
The Association between Gestational Diabetes Mellitus and Infections in Pregnancy—Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria, Information Sources, and Search Strategy
2.2. Data Extraction
2.3. Outcomes
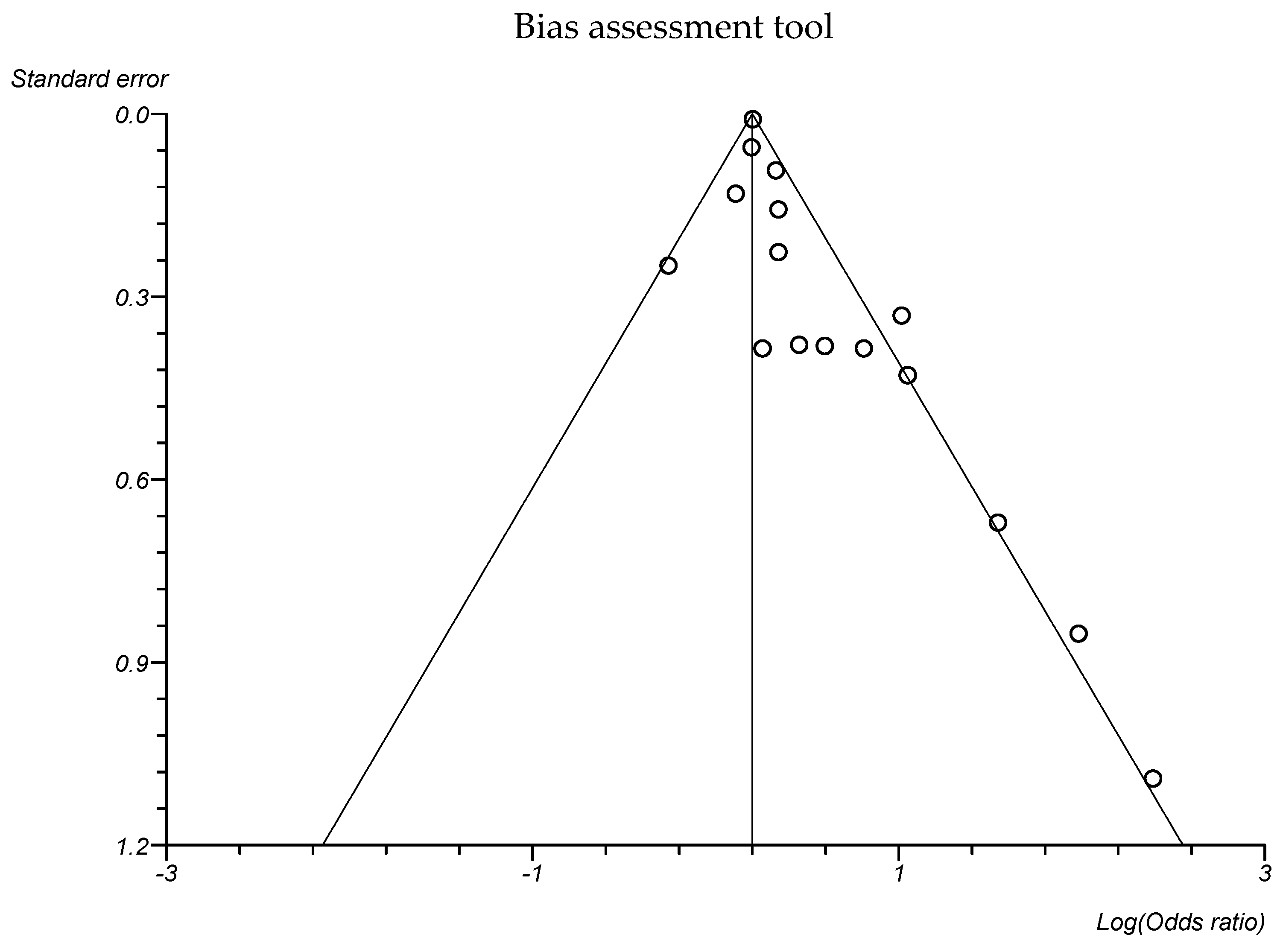
2.4. Data Synthesis and Assessment of the Risk of Bias
3. Results
3.1. General Features
3.2. Association between Gestational Diabetes Mellitus and Infections
3.3. Association between Gestational Diabetes Mellitus and Type of Infection Site
3.4. Association between Gestational Diabetes Mellitus and Type of Pathogens
3.5. Association between Gestational Diabetes Mellitus and Diagnostic Criteria
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lawrence, J.M.; Contreras, R.; Chen, W.; Sacks, D.A. Trends in the Prevalence of Preexisting Diabetes and Gestational Diabetes Mellitus Among a Racially/Ethnically Diverse Population of Pregnant Women, 1999–2005. Diabetes Care 2008, 31, 899–904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wier, L.M.; Witt, E.; Burgess, J.; Elixhauser, A. Hospitalizations Related to Diabetes in Pregnancy, 2008. In Healthcare Cost and Utilization Project (HCUP) Statistical Briefs [Internet]; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2006. [Google Scholar]
- DeSisto, C.L.; Kim, S.Y.; Sharma, A.J. Prevalence Estimates of Gestational Diabetes Mellitus in the United States, Pregnancy Risk Assessment Monitoring System (PRAMS), 2007–2010. Prev. Chronic. Dis. 2014, 11, 130415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiefari, E.; Arcidiacono, B.; Foti, D.; Brunetti, A. Gestational diabetes mellitus: An updated overview. J. Endocrinol. Investig. 2017, 40, 899–909. [Google Scholar] [CrossRef]
- Varner, M.W.; Rice, M.M.; Landon, M.B.; Casey, B.M.; Reddy, U.M.; Wapner, R.J.; Rouse, D.J.; Tita, A.T.N.; Thorp, J.M.; Chien, E.K.M.; et al. Pregnancies After the Diagnosis of Mild Gestational Diabetes Mellitus and Risk of Cardiometabolic Disorders. Obstet. Gynecol. 2017, 129, 273–280. [Google Scholar] [CrossRef]
- Waters, T.P.; Dyer, A.R.; Scholtens, D.M.; Dooley, S.L.; Herer, E.; Lowe, L.P.; Oats, J.J.; Persson, B.; Sacks, D.A.; Metzger, B.E.; et al. Maternal and Neonatal Morbidity for Women Who Would Be Added to the Diagnosis of GDM Using IADPSG Criteria: A Secondary Analysis of the Hyperglycemia and Adverse Pregnancy Outcome Study. Diabetes Care 2016, 39, 2204–2210. [Google Scholar] [CrossRef] [Green Version]
- Sacks, D.A.; Black, M.H.; Li, X.; Montoro, M.N.; Lawrence, J.M. Adverse Pregnancy Outcomes Using the International Association of the Diabetes and Pregnancy Study Groups Criteria. Obstet. Gynecol. 2015, 126, 67–73. [Google Scholar] [CrossRef] [Green Version]
- Metzger, B.E.; Buchanan, T.A.; Coustan, D.R.; de Leiva, A.; Dunger, D.B.; Hadden, D.R.; Hod, M.; Kitzmiller, J.L.; Kjos, S.L.; Oats, J.N.; et al. Summary and Recommendations of the Fifth International Workshop-Conference on Gestational Diabetes Mellitus. Diabetes Care 2007, 30 (Suppl. 2), S251–S260. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Liao, Q.; Wang, F.; Li, D. Association of gestational diabetes mellitus and abnormal vaginal flora with adverse pregnancy outcomes. Medicine 2018, 97, e11891. [Google Scholar] [CrossRef]
