
Impact of Latent Virus Infection in the Cornea on Corneal Healing after Small Incision Lenticule Extraction
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Examinations
2.5. Surgical Procedures
2.6. Virus Detection
2.7. Postoperative Examinations
2.8. Corneal Confocal Microscopy
2.9. Statistical Analysis
3. Results
3.1. Results
3.1.1. General Results
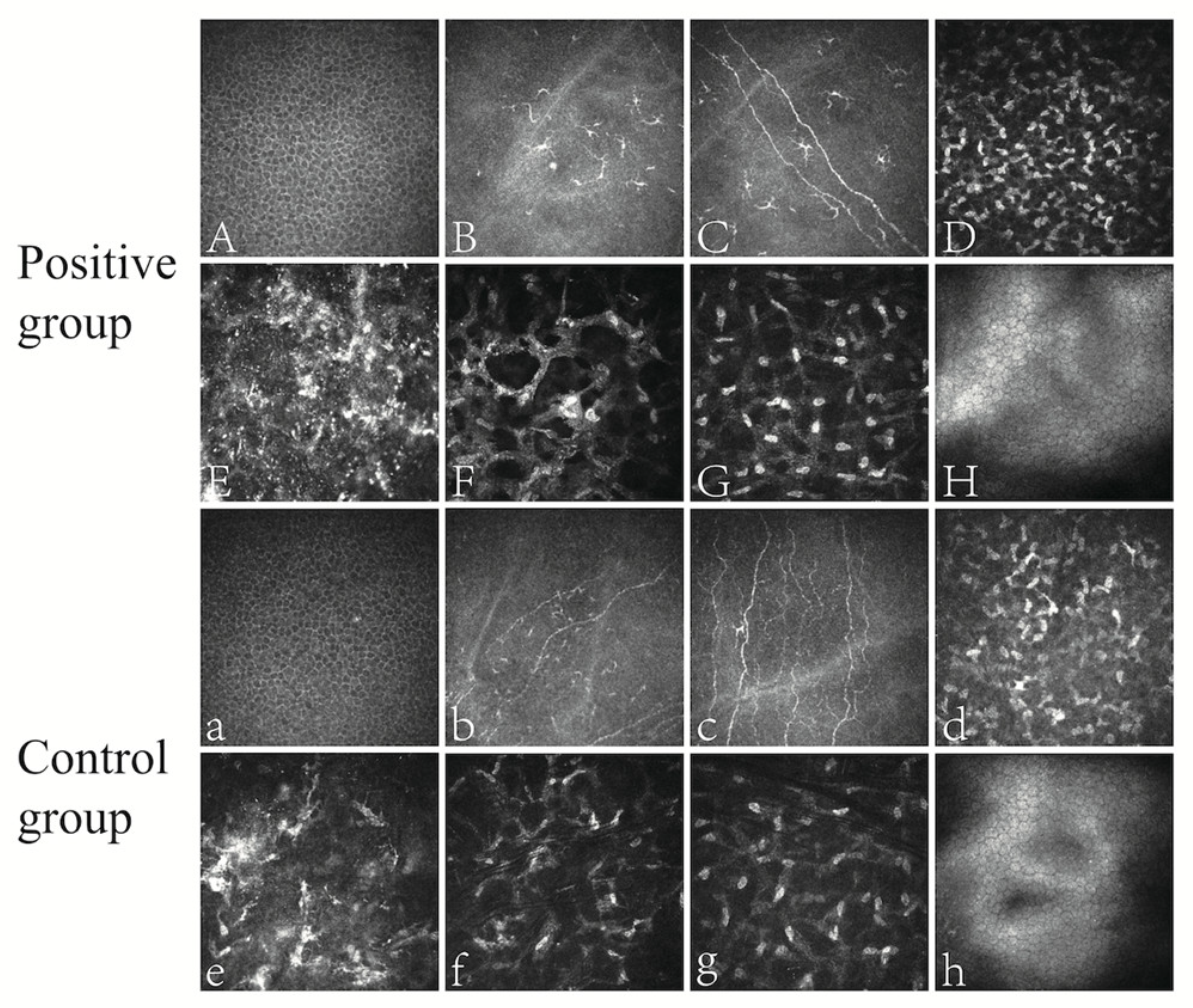
3.1.2. Corneal Confocal Microscopy Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Austin, A.; Lietman, T.; Rose-Nussbaumer, J. Update on the management of infectious keratitis. Ophthalmology 2017, 124, 1678–1689. [Google Scholar] [CrossRef] [PubMed]
- Koganti, R.; Yadavalli, T.; Naqvi, R.A.; Shukla, D.; Naqvi, A.R. Pathobiology and treatment of viral keratitis. Exp. Eye Res. 2021, 205, 108483. [Google Scholar] [CrossRef] [PubMed]
- Farooq, A.V.; Shukla, D. Corneal latency and transmission of herpes simplex virus-1. Future Virol. 2011, 6, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Chen, Y.; Wang, D.; Zhou, Y.; Zhang, X.; He, J.; Zhang, T.; Sun, Y.; Liu, Q. Clinical outcomes after SMILE and femtosecond laser-assisted LASIK for myopia and myopic astigmatism: A prospective randomized comparative study. Cornea 2016, 35, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Kunert, K.S.; Melle, J.; Sekundo, W.; Dawczynski, J.; Blum, M. One-year results of small incision lenticule extraction (SMILE) in myopia. Klin. Monbl. Augenheilkd. 2015, 232, 67–71. [Google Scholar] [CrossRef] [PubMed]
- Moshirfar, M.; Milner, D.C.; Baker, P.A.; McCabe, S.E.; Ronquillo, Y.C.; Hoopes, P.C. Corneal refractive surgery in patients with a history of herpes simplex keratitis: A narrative review. Clin. Ophthalmol. 2020, 14, 3891–3901. [Google Scholar] [CrossRef] [PubMed]
- Arora, T.; Sharma, N.; Arora, S.; Titiyal, J.S. Fulminant herpetic keratouveitis with flap necrosis following laser in situ keratomileusis: Case report and review of literature. J. Cataract Refract. Surg. 2014, 40, 2152–2156. [Google Scholar] [CrossRef]
- Ramirez-Miranda, A.; Mangwani-Mordani, S.; Quiroz-Casian, N.; Oliva-Bienzobas, V.; Cabral-Macias, J.; Navas, A.; Graue-Hernandez, E.O. Combined bacterial and herpes simplex virus keratitis following small-incision lenticule extraction for the correction of myopia. Case Rep. Ophthalmol. 2021, 12, 227–231. [Google Scholar] [CrossRef]
- Krueger, R.R.; Meister, C.S. A review of small incision lenticule extraction complications. Curr. Opin. Ophthalmol. 2018, 29, 292–298. [Google Scholar] [CrossRef]
