± 0.3 * |
| LDL (mg/dL) | 26 ± 4 | 23 ± 6 | 24 ± 4 | 20 ± 4 | 26 ± 7 | 26 ± 8 | 23 ± 7 |
| HDL (mg/dL) | 49 ± 5 | 46 ± 7 | 39 ± 6 | 49 ± 2 | 46 ± 10 | 43 ± 5 | 41 ± 6 |
| Lactate (mg/dL) | 42 ± 7 | 46 ± 14 | 65 ± 10 * | 68 ± 14 * | 67 ± 10 * | 69 ± 9 * | 64 ± 5 * |
| LDH (U/L) | 623 ± 130 | 1027 ± 314 | 979 ± 387 | 1183 ± 223 * | 929 ± 395 | 1250 ± 264 * | 1022 ± 334 |
| ALP (U/L) | 21 ± 4 | 41 ± 10 * | 54 ± 13 * | 57 ± 14 * | 31 ± 9 ** | 27 ± 12 ** | 25 ± 6 ** |
| Urea (mg/dL) | 15 ± 1 | 16 ± 3 | 13 ± 2 | 11 ± 1 * | 12 ± 3 | 15 ± 2 ** | 11 ± 2 * |
| URA (μM/L) | 44 ± 10 | 88 ± 32 * | 84 ± 41 * | 76 ± 15 * | 81 ± 19 * | 78 ± 13 * | 85 ± 16 * |
| CRE (μM/L) | 8 ± 2 | 13 ± 3 | 11 ± 3 | 15 ± 4 * | 12 ± 2 | 11 ± 2 | 17 ± 3 * |
| CON | DIO | DCC | DCA | PRK1 | PRK2 | PRK3 | |
|---|---|---|---|---|---|---|---|
| IL–1β (pg/mL) | 51 ± 16 | 78 ± 29 | 99 ± 13 * | 76 ± 12 * | 45 ± 7 ** | 57 ± 10 ** | 56 ± 6 ** |
| TNF–α (pg/mL) | 19 ± 2 | 21 ± 5 | 21 ± 2 | 28 ± 3 * | 20 ± 2 ** | 18 ± 2 ** | 17 ± 2 ** |
| IL–2 (pg/mL) | 2.4 ± 0.2 | 4.3 ± 0.6 * | 6.7 ± 1.9 * | 6.1 ± 1.4 * | 2.9 ± 0.5 ** | 3.0 ± 0.7 ** | 3.9 ± 0.9 *,** |
| IL–8 (pg/mL) | 28 ± 6 | 48 ± 9 * | 72 ± 24 * | 62 ± 12 * | 32 ± 14 ** | 61 ± 28 | 25 ± 4 ** |
| BDNF (ng/mL) | 6 ± 2 | 7 ± 2 | 12 ± 4 * | 9 ± 2 * | 6 ± 2 ** | 7 ± 3 | 9 ± 3 * |
| TGF–β (ng/mL) | 5 ± 2 | 7 ± 4 | 9 ± 3 * | 12 ± 3 * | 8 ± 4 | 16 ± 7 * | 4 ± 2 ** |
| IL–10 (pg/mL) | 19 ± 2 | 23 ± 3 | 22 ± 3 | 18 ± 2 | 23 ± 2 | 19 ± 3 | 19 ± 3 |
| LPS (ng/mL) | 6 ± 2 | 11 ± 2 * | 78 ± 10 * | 32 ± 8 * | 11 ± 5 ** | 36 ± 7 * | 29 ± 2 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borshchev, Y.Y.; Burovenko, I.Y.; Karaseva, A.B.; Minasian, S.M.; Protsak, E.S.; Borshchev, V.Y.; Semenova, N.Y.; Borshcheva, O.V.; Suvorov, A.N.; Galagudza, M.M. Probiotic Therapy with Lactobacillus acidophilus and Bifidobacterium animalis subsp. lactis Results in Infarct Size Limitation in Rats with Obesity and Chemically Induced Colitis. Microorganisms 2022, 10, 2293. https://doi.org/10.3390/microorganisms10112293
Borshchev YY, Burovenko IY, Karaseva AB, Minasian SM, Protsak ES, Borshchev VY, Semenova NY, Borshcheva OV, Suvorov AN, Galagudza MM. Probiotic Therapy with Lactobacillus acidophilus and Bifidobacterium animalis subsp. lactis Results in Infarct Size Limitation in Rats with Obesity and Chemically Induced Colitis. Microorganisms. 2022; 10(11):2293. https://doi.org/10.3390/microorganisms10112293
Chicago/Turabian StyleBorshchev, Yury Y., Inessa Y. Burovenko, Alena B. Karaseva, Sarkis M. Minasian, Egor S. Protsak, Victor Y. Borshchev, Natalia Y. Semenova, Olga V. Borshcheva, Alexander N. Suvorov, and Michael M. Galagudza. 2022. "Probiotic Therapy with Lactobacillus acidophilus and Bifidobacterium animalis subsp. lactis Results in Infarct Size Limitation in Rats with Obesity and Chemically Induced Colitis" Microorganisms 10, no. 11: 2293. https://doi.org/10.3390/microorganisms10112293
APA StyleBorshchev, Y. Y., Burovenko, I. Y., Karaseva, A. B., Minasian, S. M., Protsak, E. S., Borshchev, V. Y., Semenova, N. Y., Borshcheva, O. V., Suvorov, A. N., & Galagudza, M. M. (2022). Probiotic Therapy with Lactobacillus acidophilus and Bifidobacterium animalis subsp. lactis Results in Infarct Size Limitation in Rats with Obesity and Chemically Induced Colitis. Microorganisms, 10(11), 2293. https://doi.org/10.3390/microorganisms10112293