- Xiong, X.; Saunders, L.D.; Wang, F.L.; Demianczuk, N.N. Gestational diabetes mellitus: Prevalence, risk factors, maternal and infant outcomes. Int. J. Gynaecol. Obstet. 2001, 75, 221–228. [Google Scholar] [CrossRef]
- Committee on Practice Bulletins—Obstetrics. ACOG Practice Bulletin No. 190 Summary: Gestational Diabetes Mellitus. Obstet. Gynecol. 2018, 131, 406–408. [Google Scholar] [CrossRef]
- Roeckner, J.T.; Sanchez-Ramos, L.; Jijon-Knupp, R.; Kaunitz, A.M. Single abnormal value on 3-hour oral glucose tolerance test during pregnancy is associated with adverse maternal and neonatal outcomes: A systematic review and metaanalysis. Am. J. Obstet. Gynecol. 2016, 215, 287–297. [Google Scholar] [CrossRef]
- Committee on Practice Bulletins—Obstetrics. Practice Bulletin No. 180 Summary: Gestational Diabetes Mellitus. Obstet. Gynecol. 2017, 130, 244–246. [Google Scholar] [CrossRef]
- Langer, O.; Brustman, L.; Anyaegbunam, A.; Mazze, R. The significance of one abnormal glucose tolerance test value on adverse outcome in pregnancy. Am. J. Obs. Gynecol. 1987, 157, 758–763. [Google Scholar] [CrossRef] [PubMed]
- Mannan, M.; Rahman, M.; Ara, I.; Afroz, H. Prevalence and Pregnancy Outcome of Gestational Diabetes Mellitus Among Bangladeshi Urban Pregnant Women. J. Med. 2012, 13, 147–151. [Google Scholar] [CrossRef]
- Khatun, N.; Latif, S.A.; Uddin, M.M. Pregnancy associated complications of mothers with gestational diabetes mellitus. Mymensingh Med. J. 2005, 14, 196–198. [Google Scholar] [PubMed]
- Mazziotti, F.; Arena, V.; Mastro, F.L.; La Torre, R.; Fallucca, F.; Di Biase, N.; Napoli, A. Diabetes and pregnancy: Prophylaxis of genital infections. Ann. Dell’istituto Super. Di Sanità 1997, 33, 343–345. [Google Scholar]
- Nowakowska, D.; Kurnatowska, A.; Stray-Pedersen, B.; Wilczyński, J. Activity of hydrolytic enzymes in fungi isolated from diabetic pregnant women: Is there any relationship between fungal alkaline and acid phosphatase activity and glycemic control? APMIS 2004, 112, 374–383. [Google Scholar] [CrossRef]
- Nugent, R.P.; Krohn, M.A.; Hillier, S.L. Reliability of diagnosing bacterial vaginosis is improved by a standardized method of gram stain interpretation. J. Clin. Microbiol. 1991, 29, 297–301. [Google Scholar] [CrossRef]
- Mirmonsef, P.; Hotton, A.L.; Gilbert, D.; Burgad, D.; Landay, A.; Weber, K.M.; Cohen, M.; Ravel, J.; Spear, G.T. Free glycogen in vaginal fluids is associated with Lactobacillus colonization and low vaginal pH. PLoS ONE 2014, 9, e102467. [Google Scholar] [CrossRef] [Green Version]
- Guggenheimer, J.; Moore, P.A.; Rossie, K.; Myers, D.; Mongelluzzo, M.B.; Block, H.M.; Weyant, R.; Orchard, T. Insulin-dependent diabetes mellitus and oral soft tissue pathologies. II. Prevalence and characteristics of Candida and candidal lesions. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endodontol. 2000, 89, 570–576. [Google Scholar] [CrossRef]