- Hou, C.; Li, J.; Li, J.; Peng, H.; Wang, Q. In vivo confocal microscopy of sub-basal corneal nerves and corneal densitometry after three kinds of refractive procedures for high myopia. Int. Ophthalmol. 2022, 43, 925–935. [Google Scholar] [CrossRef]
- Yokogawa, H.; Kobayashi, A.; Tagawa, K.; Sugiyama, K. In vivo laser confocal microscopic analysis of corneal K-structures after keratorefractive surgery (LASIK and epi-LASIK). Ophthalmic Surg. Lasers Imaging 2010, 41, 494–498. [Google Scholar] [CrossRef]
- Goodrum, F. The complex biology of human cytomegalovirus latency. Adv. Virus Res. 2022, 112, 31–85. [Google Scholar] [CrossRef] [PubMed]
- Hill, J.M.; Ball, M.J.; Neumann, D.M.; Azcuy, A.M.; Bhattacharjee, P.S.; Bouhanik, S.; Clement, C.; Lukiw, W.J.; Foster, T.P.; Kumar, M.; et al. The high prevalence of herpes simplex virus type 1 DNA in human trigeminal ganglia is not a function of age or gender. J. Virol. 2008, 82, 8230–8234. [Google Scholar] [CrossRef] [PubMed]
- Matundan, H.; Ghiasi, H. Herpes simplex virus 1 ICP22 suppresses CD80 expression by murine dendritic cells. J. Virol. 2019, 93, e01803-18. [Google Scholar] [CrossRef] [PubMed]
- Tormanen, K.; Wang, S.; Ghiasi, H. CD80 plays a critical role in increased inflammatory responses in herpes simplex virus 1-infected mouse corneas. J. Virol. 2020, 94, e01511-19. [Google Scholar] [CrossRef] [PubMed]
- Kurt-Jones, E.A.; Orzalli, M.H.; Knipe, D.M. Innate immune mechanisms and herpes simplex virus infection and disease. Adv. Anat. Embryol. Cell Biol. 2017, 223, 49–75. [Google Scholar] [CrossRef] [PubMed]
- Young, R.C.; Hodge, D.O.; Liesegang, T.J.; Baratz, K.H. Incidence, recurrence, and outcomes of herpes simplex virus eye disease in Olmsted County, Minnesota, 1976–2007: The effect of oral antiviral prophylaxis. Arch. Ophthalmol. 2010, 128, 1178–1183. [Google Scholar] [CrossRef] [PubMed]
- Santra, M.; Liu, Y.C.; Jhanji, V.; Yam, G.H.F. Human SMILE-derived stromal lenticule scaffold for regenerative therapy: Review and perspectives. Int. J. Mol. Sci. 2022, 23, 7967. [Google Scholar] [CrossRef]
- Jiang, Y.; Li, Y.; Liu, X.W.; Xu, J. A novel tectonic keratoplasty with femtosecond laser intrastromal lenticule for corneal ulcer and perforation. Chin. Med. J. 2016, 129, 1817–1821. [Google Scholar] [CrossRef]