- Hirji, I.; Andersson, S.W.; Guo, Z.; Hammar, N.; Gomez-Caminero, A. Incidence of genital infection among patients with type 2 diabetes in the UK General Practice Research Database. J. Diabetes Complicat. 2012, 26, 501–505. [Google Scholar] [CrossRef] [PubMed]
- Rahman, T.; Khan, I.H.; Begum, J. High vaginal swab (HVS), routine microscopy and culture sensitivity in diabetic and non diabetic, a comparative retrospective study of five years. Indian J. Med. Sci. 1991, 45, 212–214. [Google Scholar]
- Nowakowska, D.; Kurnatowska, A.; Stray-Pedersen, B.; Wilczynski, J. Prevalence of fungi in the vagina, rectum and oral cavity in pregnant diabetic women: Relation to gestational age and symptoms. Acta Obstet. Gynecol. Scand. 2004, 83, 251–256. [Google Scholar] [CrossRef]
- Gonçalves, B.; Ferreira, C.; Alves, C.T.; Henriques, M.; Azeredo, J.; Silva, S. Vulvovaginal candidiasis: Epidemiology, microbiology and risk factors. Crit. Rev. Microbiol. 2016, 42, 905–927. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leitich, H.; Bodner-Adler, B.; Brunbauer, M.; Kaider, A.; Egarter, C.; Husslein, P. Bacterial vaginosis as a risk factor for preterm delivery: A meta-analysis. Am. J. Obstet. Gynecol. 2003, 189, 139–147. [Google Scholar] [CrossRef] [PubMed]
- Goldenberg, R.L.; Culhane, J.F.; Iams, J.D.; Romero, R. Epidemiology and causes of preterm birth. Lancet 2008, 371, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Rizk, D.E.; Mustafa, N.; Thomas, L. The prevalence of urinary tract infections in patients with gestational diabetes mellitus. Int. Urogynecol. J. Pelvic Floor. Dysfunct. 2001, 12, 317–321. [Google Scholar] [CrossRef]
- Schneeberger, C.; Geerlings, S.E.; Erwich, J.J.H.; Heuvel, E.R.V.D.; Middleton, P.; Crowther, C.A. Asymptomatic Bacteriuria and Urinary Tract Infection in Pregnant Women with and without Diabetes Mellitus and Gestational Diabetes Mellitus—A Case-Control Study. J. Diabetes Mellit. 2017, 7, 184–194. [Google Scholar] [CrossRef]
- Schneeberger, C.; Erwich, J.J.H.M.; van den Heuvel, E.R.; Mol, B.W.J.; Ott, A.; Geerlings, S.E. Asymptomatic bacteriuria and urinary tract infection in pregnant women with and without diabetes: Cohort study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2018, 222, 176–181. [Google Scholar] [CrossRef]
- Stroup, D.F. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008. [Google Scholar] [CrossRef]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and Elaboration. PLoS Med. 2007, 4, e297. [Google Scholar] [CrossRef]
- GA Wells BSDOJPVWMLPT. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-analyses. Available online: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 10 July 2023).
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Vist, G.E.; Falck-Ytter, Y.; Schünemann, H.J. What is “quality of evidence” and why is it important to clinicians? BMJ 2008, 336, 995–998. [Google Scholar] [CrossRef] [Green Version]
- Eskenazi, B.; Rauch, S.; Iurlaro, E.; Gunier, R.B.; Rego, A.; Gravett, M.G.; Cavoretto, P.I.; Deruelle, P.; García-May, P.K.; Mhatre, M.; et al. Diabetes mellitus, maternal adiposity, and insulin-dependent gestational diabetes are associated with COVID-19 in pregnancy: The INTERCOVID study. Am. J. Obstet. Gynecol. 2022, 227, e1–e74. [Google Scholar] [CrossRef]
- Johnson, C.Y.; Rocheleau, C.M.; Howley, M.M.; Chiu, S.K.; Arnold, K.E.; Ailes, E.C. Characteristics of Women with Urinary Tract Infection in Pregnancy. J. Womens Health 2021, 30, 1556–1564. [Google Scholar] [CrossRef] [PubMed]
- Radan, A.-P.; Fluri, M.-M.; Nirgianakis, K.; Mosimann, B.; Schlatter, B.; Raio, L.; Surbek, D. Gestational diabetes is associated with SARS-CoV-2 infection during pregnancy: A case-control study. Diabetes Metab. 2022, 48, 101351. [Google Scholar] [CrossRef] [PubMed]
- Epelboin, S.; Labrosse, J.; De Mouzon, J.; Fauque, P.; Gervoise-Boyer, M.-J.; Levy, R.; Sermondade, N.; Hesters, L.; Bergère, M.; Devienne, C.; et al. Obstetrical outcomes and maternal morbidities associated with COVID-19 in pregnant women in France: A national retrospective cohort study. PLoS Med. 2021, 18, e1003857. [Google Scholar] [CrossRef] [PubMed]
- Lukic, A.; Napoli, A.; Santino, I.; Bianchi, P.; Nobili, F.; Ciampittiello, G.; Nardone, M.R.; Santomauro, M.; Di Properzio, M.; Caserta, D. Cervicovaginal bacteria and fungi in pregnant diabetic and non-diabetic women: A multicenter observational cohort study. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 2303–2315. [Google Scholar]
- Gogeneni, H.; Buduneli, N.; Ceyhan-Öztürk, B.; Gümüş, P.; Akcali, A.; Zeller, I.; Renaud, D.E.; Scott, D.A.; Özçaka, Ö. Increased infection with key periodontal pathogens during gestational diabetes mellitus. J. Clin. Periodontol. 2015, 42, 506–512. [Google Scholar] [CrossRef] [Green Version]
- Son, K.H.; Lim, N.-K.; Lee, J.-W.; Cho, M.-C.; Park, H.-Y. Comparison of maternal morbidity and medical costs during pregnancy and delivery between patients with gestational diabetes and patients with pre-existing diabetes. Diabet. Med. 2015, 32, 477–486. [Google Scholar] [CrossRef] [Green Version]
- Keskin Kurt, R.; Kaya, O.A.; Karateke, A.; Silfeler, D.B.; Karapınar, O.S.; Akkoca, A.N.; Hakverdi, A.U. Increased Density of Demodex folliculorum Mites in Pregnancies with Gestational Diabetes. Med. Princ. Pract. 2014, 23, 369–372. [Google Scholar] [CrossRef]
- Esteves Lima, R.P.; Miranda Cota, L.O.; Costa, F.O. Association Between Periodontitis and Gestational Diabetes Mellitus: A Case-Control Study. J. Periodontol. 2013, 84, 1257–1265. [Google Scholar] [CrossRef] [PubMed]
- Chokwiriyachit, A.; Dasanayake, A.P.; Suwannarong, W.; Hormdee, D.; Sumanonta, G.; Prasertchareonsuk, W.; Wara-Aswapati, N.; Combellick, J.; Pitiphat, W. Periodontitis and Gestational Diabetes Mellitus in Non-Smoking Females. J. Periodontol. 2013, 84, 857–862. [Google Scholar] [CrossRef] [PubMed]
- Xiong, X.; Elkind-Hirsch, K.E.; Vastardis, S.; Delarosa, R.L.; Pridjian, G.; Buekens, P. Periodontal Disease Is Associated With Gestational Diabetes Mellitus: A Case-Control Study. J. Periodontol. 2009, 80, 1742–1749. [Google Scholar] [CrossRef] [PubMed]
- Odar, E.; Wandabwa, J.; Kiondo, P. Maternal and fetal outcome of gestational diabetes mellitus in Mulago Hospital, Uganda. Afr. Health Sci. 2004, 4, 9–14. [Google Scholar] [PubMed]