- Qu, J.-H.; Peng, R.-M.; Xiao, G.-G.; Qu, H.-Q.; Yu, T.; Zhang, S.; Hong, J. The incidence and influence of the donor corneas positive for herpesviridae DNA in keratoplasty. Graefes Arch. Clin. Exp. Ophthalmol. 2020, 258, 2767–2774. [Google Scholar] [CrossRef]
- Shang, Y.; Li, Y.; Wang, Z.; Sun, X.; Zhang, F. Risk evaluation of human corneal stromal lenticules from SMILE for reuse. J. Refract. Surg. 2021, 37, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Solomon, R.; Donnenfeld, E.D.; Holland, E.J.; Yoo, S.H.; Daya, S.; Güell, J.L.; Mah, F.S.; Scoper, S.V.; Kim, T. Microbial keratitis trends following refractive surgery: Results of the ASCRS infectious keratitis survey and comparisons with prior ASCRS surveys of infectious keratitis following keratorefractive procedures. J. Cataract Refract. Surg. 2011, 37, 1343–1350. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.K.; Chen, K.H.; Lee, S.M.; Hsu, W.M.; Lai, J.Y.; Li, Y.S. Herpes simplex keratitis following excimer laser application. J. Refract. Surg. 2006, 22, 509–511. [Google Scholar] [CrossRef]
- Dhaliwal, D.K.; Romanowski, E.G.; Yates, K.A.; Hu, D.; Goldstein, M.; Gordon, Y.J. Experimental laser-assisted in situ keratomileusis induces the reactivation of latent herpes simplex virus. Am. J. Ophthalmol. 2001, 131, 506–507. [Google Scholar] [CrossRef] [PubMed]
- Levy, J.; Lapid-Gortzak, R.; Klemperer, I.; Lifshitz, T. Herpes simplex virus keratitis after laser in situ keratomileusis. J. Refract. Surg. 2005, 21, 400–402. [Google Scholar] [CrossRef] [PubMed]
- Brennan, D.C.; Aguado, J.M.; Potena, L.; Jardine, A.G.; Legendre, C.; Säemann, M.D.; Mueller, N.J.; Merville, P.; Emery, V.; Nashan, B. Effect of maintenance immunosuppressive drugs on virus pathobiology: Evidence and potential mechanisms. Rev. Med. Virol. 2013, 23, 97–125. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Ma, J.; Zhang, L.; Zou, H.; Li, J.; Zhang, Y.; Jhanji, V. Postoperative corneal complications in small incision lenticule extraction: Long-term study. J. Refract. Surg. 2019, 35, 146–152. [Google Scholar] [CrossRef]
- Chehaibou, I.; Sandali, O.; Ameline, B.; Bouheraoua, N.; Borderie, V.; Laroche, L. Bilateral infectious keratitis after small-incision lenticule extraction. J. Cataract Refract. Surg. 2016, 42, 626–630. [Google Scholar] [CrossRef]
- Dupps, W.J.; Wilson, S.E. Biomechanics and wound healing in the cornea. Exp. Eye Res. 2006, 83, 709–720. [Google Scholar] [CrossRef]