- Piper, J.M.; Georgiou, S.; M-j Xenakis, E.; Langer, O. Group B Streptococcus Infection Rate Unchanged by Gestational Diabetes. Obstet. Gynecol. 1999, 93, 292–296. [Google Scholar]
- ElSayed, N.A.; Aleppo, G.; Aroda, V.R.; Bannuru, R.R.; Brown, F.M.; Bruemmer, D.; Collins, B.S.; Gaglia, J.L.; Hilliard, M.E.; Isaacs, D.; et al. Classification and Diagnosis of Diabetes: Standards of Care in Diabetes-2023. Diabetes Care 2023, 46 (Suppl. S1), S19–S40. [Google Scholar] [CrossRef]
- Abu-Ashour, W.; Twells, L.; Valcour, J.; Randell, A.; Donnan, J.; Howse, P.; Gamble, J.-M. The association between diabetes mellitus and incident infections: A systematic review and meta-analysis of observational studies. BMJ Open Diabetes Res. Care 2017, 5, e000336. [Google Scholar] [CrossRef]
- Lipsky, B.A.; Boyko, E.J.; Inui, T.S.; Koepsell, T.D. Risk factors for acquiring pneumococcal infections. Arch. Intern. Med. 1986, 146, 2179–2185. [Google Scholar] [CrossRef]
- Dunkel, N.; Uçkay, I.; Belaieff, W.; Assal, M.; Corni, V.; Lacraz, A.; Karaca, Ş. Wound dehiscence and stump infection after lower limb amputation: Risk factors and association with antibiotic use. J. Orthop. Sci. 2012, 17, 588–594. [Google Scholar] [CrossRef]
- António, N.; Prieto, D.; Providência, L.A.; Antunes, M.J. Diabetes mellitus does not affect one-year outcome after heart transplantation. Rev. Port. Cardiol. 2010, 29, 205–220. [Google Scholar]
- Aagaard, K.; Riehle, K.; Ma, J.; Segata, N.; Mistretta, T.-A.; Coarfa, C.; Raza, S.; Rosenbaum, S.; Veyver, I.V.D.; Milosavljevic, A.; et al. A Metagenomic Approach to Characterization of the Vaginal Microbiome Signature in Pregnancy. PLoS ONE 2012, 7, e36466. [Google Scholar] [CrossRef] [PubMed]
- Koren, O.; Goodrich, J.K.; Cullender, T.C.; Spor, A.; Laitinen, K.; Bäckhed, H.K.; Gonzalez, A.; Werner, J.J.; Angenent, L.T.; Knight, R.; et al. Host Remodeling of the Gut Microbiome and Metabolic Changes during Pregnancy. Cell 2012, 150, 470–480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacIntyre, D.A.; Chandiramani, M.; Lee, Y.S.; Kindinger, L.; Smith, A.; Angelopoulos, N.; Lehne, B.; Arulkumaran, S.; Brown, R.; Teoh, T.G.; et al. The vaginal microbiome during pregnancy and the postpartum period in a European population. Sci. Rep. 2015, 5, 8988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marschalek, J.; Farr, A.; Kiss, H.; Hagmann, M.; Göbl, C.S.; Trofaier, M.-L.; Kueronya, V.; Petricevic, L. Risk of Vaginal Infections at Early Gestation in Patients with Diabetic Conditions during Pregnancy: A Retrospective Cohort Study. PLoS ONE 2016, 11, e0155182. [Google Scholar] [CrossRef] [Green Version]
- Stoikou, M.; Grimolizzi, F.; Giaglis, S.; Schäfer, G.; Van Breda, S.V.; Hoesli, I.M.; Lapaire, O.; Huhn, E.A.; Hasler, P.; Rossi, S.W.; et al. Gestational Diabetes Mellitus Is Associated with Altered Neutrophil Activity. Front. Immunol. 2017, 8, 702. [Google Scholar] [CrossRef] [Green Version]
- Taddei, C.R.; Cortez, R.V.; Mattar, R.; Torloni, M.R.; Daher, S. Microbiome in normal and pathological pregnancies: A literature overview. Am. J. Reprod. Immunol. 2018, 80, e12993. [Google Scholar] [CrossRef] [PubMed]
- Donders, G.G.G.; Bosmans, E.; Dekeersmaeckerb, A.; Vereecken, A.; Van Bulck, B.; Spitz, B. Pathogenesis of abnormal vaginal bacterial flora. Am. J. Obs. Gynecol. 2000, 182, 872–878. [Google Scholar] [CrossRef]
- De Siena, M.; Laterza, L.; Matteo, M.V.; Mignini, I.; Schepis, T.; Rizzatti, G.; Ianiro, G.; Rinninella, E.; Cintoni, M.; Gasbarrini, A. Gut and Reproductive Tract Microbiota Adaptation during Pregnancy: New Insights for Pregnancy-Related Complications and Therapy. Microorganisms 2021, 9, 473. [Google Scholar] [CrossRef]
- Cobb, C.; Kelly, P.; Williams, K.; Babbar, S.; Angolkar, M.; Derman, R. The oral microbiome and adverse pregnancy outcomes. Int. J. Womens Health 2017, 9, 551–559. [Google Scholar] [CrossRef] [Green Version]
- Nae, B.; Wainstock, T.; Sheiner, E. The significance of maternal asymptomatic bacteriuria during pregnancy on long-term offspring infectious hospitalizations. J. Dev. Orig. Health Dis. 2022, 13, 508–513. [Google Scholar] [CrossRef]
- Renko, M.; Tapanainen, P.; Tossavainen, P.; Pokka, T.; Uhari, M. Meta-Analysis of the Significance of Asymptomatic Bacteriuria in Diabetes. Diabetes Care 2011, 34, 230–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, B.R.; Hux, J.E. Quantifying the Risk of Infectious Diseases for People with Diabetes. Diabetes Care 2003, 26, 510–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Golan, A.; Wexler, S.; Amit, A.; Gordon, D.; David, M.P. Asymptomatic bacteriuria in normal and high-risk pregnancy. Eur. J. Obstet. Gynecol. Reprod. Biol. 1989, 33, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Delzell, J.E.; Lefevre, M.L. Urinary tract infections during pregnancy. Am. Fam. Physician 2000, 61, 713–721. [Google Scholar] [PubMed]
- Cortez, R.V.; Taddei, C.R.; Sparvoli, L.G.; Ângelo, A.G.S.; Padilha, M.; Mattar, R.; Daher, S. Microbiome and its relation to gestational diabetes. Endocrine 2019, 64, 254–264. [Google Scholar] [CrossRef] [PubMed]
- Folli, F.; Corradi, D.; Fanti, P.; Davalli, A.; Paez, A.; Giaccari, A.; Perego, C.; Muscogiuri, G. The Role of Oxidative Stress in the Pathogenesis of Type 2 Diabetes Mellitus Micro- and Macrovascular Complications: Avenues for a Mechanistic-Based Therapeutic Approach. Curr. Diabetes Rev. 2011, 7, 313–324. [Google Scholar] [CrossRef] [PubMed]
- Halim, M.; Halim, A. The effects of inflammation, aging and oxidative stress on the pathogenesis of diabetes mellitus (type 2 diabetes). Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 1165–1172. [Google Scholar] [CrossRef]
- Morrell, C.N. Reactive oxygen species: Finding the right balance. Circ. Res. 2008, 103, 571–572. [Google Scholar] [CrossRef]
- Craig, M.E.; Nair, S.; Stein, H.; Rawlinson, W.D. Viruses and type 1 diabetes: A new look at an old story. Pediatr. Diabetes 2013, 14, 149–158. [Google Scholar] [CrossRef]
- Bendek, M.J.; Canedo-Marroquín, G.; Realini, O.; Retamal, I.N.; Hernández, M.; Hoare, A.; Busso, D.; Monteiro, L.J.; Illanes, S.E.; Chaparro, A. Periodontitis and Gestational Diabetes Mellitus: A Potential Inflammatory Vicious Cycle. Int. J. Mol. Sci. 2021, 22, 11831. [Google Scholar] [CrossRef]