- Dong, Z.; Zhou, X.; Wu, J.; Zhang, Z.; Li, T.; Zhou, Z.; Zhang, S.; Li, G. Small incision lenticule extraction (SMILE) and femtosecond laser LASIK: Comparison of corneal wound healing and inflammation. Br. J. Ophthalmol. 2014, 98, 263–269. [Google Scholar] [CrossRef]
- Liu, Y.C.; Teo, E.P.W.; Lwin, N.C.; Yam, G.H.F.; Mehta, J.S. Early corneal wound healing and inflammatory responses after SMILE: Comparison of the effects of different refractive corrections and surgical experiences. J. Refract. Surg. 2016, 32, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Erie, J.C.; McLaren, J.W.; Patel, S.V. Confocal microscopy in ophthalmology. Am. J. Ophthalmol. 2009, 148, 639–646. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Liu, L.; Shi, Y.; Sun, L.; Ma, X.; Zou, J. Age-related differences in corneal nerve regeneration after SMILE and the mechanism revealed by metabolomics. Exp. Eye Res. 2021, 209, 108665. [Google Scholar] [CrossRef] [PubMed]
- Zheng, T.; Le, Q.; Hong, J.; Xu, J. Comparison of human corneal cell density by age and corneal location: An in vivo confocal microscopy study. BMC Ophthalmol. 2016, 16, 109. [Google Scholar] [CrossRef] [PubMed]
- Lum, E.; Corbett, M.C.; Murphy, P.J. Corneal sensitivity after ocular surgery. Eye Contact Lens. 2019, 45, 226–237. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.C.; Jung, A.S.J.; Chin, J.Y.; Yang, L.W.Y.; Mehta, J.S. Cross-sectional study on corneal denervation in contralateral eyes following SMILE versus LASIK. J. Refract. Surg. 2020, 36, 653–660. [Google Scholar] [CrossRef]
- Recchioni, A.M.; Sisó-Fuertes, I.; Hartwig, A.; Hamid, A.B.; Shortt, A.J.M.; Morris, R.M.; Vaswani, S.B.; Dermott, J.D.B.; Cerviño, A.; Wolffsohn, J.S.; et al. Short-term impact of FS-LASIK and SMILE on dry eye metrics and corneal nerve morphology. Cornea 2020, 39, 851–857. [Google Scholar] [CrossRef]

{kind=link}
| General Condition | Positive Group (n = 21) | Control Group (n = 449) | p Value |
|---|---|---|---|
| Gender (male/female) | 6/5 | 162/67 | 0.3129 |
| Age (years) | 21.73 ± 2.05 | 22.99 ± 4.79 | 0.9110 |
| Preoperative spherical equivalent (D) | −5.67 ± 1.37 | −4.98 ± 1.64 | 0.0504 |
| Preoperative corrected visual acuity | 0.01 ± 0.06 | −0.01 ± 0.07 | 0.1152 |
| Preoperative corneal curvature, Kf (D) | 42.46 ± 0.68 | 42.06 ± 1.19 | 0.1307 |
| Preoperative corneal curvature, Ks (D) | 43.84 ± 0.75 | 43.28 ± 1.35 | 0.0598 |
| Preoperative corneal thickness (μm) | 547.43 ± 16.36 | 548.34 ± 24.59 | 0.8447 |
| Preoperative intraocular pressure (mmHg) | 18.37 ± 2.27 | 18.20 ± 2.28 | 0.9283 |