- Zhang, J.; He, L.; Huang, R.; Alvarez, J.F.; Yang, D.H.; Sun, Q.; Wang, F.; Peng, Z.; Jiang, N.; Su, L. Synergistic effect of elevated glucose levels with SARS-CoV-2 spike protein induced NOX-dependent ROS production in endothelial cells. Mol. Biol. Rep. 2023, 50, 6039–6047. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Authors | Location of Study | Study Design | Multicenter | Type of Infection | GDM Diagnosis Criteria | Number of Total Patients | Number of Patients without GDM with Infection/Total without GDM | Number of Patients with GDM with Infection/Total GDM | Strobe Score (Out of 22) |
|---|---|---|---|---|---|---|---|---|---|
| Eskenazi B, et al. 2022 [35] | Multinational 18 countries | Prospective cohort study | Yes | SARS-CoV-2 | Abstracted from medical records | 2071 | 564/1824 | 75/194 | 20 |
| Johnson CY, et al. 2021 [36] | USA | Case control study | Yes | urinary tract infections | N/A | 41,869 | 7003/38,908 | 445/2118 | 18 |
| Radan AP, et al. 2022 [37] | Switzerland | Case control study | No | SARS-CoV-2 | IADPSG criteria | 224 | 24/149 | 26/75 | 20 |
| Epelboin S, et al. 2021 [38] | France | Retrospective cohort study | Yes | SARS-CoV-2 | ICD 10 codes | 244,645 | 735/214,735 | 139/29,251 | 22 |
| Lukic A, et al. 2017 [39] | Italy | Prospective cohort study | Yes | Cervicovaginal Bacteria—group B Streptococcus, Gardnerella vaginalis, Candida spp., Chlamydia trachomatis, Mycoplasma hominis, and Ureaplasma urealyticum | N/A | 473 | 169/346 | 59/103 | 19 |
| Gogeneni H, et al. 2015 [40] | Turkey | Case control study | No | Gingivitis—Porphyromonas gingivalis, Filifactor alocis and Treponema denticola | IADPSG criteria | 117 | 31/58 | 38/59 | 18 |
| Son KH, et al. 2015 [41] | South Korea | Retrospective cohort study | Yes | Infection of genitourinary tract | ICD-10 codes (Data from National Health Insurance) | 1,282,498 | 246,378/1,171,575 | 19,323/78,716 | 18 |
| Keskin Kurt R, et al. 2013 [42] | Turkey | Prospective cohort study | No | Demodex folliculorum | Carpenter and Coustan criteria | 66 | 30-Jan | 9/33 | 18 |
| Esteves Lima RP, et al. 2013 [43] | Brazil | Case control study | No | Periodontitis | IADPSG criteria | 360 | 125/270 | 36/90 | 20 |
| Chokwiriyachit A, et al.2013 [44] | Thailand | Case control study | Yes | Periodontitis | the NDDG criteria | 100 | 13/50 | 25/50 | 18 |
| Mannan M, et al. 2012 [15] | Bangladesh | Cross-sectional study | Yes | urinary tract infections | Modified method of Carpenter and Coustan criteria following 75 g OGTT | 960 | 3/72 | 12/71 | 19 |
| Xiong X, et al. 2009 [45] | USA | Case control study | No | Periodontitis | Carpenter and Coustan criteria | 159 | 64/102 | 41/53 | 20 |
| Odar E, et al. 2004 [46] | Uganda | Prospective cohort study | No | Vaginal candidiasis | The WHO criteria for diagnosis of diabetes—two-hour 75 g oral glucose load | 90 | 2/60 | 30-Jun | 19 |
| Nowakowska D, et al. 2004 [24] | Poland | Cross-sectional study | No | Vaginal mycosis | N/A | 251 | 18/132 | 16/72 | 14 |