| Axial length (mm) | 25.46 ± 1.01 | 25.67 ± 0.91 | 0.3116 |
| Optical zone diameter (mm) | 6.68 ± 0.17 | 6.72 ± 0.14 | 0.3657 |
| Lenticule depth (μm) | 124.14 ± 20.89 | 116.41 ± 23.57 | 0.1405 |
| Residual corneal thickness (μm) | 305.67 ± 24.10 | 312.61 ± 26.34 | 0.2033 |
| Added refractive value (D) | 0.83 ± 0.14 | 0.81 ± 0.14 | 0.4182 |
| Postoperative Examination Results | Positive Group (n = 21) | Control Group (n = 449) | p Value |
|---|---|---|---|
| Postoperative uncorrected visual acuity | −0.02 ± 0.07 | 0.01 ± 0.09 | 0.0798 |
| Postoperative spherical equivalent (D) | −0.07 ± 0.45 | −0.11 ± 0.52 | 0.9502 |
| Postoperative intraocular pressure (mmHg) | 13.61 ± 0.96 | 13.19 ± 1.93 | 0.2793 |
| Postoperative corneal curvature Kf (D) | 37.95 ± 1.14 | 38.13 ± 1.71 | 0.6203 |
| Postoperative corneal curvature Ks (D) | 38.73 ± 1.21 | 38.84 ± 1.81 | 0.7865 |
| Postoperative corneal thickness (μm) | 435.57 ± 27.72 | 444.97 ± 29.15 | 0.0763 |
| Corneal transparency (edema/transparency) | 1/20 | 15/434 | 0.5246 |
| Corneal staining (with/without staining) | 0/21 | 5/444 | >0.9999 |
| Positive Group (n = 21) | Control Group (n = 15) | p Value | |
|---|---|---|---|
| Stromal cells number | 70.65 ± 30.97 | 63.71 ± 20.77 | 0.5536 |
| Inflammatory cells number (<5/5–10/>10) | 10/5/6 | 9/2/4 | 0.6841 |
| CNFD (/mm2) | 6.96 ± 8.01 | 6.53 ± 6.66 | 0.9306 |
| CNBD (/mm2) | 4.64 ± 7.75 | 7.22 ± 11.99 | 0.4036 |
| CNFL (mm/mm2) | 7.01 ± 3.52 | 8.03 ± 3.15 | 0.0622 |
| CTBD (/mm2) | 15.32 ± 14.48 | 18.33 ± 17.85 | 0.5062 |
| CNFW (mm) | 0.0239 ± 0.0032 | 0.0229 ± 0.0026 | 0.2346 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, M.; Song, W.; Gao, W.; Jiang, L.; Pan, H.; Luo, D.; Shi, L. Impact of Latent Virus Infection in the Cornea on Corneal Healing after Small Incision Lenticule Extraction. Microorganisms 2023, 11, 2441. https://doi.org/10.3390/microorganisms11102441
Liu M, Song W, Gao W, Jiang L, Pan H, Luo D, Shi L. Impact of Latent Virus Infection in the Cornea on Corneal Healing after Small Incision Lenticule Extraction. Microorganisms. 2023; 11(10):2441. https://doi.org/10.3390/microorganisms11102441
Chicago/Turabian StyleLiu, Ming, Wenting Song, Wen Gao, Lili Jiang, Hongbiao Pan, Dan Luo, and Lei Shi. 2023. "Impact of Latent Virus Infection in the Cornea on Corneal Healing after Small Incision Lenticule Extraction" Microorganisms 11, no. 10: 2441. https://doi.org/10.3390/microorganisms11102441