| Rizk DE, et al. 2001 [28] | United Arab Emirates | Prospective cohort study | No | E. coli, Klebsiella pneumonia, Proteus mirabilis, Staphylococcus aureus, and group B streptococcus Asymptomatic bacteriuria Symptomatic urinary tract infections Acute cystitis Acute pyelonephritis | Venous plasma glucose levels of 5.3 mmol/L after fasting and/or 8.6 mmol/L 2 h after an oral 75 g glucose load | 447 | 19/298 | 12/149 | 16 |
| Piper JM, et al. 1999 [47] | USA | Prospective cohort study | No | Group B Streptococcus colonization | At least one abnormal OGTT value according to the NDDG criteria | 1492 | 253/1046 | 117/466 | 18 |
| Authors | Selection | Comparability of Groups | Outcome/ Exposure | Total | Study Design | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |||
| Eskenazi B, et al. 2022 [35] | * | * | * | * | ** | * | * | * | 9 | Prospective cohort study |
| Johnson CY, et al. 2021 [36] | * | * | ** | * | * | * | 7 | Case control study | ||
| Radan AP, et al. 2022 [37] | * | * | * | ** | * | * | * | 8 | Case control study | |
| Epelboin S, et al. 2021 [38] | * | * | * | ** | * | * | * | 8 | Retrospective cohort study | |
| Lukic A, et al. 2017 [39] | * | * | * | ** | * | * | 7 | Prospective cohort study | ||
| Gogeneni H, et al. 2015 [40] | * | * | * | * | * | * | * | 7 | Case control study | |
| Son KH, et al. 2015 [41] | * | * | * | * | * | * | 6 | Retrospective cohort study | ||
| Keskin Kurt R, et al. 2013 [42] | * | * | * | * | ** | * | * | * | 9 | Prospective cohort study |
| Esteves Lima RP, et al. 2013 [43] | * | * | * | ** | * | * | * | 8 | Case control study | |
| Chokwiriyachit A, et al.2013 [44] | * | * | * | * | ** | * | * | * | 9 | Case control study |
| Mannan M, et al. 2012 [15] | * | * | * | ** | * | * | * | 8 | Cross-sectional study | |
| Xiong X, et al. 2009 [45] | * | * | * | * | ** | * | * | * | 9 | Case control study |
| Odar E, et al. 2004 [46] | * | * | * | * | * | * | * | 7 | Prospective cohort study | |
| Nowakowska D, et al. 2004 [24] | * | * | * | ** | * | * | * | 8 | Cross-sectional study | |
| Rizk DE, et al. 2001 [28] | * | * | * | * | ** | * | * | * | 9 | Prospective cohort study |
| Piper JM, et al. 1999 [47] | * | * | * | ** | * | * | * | 8 | Prospective cohort study | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yefet, E.; Bejerano, A.; Iskander, R.; Zilberman Kimhi, T.; Nachum, Z. The Association between Gestational Diabetes Mellitus and Infections in Pregnancy—Systematic Review and Meta-Analysis. Microorganisms 2023, 11, 1956. https://doi.org/10.3390/microorganisms11081956
Yefet E, Bejerano A, Iskander R, Zilberman Kimhi T, Nachum Z. The Association between Gestational Diabetes Mellitus and Infections in Pregnancy—Systematic Review and Meta-Analysis. Microorganisms. 2023; 11(8):1956. https://doi.org/10.3390/microorganisms11081956
Chicago/Turabian StyleYefet, Enav, Aviv Bejerano, Rula Iskander, Tal Zilberman Kimhi, and Zohar Nachum. 2023. "The Association between Gestational Diabetes Mellitus and Infections in Pregnancy—Systematic Review and Meta-Analysis" Microorganisms 11, no. 8: 1956. https://doi.org/10.3390/microorganisms11081956